Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Community Knowledge, Self-Reported Prevalence, and Management of Epilepsy in Lira District: A Descriptive Cross-Sectional Study
Authors Okullo CO ![]() , Nakaziba R
, Nakaziba R ![]()
Received 14 April 2026
Accepted for publication 26 June 2026
Published 9 July 2026 Volume 2026:22 616816
DOI https://doi.org/10.2147/NDT.S616816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Christopher Oneka Okullo,1 Rebecca Nakaziba2
1Department of Community Health, Lira University, Lira, Uganda; 2Department of Pharmacology & Therapeutics, Lira University, Lira, Uganda
Correspondence: Christopher Oneka Okullo, Email [email protected]
Background: Epilepsy is a chronic neurological disorder characterized by spontaneous, recurrent seizures affecting over 70 million individuals worldwide, irrespective of age, gender, or location. The burden is poorly documented in rural communities in Sub-Saharan Africa. People with epilepsy face social stigma, discrimination, and overall productivity losses. This study investigated self-reported prevalence, community knowledge, and the management approaches of epilepsy in Lira district, Uganda.
Methods: A descriptive cross-sectional community –based study was conducted across the ten sub-counties of Lira District, employing random sampling among 400 adults, one per household. Data were collected using a pre-tested, interviewer-administered questionnaire translated into the local language (Leb Lango). Data was analyzed using SPSS v26, employing descriptive statistics (frequencies and percentages) and presented in form of tables and figures.
Results: The majority (81%) of the 400 participants described epilepsy as a disease of sudden falling. 51.7% attributed it to severe malaria, and overthinking. While 54.8% reported having a close family member with epilepsy, the self-reported prevalence of the actual cases of epilepsy observed during the study was 25/400 (6.25%). Study participants reported symptoms such as black outs and sudden falls (91.8%) as well as convulsions (86.3%). Epilepsy onset was predominantly reported in childhood (42.5%). Most attacks occurred at no specific time (40.5%) or during moonrise/moonset (32.5%). 75% of respondents reported warning signs including dizziness (78.3%), palpitations (72.5%), and blurred vision (64.5%). Approximately 35% of families sought help from a hospital or herbalist, and 80% reported no improvement.
Conclusion: This study documents a high self-reported prevalence and poor community management for epilepsy in Lira district. Community-based self-reports, rather than clinically verified findings, highlight the need for validated community screening programs, training of community health workers, strengthening of referral pathways, and supporting clinically validated prevalence studies.
Keywords: epilepsy, community knowledge, self-reported prevalence, management
Background
Epilepsy is a common and chronic neurological CNS disorder characterized by spontaneous seizures affecting over 70 million individuals worldwide, irrespective of age, gender, or location1,2. The silent burden of epilepsy in Africa is high due to fewer studies, especially in rural areas, with an estimated 9/1000 and 16/1000 active and lifetime cases, respectively.3 It is important to note that the onchocerciasis-associated epilepsy primarily documented in West and Central Africa is not a dominant etiology in the Lira district of Northern Uganda.1,2 Over 60% of epileptic patients in Sub-Saharan Africa receive no treatment, yet the prevalence almost doubles that in Asia, Europe, and North America.3,4 Eastern and Western Uganda are the most affected regions.5 When left untreated, people with epilepsy face devastating social consequences, including stigma and discrimination, and premature mortality.6–8 The stigma related to epilepsy, including being unmarried or unemployed, is intense since it is widely believed to be contagious and linked with witchcraft and/or evil spirits.6
Epilepsy is thought to occur due to genetic, metabolic, immunological, and acquired environmental factors.9,10 The resultant recurrent seizures then lead to synaptic remodeling, abnormal synaptic protein expression, and neuronal network formation.10–12
Epilepsy is treated using antiepileptic drugs such as phenytoin, ethosuximide, lamotrigine, and carbamazepine.8,12 Unfortunately, the available drugs that have to be used chronically are associated with unbearable adverse reactions.8,13,14 Moreover, natural drugs have also demonstrated clinical efficacy in epilepsy with a broad spectrum of antiepileptic activity and higher safety, except in some refractory epilepsies.15–17 It is reported that a combination of natural and conventional medicines reduces adverse reactions and improves the overall efficacy.17–19
The traditional management as used in this study refers to non-biomedical interventions, including herbal remedies, spiritual or religious healings, and other community-based practices not endorsed by the formal health system. In Uganda, accurate data regarding the regional prevalence of Epilepsy is lacking.20,21 Therefore, this study investigated the self-reported prevalence of Epilepsy, community knowledge, and traditional management in Lira district, to inform relevant bodies of its status and to stimulate further consideration or action on the subject as a public health priority.
Methods and Materials
Study Design
The study was a community-based descriptive cross-sectional study employing a quantitative approach to data collection, analysis, and interpretation.
Study Site and Setting
The study was conducted in Lira district, located in the Lango sub-region of Northern Uganda, 342 km from Kampala, Uganda’s capital. Lira district is bordered by Pader in the north, Otuke in the northeast, Alebtong in the east, Dokolo in the southeast, Apac in the southwest, and Kole in the west. The district is mainly populated by the Lango people, though it also has other tribes from across Uganda, including Acholi, Ateso, and Bantu-speaking groups. The residents are mainly subsistence farmers cultivating cereals, including maize and cassava. Community disease treatment is mainly through traditional approaches due to limited access to resources and long distances to health facilities.
Study Population
The study was conducted among adult (18 years and above) residents of Lira district who were present during the data collection period. Health workers, and the mentally unstable individuals were excluded. This criterion reflects the study’s focus on community knowledge and experience rather than clinical diagnosis.
Sample Size
The sample size was determined using the Slovin’s formula for survey sample size estimation as follows:22 n = N/1 + Ne2
Where:
n = Required sample size
N = Total population size
e = Margin of error (0.05 for 5%)
hence,
n=457000/1+(457000x0.052)
n=457000/1+1142.5
n=457000/1143.5
n=399.65
hence, 400
This sample size was equally distributed across the ten sub-counties of the district. Thus 40 participants were identified from each sub-county to get the total sample size of 400.
Sampling Procedure
The single stage cluster sampling technique was used in this study, with the ten sub-counties serving as the clusters. Within each cluster, 40 eligible participants were conveniently selected by moving to the first forty homes and identifying one eligible participant per household. This ensured geographic spread across the district. Upon identification, the participants provided a written informed consent before being recruited.
Data Collection Tool
Data was collected using an interviewer-administered questionnaire. The questionnaire (originally designed in English) was translated into the local language (Leb Lango) to ease understanding by the community. The study tool was designed to collect participants’ biodata, knowledge of epilepsy (defined as the occurrence of seizure activity characterized by symptoms such as sudden falls, jerking/convulsions, and loss of consciousness), experience with epilepsy, and management approaches.
Data Collection Procedure
Before each interview, the study purpose was fully explained to each eligible participants and obtained their individual consent. Following acquisition of informed consent, the interview was conducted with each eligible participant while taking note of the responses into the data collection tool. After each interview, the enumerator double checked the form to ensure completeness. Each interview session took between 25 and 35 minutes.
Data Management and Analysis
Data was checked for completeness, cleaned, and double-entered into the SPSS software version 26. Descriptive statistics (frequencies, and percentages) were computed for all variables. The findings are presented in form of tables and figures.
Ethical Considerations
The study was approved by the Lira University Research Ethics Committee (LUREC) under the approval number LUREC-2024-184. Prior to study commencement, approval was obtained from the District Health Officer (DHO) of Lira district and the sub-county Community Development Officer (CDO) for each respective sub-county in Lira District. All participants agreed to participate in the study by signing an informed consent form before being recruited. In this, the study title, objectives, and the benefits and risks associated with the study were explained to each participant, and only those who consented by signing the consent form were recruited. The participant anonymity was ensured by assigning unique participant codes and not recording personal identifiers on questionnaires; while participation was entirely voluntary and participants could withdraw at any time without any consequence. Moreover, international ethical codes such as the Helsinki declaration were upheld.
Results
Data were collected from 400 participants across the 10 sub-counties of Lira district, including Aromo, Ayami, Ogur, Iwal, Barr, Itek, Amach, Awiodyek, Agali, and Agweng. All the 400 respondents agreed to participate in the study hence 100% response rate.
Participant Biodata
Data was collected from mainly married (80.3%), Lango (95.5%), female (51.5%) participants aged 18–30 years. They were Roman Catholics (42.8%), had a primary level of education (63.7%), were farmers (65.8%), and had mobile phones (68.3%) (Table 1).
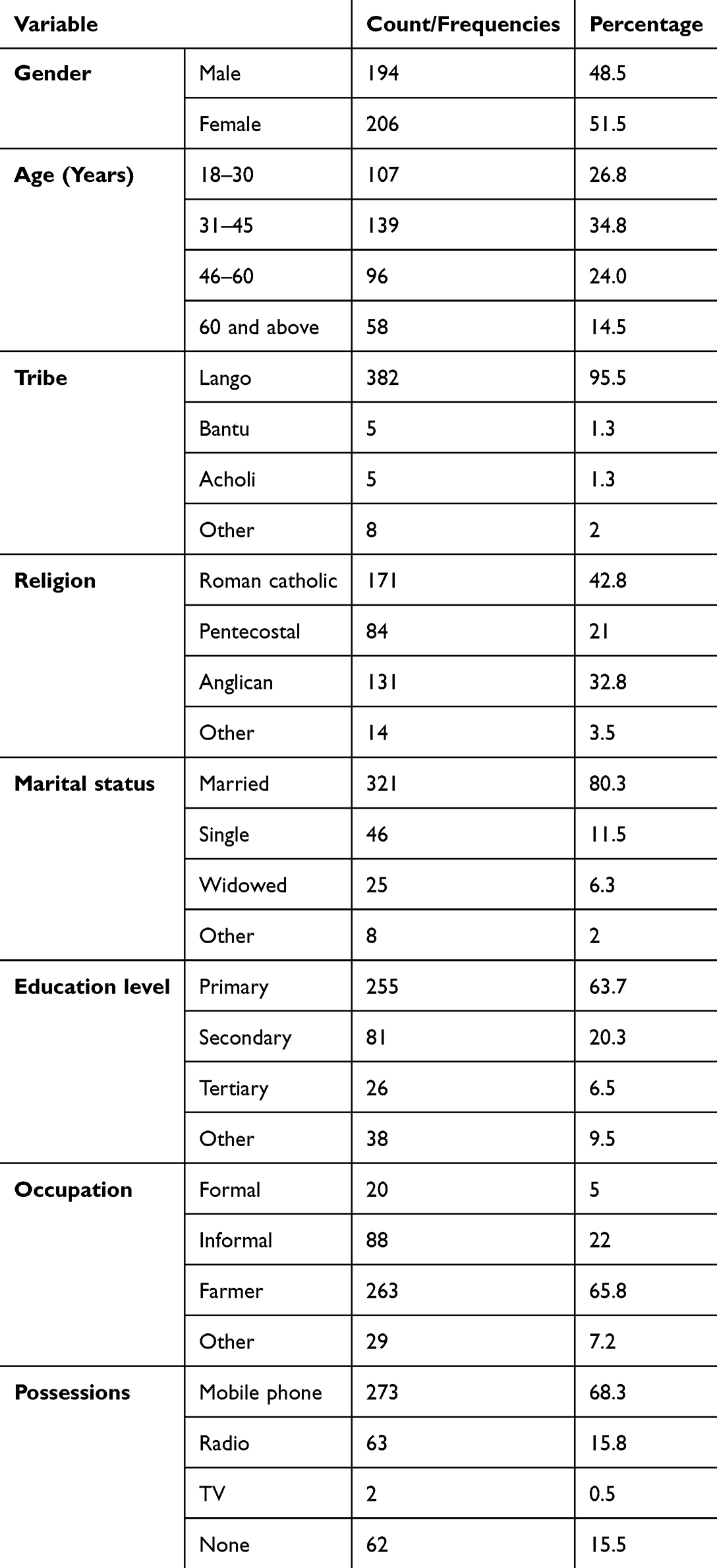 |
Table 1 Demographic Characteristics of Participants |
Epilepsy Knowledge
Most of the respondents (81%) described epilepsy as a disease characterized by falling, and (51.7%) attributed it to severe malaria and/or overthinking. A description of epilepsy as a disease associated with falling was the most common lay definition across all the sub-counties (Figures 1 and 2).
 |
Figure 1 Pie chart showing how different respondents described epilepsy. |
 |
Figure 2 Bar graph showing different causes of epilepsy as reported by the participants. |
Epilepsy in the Family
Of the 400 participants, 219 (54.5%) reported having a family member with epilepsy which predominantly started during childhood (42%). 25 cases (6.25%) were directly observed during the study (Table 2). Moreover, 63.2% reported having witnessed a seizure activity among their family members (Figure 3).
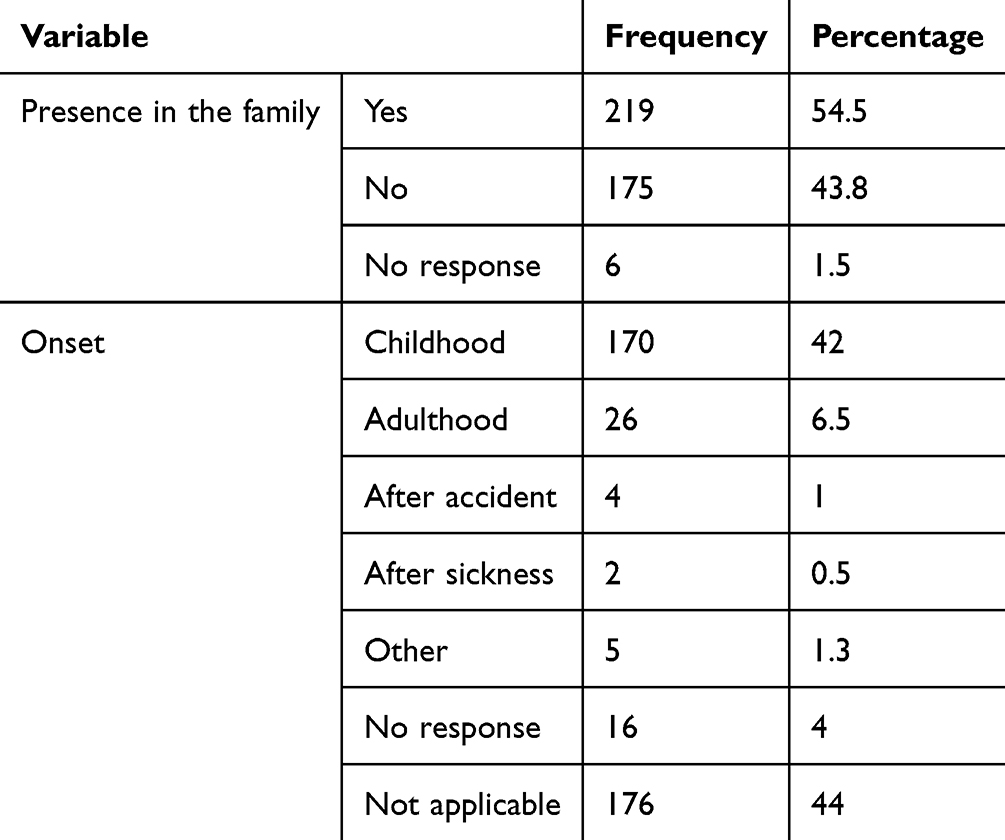 |
Table 2 Presence of Epilepsy in the Family and the Onset Time as Reported by the Study Participants |
 |
Figure 3 Bar graph showing percentage awareness of seizures in the family as reported by the participants. |
Occurrence of Epileptic Attacks
Most of the reported epileptic attacks occurred at no specific predicted time (40.5%), with a notable proportion reporting occurrence during moonrise/moonset (32.5%) (Table 3).
 |
Table 3 Occurrence of Epileptic Attacks in Lira District |
Symptoms of Epilepsy
The most reported symptoms included blackout and sudden fall/loss of consciousness (both 91.8%), jerking/convulsions (86.3%), falling and biting the tongue (82.5%) (Table 4).
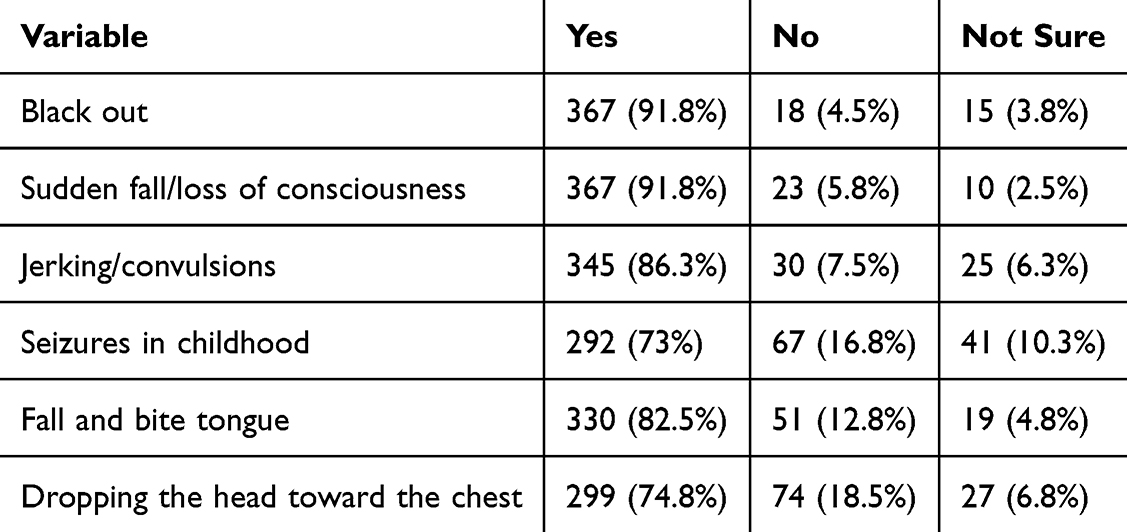 |
Table 4 Symptoms of Epilepsy |
Warning Signs
When asked about any warning signs, 75.5% of the respondents reported dizziness (78%), blurred vision (64.5%), and palpitations (pounding heart) (72.5%) (Table 5).
 |
Table 5 Warning Signs for an Epileptic Attack as Reported by the Respondents |
Experiences Before, During, and After the Event of an Epileptic Attack
As presented in Table 6, the most common reports before the event were a lack of self-awareness (81.5%) and a feeling of a strange environment or dream-like state (73.3%) while during the attack, jerking/convulsions (88.0%), stiff arms (85.3%), and automatisms (licking, chewing, swallowing, laughing; 83.8%) were most frequently reported. After the event, post-ictal confusion/drowsiness was nearly universal (88.1%).
 |
Table 6 Experiences Before, During, and After an Epileptic Attack |
Epilepsy Management (Family Attempts to Help Epileptic Patients)
About 35% of respondents sought help for their patients either at a hospital or from an herbalist. Of those who visited the herbalist, 85% did not know what was administered. Approximately 80% of respondents reported no improvement from these interventions (Figures 4 and 5).
 |
Figure 4 Pie chart showing different attempts by the family members to manage the epileptic patient. |
 |
Figure 5 Bar chart showing the frequency of effectiveness of the family’s attempts to support an epileptic patient. |
Discussion
This study examined the community knowledge, self-reported prevalence and management practices of Epilepsy in Lira district, Northern Uganda. The findings indicated an adequate level of knowledge since the participants correctly identified the symptoms of epilepsy (eg sudden falls and jerking/convulsions) which occurred any time right from childhood. According to the participants’ reports, the prevalence of Epilepsy in the district was alarmingly high (54.5%). However, only 25 (6.25%) physical cases were seen during the study. Unfortunately, there was poor management of the cases since most participants reported visiting both the hospital and the traditional healers with no improvement.
Self-Reported Prevalence
The self-reported prevalence of epilepsy cases was 6.25% (25/400). Meanwhile, 54.5% of the participants in the present study reported having a close family member with Epilepsy. However, these figures cannot be directly compared with clinically confirmed prevalence rates from studies employing EEG or video-EEG monitoring, as the methods of case ascertainment differ fundamentally. For reference, a peer-reviewed study of epilepsy prevalence across 25 sub-counties in three districts of Northern Uganda (including areas adjacent to Lira) reported substantially lower rates using community screening tools.20 A study in Kenya reported approximately 11.9 per 1,000 cases, while a pooled analysis of epilepsy in children and adolescents across Africa found a rate of 17.3 per 1,000.5 A study in southern Rwanda reported that 17.4% of community members screened positive for epilepsy, though confirmed diagnoses were fewer.
The elevated self-reported value in the present study likely reflects several sources of overestimation such as the lay definition of epilepsy as “falling and jerking” which may encompass conditions such as febrile rigors, nodding syndrome, syncope, and neurocysticercosis that present with similar symptoms. Moreover, data were based entirely on community self-report without clinical or electrophysiological verification. These caveats are critical for interpreting the values reported which should therefore be regarded as a community-perceived prevalence rather than an epidemiological prevalence estimate.
Community Knowledge
Most respondents (81%) described epilepsy in terms of sudden falling, consistent with recognition of convulsive/tonic-clonic presentations. This finding aligns with a cross-sectional study in Mukono district, Uganda, where over 90% of community members recognized epilepsy.23 However, community awareness appears to be largely limited to convulsive seizures, with non-convulsive seizure types (absence, focal aware, focal impaired awareness) likely underrecognized. The attribution of epilepsy to supernatural causes, malaria, and overthinking (51.7%) reflects persistent community misconceptions that contribute to stigma and delay in care-seeking. Targeted community education addressing both the biomedical nature of epilepsy and the spectrum of seizure types is urgently needed. The symptom profile, particularly the presence of aura, automatisms, and post-ictal confusion, is broadly consistent with generalized tonic-clonic seizures with possible focal onset components, though clinical verification was not performed. Most reported cases (42%) had childhood onset. This is consistent with the broader literature on epilepsy in sub-Saharan Africa, which highlights the role of adverse perinatal events, birth asphyxia, and febrile illnesses in childhood-onset epilepsy.5,10 These findings suggest that targeted perinatal care, particularly during labor and delivery, may be a preventive entry point for reducing epilepsy burden in resource-limited settings. While 40.5% of respondents reported seizures occurring at no specific time, 32.5% reported occurrence during moonrise/moonset. The biological basis for this association is unclear. A plausible explanation is a psychosocial or anticipatory mechanism. Individuals who believe seizures are associated with lunar phases may experience heightened anxiety during these periods, which could itself function as a trigger in susceptible individuals. The presence of pre-ictal aura symptoms, particularly dizziness, palpitations, and blurred vision in 75.5% of cases, is consistent with recognized somatosensory and autonomic aura descriptions in epilepsy.11 These warning signs represent an important opportunity for caregiver preparation and seizure first-aid.
Management Practices
Approximately 35% of the families visited a hospital or herbalist. 78.5% participants also reported no improvement thus reflecting well-documented barriers to effective epilepsy management in resource-limited settings including misdiagnosis, lack of diagnostic equipment, unavailability of antiepileptic drugs, and poor treatment adherence.8 The fact that 85% of those who visited herbalists did not know what was administered underscores the opacity and potentially unsafe nature of some traditional practices. Traditional management, in the absence of pharmacological treatment, cannot address the underlying neurological pathophysiology of epilepsy and may delay effective medical care. Strengthening community referral pathways and ensuring the availability of affordable antiepileptic drugs at the primary care level are essential steps.
Study Limitations
- Selection bias. The convenience sampling rendered the sample unrepresentative of the general community population. However, representations was improved by combination with cluster sampling.
- Information bias and reliance on self-report. All epilepsy diagnoses were based on community self-report, without clinical or electrophysiological verification (EEG or video-EEG). This may result in both over- and under-reporting.
- Misclassification of epilepsy. The lay definition of epilepsy may encompass conditions such as febrile convulsions, nodding syndrome, syncope, and neurocysticercosis, leading to potential overestimation of epilepsy frequency. It is acknowledged that some participants could have reported symptoms of malaria rather than true epilepsy, especially severe malaria with episodes resembling seizures characterized by febrile convulsions. This further underscores the need for clinical research to establish the true prevalence of clinically established epilepsy.
- Absence of medication data. The study did not systematically record medications prescribed at healthcare facilities, limiting the conclusions that can be drawn about pharmacological management.
- Cross-sectional design. The cross-sectional nature of the study limits causal inference and prevents assessment of disease trajectory over time.
Conclusion and Recommendation
This study documents a high community-reported prevalence of epilepsy and limited management capacity. The community demonstrates broad awareness of convulsive seizure presentations but harbors significant misconceptions regarding etiology, contagiousness, and management. All management practices were largely ineffective. These findings, while based on community self-reports without clinical validation, underscore the urgent need for:
- Validated community screening programs using standardized epilepsy detection tools recommended by the World Health Organization (WHO), International League Against Epilepsy (ILAE), or the Ministry of Health of Uganda.
- Capacity-building for community health workers in epilepsy recognition, seizure first-aid, and referrals, as well as strengthening referral pathways between communities and health facilities with diagnostic capacity by the Ministry of health, Uganda.
- Improved access to affordable anti-epileptic medications at the primary care level by the drug supply agencies in the country.
- Community sensitization campaigns to address misconceptions about epilepsy etiology, contagiousness, and management.
- Clinically validated epidemiological studies of epilepsy prevalence in Lira district and the broader districts.
Acknowledgment
We sincerely thank all participants for their generous acceptance to take part in this study. We also gratefully acknowledge the contributions of the community health workers and sub-county Community Development Officers of Lira district for facilitating data collection. In addition, we applause the Lira University Research and Innovation Fund for facilitating this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflict of interest in relation to the publication of this work.
References
1. Kariuki SM, Ngugi AK, Kengne AP, et al. Diagnosis and classification of pediatric epilepsy in Sub-Saharan Africa: a COMPREHENSIVE REVIEW. J Clin Med. 2024;13(21):6396. doi:10.3390/jcm13216396
2. Van Cutsem G, Siewe Fodjo J, Hadermann A, et al. Onchocerciasis-associated epilepsy: charting a path forward. Seizure Eur J Epilepsy. 2024. doi:10.1016/j.seizure.2024.04.018
3. Ba-Diop A, Marin B, Druet-Cabanac M, Ngoungou EB, Newton CR, Preux PM. Epidemiology, causes, and treatment of epilepsy in sub-Saharan Africa. Lancet Neurol. 2014;13(10):1029–12. doi:10.1016/S1474-4422(14)70114-0
4. Bhalla D, Lotfalinezhad E, Timalsina U, et al. A meta-analysis of the epidemiology of epilepsy in developing countries of the Asia-Pacific region. Epilepsy Res. 2019;157:106193. doi:10.1016/j.eplepsyres.2019.106193
5. Fuller AT, Almojuela A, Kaddumukasa MN, et al. Hospital-based epilepsy care in Uganda: a prospective study of three major public referral hospitals. Epilepsy Behav. 2021;114:107301. doi:10.1016/j.yebeh.2020.107301
6. Kariuki SM, Matuja W, Akpalu A, et al. Clinical features, proximate causes, and consequences of active convulsive epilepsy in Africa. Epilepsia. 2014;55(1):76–85. doi:10.1111/epi.12528
7. Musekwa OP, Makhado L, Maphula A, et al. How Much Do We Know? Assessing Public Knowledge, Awareness, Impact, and Awareness Guidelines for Epilepsy: A Systematic Review [Internet]. 2020. doi: 10.2174/1874944502013010794
8. Löscher W, Potschka H, Sisodiya SM, Vezzani A. Drug resistance in epilepsy: clinical impact, potential mechanisms, and new innovative treatment options. Pharmacol Rev. 2020;72(3):606–638. doi:10.1124/pr.120.019539
9. Vera-González A. Pathophysiological mechanisms underlying the etiologies of seizures and epilepsy. In: Czuczwar SJ, editor. Epilepsy [Internet]. Brisbane (AU): Exon Publications;2022. http://www.ncbi.nlm.nih.gov/books/NBK580618/.
10. Marin-Castañeda LA, Pacheco Aispuro G, González-Garibay G, et al. Interplay of epilepsy and long-term potentiation: implications for memory. Front Neurosci. 2025. doi:10.3389/fnins.2024.1451740
11. Vlooswijk MCG, Jansen JFA, de Krom MCTFM, et al. Somatosensory auras in epilepsy: a case series. Epilepsy Behav. 2010;18(1–2):96–99.
12. Devinsky O, Vezzani A, O’Brien TJ, et al. Epilepsy. Nat Rev Dis Primers. 2018;4:18024. doi:10.1038/nrdp.2018.24
13. Epilepsy and seizures treatment & management: approach considerations, anticonvulsant therapy, anticonvulsants for specific seizure types [Internet]. 2025. Available from: https://emedicine.medscape.com/article/1184846-treatment?form=fpf.
14. Mohanraj R, Brodie MJ. Measuring the efficacy of antiepileptic drugs. Seizure. 2003;12(7):413–443. doi:10.1016/S1059-1311(03)00047-5
15. French JA, Perucca E. Time to start calling things by their own names? The case for antiseizure medicines. Epilepsy Curr. 2020;20(2):69–72. doi:10.1177/1535759720905516
16. Liu W, Ge T, Pan Z, Leng Y, Lv J, Li B. The effects of herbal medicine on epilepsy. Oncotarget. 2017;8(29):48385–48397. doi:10.18632/oncotarget.16801
17. Sander JW. Overview of established antiepileptic drugs. Seizure. 2004;13(Suppl 1):S25–30.
18. van Wyk AS, Prinsloo G. Health, safety and quality concerns of plant-based traditional medicines and herbal remedies. South Afr J Bot. 2020;133:54–62. doi:10.1016/j.sajb.2020.06.031
19. Builders MI. Herbal medicines in African traditional medicine. In: Builders MI, editor. Herbal Medicine. London: IntechOpen; 2019. doi:10.5772/intechopen.80348
20. Musekwa OP, Makhado L, Maphula A, Mabunda JT. How much do we know? Assessing public knowledge, awareness, impact, and awareness guidelines for epilepsy: A systematic review. Open Neurol J. 2020;13(1):79–94. doi:10.2174/1874944502013010794
21. Snouse SJ. ABSTRACT national Epilepsy prevalence in Uganda: a first glimpse. 2020.
22. Sample Size calculator with Slovin’s formula for more precise surveys [Internet]. 2025. Available from: https://surveysparrow.com/blog/sample-size-calculator/.
23. Kaddumukasa M, Kakooza A, Kayima J, et al. Community knowledge of and attitudes toward epilepsy in rural and urban Mukono district, Uganda: a cross-sectional study. Epilepsy Behav. 2016;54:7–11. doi:10.1016/j.yebeh.2015.10.023
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.