Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Community-Driven Development of the Chalerm App: A Mobile Health Application for Chronic Disease Management and Elderly Care in Southern Thailand
Authors Lekapol A, Raksanam B ![]() , Sornkaew W
, Sornkaew W ![]() , Thirarattanasunthon P
, Thirarattanasunthon P ![]() , Nak-ai W
, Nak-ai W ![]() , Bunmalert A, Kraikaew R, Chuaykaew B, Munira L, Mallongi A
, Bunmalert A, Kraikaew R, Chuaykaew B, Munira L, Mallongi A
Received 21 May 2025
Accepted for publication 3 September 2025
Published 24 September 2025 Volume 2025:18 Pages 6115—6125
DOI https://doi.org/10.2147/JMDH.S541792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David C. Mohr
Akkachai Lekapol,1 Buppha Raksanam,2 Wittaya Sornkaew,1 Phiman Thirarattanasunthon,3 Worayuth Nak-ai,4 Abdulloh Bunmalert,1 Rattana Kraikaew,1 Benjawan Chuaykaew,5 Lafi Munira,3 Anwar Mallongi6
1Chang Klang District Public Health Office, Chang Klang, Nakhon Si Thammarat, Thailand; 2Sirindhorn College of Public Health, Trang, Faculty of Public Health and Allied Health Sciences, Praboromarajchanok Institute, Kantang, Trang, Thailand; 3Excellent Center for Public Health Research, School of Public Health, Walailak University, Tha Sala, Nakhon Si Thammarat, Thailand; 4Sirindhorn College of Public Health, Chonburi, Faculty of Public Health and Allied Health Sciences, Praboromarajchanok Institute, Mueang, Chonburi, Thailand; 5Boromarajonani College of Nursing, Trang, Faculty of Nursing, Praboromarajchanok Institute, Mueang, Trang, Thailand; 6Department of Environmental Health, Faculty of Public Health, Hasanuddin University, Makassar, Indonesia
Correspondence: Phiman Thirarattanasunthon, Email [email protected]
Background: Mobile health (mHealth) applications have the potential to improve chronic disease management and healthcare support for older adults. However, their development and contextual adaptation in rural communities remain limited. This study aimed to develop and evaluate the Chalerm App, a mobile health application designed to strengthen chronic disease management, service accessibility, and caregiver support among older adults in Southern Thailand.
Methods: A participatory action research (PAR) design was conducted at a Health Promoting Hospital in Nakhon Si Thammarat Province, Southern Thailand, from March to August 2024. The Chalerm App was developed on Android- and iOS-based platforms through collaboration with software developers, health professionals, and community stakeholders. The study comprised three phases. In Phase 1 (Situation analysis), 223 participants—including 30 elderly individuals, 10 health staff, 7 community leaders, and 176 community members—were recruited using stratified random sampling and participated in interviews and focus groups to identify care gaps. In Phase 2 (Mobile Health Application Development), 30 participants—including 10 health staff, 7 community leaders, and 13 elderly individuals with their caregivers—engaged in co-designing the app. In Phase 3 (Usability and Effectiveness Assessment), 30 elderly individuals and caregivers, recruited via simple random sampling, evaluated the app using a validated researcher-developed tool.
Results: In Phase 1, the main challenges identified included the high prevalence of chronic diseases (hypertension, diabetes, and degenerative joint disease), psychological issues such as loneliness and depression, limited access to healthcare due to geographical and workforce constraints, and low levels of digital literacy. In Phase 2, the Chalerm App was developed with four key functions: (1) Remote Appointment Scheduling, (2) Demographic Information Display, (3) Home Navigation Support, and (4) Health Knowledge Repository. In Phase 3, the evaluation demonstrated that the app significantly exceeded the quality benchmark (p < 0.001), showing notable improvements in elderly healthcare performance, perceptions of the innovation, and the overall quality of care services (p < 0.001).
Conclusion: The Chalerm App improved chronic disease management, service accessibility, and caregiver support for older adults in a rural Thai community. Findings suggest that community-driven mHealth solutions can reduce healthcare inequities in resource-limited settings with potential applicability to similar contexts.
Keywords: caregiver support, chronic disease management, elderly healthcare, health innovation, mobile application
Introduction
The global population is undergoing a rapid demographic transition, characterized by increased longevity and declining fertility, resulting in a growing proportion of older adults. By 2050, approximately one in six individuals worldwide will be aged 65 years or older, compared with one in eleven in 2019.1 This shift is particularly pronounced in Asia, where the pace of population aging often exceeds that of high-income countries.2 In Thailand, older adults accounted for 19.4% of the population in 2023, with projections suggesting this figure will surpass 30% by 2040, classifying the country as a “super-aged” society.3,4
Population aging poses multifaceted challenges to health systems, particularly in low- and middle-income countries (LMICs), where infrastructure and resources are often insufficient. Older adults are at elevated risk for chronic non-communicable diseases (NCDs), frailty, cognitive and sensory impairments, and functional limitations, which increase dependence on formal and informal care networks.5–8 In Southern Thailand, Nakhon Si Thammarat Province reflects national trends: older adults constitute 17.24% of the population, and in Chang Klang District, prevalent conditions include diabetes, hypertension, musculoskeletal disorders, depression, urinary incontinence, and recurrent falls. These conditions compromise quality of life and impose considerable burdens on caregivers and local health services.9–11
Mobile health (mHealth) applications have emerged as promising tools to enhance access to care, promote self-management, and improve communication between patients and healthcare providers. Recent reviews highlight the integration of artificial intelligence (AI) within mHealth platforms, enabling personalized recommendations, predictive alerts, adaptive goal-setting, and improved medical communication.12,13 Such AI-driven features can facilitate timely interventions, support chronic disease management, and enhance clinical decision-making.
Effective mHealth applications typically incorporate several key parameters, including: 1) User interface design – intuitive navigation, readable fonts, culturally appropriate graphics, and accessibility features for sensory or motor limitations. 2) Health monitoring and tracking – integration with wearable devices or manual input to record vital signs, physical activity, medication adherence, and symptoms. 3) Data security and privacy – adherence to ethical and regulatory standards for protecting personal health information. 4) Personalized feedback and decision support – AI-driven recommendations and reminders tailored to individual health profiles. 5) Interoperability – synchronization with electronic health records, wearable devices, and healthcare providers to ensure continuity of care.14–17
Evidence indicates that mHealth interventions incorporating these parameters can improve medication adherence, promote physical activity, enhance chronic disease self-management, reduce hospitalizations, and alleviate caregiver burden.15–18 However, the effectiveness of these applications depends on user engagement, digital literacy, and alignment with local health system policies and workflows.19,20
Community-driven, participatory approaches have been shown to increase the relevance, acceptability, and sustainability of health innovations. Participatory action research (PAR) frameworks enable co-creation of interventions with end-users, local healthcare providers, and policymakers, ensuring cultural appropriateness and responsiveness to community needs.21–23 In Thailand, collaborations among government agencies, academic institutions, and local health networks have initiated digital solutions for elderly care, yet challenges remain in scaling up due to limited digital literacy, suboptimal engagement, and fragmented policy frameworks.24,25
Despite increasing evidence of the benefits of mHealth, few studies have systematically examined AI-enabled mobile applications for community-based elderly care in rural, resource-limited contexts. There is a critical need to integrate digital technologies with participatory, context-sensitive strategies to address the intertwined health and social care needs of older adults.
Therefore, the present study aimed to develop and evaluate the Chalerm App, a mobile health application designed to strengthen chronic disease management, service accessibility, and caregiver support among older adults in the Chalerm Phra Kiat Wat Suan Khan Health Promoting Hospital service area, Chang Klang District, Nakhon Si Thammarat Province. This intervention integrates digital innovation, participatory design, and coordinated care strategies to improve health outcomes, promote functional independence, and enhance the resilience and responsiveness of local health systems.
Methods
An action research design was employed, guided by the Planning, Action, Observation, and Reflection (PAOR) framework,18 conducted from March to August 2024. The study applied a Participatory Action Research (PAR) approach, ensuring active involvement of community members, healthcare personnel, and other stakeholders throughout the design, development, and evaluation of the Chalerm App. A mixed-methods approach integrated quantitative and qualitative data, providing a comprehensive understanding of the intervention’s impact.
Study Population and Sampling
The study comprised three phases with distinct participant groups.
Phase 1 (Situation Analysis)
A total of 223 participants were recruited using stratified random sampling, consisting of 30 elderly individuals, 10 healthcare personnel, 7 community leaders, and 176 residents.Inclusion criteria: individuals involved in or related to elderly health promotion, residents within the service area of Chalermphrakiat Wat Suan Khan Health Promoting Hospital (Chang Klang District, Nakhon Si Thammarat Province), and those aged ≥18 years with literacy in Thai.
Exclusion criteria: unwillingness or inability to participate throughout the study period, absence from the study area during data collection, or diagnosis with a serious communicable disease.
Phase 2 (Application Development)
30 participants—13 elderly individuals, 10 healthcare personnel, and 7 community leaders—were purposively selected to engage in co-design workshops to define the application’s features, content, and interface.Inclusion criteria: representatives from relevant sectors and stakeholders directly engaged in elderly health promotion within Chang Klang District.Exclusion criteria: identical to Phase 1.
Phase 3 (Evaluation)
30 elderly individuals and caregivers from Phases 1 and 2 were purposively selected for pilot testing to ensure diversity in user representation. Sample size estimation using G*Power for paired t-tests (α = 0.05, power = 0.80, effect size = 0.80) indicated a minimum of 27 participants; 30 were included to account for attrition.
Inclusion criteria: participants who had previously taken part in the context analysis or innovation development phases.
Exclusion criteria: identical to Phases 1 and 2.
Participatory Action Research (PAR) Process
The PAR process was fully integrated into the PAOR cycle, ensuring co-creation, reflection, and iterative refinement:
- Planning stage: Stakeholders collaboratively identified health needs, defined app objectives, and determined relevant health content. Workshops engaged participants in mapping community priorities, discussing barriers to elderly care, and suggesting technological solutions. Key decisions, such as IoT device integration and AI-driven notifications, were made jointly with health personnel and elderly representatives.
- Action stage: Participants were actively involved in the co-design of Chalerm App, contributing to the development of the user interface, module architecture, and usability features. An iterative prototyping process was implemented, during which community members provided structured feedback on content clarity, navigation flow, and overall interaction. Internet of Things devices were integrated to capture real-time health indicators (e.g., blood pressure, glucose levels), while artificial intelligence (AI) algorithms were trained on anonymized historical community health data. Both alpha and beta testing cycles incorporated direct user engagement to identify functional limitations and usability concerns.
- Observation stage: Community members assisted in data collection and evaluation, including structured surveys, focus groups, and participatory observation. Elderly users and caregivers reported on usability, satisfaction, and perceived impact, while healthcare personnel provided professional insights on app functionality and health behavior outcomes. Observation sessions were audio- and video-recorded to capture contextual nuances, and iterative feedback informed app refinement.
- Reflection stage: Stakeholders reviewed quantitative and qualitative findings in group reflection sessions. Discussions focused on identifying operational challenges, improving app functionality, and ensuring long-term sustainability. Feedback was incorporated into the final app version and informed recommendations for scaling and replication in other communities.
Mobile Application Development
The Chalerm App was developed using the Flutter cross-platform framework for simultaneous deployment on Android and iOS devices. Firebase backend services enabled real-time data storage, secure authentication, and analytics. A schematic diagram (Figure 1) illustrates the app content flow, covering modules for health education, self-monitoring, reminders, and healthcare communication. IoT devices captured physiological data, transmitted via Bluetooth, Wifi, and integrated with AI-driven alerts for personalized recommendations. Development followed an iterative cycle: initial prototyping, alpha testing, feedback incorporation, and beta testing with representative users. Usability testing employed the System Usability Scale, and functionality testing verified data integrity, synchronization, and alert accuracy.
The “Chalerm App” was developed as a strategic response to address the barriers identified in Phase 1, with a strong emphasis on user-centered design, accessibility, and simplicity. The primary goal was to create an intuitive digital platform to improve the quality and continuity of care for elderly individuals and those with chronic conditions, particularly diabetes and hypertension. The Chalerm App integrates four key features designed to streamline healthcare services and support patient self-care (Figure 1).
- Demographic Information Display: The app provides authorized healthcare providers and caregivers with secure access to essential demographic and medical data, including chronic disease profiles, medication history, and allergy records. This functionality enhances care coordination and facilitates timely decision-making during both routine and emergency care.
- Navigation Support: By integrating GPS technology, the app assists healthcare workers and community health volunteers in efficiently locating patients’ residences, particularly in rural and remote areas. This feature reduces response times during medical visits, promotes proactive follow-up care, and improves the delivery of community-based health services.
- Health Knowledge Repository: The app offers a comprehensive digital library of educational resources, including care guidelines, interactive e-posters, and instructional videos tailored to chronic disease prevention, elderly care, and emergency response. These resources are designed to enhance caregivers’ competencies, promote self-care behaviors, and strengthen health literacy withinthe community.
- Health Knowledge Repository: Offered educational resources, including care guidelines, e-posters, and instructional videos, to support caregivers in both routine and emergency care situations.
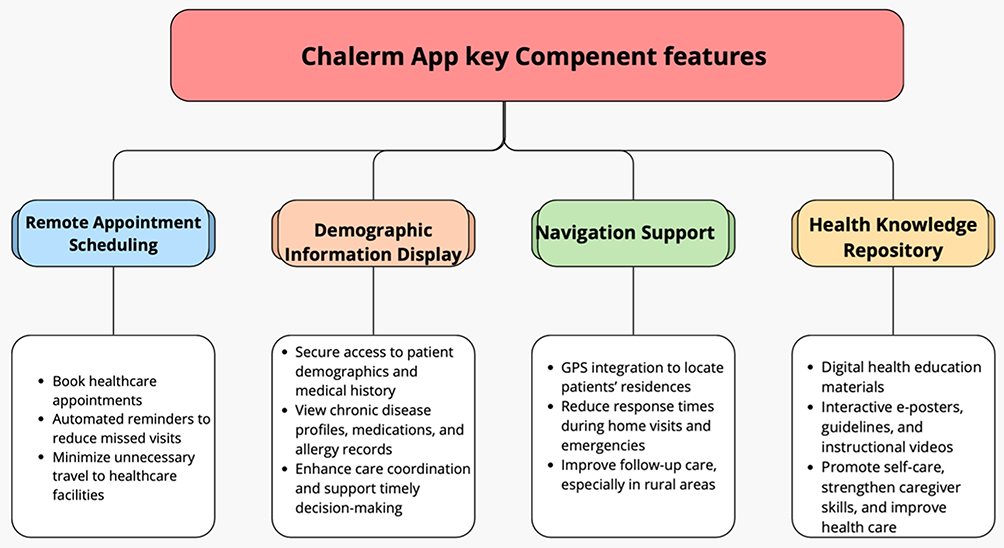 |
Figure 1 Chalerm App key Component framework. |
Research Instruments
The questionnaire consisted of five main sections.
The first section focused on demographic characteristics and included six items that collected information on participants’ gender, age, marital status, occupation, monthly income, and educational level. These demographic data were used to describe the sample characteristics and facilitate the interpretation of the study findings.
The second section assessed the quality of the innovation and consisted of ten items. A five-point Likert scale was employed, and participants were instructed to choose only one response per item. Higher scores indicated a better perceived quality. Specifically, a score of 5 represented “excellent”, 4 denoted “good”, 3 indicated “fairly good”, 2 reflected “fair”, and 1 referred to “needs improvement”.
The third section evaluated participants’ competency in elderly health care and consisted of fifteen items. A three-point rating scale was applied, considering both positive and negative performance perspectives. For positive competency behaviors, scores were assigned as follows: 2 points for frequent performance, 1 point for occasional performance, and 0 points for non-performance. Conversely, for negative competency behaviors, the scoring was reversed: 0 points for frequent performance, 1 point for occasional performance, and 2 points for non-performance. The mean scores derived from this section were used to classify competency levels into three categories:Low competency: 0.00–0.66, Moderate competency: 0.67–1.32, and High competency: 1.33–2.00.
The fourth section measured innovation usability and satisfaction. This section evaluated three core dimensions: ease of use, perceived usefulness, and overall satisfaction with the developed innovation. A five-point Likert scale was applied, where higher scores indicated greater usability and overall satisfaction.
The fifth section consisted of focus group discussions (FGDs), in-depth interviews, and participant observation guidelines, which were used to explore barriers, success factors, and recommendations for developing community-based elderly healthcare innovations.
Content validity was established through an expert review conducted by three specialists, with an Item-Objective Congruence (IOC) index ranging from 0.67 to 1.00. The internal consistency of the questionnaire was found to be acceptable, with a Cronbach’s alpha coefficient of 0.80.
Data Collection
Preliminary stakeholder meetings established shared objectives and engagement strategies. Research assistants were trained to standardize data collection and app guidance. Quantitative data were collected at baseline and post-intervention (20–30 minutes per session) and entered systematically.
Qualitative data were collected using three approaches: focus group discussions (FGDs), in-depth interviews, and participant observation to explore barriers, success factors, and recommendations for developing elderly healthcare innovations in the community. Focus Group Discussions (FGDs): Two FGDs were conducted with 12 stakeholders per group, including healthcare providers, community health volunteers, and local leaders from the Chalermphrakiat Wat Suankhan Subdistrict Health Promoting Hospital service area. A semi-structured guide was used, and discussions lasted 45–60 minutes. Key topics included current elderly healthcare practices, challenges, enablers, and suggestions for improvement. In-depth Interviews: 10 key informants per subdistrict, including health workers and stakeholders, were purposively selected. Semi-structured interviews focused on participants’ experiences, barriers, and recommendations. Each session lasted 30–60 minutes, and data were collected until saturation was achieved. Participant Observation:Participant observation was conducted during elderly healthcare activities to validate findings from FGDs and In-depth Interviews. The researcher recorded detailed field notes, audio recordings (with consent), and photographs. Triangulation across methods enhanced the credibility and trustworthiness of findings.
Data Analysis
Descriptive statistics summarized participant demographics and baseline characteristics. Paired t-tests assessed pre- and post-intervention changes in elderly health competency and satisfaction. One-sample t-tests compared innovation quality scores to predefined benchmarks (mean ≥4.0). Normality assumptions were verified using Q–Q plots. Qualitative data were analyzed using thematic analysis with methodological triangulation (observations, interviews, documents), ensuring credibility and trustworthiness.
Ethical Considerations
Ethical approval was obtained from the Nakhon Si Thammarat Provincial Public Health Office Ethics Committee (Approval No. NSTPH 11/2567, February 27, 2024). The study was conducted in accordance with the Declaration of Helsinki. Confidentiality was maintained through anonymous data collection, and informed written consent was obtained from all participants prior to study involvement.
Results
General Characteristics of the Participants
Situation analysis phase: Among the 223 participants, the majority were female (57.81%). Most participants were aged 60 years and above (38.86%), and more than half were married (51.81%). Regarding educational attainment, 25.91% had completed secondary school. In terms of occupation, the largest group consisted of farmers (20.73%).
Evaluation phase: A total of 30 participants were included in this phase, with the majority being female (60.0%). The highest age distribution was observed in the 66–69 and 70–79 age groups (23.33% each). Most participants were married (30.0%) and had completed elementary education (26.67%). In terms of employment status, 30.66% of the elderly participants were unemployed.
Phase 1: Community-Based Situation Analysis
The situation analysis revealed prevalent chronic conditions, including hypertension, diabetes, and arthritis, requiring continuous monitoring. Limited access to healthcare services, geographic isolation, and provider shortages were critical barriers. Mental health concerns, particularly social isolation, were reported as major challenges. One participant stated, “Sometimes I feel lonely and cannot go to the clinic because it is too far, and nobody can accompany me”. Another caregiver noted, “We often don’t know how to use the health apps; training would help a lot”.
Financial limitations and technological illiteracy hindered adoption of healthcare innovations. These findings highlight the need for simple, contextually appropriate interventions, such as portable blood pressure monitors and medication reminder boxes, supported by caregiver training and community peer networks.
Overall, the elderly health care competency score of participants was generally moderate, with mean scores ranging from 1.05 to 1.48 across 15 domains. The highest scores were observed in three domains: providing regular guidance on elderly care (Mean = 1.48, S.D. = 0.69), developing and disseminating beneficial health information (Mean = 1.48, S.D. = 0.73), and receiving support from relevant agencies for elderly-related projects (Mean = 1.47, S.D. = 0.68). These results suggest that staff were able to deliver ongoing guidance, maintain information-sharing practices, and access institutional support, classifying these competencies as high-level. Conversely, the lowest scores were in creating an environment conducive to elderly living (Mean = 1.05, S.D. = 0.64), consistent follow-up and home visits (Mean = 1.14, S.D. = 0.57), and collaboration with community leaders to support elderly mental health (Mean = 1.08, S.D. = 0.76). This indicates limitations in environmental adaptation, continuity of home-based care, and integration of mental health activities within community networks. Several competencies remained at a moderate level despite being essential for elderly health promotion, including providing consistent health services (Mean = 1.22, S.D. = 0.82), monitoring care for ill elderly individuals (Mean = 1.32, S.D. = 0.42), and organizing health education sessions (Mean = 1.28, S.D. = 0.63). While services were offered, gaps persisted in structured health education and systematic follow-up (Figure 2).
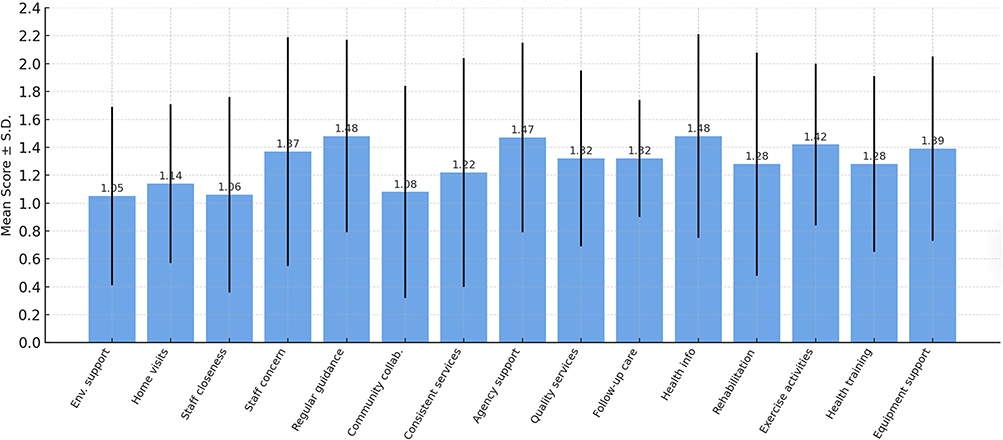 |
Figure 2 Mean scores of competency levels of elderly health care within the catchment area of Chalerm Phrakiat Wat Suan Khan Subdistrict Health Promoting Hospital. |
Phase 2: Development of the Chalerm App
The Chalerm App was developed to address barriers identified in Phase 1, emphasizing user-centered design, accessibility, and simplicity. Its four core functions—Remote Appointment Scheduling, Demographic Information Display, Home Navigation Support, and Health Knowledge Repository—enabled seamless connection between elderly patients, caregivers, healthcare providers, and community health workers. Implementation of the app facilitated efficient, patient-centered management of chronic conditions, particularly diabetes and hypertension, by combining remote service delivery, data accessibility, geolocation navigation, and knowledge-sharing tools. Overall, the Chalerm App supported continuity of care, enhanced self-management among elderly users, and strengthened community-based healthcare systems (Figure 3).
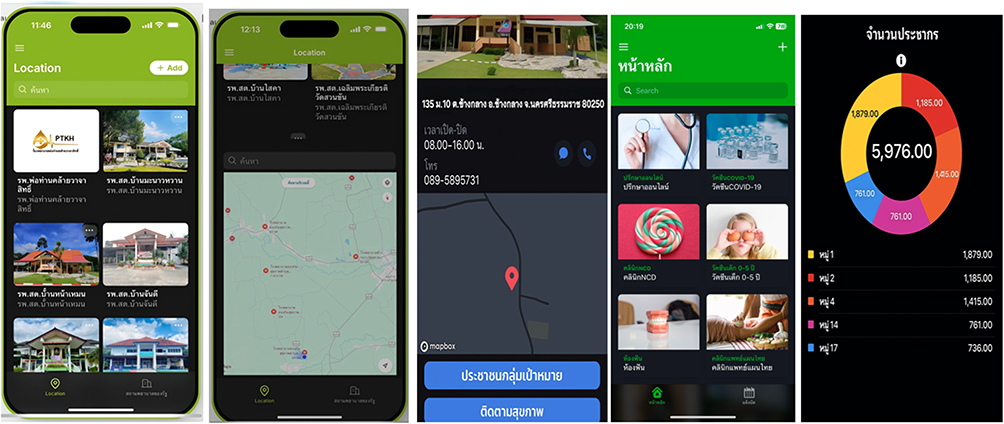 |
Figure 3 Chalerm App, a mobile health application for chronic disease management and elderly care (developed by the local healthcare workers and community ideas). |
The evaluation against predefined criteria demonstrated high quality across multiple dimensions, including content, usability, appearance, utility, and overall performance (Table 1). Effect sizes (Cohen’s d) for overall quality exceeded 1.5, indicating a very large effect. These findings highlight the app’s novelty and its significant contribution to community-based elderly care by seamlessly integrating technology, health knowledge, and accessibility into a single platform.
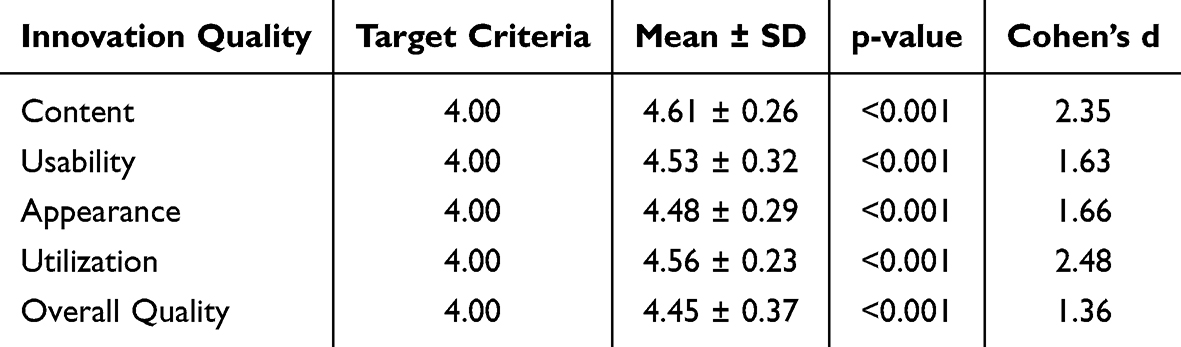 |
Table 1 Evaluation of Chalerm App Quality Against Target Criteria (n = 30) |
Phase 3: Evaluation of Innovation Implementation
Implementation of the Chalerm App resulted in significant improvements in elderly health care performance, user perceptions, and overall quality of care (Table 2). Paired t-tests revealed highly significant differences (p < 0.001) with large effect sizes (Cohen’s d > 0.8). Direct quotes further contextualized the findings: “The app reminds me to take my medicine on time. I feel safer now” and “I can locate patients quickly and check their records efficiently”, illustrating practical benefits in real-life settings.
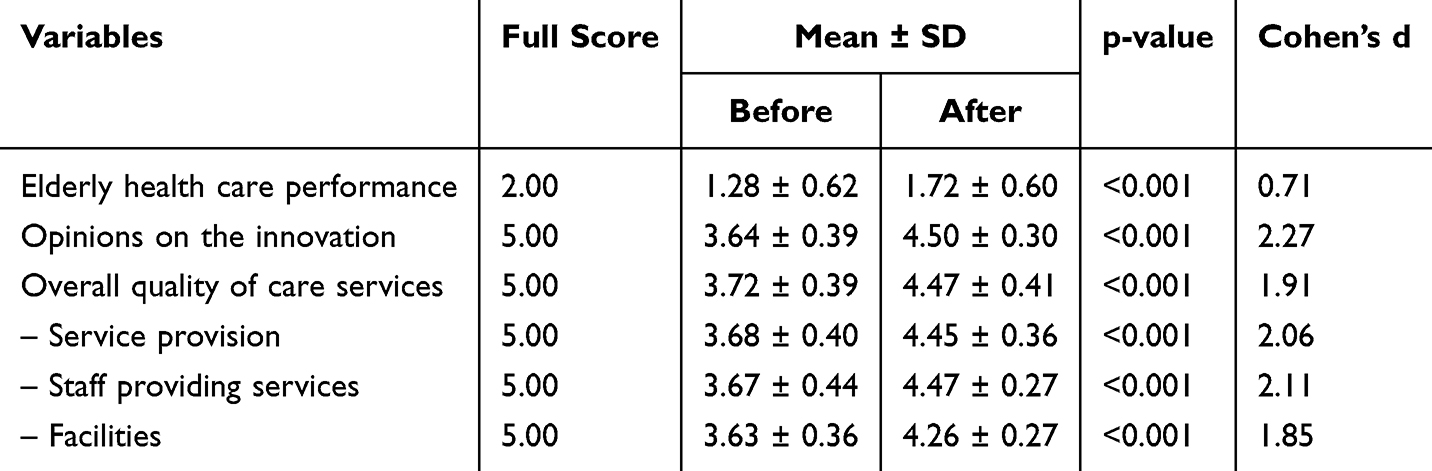 |
Table 2 Comparison of Elderly Care Outcomes Before and After Implementation of Chalerm App (n = 30) |
The results demonstrate that the Chalerm App is a novel, community-based digital intervention integrating user-centered design, healthcare monitoring, navigation, and educational support for elderly care. The app significantly improves healthcare performance, user satisfaction, and overall quality of services while addressing barriers related to access, technology literacy, and caregiver support.
Discussion
The implementation of the Chalerm App demonstrated significant improvements in healthcare accessibility, reduced the burden on local facilities, and enhanced elderly care management in rural Southern Thailand. Real-time health data exchange between users and healthcare professionals facilitated continuous monitoring and personalized interventions, thereby empowering elderly participants to engage in better self-care and improving healthcare responsiveness. These findings support the growing body of evidence highlighting the potential of mobile health (mHealth) solutions as transformative tools for strengthening primary healthcare delivery in resource-limited settings.1,4,10
Elderly participants exhibited notable improvements in several key health behaviors, particularly in medication adherence, regular health monitoring, and physical activity. The app served not only as a service-access platform but also as a behavioral catalyst by providing personalized health prompts, tracking tools, and reminders to encourage positive lifestyle changes. These outcomes are consistent with previous studies demonstrating that digital health interventions enhance patient engagement and improve treatment compliance.8,20 From a technology acceptance perspective, the high level of user engagement observed among elderly participants aligns with Davis’s Technology Acceptance Model, which highlights perceived usefulness and ease of use as critical factors influencing adoption.12,17,24 Furthermore, the success of the app was partly attributed to its age-appropriate interface design and the availability of community-based digital literacy support, as emphasized in prior research.22,25,26
The study highlights important implications for rural healthcare systems, particularly in areas like Chang Klang District, where geographical and logistical barriers limit access to services. Customized digital innovations such as the Chalerm App can play a transformative role in bridging these gaps. To enhance the app’s effectiveness and sustainability, several strategies should be considered, including integrating AI-driven features such as symptom checkers and chatbots to provide real-time decision support, enabling teleconsultation services to connect elderly users with healthcare providers, and applying user-centered design principles to ensure inclusivity and optimize usability.15,23,27–29 Expanding digital literacy initiatives and tailoring app functionality to the needs of older adults could further strengthen long-term engagement and maximize impact.
Despite these promising outcomes, several limitations must be acknowledged. The relatively short implementation period limited the ability to assess long-term behavioral changes, sustainability, and clinical outcomes.13,30 Differences in digital literacy among participants may have influenced levels of engagement, despite efforts to simplify the design.17,24 In addition, reliance on self-reported data introduces the possibility of response and social desirability bias,19,21 and the absence of a control group restricts causal inference regarding the app’s effectiveness.30,31 The study was also conducted within a single subdistrict, which may limit generalizability to other settings.32,33 Finally, technical issues, including inconsistent internet connectivity and device incompatibility, posed challenges to user experience and are common barriers in rural mHealth implementation.34,35
Future research should focus on evaluating the scalability and adaptability of the Chalerm App across diverse rural contexts. Longitudinal studies are needed to examine sustained behavioral change and measure long-term health outcomes, while randomized controlled trials would help establish causal relationships between app usage and health improvements. Integrating Internet of Things (IoT) devices, such as wearable health sensors, could enhance real-time monitoring and support personalized health interventions for elderly populations.31,34,36 In addition, cost-effectiveness analyses are warranted to guide system-level adoption decisions and ensure the long-term sustainability of the intervention within primary care frameworks.
Conclusion
The Chalerm App proved effective in enhancing healthcare accessibility, supporting chronic disease self-management, and strengthening community-based care for older adults in rural Southern Thailand. Its integration into existing health systems, coupled with culturally sensitive design, highlights its potential as a scalable mHealth innovation for underserved settings. However, sustainability will require addressing structural challenges, including digital literacy disparities, infrastructure limitations, and resource constraints. With further refinement, extended evaluation, and potential integration of advanced digital technologies, the Chalerm App could serve as a model for improving elderly care in similar rural and resource-limited communities worldwide.
Acknowledgments
This study was funded by Thailand Science Research and Innovation under the project Thailand Health System Development and Innovation for Elderly Care (Protocol No. 4411569). The authors extend their gratitude to all participants for their valuable contributions.
Disclosure
The authors declare no conflicts of interest with respect to the authorship and/or publication of this article.
References
1. United Nations. World population aging: 1950–2050. New York: United Nations; 2009. Available from: http://www.un.org/esa/population/publications/worldageing19502050.
2. Population and Social Research Institute. Health Dimensions of an Aging Society in Thailand [Internet]. 2023 [cited October 10, 2024]. Available from: https://www.thaihealthreport.com/th/articles_detail.php?id=222.
3. National Economic and Social Development Council. Report on the situation of poverty and income inequality in Thailand by region, 2018. Bangkok: NESDC; 2019.
4. Whaikid P, Piaseu N. The prevalence and factors associated with sarcopenia in Thai older adults: a systematic review and meta-analysis. Int J Nurs Sci. 2024;11:31–45. doi:10.1016/j.ijnss.2023.11.002
5. Ministry of Public Health HDC. Percentage of healthy ageing in Nakhon Si Thammarat Province, fiscal year 2023. Thai: Nakhon Si Thammarat: Provincial Public Health Office; 2023.
6. Somchai B. Development of an application for elderly health care in the community. Community Health Res J. 2019;10(2):123–134.
7. Tangcharoensathien V, Thwin AA, Patcharanarumol W. Implementing mobile health (mHealth) in the context of universal health coverage: a case study of Thailand. WHO South-East Asia J Public Health. 2021;10(2):67–74.
8. Tun SYY, Madanian S, Mirza F. Internet of things (IoT) applications for elderly care: a reflective review. Aging Clin Exp Res. 2021;33(4):855–867. doi:10.1007/s40520-020-01545-9
9. Rosen AB, O’Leary MC, Stroud C, Shekelle PG. Factors influencing the adoption of mobile health applications for self-management among older adults: a systematic review. JMIR Aging. 2020;3(2):e20621.
10. Kelley MM, Powell T, Camara D, et al. Mobile health apps, family caregivers, and care planning: scoping review. J Med Internet Res. 2024;26:e46108. doi:10.2196/46108
11. Fuller-Tyszkiewicz M, Richardson B, Little K, et al. Efficacy of a smartphone app intervention for reducing caregiver stress: randomized controlled trial. JMIR Ment Health. 2020;7:e17541. doi:10.2196/17541
12. Supakit K. The development of health innovations in the community. Community Med J. 2019;14(3):101–115.
13. Wichai W. The development of innovations for elderly care using community context data. Community Health J. 2018;12(1):67–80.
14. Sunthorn T. Developing health applications for the elderly. Med Innov J. 2020;15(4):45–63.
15. Suradet P. Health applications and their role in improving the quality of life for the elderly. Med Innov J. 2021;12(3):45–59.
16. Sharifan F, Farhoudi F, Akbarzadeh F, Sadeghi Bimorgh M, Emadzadeh A. The effect of educating caregivers of the elderly with cognitive disorders using mobile application on the care burden. J Fundam Ment Health. 2021;23(6):437–444.
17. Kim H, Lee SH, Cho NB, You H, Choi T, Kim J. User-dependent usability and feasibility of a swallowing training mHealth app for older adults: mixed methods pilot study. JMIR Mhealth Uhealth. 2020;8(7):e19585. doi:10.2196/19585
18. Kemmis S, McTaggart R. The Action Research Planner.
19. Lee T, Kim S, Park S. Mobile health applications for communication between caregivers of community-dwelling older adults: a scoping review. Geriatr Nurs. 2023;52:172–180. doi:10.1016/j.gerinurse.2023.06.011
20. Marston HR, Musselwhite CB. Improving older people’s lives through digital technology and practices. Gerontol Geriatr Med. 2021;7:23337214211036255. doi:10.1177/23337214211036255
21. Sen K, Prybutok G, Prybutok V. The use of digital technology for social wellbeing reduces social isolation in older adults: a systematic review. SSM Popul Health. 2022;17:101020. doi:10.1016/j.ssmph.2021.101020
22. Whitelaw S, Mamas MA, Topol E, Van Spall HGC. Applications of digital technology in COVID-19 pandemic planning and response. Lancet Digit Health. 2020;2(8):e435–44. doi:10.1016/S2589-7500(20)30142-4
23. Anthony Berauk VL, Murugiah MK, Soh YC, et al. Mobile health applications for caring of older people: review and comparison. Ther Innov Regul Sci. 2018;52(3):374–382. doi:10.1177/2168479017725556
24. Garavand A, Ameri F, Salehi F, Talebi AH, Karbasi Z, Sabahi A. A systematic review of health management mobile applications in COVID-19 pandemic: features, advantages, and disadvantages. Biomed Res Int. 2024;2024:8814869. doi:10.1155/2024/8814869
25. Castro LA, Favela J, García-Peña C, Mora J. In-situ evaluation of a telephone triage mobile application for in-home elderly care. In:
26. Androutsou T, Kouris I, Anastasiou A, et al. A smartphone application designed to engage the elderly in home-based rehabilitation. Front Digit Health. 2020;2:15. doi:10.3389/fdgth.2020.00015
27. Oliveira AE, França R, Rendeiro M, Bernardes E, Dias P, Pereira F. Educational application for mobile devices in elderly health care area: the experience of a public university. In: Global Learn. Association for the Advancement of Computing in Education (AACE); 2015:68–76.
28. Westerman M, Sharma T, Lamnisos D. Aging and global health. In: Handbook of Global Health. Cham: Springer; 2021:73–102.
29. Harte R, Hall T, Glynn L, et al. Enhancing home health mobile phone app usability through general smartphone training: usability and learnability case study. JMIR Hum Factors. 2018;5(2):e18. doi:10.2196/humanfactors.7718
30. Solangi ZA, Solangi YA, Maher ZA. Adoption of IoT-based smart healthcare: an empirical analysis in the context of Pakistan. J Hunan Univ Nat Sci. 2021;48(9):143–153.
31. Sala-Gonzalez M, Perez-Jover V, Guilabert M, Mara JJ. Mobile apps for helping informal caregivers: a systematic review. Int J Environ Res Public Health. 2021;18(4):1702. doi:10.3390/ijerph18041702
32. Vintimilla-Tapia PE, Bravo-Torres JF, Tamariz-Ordóñez PE, et al. Development of a mobile application for the integral care and attention of elderly people. In:
33. Barbosa Neves B, Franz R, Judges R, Beermann C, Baecker R. Can digital technology enhance social connectedness among older adults? A feasibility study. J Appl Gerontol. 2019;38(1):49–72. doi:10.1177/0733464817741369
34. Nuanmeesri S, Poomhiran L. Developing of intelligence walking stick and mobile application for elderly health care using the Internet of Things. Int J Interact Mob Technol. 2020;14(14):4–15. doi:10.3991/ijim.v14i14.14813
35. Chirayus K, Nanthaamornphong A. A systematic mapping review: mobile user interface design guidelines for the elderly with cognitive impairments. In:
36. Yodmai K, Somrongthong R, Nanthamongkolchai S, Suksatan W. Digital technology and health promotion for older adults: a community-based approach. J Aging Res. 2021;2021:6692375.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.