Back to Journals » Integrated Pharmacy Research and Practice » Volume 5
Community pharmacists provided telephone treatment support for patients who received long-term prescribed medication
Authors Yamamoto N, Nitta M, Kamei M ![]() , Hara K, Watanabe F, Akagawa K, Kurata N
, Hara K, Watanabe F, Akagawa K, Kurata N
Received 11 November 2015
Accepted for publication 7 January 2016
Published 29 March 2016 Volume 2016:5 Pages 27—32
DOI https://doi.org/10.2147/IPRP.S100336
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Nobuo Yamamoto,1 Mitsuyo Nitta,1 Miwako Kamei,2 Kazuo Hara,1 Fumiyuki Watanabe,2 Keiko Akagawa,1 Naomi Kurata1
1Division of Community Healthcare and Pharmacy, Department of Healthcare and Regulatory Sciences, Showa University School of Pharmacy, Tokyo, Japan; 2Division of Health Communication, School of Pharmacy, Nihon University, Chiba, Japan
Purpose: This study was conducted to evaluate whether a community pharmacist’s assistance during the treatment of a patient with a chronic illness would help to discover and improve issues regarding the treatment.
Method: We employed a prospective intervention study with a control group. The patients ranging in age from 60 to 74, were using one of the six selected community pharmacies in the Tokyo metropolitan area. They had been prescribed six or fewer kinds of medications, one of which was amlodipine. The medication dosages covered 1 month or longer. Patients who agreed to participate in the study were randomly assigned to the groups at each pharmacy. For the patients in the intervention group, the pharmacists provided telephone counseling between physician visits, in addition to the time they visited the pharmacies to collect their medications. For the patients in the control group, the pharmacists provided counseling only at their pharmacies.
Results and discussion: The average days of medication administration were 49.2 days for the 58 patients in the intervention group, and 49.8 days for the 53 patients in the control group, with the average number of medications being 3.4 items per person for both groups. Through the telephone counseling, we were able to collect more information, eg, changes in physical condition and occurrences of side effects, from the intervention group than from the control group. The rate of incident detection in the information from the intervention group was five times that of the control group, making subsequent incident resolutions faster.
Conclusion: This study suggested that phone counseling between physician visits could enable the identification of more issues regarding patients’ conditions.
Keywords: community pharmacy, outpatient, long-term dosage, telephone assistance
Introduction
Under the national health care system in Japan, physicians were only allowed to prescribe medications covering a maximum of either 14 or 30 days, except for medications for epilepsy and thyroid hormones, for which the maximum was 90 days.1 In April 2002, this restriction on the length of prescriptions was removed, allowing longer-term prescriptions.2 Consequently, the length of prescriptions continued to become longer to this day, 12 years later.3 Currently, the Japanese system does not allow prescription refills. When pharmacists in Japan fill a prescription, they generally dispense for the entire prescription period at the same time. To dispense only part of a prescription, a reason related to the quality management of the medication and the patient’s agreement are required. If there are no quality-related issues, the entire prescription amount is given to the patient, eg, 180 days’ worth of medication is given if the medication was prescribed for a 180-day period.
Although longer-term prescriptions may alleviate patient crowding in medical institutions and the burden on the physician, as well as alleviating the burden on the patient collecting their medications at the hospital, they result in more difficulty in ascertaining the condition of the patient during the prescription period, with the possibility of decreased quality of care due to health changes or misadministration, and of an increased number of unused prescriptions.4–7 A 2010 Japan Medical Association survey carried out on physicians cited reports of delays in physicians’ discovery of changes in the patient’s health due to long-term prescriptions, cases of acute exacerbation and growing severity, and elderly patients who endured declining health conditions during a long-term prescription.8
When handing dispensed medications to their patients, pharmacists are required to collect information from the patients and provide them with information regarding the proper use of the medications.9 However, patients come to the pharmacy after having waited for a long time to be seen by their physicians. Thus, patients are often reluctant to wait again at the pharmacy, resulting in insufficient interaction.
To address the various issues that long-term prescriptions entail, a pilot study was conducted, in which treatment assistance during the prescription period was selected from: 1) split dispensing (partial prescription filling), 2) house calls, and 3) telephone calls.10 The study suggested that regular involvement of the pharmacist provides benefits in terms of the usefulness and safety of pharmacotherapy. Reports from other countries suggest telephone counseling and early intervention by the pharmacist improve adherence and effectively reduce medical expenses,11 and that telephone counseling by the pharmacist improves cardiovascular disease patient compliance and reduces the mortality rate.12
In this study, community pharmacists provided medication assistance by telephone to patients taking amlodipine, which is known to be administered to many patients on a long-term basis. Data were collected and sorted and issues to be resolved were identified, while the effectiveness of the pharmacists’ treatment assistance during the prescription period was evaluated.
Methods
Study design and setting
This was a prospective intervention study with a control group. The study protocol was approved by the research ethics committee of Showa University. Six community pharmacies in the Tokyo metropolitan area of Japan participated in the study. Participants were patients who visited one of the participating stores in September 2010 and who:
- were hypertension patients between the ages of 60 and 74;
- were prescribed six or fewer medications including amlodipine;
- had 28 days of prescription or longer;
- agreed to telephone counseling;
- agreed to participate in the study.
Participating pharmacies managed patient information on a closed online network. Names of patients who met the inclusion criteria appeared on the store computer, making them candidates for recruitment. Patients who agreed to participate in the study were automatically and randomly assigned to the groups at each pharmacy using the minimization method, based on age (60s and 70s), sex, and number of prescribed medications (one to three; and four to six). The study period was from July 2010 to January 2011, with each case starting after the patient gave written informed consent.
Intervention
A total of seven pharmacists provided counseling. They were selected from those who had had at least 3 years of experience at their pharmacies and consented to participate in this study.
In the intervention group, a pharmacist called the patient at home for counseling once between two physician visits. If the interval between physician visits exceeded 2 months, telephone counseling was provided once a month. The same support for medication administration was provided for both groups when they visited the pharmacy.
The pharmacist who provided counseling recorded all patient information in the same format in compliance with the procedure manual of this study. Recorded items totaled eleven: blood pressure; changes in physical condition; side effects; medication administration; quality change in unused medications; visits to physicians of other specialties; concomitant medications; over-the-counter medication; medication interactions; changes in lifestyle; and other (Table 1).
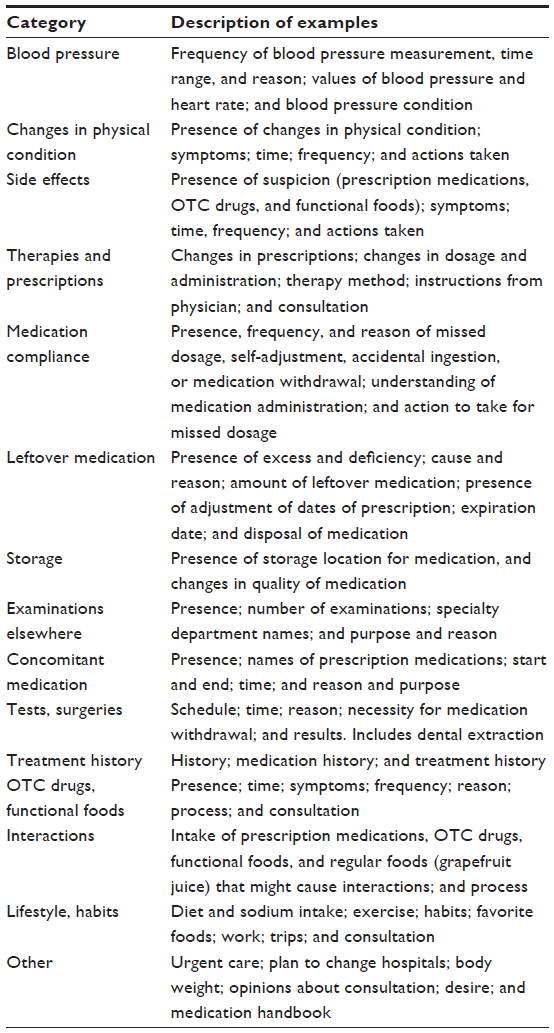 | Table 1 Category of recorded items |
Measurement of outcomes
The follow-up period was 4 months for each patient. After this period, we counted the number of items recorded using the records obtained from counseling, the number of items with incidents, and the number of items whose incidents had been resolved. We also conducted a survey using a self-completed questionnaire to measure changes in the awareness and behavior compared to 4 months earlier.
Data analysis
Patient characteristics, the number of counseling sessions, the number of items recorded, the number of items with incidents, and the number of items whose incidents had been resolved were tallied up, categorized by counseling given at the pharmacy and by telephone, after which we compared the results between the two groups. The intention to treat method was used for the analysis. The Student’s t-test and χ2 test were used to determine significance in differences.
Results
Attributes of study participants
The control group consisted of 53 participants, and the intervention group 59 participants. The average age was 67.6±4.3 for the control group, and 66.9±3.9 for the intervention group. The average initial prescription period per prescription for the control group was 61.3±23.2 days (maximum 180 days), and the intervention group 56.9±23.3 days (maximum 104 days) (Table 2).
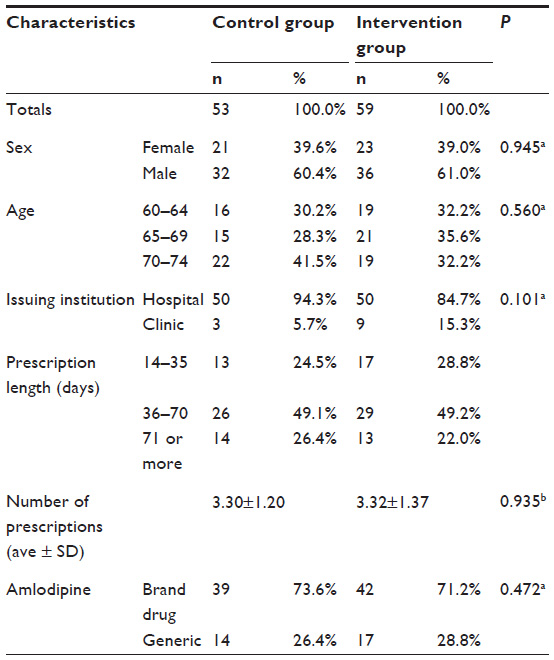 | Table 2 Characteristics of participants at start of study |
The control group had two withdrawals. The intervention group had two withdrawals from telephone counseling, one hospital transfer, and one withdrawal due to use of more than one pharmacy.
Number of counseling sessions
The average number of times the pharmacists provided treatment assistance to the participants was 2.9 times per person for the control group and 4.8 times per person for the intervention group. The control group received treatment assistance only when they visited the pharmacy to fill a prescription, whereas the intervention group additionally received telephone counseling (1.9 times per participant).
Data collection
The number of data items collected from counseling is shown in Table 3. For the control group, the number of counseling sessions conducted at the pharmacy was 837 (15.8 per person), and 935 for the intervention group (57.9% or 15.8 per person). Additionally, the intervention group received 680 telephone counseling sessions (42.1% or 11.5 per person). Seventy to 80% of the collected data were only recorded without any action. However, the intervention group, who also received counseling by telephone, received nearly three times as much counseling as the control group.
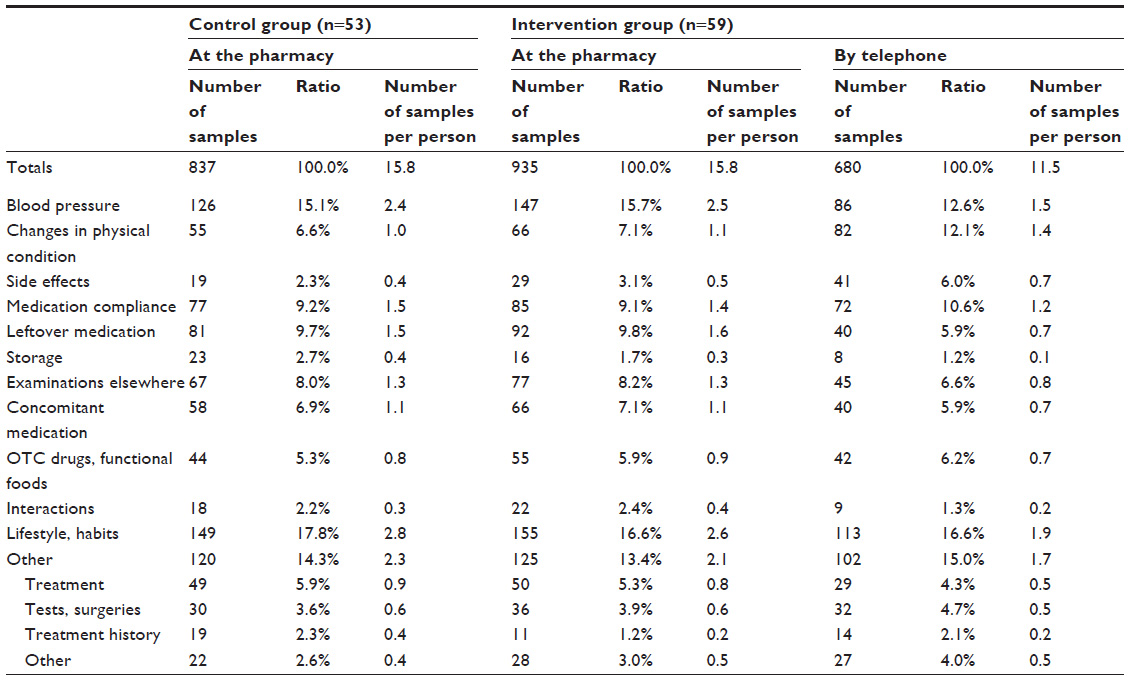 | Table 3 Number of data items collected from counseling |
Issues and actions (counseling)
Table 4 shows the incidents with priority needs, eg, high urgency and/or importance. The number of items with these incidents was nine (5.7%) for the control group, whereas it was 46 (10.2%), including 37 (8.2%) by phone counseling, for the intervention group, representing approximately five times as many as that of the control group. The number of items whose incidents had been resolved during the 4-month follow-up period was three (1.9%) for the control group and 25 (5.6%) for the intervention group. Table 5 shows the breakdown of the assistance for issues with high priority and the numbers of incidents verified as resolved.
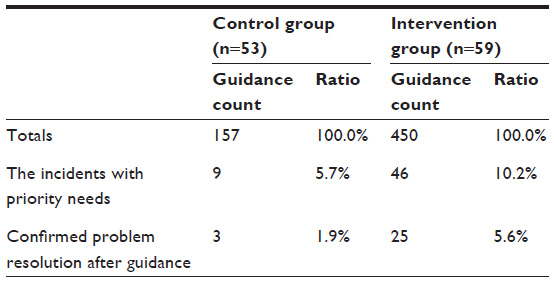 | Table 4 Number of times guidance provided |
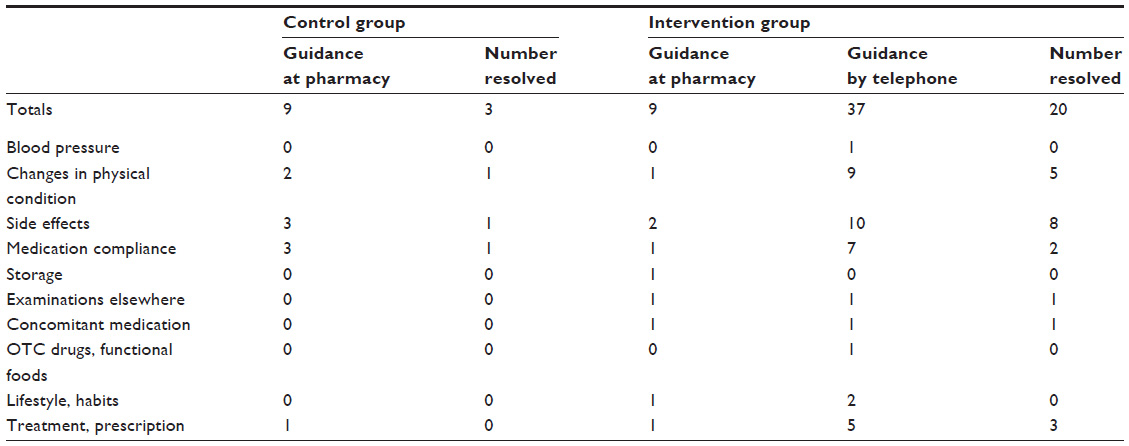 | Table 5 Guidance for important items and number of resolved cases |
Changes in attitude and behavior
One of the questions in the questionnaire asked about any changes in the patient’s attitude and behavior between the start of the study and the time of evaluation. The responses are shown in Table 6. Only “have a higher desire for treatment” scored higher in the intervention group.
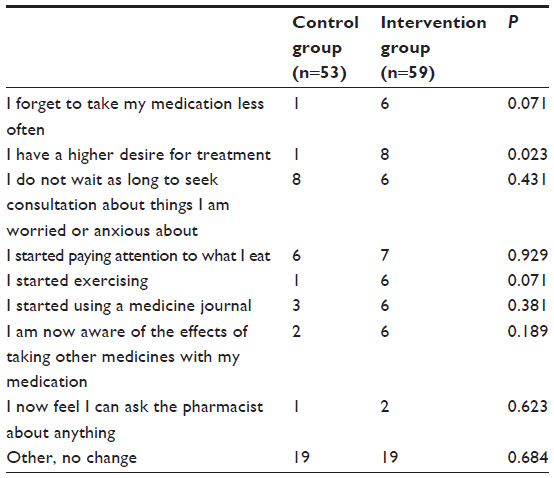 | Table 6 Changes in awareness and behavior at end of study |
Discussion
This study was conducted on elderly patients taking amlodipine, including its generics, which are commonly used for long-term prescriptions. A 2011 national survey by the Ministry of Health, Labour and Welfare indicates a higher prevalence of hypertension in the population of 60 years and older and there are approximately 1.9 million patients with hypertension.13 According to another survey by the Ministry of Health, Labour and Welfare in 2011, the greatest number of medications dispensed at community pharmacies was 21.9%, which were cardiovascular medications by therapeutic classification.14 There are also studies that reported that the drugs most often prescribed over a long term were antilipemic medications and antihypertensive medications.8,10 Another study reported that the examination of the management of hypertension in the elderly suggested that their blood pressure management was inadequate.15
Because the intervention group had more opportunities to talk with the pharmacists than the control group, more information was obtained from the intervention group and their situations were better identified. Although most of the information identified was verified by the pharmacist and recorded with no action taken, guidance was provided when necessary, just as with regular medication guidance. The number of counseling sessions for incidents determined to be of high urgency and/or importance was greater in the intervention group than the control group. In fact, telephone counseling enabled early assistance in dealing with side effects, changes in physical condition, and urgent incidents caused by a lack of understanding in how to take medications. Additionally, the intervention group scored high for the item “the desire for treatment increased”, which indicates that changes in awareness and behavior may have improved medication adherence. The telephone counseling enabled regular and continuous assistance to resolve issues. It may also have assisted in resolution of issues, in addition to illnesses, that could not have been covered by on-site counseling alone.
At times it was difficult to identify the patient’s situation as well as mental and physical conditions during telephone counseling, with some intervention group members withdrawing from telephone counseling. On the other hand, some patients went to the pharmacy for counseling on medications as well as for having their prescriptions filled, indicating that this study may have created an opportunity to discover that they could talk to their pharmacist any time they had questions. Treatment assistance with pharmacist participation during the prescription period may not only allow early response to issues, but also result in changes in attitude and behavior that lead to issue resolution.
Conclusion
In Japan, where prescriptions are not refilled, patients must always visit medical institutions to see physicians before receiving prescribed medications at pharmacies. For this reason, many patients do not feel the need to interact with pharmacists. Under these circumstances, days of medication administration lengthen year after year, with nobody being able to notice any changes in the patients for months. This study suggested that telephone counseling by pharmacists between physician visits might accelerate the resolution of patients’ issues, if only a little.
Acknowledgments
We would like to express our sincere thanks to the pharmacists at the six pharmacies who participated in this study.
Disclosure
The authors have no conflicts of interest to disclose.
References
Ministry of Health, Labour and Welfare Notification No 73, March 17, 2000. http://www.mhlw.go.jp/topics/bukyoku/hoken/sinryou/02kokuji/dl/kokuji26a.pdf. Accessed February 6, 2011. | |
Ministerial Ordinance Concerning National Health Insurance Act, No 23, 2002. http://www.mhlw.go.jp/topics/bukyoku/hoken/sinryou/02kokuji/dl/syourei1.pdf. Accessed February 6, 2011. | |
Ministry of Health, Labour and Welfare, Trends of Health Expenditure of Community Pharmacy [webpage on the Internet]. Japan: Ministry of Health, Labour and Welfare; 2014. Available from: http://www.mhlw.go.jp/bunya/iryouhoken/database/zenpan/cyouzai_doukou.html. Accessed January 12, 2016. | |
Kamei M, Onda M. Effects of deregulation on prescription term for outpatients’ drug therapy. Journal of Japan Society for Health Care Management. 2003;4(3):377–383. | |
Onda M, Kamei M. [Impacts of deregulation of drug prescription term to the patient adherence]. Japanese Journal of Social Pharmacy. 2004;23(1):29–34. Japanese. | |
Onda M, Kamei M, Kono K. Impacts on the quality of medication service for outpatients and management of medical institutions by deregulation of drug prescription term. Japanese Journal of Health Economics and Policy. 2004;15:5–22. | |
Japan Pharmaceutical Association. Working paper. Available from: http://www.nichiyaku.or.jp/action/wp-content/uploads/2009/02/choukitouyaku.pdf. Japan Pharmaceutical Association; 2009. Accessed February 27, 2011. | |
Japan Medical Association Research Institute, Working paper No 225, 2010. http://www.med.or.jp/etc/eq201103/hoken/110311eq140.pdf. Accessed February 27, 2011. | |
Pharmacists Act, Article 25-2, 2013. http://www.japaneselawtranslation.go. jp/law/detail_main?re=01&vm=04&id=2596. Acccessed September 1, 2015. | |
Kamei M, Ikeda S, Muto M, Iijima U, Yamamoto N. [A Study on the effectiveness of pharmaceutical care management to the elderly patients with chronic disease]. Journal of Japan Society for Healthcare Administration. 2007;44:144. Japanese. | |
Elliott RA, Barber N, Clifford S, Horne R, Hartley E. The cost effectiveness of a telephone-based pharmacy advisory service to improve adherence to newly prescribed medicines. Pharm World Sci. 2008;30(1):17–23. | |
Wu JY, Leung WY, Chang, S, et al. Effectiveness of telephone counseling by a pharmacist in reducing mortality in patients receiving polypharmacy: randomized controlled trial. BMJ. 2006;333(7567):522. | |
Ministry of Health, Labour and Welfare [homepage on the Internet]. Summary of Patient Survey 2011. Ministry of Health, Labour and Welfare; 2012. Available from: http://www.mhlw.go.jp/english/database/db-hss/sps_2011.html. Accessed January 12, 2016. | |
Ministry of Health, Labour and Welfare [homepage on the Internet]. Estimates of National Medical Care Expenditure FY 2012. Ministry of Health, Labour and Welfare; 2014. Available from: http://www.mhlw.go.jp/english/database/db-hss/enmce_2012.html. Accessed January 12, 2016. | |
Ohta Y, Dobashi T, Miyata E, Onaka U. [A study on the management status of elderly patients with hypertension]. Journal of Blood Pressure. 2008;15(8):712–715. Japanese. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.