Back to Journals » Infection and Drug Resistance » Volume 19
Community-Based Rapid Testing for HIV in Europe and Central Asia: A Narrative Review of Models, Effectiveness, and Implementation Challenges
Authors Fernàndez-López L ![]()
Received 17 March 2026
Accepted for publication 30 May 2026
Published 16 June 2026 Volume 2026:19 541591
DOI https://doi.org/10.2147/IDR.S541591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yan Li
Laura Fernàndez-López1– 3
1Centre of Epidemiological Studies of HIV/AIDS and STI of Catalonia (CEEISCAT), Health Department, Generalitat de Catalunya, Badalona, Spain; 2Institute for Health Science Research Germans Trias I Pujol (IGTP), Badalona, Spain; 3CIBER of Epidemiology and Public Health (CIBERESP), Madrid, Spain
Correspondence: Laura Fernàndez-López, Centre of Epidemiological Studies of HIV/AIDS and STI of Catalonia (CEEISCAT), Ctra. de Can Ruti, Camí de les Escoles s/n, Badalona, 08916, Spain, Tel +34 93 497 8745, Email [email protected]
Abstract: This narrative review examines the evolution, implementation, and impact of Community-Based HIV Testing (CBT) across Europe and Central Asia (ECA), a region where late diagnosis remains a persistent challenge and key populations continue to face substantial structural, legal, and social barriers to accessing conventional healthcare. This review synthesises evidence from academic studies, surveillance reports, and European initiatives to describe the diverse modalities of CBT, as well as their contribution to earlier diagnosis, improved case-finding among first-time testers, and more timely linkage to care. Across the region, CBT showed higher acceptability and positivity yields than facility-based testing, reaching populations disproportionately affected by HIV, such as men who have sex with men, people who inject drugs, migrants, and sex workers, and supports differentiated, person-centred service delivery aligned with World Health Organization and European Centre for Disease Prevention and Control guidance. Despite clear progress, major implementation gaps persist, driven by restrictive regulatory frameworks, uneven adoption of innovations such as lay provider testing and HIV self-testing, limited integration of community-generated data into national surveillance systems, and structural inequities including stigma, criminalisation, and lack of universal healthcare entitlements. This review also notes the resilience and adaptability of community-based models during recent crises, including COVID-19 and the war in Ukraine. Overall, the evidence demonstrates that CBT is a fundamental component of HIV prevention and diagnosis in ECA. Fully realising its potential requires updated policies that enable task-sharing, integration of multi-disease testing, strong referral pathways, sustainable financing, and formal incorporation of community-generated data into national monitoring frameworks. Strengthening these components is essential to accelerate progress toward the 2030 goal of ending AIDS as a public health threat.
Keywords: differentiated service delivery, key populations, early diagnosis, linkage to care, lay providers, integrated screening, CBVCT, HIV self-testing
Introduction
HIV remains a major public health concern across Europe and Central Asia (ECA) despite substantial advancements in antiretroviral therapy (ART) and prevention.1–3 Persistent gaps in early diagnosis and equitable access to testing remain central obstacles to achieving regional and global HIV elimination targets.1–6 Individuals and communities most affected by HIV often face structural, social, and legal barriers that limit engagement with conventional, facility-based health services.2–4 Addressing these barriers is essential to reduce late diagnosis, stop onward transmission, and ensure timely linkage to prevention and care.
In this context, Community-Based Testing (CBT), also known as Community-Based Voluntary Counselling and Testing (CBVCT), has emerged as a key component of differentiated service delivery models aimed at closing these gaps.3,7,8 By offering testing outside traditional clinical settings, often in “low-threshold”, peer-led environments such as Checkpoints, CBT provides a flexible, inclusive, and stigma-reducing alternative that has demonstrated high acceptance among underserved groups.3,7,9 These approaches align with global recommendations emphasising decentralisation, integration with multi-disease screening (including viral hepatitis and Sexually Transmitted Infections (STIs)), and task sharing with trained lay providers.1,2,7 Beyond enhancing accessibility and normalising testing, CBT enhances community trust, contributes to earlier diagnosis, and improves linkage to care.1,10
Over the past decade, CBT in ECA has evolved substantially, incorporating a wide range of service models and technological innovations, including rapid tests, HIV Self-Testing (HIVST) and self-sampling, mobile and outreach services, and integrated screening for HIV, viral hepatitis, and STIs. At the same time, implementation has remained unequal across the region, reflecting differences in epidemiological patterns, legal frameworks, health system organisation, and the extent to which communities are empowered to lead service delivery. As the 2030 targets approach there is a clear need to synthesise current evidence on how CBT contributes to HIV responses in ECA, as well as to identify remaining gaps and implementation challenges.
The objective of this narrative review is to critically examine the current landscape of CBT in ECA by: i) describing the main models and modalities currently implemented in the region; ii) summarising evidence on their effectiveness in reaching key populations, identifying first-time testers, supporting early diagnosis and facilitating linkage to care; iii) and analysing structural, regulatory, and operational barriers that continue to limit the scale-up and integration of CBT into national strategies. By consolidating evidence from academic literature, surveillance data, and European initiatives, this review aims to clarify the contribution of CBT to regional HIV responses and to inform policy and programme development needed to accelerate progress toward ending AIDS as a public health threat by 2030.
Methodology of the Review
This narrative review synthesised academic and grey literature describing community-based rapid HIV testing in ECA between 2012 and 2025. Geographical scope followed the WHO/UNAIDS definition of the ECA region.
Evidence was identified through structured searches of PubMed/MEDLINE, Embase, Scopus, Web of Science, and repositories of major institutional stakeholders, including the European Centre for Disease Prevention and Control (ECDC), UNAIDS, and World Health Organization (WHO). Additional sources included conference materials and documents produced by community-based organisations as well as websites of European initiatives and projects. The search terms combined concepts related to HIV, rapid or point-of-care testing, community-based services, and ECA. The representative academic search string used was: (“HIV” OR “human immunodeficiency virus”) AND (“rapid testing” OR “point-of-care” OR “POC”) AND (“community-based” OR “community health services”) AND (Europe OR “Central Asia” OR Armenia OR Azerbaijan OR Georgia OR Kazakhstan OR Kyrgyzstan OR Tajikistan OR Turkmenistan OR Uzbekistan).
Documents were included if they reported empirical findings or relevant contextual information regarding community-based rapid or point-of-care HIV testing in the ECA region during the study period. The exclusion criteria included studies unrelated to HIV testing and analyses limited exclusively to hospital-based testing, opinion pieces, and media reports.
The academic search identified 91 articles, of which 15 were excluded because they did not meet defined time period, did not focus on HIV testing, or were conducted outside the ECA region. The grey literature yielded 53 documents: 28 were guidelines, reports, recommendations, or policy briefs from UNAIDS, WHO, and ECDC, and 25 were conference abstracts, articles published in non-peer-reviewed journals, and reports or presentations from projects or NGO websites.
In total, 129 documents were considered for the narrative review. In addition, 14 further documents (12 academic papers and 2 guidelines/recommendations) were added as references when discussing topics not directly linked to the main search, such us the effectiveness of early diagnosis and ART, POC tests, and the COVID-19 pandemic and war in Ukraine.
Findings were synthesised narratively, with attention paid to patterns across service delivery approaches, populations served, regional differences, and structural facilitators and barriers. Quantitative data were summarised descriptively and no meta-analysis was conducted. Grey literature (apart from reports, guidelines/recommendations from WHO, ECDC, UNAIDS) was used mainly to expose examples or particular cases of community-based testing models.
Background and Regional Context
Epidemiology and the Challenge of Late Diagnosis
Epidemiological trends across ECA highlight the need for more tailored CBT approaches. The distribution of new HIV diagnoses differs by subregion, affecting the key population groups in a different way.
In Western Europe, Men who have Sex with Men (MSM) remain the group most affected by new HIV diagnoses and represent the largest share of reported cases.1,3,11 Overall, MSM account for a stable proportion of reported transmission modes across the wider region (26%), yet they continue to dominate new infections in this sub-region.1,3,11
In contrast, in Eastern Europe and Central Asia (EECA), the epidemic is increasingly driven by heterosexual transmission and disproportionally affects People Who Inject Drugs (PWID) and their sexual partners.1,3,11 In addition, increasing numbers of infections among sex workers and their clients have been documented, particularly in EECA.1,2,4,9,12
Across the European Union/European Economic Area (EU/EEA), migrants account for more than half of new HIV diagnoses, and face significant structural barriers such as insecure legal status, restricted access to services, and fear of criminalisation or deportation.1
Overall, these regional patterns reflect persistent gaps in prevention coverage, testing uptake, and access to health services among key and marginalized populations.
Late HIV diagnosis remains one of the most persistent challenges in ECA. More than half of individuals newly diagnosed with HIV across the WHO European Region (52.4%) are identified at a late stage, typically defined as a CD4 count below 350 cells/mm3 or the presence of an AIDS-defining event.1,3,4,12 Recent surveillance data indicates that approximately one third present with advanced HIV disease (33.6%), reflecting gaps in timely testing and access to prevention services.1 Substantial geographical differences persist: late diagnosis rates are highest in Eastern and Central subregions and remain significant even in Western Europe and the EU/EEA.1
Some groups are disproportionately affected. Older adults (≥50 years) consistently report the highest levels of late presentation, with approximately two-thirds diagnosed at a late stage.1,13 Heterosexual individuals, particularly men, also show elevated rates, and migrants from sub-Saharan Africa and Asia, along with PWID, continue to be overrepresented among late presenters.1,3,12 In contrast, MSM exhibit the lowest proportion of late diagnoses, likely reflecting higher risk perception and more frequent testing behaviours.1,3
Late diagnosis is associated with increased morbidity, mortality, delayed treatment initiation and an increased risk of onward transmission.14 Evidence indicates that CBT plays an important role in mitigating this burden, with individuals tested in community settings being more often diagnosed earlier and with higher median CD4 counts than those diagnosed in traditional healthcare facilities.7,9,15,16 This suggests that CBT can help reach populations who might otherwise be tested only after symptom onset or disease progression.
Global and Regional Strategic Frameworks
CBT remains a central pillar of the international HIV response as efforts transition to the 2025 milestones toward the 2030 goal of ending AIDS as a public health threat.17 Beyond achieving the 95-95-95 targets, global strategies increasingly emphasise the UNAIDS 30-80-60 commitments, which mandates that 30% of testing and treatment services and 80% of prevention programs for key populations are led by the community.17,18
The WHO strongly recommends community-based HIV testing services, highlighting their important role in reaching populations underserved by conventional health systems and ensuring a timely linkage to prevention, care, and treatment.7,19–21 The framework of differentiated service delivery, central to WHO guidance, adapts testing approaches to population needs and local contexts, emphasizing several strategic components:7
- Task sharing, which authorises trained lay providers and peers to independently perform rapid diagnostic tests, helping extend testing beyond clinical settings.
- Technological innovations, including HIVST and network-based approaches, to reach individuals less likely to access traditional healthcare services.
- Integrated, person‑centred care, promoting multiplex testing (eg dual HIV/syphilis), and combined screening for HBV, HCV, STIs, and tuberculosis.
- Adherence to the 5 Cs of HIV testing services: Consent, Confidentiality, Counselling, Correct results, and Connection to care.
Within the WHO European Region, the Regional Action Plans for HIV, viral hepatitis, and STIs (2022–2030) provide a unified framework that positions community-based services as essential to ending epidemics.22 The ECDC’s recommendations are aligned with those of the WHO, advocating for the integration of community-led and community-based testing into national health systems, the removal of regulatory restrictions on who may perform HIV tests, and the scaling-up of diversified testing approaches.12,14,23
Recent policy developments, including the European Standards of HIV Prevention and Care (2025), set a higher bar for implementation efforts.13 These standards recommends that all national strategies include CBT for at least one key population and incorporate self-testing and self-sampling.13 They also prioritise linkage to care, recommending that a confirmatory test be offered within five working days of a reactive result.13
Trends in Coverage and Implementation in Europe and Central Asia
CBT has evolved into an important pillar of national HIV strategies, accounting for an increasing proportion of new diagnoses among populations disproportionately affected by HIV, including MSM, migrants, sex workers, PWID, and transgender individuals.3,4,24 Data from the COBATEST network and other regional initiatives indicates that a substantial percentage of HIV tests are now delivered outside traditional clinical settings through community centres, mobile units, and outreach programs.3,25,26
According to the recent ECDC and WHO monitoring, the availability of CBT has increased significantly over the past decade. The percentage of countries in the WHO European Region providing community testing has increased from 35% in 2018 to 51% in 2022, but it has not improved since then, with the same number of countries reporting CBT in 2024.3,4,12 Coverage within the EU/EEA is even higher, with 86% of countries reporting community-provided testing.3,12 By 2024, 44 countries in the wider region had implemented some form of CBT, and in several settings community-led approaches were growing faster than clinic-based provider-initiated testing.3,4
Despite these encouraging trends, implementation remains highly heterogeneous. CBT is widely established in Western and Southern Europe, but it remains severely underutilised in Eastern Europe, where only five countries reported providing such services as of 2022.3,4 Furthermore, while CBT is increasingly available, traditional clinic-based interventions still maintain a higher overall coverage and are currently the most implemented testing modality across ECA.4
Although there is growing political commitment to diversified testing strategies, including self-testing and lay provider testing, most testing in the region still takes place in traditional clinics.
Key Implementation Gaps in Europe and Central Asia
Despite clear progress in expanding CBT across ECA, major implementation gaps continue to limit its full-scale implementation and effectiveness.2,4,13
A key barrier is the slow adaptation of the national HIV testing guidelines. Nearly half of the national policy documents are now more than five years old, and many no reflect innovations, such as lay provider testing, indicator-condition testing, HIVST, or integrated screening for viral hepatitis and other STIs.2,4,12 As a result, national frameworks frequently remain behind WHO recommendations, which have supported task-sharing and lay provider testing since 2015 as essential strategies for improving access among underserved populations.27
Legal and regulatory constraints have limited the expansion of community-led models. Thirty-three countries across the region still restrict HIV test administration to medical personnel, and in the EU/EEA specifically, 22 countries prohibit trained lay providers from conducting rapid tests independently.4,12 These restrictions significantly limit the scale-up of peer-driven services, which is crucial for engaging populations that are unlikely to use traditional healthcare facilities. Although many countries now allow lay providers to administer tests, the number remains substantially lower than those authorising CBT performed by medical professionals (in the EU/EEA, 20 countries versus 25, respectively), highlighting a persistent implementation gap.12
A punitive legal environment can worsen these challenges. The criminalisation of HIV transmission, sex work, and drug use discourage key populations from accessing testing and prevention services because of fear of legal repercussions, stigma, and discrimination. These structural barriers reduce CBT uptake, contribute to late diagnosis, and perpetuate gaps in linkage to care.4,12
Overall, while CBT is now widely recognised as a critical component of HIV testing strategies in the region, its potential remains constrained by regulatory obstacles, policy inertia, and stark regional differences in implementation. Addressing these gaps through updated national guidelines, the removal of legal restrictions on lay provider testing, and reforms to reduce the impact of punitive laws will be essential to harness the full benefits of community-based approaches and advance progress toward ending AIDS as a public health threat by 2030.12,17,18,22
Models and Modalities of Community-Based Testing
In ECA, the landscape of HIV testing outside traditional medical environments is characterised by a variety of terminologies and operational modalities designed to reach key populations and overcome barriers to care.
Terminology and Definitions
The terminology used to describe testing delivered in community settings has evolved significantly. Early initiatives focused mainly on offering voluntary counselling and testing outside hospitals or clinics. Over time, as services diversified and community leadership became increasingly important, the vocabulary evolved to reflect new operational realities, levels of community governance, and technological advances in testing.
Community-Based Voluntary Counselling and Testing (CBVCT) was one of the earliest standardised terms. Before 2010, definitions varied widely across countries. A regional consensus, developed during the HIV-COBATEST project and published in International Journal of STD & AIDS (2015), established CBVCT as
Any programme or service that offers HIV counselling and testing on a voluntary basis outside formal health facilities, and that has been designed to target specific groups of the population most at risk and is clearly adapted for and accessible to those communities. Moreover, these services should ensure the active participation of the community with the involvement of community representatives either in planning or implementing HIV testing interventions and strategies.15
This definition became a key reference for European practice and remained one of the most standardised terms for describing community-delivered HIV testing.
As testing technologies and community-led models advanced, organisations such as the COBATEST Network expanded the definition. The updated formulation includes testing for STIs and viral hepatitis, incorporates a wider range of testing methods, and emphasises accessibility, adaptation to community needs, and meaningful community participation (Table 1).28
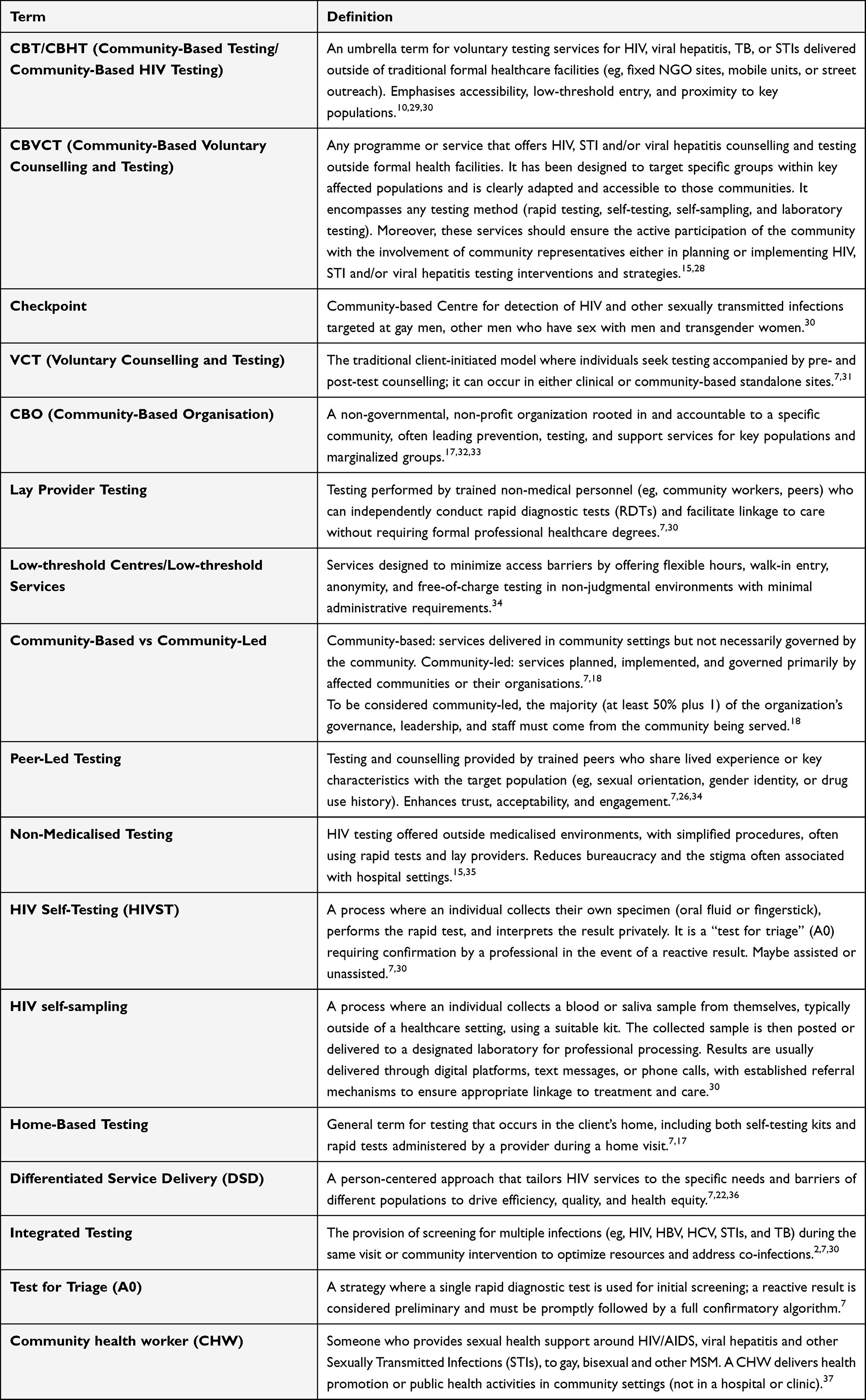 |
Table 1 Definitions of Key Terms |
Over time, new terms have been adopted to describe different models, including community-led services, peer-led testing, lay provider testing, low-threshold services, and home-based testing. The expansion of self-testing and self-sampling has diversified the conceptual landscape. Today, CBT is understood not as a single model but as a range of approaches that prioritise accessibility, person-centred design, and reducing health inequities. The terminologies identified are presented in Table 1.
Heterogeneity in Community-Testing Models
CBT services in ECA differ widely in their organisation, staffing models, size, target population, delivery model, setting, and level of integration with formal health systems.15 Rather than following a single model, these services range from highly medicalized structures to fully community-led approaches.15 This variation reflects not only differences in national legal frameworks that determine who can perform HIV testing, but also the level of medical involvement within each service.12,14,15 Centres offering comprehensive check-ups, extended infection screening, or confirmatory testing require more specialised personnel and operate more like community clinics, whereas others maintain a low-threshold, community-centred model focused on rapid testing alone.15,29,30,36,38 Figure 1 shows a conceptual diagram of the different models, mapped according to their degree of medicalisation and community involvement.
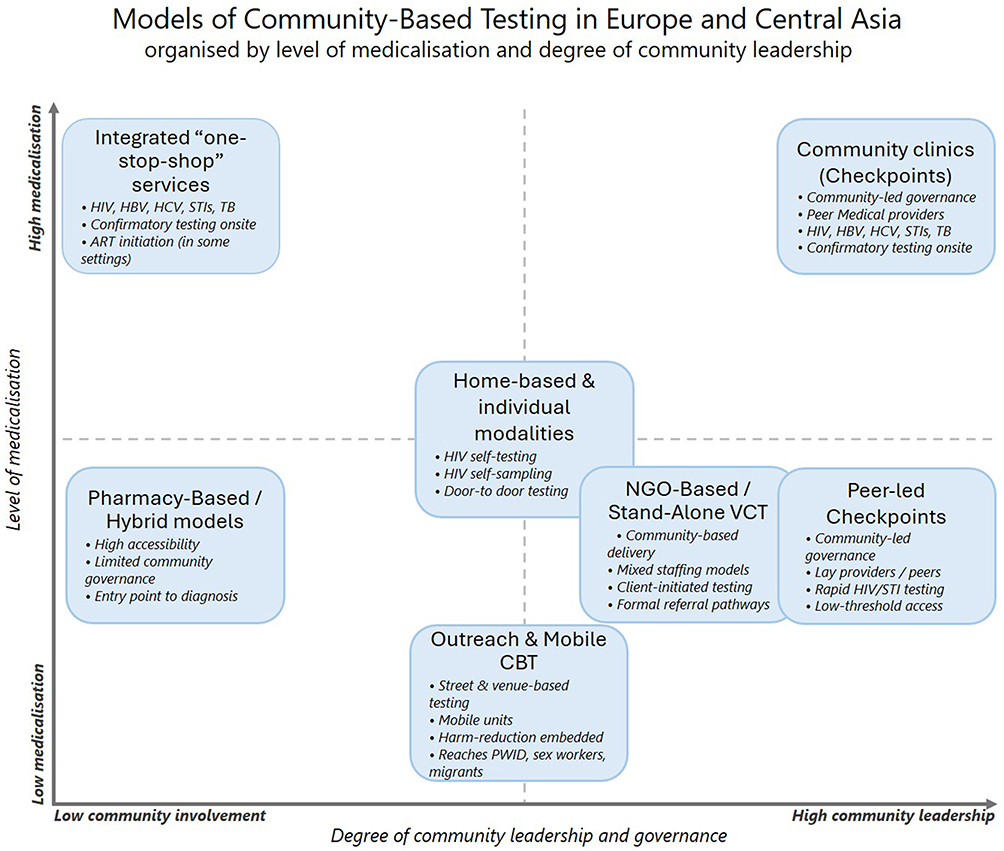 |
Figure 1 Conceptual diagram of models of Community-Based Testing in Europe and Central Asia, organised by level of medicalisation and degree of community leadership. |
Typologies of Services
Following the definition of key terms, Table 2 presents a structured classification of CBT services in two dimensions: the delivery model and service setting. This framework differentiated fixed-site models from outreach and mobile approaches, as well as home-based and individual modalities and more integrated or network-driven models, capturing the operational diversity of CBT and highlighting how each modality adapts to the needs and contexts of key populations.
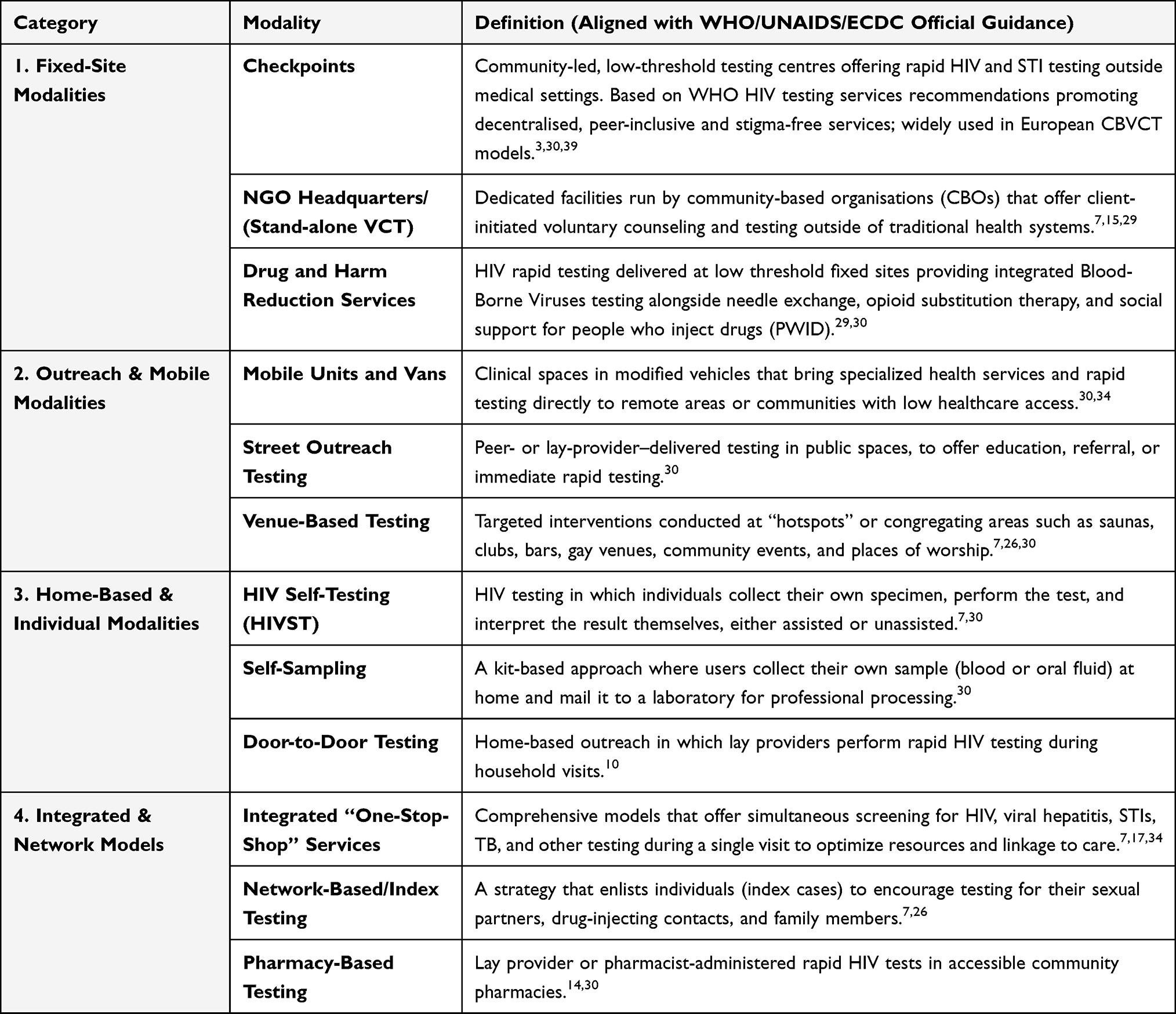 |
Table 2 Classification of the Different Modalities of CBT According to the Delivery Model and the Service Setting |
Technologies Enabling Community-Based Rapid Testing
Rapid Testing Technologies
Rapid diagnostic tests (RDTs) are the core technology for CBT, specifically designed for ease of use and immediate results.7,24,40 These immunoassays provide results in less than 30 min using non-invasive specimen collection, such as oral fluid or finger-stick capillary blood.7,41 Most RDTs currently implemented are either third-generation (detecting antibodies) or fourth-generation (detecting both antibodies and the p24 antigen), the latter of which can identify more recent infections.7,42,43 The WHO recommends that RDTs used in these settings achieve at least 99% sensitivity and 98% specificity.7 As they do not require a clinical laboratory or venipuncture, these tests are highly suitable for task sharing with trained lay providers and peer educators.4,7,24,40,44
In community-based models, a single RDT typically serves as a “Test for Triage” (A0), and a reactive result is considered preliminary and must always be followed by confirmatory testing using the full national testing algorithm.7,42
Multiplex technologies now enable combined testing for HIV and syphilis or integrated screening for hepatitis B and C, supporting more routine testing and better use of resources.7,8,34,45
Beyond rapid testing alone, more medicalised community-based models, often supported by doctors, nurses, or formal links with hospitals, offer a wider set of clinical services tailored to the needs of key populations.15 Many of these services include nucleic acid amplification testing for asymptomatic pharyngeal and rectal gonorrhoea and chlamydia, infections that are often missed with standard urethral screening.38 In high-prevalence settings, these “one-stop-shop” sites may also provide on-site CD4 cell count and viral load monitoring to allow for rapid ART initiation and monitor treatment effectiveness.34 Furthermore, some medicalised initiatives normalise HIV screening by integrating it into general health checks, including measurements of blood pressure, body mass index, and blood glucose.7,46 This broader approach not only helps identifies underlying non-communicable diseases, but also improves the detection of co-infections such as tuberculosis, improving overall health outcomes for marginalised groups who tend to avoid traditional clinical settings.34
Self-Testing
HIVST has become an important innovation to broaden access to HIV diagnosis by allowing individuals to test privately and at their convenience.2,7 Its implementation has grown significantly in the WHO European region, with the number of countries reporting HIVST availability increasing from 17 in 2018 to 31 in 2022.4,12 While HIVST empowers users and reduces structural barriers, a reactive self-test result is not a definitive diagnosis and requires confirmation by a trained provider.2,7 Self-sampling approaches, in which individuals collect samples at home and send them to a laboratory, offer an additional option for those seeking privacy while still ensuring laboratory-validated results.9
By 2025, CBT services have become key settings for implementing these technologies, moving beyond on-site testing to provide broader support for self-managed HIV care.3,13 CBT programmes contribute to the effective roll-out of HIVST through several mechanisms. First, CBT sites act as complementary access points, offering trusted, non-medicalised environments in which individuals who avoid conventional healthcare can receive hands-on support on using self-testing or home-sampling kits.3,13 CBT organisations are increasingly taking the lead in digital HIVST by combining online kit distribution with social media outreach, virtual counselling, and telehealth support.7,47–49 Programmes such as Moldova’s MyLife+ app or Milan’s EasyTest integrate ordering, result reporting, and peer-based virtual support within a single platform, improving accessibility for people facing legal, social, or geographic barriers.47,50
Reaching populations traditionally missed by health systems has become central to CBT strategies. By using approaches like vending machines in gay saunas, mobile outreach for sex workers, and integration within harm-reduction services, CBT providers broaden access to HIVST for first-time testers, people with irregular working hours, and those who rarely use health facilities.26,51 Finally, robust referral and linkage pathways remain a core responsibility for CBT services, ensuring that people who self-test, particularly those with reactive results, are supported and guided to confirmatory appointments.7,13
By combining the privacy of self-testing with the trust and navigation support of CBT, these integrated models are essential for closing the remaining testing gaps and achieving the 2030 goal of ending the AIDS epidemic.1,2
Effectiveness of Community-Based Testing in Europe and Central Asia
Figure 2 summarize the main effectivity data of CBT in ECA detailed in this section.
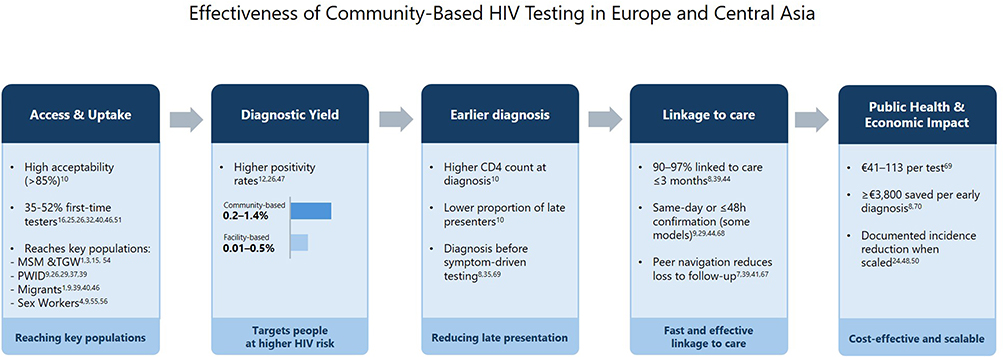 |
Figure 2 Summary figure on Effectiveness of Community-Based HIV testing in Europe and Central Asia. |
Uptake, Positivity Yield, Identification of First-Time Testers
Across ECA, CBT has proven to be an acceptable and effective strategy for reaching populations at high risk who may avoid traditional healthcare settings.29,52 Global systematic reviews report acceptance rates close to or above 85% for community-based approaches, including rapid testing, index testing, and self-testing.10
Evidence from across the region shows that HIV positivity rates in community-based settings (0.2–1.4%) are higher than in traditional healthcare settings (0.01–0.5%), suggesting greater access to populations at higher risk and with lower healthcare engagement.12,26,53 The “checkpoint” model has consistently shown high diagnostic yield and substantial public health impact, with significant declines in HIV incidence in cities where it has been fully implemented, such as the 62% reduction documented by BCN Checkpoint in Barcelona.24,54–56
CBT is particularly successful in identifying first-time testers, a critical step in reducing the undiagnosed fraction.26,46 Standardised data from the COBATEST Network show that 35–36% of individuals tested in community settings had never previously taken an HIV test.25,26,30,57 National and local projects reinforce this pattern: a demonstration project in Italy reported 45.2% first-time testers, while a pilot in Rotterdam achieved a rate of 52.3%.46,52 Targeted outreach activities, such as those conducted in sex-work venues, migrant centres, or nightlife spaces, continue to reach meaningful proportions of individuals testing for the first time.16,46 Detecting HIV among first-time testers, even at relatively low positivity rates (eg 0.6% in nationwide Italian initiatives), represents an important step in reducing the number of undiagnosed infections and reducing onward transmission.52
Visibility, accessibility, and anonymity are key drivers of uptake. Street-based testing in urban areas has been shown to attract people with no prior testing experience simply due to the high visibility and convenience of the service.58 Similarly, outreach testing on university campuses or in multicultural neighbourhoods reaches younger people, heterosexual men and women, and people with low perceived risk, groups that are frequently under-represented in facility-based testing data.9,59
Reaching Key Populations
CBT plays a key role in reaching populations disproportionately affected by HIV in ECA, helping to overcome structural, social, and legal barriers that limit access to traditional healthcare settings.
Among MSM and transgender women, peer-led community services, often based on the “Checkpoint” model, are the most widespread approach in Europe, with around 80% of community services specifically targeting MSM, according to a survey published in 2015.15 These queer-affirming spaces reduce stigma, enhance trust, and effectively reach individuals with low testing patterns or higher risk behaviours, such as those frequenting saunas or sex-on-premises venues.1,3,15,35
Outreach-based CBT, delivered through mobile units, street-based teams and peer navigation models, is vital for engaging PWID, who often experience socially marginalisation and limited contact with formal healthcare.9,26,34 Several examples showed high acceptability and feasibility of HIV and HCV rapid testing integration into harm-reduction settings (needle-syringe programmes, opioid agonist therapy units, or “one-stop-shop” centres)29,34,44 These integrated services support immediate screening and facilitate trusted relationships that are crucial for linkage to care.34
Similarly, sex workers benefit from CBT approaches delivered directly in workplaces, such as brothels, or through dedicated mobile outreach, which help overcome the effects of criminalisation and severe stigma.4,60,61 Evidence shows that up to one in four sex workers reached through brothel-based testing are first-time testers, underscoring the importance of providing services in their own environments.9 Further expansion of tailored services remains a priority in EECA, where HIV transmission among sex workers and their clients has increased substantially over the past decade.3,4,17,61
Culturally and linguistically adapted CBT models play an important role in addressing the legal, social and language barriers often faced by migrants in formal healthcare systems.1,3,62,63 Interventions such as Rotterdam’s general health-check approach and mobile outreach with cultural mediators at migrant support centres have shown high uptake, with substantial proportions of first-time testers.1,9,34,46,52 However, despite promising case-finding, linkage to care remains a persistent challenge in contexts where undocumented individuals face restrictions on ART eligibility.4,64,65
Linkage to Care and Referral Pathways
Prompt and effective linkage to care is a core measure of effectiveness in CBT, ensuring that individuals with a reactive result receive confirmatory testing and treatment initiation in a timely manner.7,9,12,66 Across the WHO European Region, linkage to care is generally defined as attending a clinical service within three months of diagnosis, a standard used for public health monitoring in Europe.1,4 In the EU/EEA, around 97% of people diagnosed with HIV meet this criterion, indicating strong overall performance but masking persistent disparities among marginalised groups such as PWID and undocumented migrants.1,3,7
Across ECA, many CBT services have established formal referral pathways with infectious disease clinics, reducing delays and preventing loss to follow-up. Programmes such as Milan’s EasyTest or the Fast-Track City initiative in Turin have reported very high levels of linkage to care, enabled by facilitated appointments, simplified administrative processes, and short waiting times.8,50 Integrated “one-stop-shop” models in settings such as Minsk, Bălți and Brighton further strengthen this process by offering blood sampling, confirmatory testing and, in some contexts, same-day ART initiation directly within low-threshold community environments, an approach shown to support faster viral suppression than conventional rapid-start protocols.34,67–71
Peer navigation is a central component of these systems. Trained peers accompany clients to initial appointments, help them navigate administrative procedures, and build the trust required for marginalised groups, such as PWID, migrants, or sex workers, to engage in care.7,72 Initiatives such as Lisbon’s REACH U project and the Positive Movement in Belarus illustrate how peer-led accompaniment improves engagement and retention in care.34 CBT referral systems are increasingly supported by digital platforms, such us Moldova’s MyLife+ and Ukraine’s Syrex Cloud, which use QR codes, appointment tracking, and real-time feedback to coordinate linkages and support continuity of care.47
Some CBT centres have also incorporated point-of-care confirmatory diagnostics, further shortening the time between screening and care. The BCN Checkpoint in Barcelona uses rapid PCR to confirm HIV diagnoses within approximately 90 minutes, while the EasyTest in Milan typically provides confirmatory results within 24 hours and specialist consultations within 48 hours.9,29,50,73 These accelerated approaches help minimise the risk of disengagement after a reactive test result, however, their implementation remains limited to Western Europe, with no reported adoption in EECA.22 The scale-up of integrated multi-disease testing, covering HIV, HBV, HCV, STIs, and TB in a single visit, improves efficiency, facilitates earlier detection of co-infections, and is consistent with the 2025 European Standards, which stress the importance of strong referral pathways for HIV treatment and prevention, including PrEP and harm-reduction services.1,13,17,22
Enhanced referral pathways are essential for engaging individuals who might otherwise be lost to follow-up shortly after receiving a reactive result, particularly those facing stigma, housing insecurity, or high mobility. Peer navigation, personalised follow-up, and trust-based relationships rooted in the community setting contribute to more rapid ART initiation and earlier viral suppression.2,7,46
Economic Benefits and Sustainability
Early diagnosis through CBT is highly cost-effective and helps reduce long-term healthcare costs.8,42,74 Early diagnosis, with CD4 counts above 350 or 500 cells/mm3, is associated with annual care costs several thousand euros lower than those for people diagnosed at later stages, who require intensive management of advanced disease and opportunistic infections.8,75
Programmes such as the Turin Fast-Track City initiative have reported savings of more than 3800€ per individual diagnosed early, highlighting the cost-effectiveness of proactive community-based approaches.8,75 Similar economic evaluations across multiple European cities report costs per reactive test ranging from 1966€ to 9065€, among the lowest documented globally, and routine CBT costs of 41€-113€ per test, figures that compare favourably with many facility-based approaches.74
Decentralised testing also reduces the burden on hospitals and laboratories, particularly for the large proportion of negative results that require no additional clinical follow-up.10,42 Integrated multi-disease screening (HIV, HBV, HCV, STIs, TB) further optimises resources and helps prevent morbidity associated with untreated co-infections.7,17
Long-term sustainability continues to depend on a transition from donor-funded models to stable national financing. Social contracting, where governments fund community-based organisations to deliver testing and outreach, has proven effective but it still applied at a limited scale.8,17,18,22,74 Scaling-up peer-led and lay-provider models can reduce costs and increase reach and acceptability.7
Barriers, Challenges, and Structural Factors
Legal and Policy Barriers
Legal and policy frameworks remain among the most significant obstacles to the implementation of CBT across the ECA. Many countries still restrict HIV testing to medical or nursing staff, limiting the scale-up of lay-provider testing despite WHO recommendations since 2015 to demedicalise diagnostics and expand the role of trained non-medical staff.12,14 Regulations for other infections are even more restrictive, with the majority of EU/EEA countries requiring that Hepatitis B and C tests be performed by healthcare professionals, thereby limiting the implementation of integrated multi-disease screening within community settings.12 Evidence from countries that have removed these barriers confirms a positive impact on public health.76
This challenge is exacerbate by outdated national testing guidelines, as nearly half of the region’s policies are over five years old, and many countries report no plans to update them.12 As a result, national framework often lack provisions for key innovations, including HIVST, indicator-condition testing, and integrated screening for HBV, HCV and STIs.3,12
Marked regional disparities remain evident. Western Europe, despite offering a broader range of testing modalities, maintains some of the highest regulatory barriers, with most EU/EEA countries still prohibiting lay-provider testing or requiring clinician oversight.12 In Central Europe, national guidelines often lack key interventions and show limited integration between HIV and STI services.12 In EECA, punitive legal environments, including the criminalization of sex work, drug use, HIV transmission, or even HIV exposure, are inconsistent with global HIV testing guidance and continue to limit access to community-led services.3,12,17
Written consent is still a mandatory requirement in several countries, maintaining a state of “HIV exceptionalism” that reinforces stigma and discourages testing, particularly in central and eastern sub-regions.3,12,36
Structural and Social Barriers
Structural inequities and social dynamics limit the access to HIV testing. Criminalisation and punitive laws increase the fear of prosecution and contribute to the exclusion of key populations, including PWID, sex workers, migrants, and LGBTQ+ communities, from formal healthcare services.2,4,12,60 In approximately one-third of countries, user fees persist for certain populations or geographic areas, compromising equity of access.4,12 Administrative requirements such as mandatory identification or advance appointments further exclude undocumented migrants and individuals with unstable housing.4,77
Stigma remains a major factor contributing to late diagnosis.1,3,14,77–79 Concerns about confidentiality and the social consequences of a positive result lead many individuals to avoid formal healthcare services.2,3 In EECA, this stigma is particularly acute and reinforced by conservative cultural norms.2,3,11 Low self-perceived risk, especially among heterosexual populations, further limits uptake of regular testing.46,77
Operational Challenges
Operational barriers continue to limit the scalability and sustainability of CBT. Many services operate under conditions of chronic funding insecurity, with several countries relying heavily on international donors or private foundations rather than stable national public financing.1,2 This compromise the continuity of outreach, staffing, and long-term planning, particularly in rural and underserved areas.
Training gaps persist in settings where lay-provider testing is permitted but not adequately supported, resulting in variation in service quality and delivery.7,36 Supply-chain disruptions, including shortages of rapid tests and challenges in procuring integrated HIV/HCV/STI kits, further limit testing capacity.7,36 Fragmented health information systems and limited interoperability with national surveillance platforms also hinder efficient data reporting and monitoring.1,17,22,30
Disruptions Caused by Recent Crisis
Large-scale crises have had a substantial impact on HIV testing and surveillance capacity. The COVID-19 pandemic caused major disruptions in testing availability, with over half of countries reporting reduced HIV testing volumes as community-based services were constrained by lockdowns and public health restrictions.4,80,81 These declines contributed to diagnostic delays and widened existing gaps in early detection.4,8,80 At the same time, the pandemic accelerated innovation in HIVST, digital counselling, and remote kit distribution, highlighting alternative pathways for maintaining services during periods of disruption.18,22,82
The Ukrainian War has created additional barriers by interrupting the continuity of care, limiting access to medication and laboratory services, and forcing large-scale population movements.3,36,83–86 Several community-based organisations rapidly adapted their HIV prevention programs. This included expanding the distribution of prevention materials, scaling-up mobile van services, and shifting counselling activities to online formats where feasible. In parallel, many organisations introduced additional services to respond to the needs of key populations, such as providing humanitarian support (including food, hygiene items, and clothing) and establishing temporary shelters for displaced people.87
Host countries have had to rapidly adapt their surveillance, referral, and treatment systems to address the needs of refugees living with or at risk of HIV.3,36,83–86 These challenges highlight both the vulnerability of community-led services during geopolitical or humanitarian crises and the need for resilient, adaptable systems.
Integrated Testing and Integrated Services/Multi-Disease Approach
European public health guidance strongly supports integrated testing as a standard of good practice. The ECDC and WHO Regional Office for Europe recommend that community-based services routinely offer combined testing for HIV, viral hepatitis, and STIs, especially for key populations at higher risk.22,30 The 2025 European Standards for CBT further specify that integrated testing should be incorporated into routine service delivery, aligning diagnostic strategies across diseases to maximise early detection and facilitate timely linkage to care.13
Several European initiatives have contributed to advancing this approach. The INTEGRATE Joint Action supported its practical implementation by developing tools that demonstrated the feasibility of multi-disease testing in both clinical and community settings.88–91 More recently, the CORE project has shown that combining HIV, viral hepatitis, and STI testing within community programmes effectively reaches underserved groups and accelerates linkage to care.92
Examples across regions highlight the added value of integration. In Georgia, triple rapid testing for HIV, HCV, and syphilis in low-threshold settings has proven particularly effective for PWID.7,90 The introduction of multiplex technologies, such as dual HIV/syphilis rapid tests, has further enabled multiple diagnoses from a single specimen and improved case detection among key populations and pregnant women.7,93–95 Beyond diagnostics, integrated care models implemented in Minsk, Rotterdam, and several programmes in the UK and Portugal provide more comprehensive multi-disease care, including laboratory assessments, liver evaluations, and, in some cases, treatment initiation directly in community settings.34,46
Despite this progress, integration remains uneven across ECA, with many services continuing to operate in disease-specific silos. According to ECDC monitoring, only a subset of EU/EEA countries (17 of 27) has fully incorporated integrated testing for HIV, HBV, HCV, and STIs into national guidance.3,12
Monitoring, Surveillance, and Data Integration
Standardised Community-Based Testing Data Collection
Standardising the monitoring and evaluation of CBT is essential for assessing its impact on public health and for integrating these services into national responses. In Catalonia, the long-standing DEVO community testing network has used harmonized indicators and data collection tools since 1995.24,26 These standardized data have shown that the proportion of notified HIV cases attributed to community services increased form 4.5% in 2001 to 37.8% in 2017, including 70% of new diagnoses among MSM, illustrating the role of robust monitoring in quantifying impact and enabling integration with regional HIV registries.24 The COBATEST network, based on the Catalonian experience, was established to support standardised monitoring and evaluation of CBT practices in ECA. It employs harmonised tools, a shared database, and core indicators aligned with UNAIDS, WHO and ECDC guidance.15,25,57,96 Standardised data produced through the network facilitate cross-site comparisons and robust analysis, providing evidence to inform policy and improve CBT services.25,57,97
Gaps in Surveillance Integration
Despite growing recognition of the value of community-generated data, its integration into national HIV surveillance systems across ECA remains limited and inconsistent. The European Standards of HIV Prevention and Care (2025) set a target of 80% of community HIV testing services to report data through national monitoring systems; however, the lack of harmonised indicators and interoperable digital tools remains a barrier to comparable trend analysis across the region.1,13 As a result, community organisations, frequently the primary source of information on key populations, frequently report data through informal channels, hindering comparability and limiting visibility of their contribution to national testing coverage.2
Several initiatives have been implemented to address these gaps. The INTEGRATE Joint Action developed core indicators and piloted the integration of CBT data into national surveillance systems in Poland, Serbia, Slovakia, and Slovenia, demonstrating feasibility and public health value.98,99 Similarly, the COBATEST Network has reinforced standardised CBT data collection across ECA, improving data quality and facilitating alignment with national reporting frameworks.25,57,100 Since 2018, the Dublin Declaration monitoring process has incorporated specific indicators for CBT, reflecting growing institutional recognition of CBT within regional surveillance systems.101 Some countries, such as Portugal, Ireland, Poland, and Spain, have developed national mechanisms for routine CBT data reporting.98,102–104
Despite promising developments, the integration of community-generated data into the national surveillance remains incomplete. Strengthening digital infrastructure, adopting standardised indicators, and formalising data-sharing mechanisms between community providers and public health authorities will be essential to fully assess testing coverage, identify gaps, and monitor progress among key populations.
Projects and Research
The scale-up of CBT in ECA has been supported by major EU-funded initiatives and reinforced by community-based research cohorts that have provided evidence on effectiveness, monitoring, and HIV incidence among key populations. Collectively, these projects have contributed to defining core concepts, strengthening evaluation frameworks, and accelerating the adoption of innovative approaches across the region.
Major European Strategic Projects
Early European initiatives laid the groundwork for standardised CBT. The HIV-COBATEST Project (2010–2013) established the first consensus definition of CBVCT and core indicators for monitoring access, positivity, and linkage, highlighting the heterogeneity of CBT models across Europe.15,96 Building on this, EUROHIVEDAT (2014–2017) refined monitoring tools, improved guidance on early diagnosis and linkage, particularly for MSM and migrants, and explored digital and network-based testing strategies.105
The ECHOES Survey (2017), implemented under the ESTICOM project, provided the first EU-wide overview of community health workers engaged in supporting MSM, identifying their main roles and core training needs, helping to inform policies and investments in community-led testing capacity.37
The INTEGRATE Joint Action (2014–2020) contributed to broadening CBT by piloting integrated testing for HIV, hepatitis, STI, and TB, scaling-up HIVST, and promoting the inclusion of CBT data within national surveillance systems.88,98,99,106
More recent EU4Health projects (CORE, BOOST, EXPAND, REACH OUT, 4C) have strengthened community-led and outreach-based models, supporting integrated infectious-disease screening and improving access to migrants, PWID, and sex workers.107–111
Community-Based Research Cohorts and Incidence Studies
Community-based cohorts are essential for understanding HIV incidence and testing patterns among key populations, providing evidence that is often missing in traditional surveillance systems. The Lisbon Cohort (CheckpointLX) has monitored HIV incidence among MSM since 2011 through biannual peer-led testing, generating real-time evidence on behavioural risk and prevention trends, identifying an HIV incidence of 2.80 per 100 person-years in 2015.112,113 In Barcelona, the ITACA Cohort (BCN Checkpoint) documented a substantial decline in HIV incidence, from 4.17 to 1.57 per 100 person-years, associated with frequent testing and rapid ART initiation.56,114 Similarly, the Athens Cohort (Ath Checkpoint) has reported incidence rates of around 4 per 100 person-years, with younger MSM showing significantly higher seroconversion risk.115
Cohorts, including the SEXCHECK Study (Bologna) and longitudinal analyses within the COBA-Cohort, have explored co-infection patterns and behavioural risks.116,117
Recent analyses from the COBATEST Network show that routine CBT data can be reliably used to estimate HIV incidence without establishing dedicated cohorts, while also highlighting significant disparities across key populations, particularly non-European migrants, MSM, and sex workers.118
Overall Contribution
Together, these projects and community-led cohorts demonstrate the unique value of CBT as both a testing strategy and an epidemiological resource. By capturing data from populations underrepresented in facility-based surveillance, these initiatives have provided critical evidence to support programme design, policy development, and continuous improvement of community-based and community-led testing models across ECA.
Discussion
The evidence synthesised in this narrative review suggest that CBT has become a critical component of HIV-testing strategies across the ECA region. Rather than playing a marginal role, CBT consistently reaches populations underserved by conventional healthcare systems, contributes to earlier diagnosis of HIV, and facilitates timely linkage to care.1,9,13,119 The diversity of models described reflects the flexibility of community approaches to adapt to different epidemiological contexts, social environments, and population needs.7,9,29,30,34 The use of innovations such as rapid diagnostic tests (including multiplex HIV/syphilis technologies), HIVST, and digital referral ecosystems further strengthens the capacity of CBT to deliver person-centred, stigma-free services.7,8,18,30
Evidence from across the region indicates high acceptability of these approaches, higher positivity yields compared with facility-based testing, and a strong capacity to reach first-time testers, who are often among those most at risk of late diagnosis.9,10,12,25,26,29,41,50,57 Programmes supported by networks like COBATEST and aligned with policy frameworks such as the WHO Differentiated Service Delivery approach and the ECDC European Standards indicate that CBT is not only clinically effective but also scalable and economically efficient.7,9,13,26,30,74
However, progress is still constrained by legal and regulatory restrictions. In particular, limitations on lay providers testing, written consent requirements, and punitive laws affecting key populations (including sex workers, PWID, migrants, and LGBTQ+ communities), continue to challenge the expansion of evidence-based community models.2,3,12,14,17,120 Many national HIV testing guidelines remain outdated, failing to incorporate key innovations, such as HIVST, indicator-condition testing, integrated screening for HIV, hepatitis B/C, and STIs, or task-sharing approaches essential to reaching the 95-95-95 goals.12,14 These policy gaps reinforce regional differences, with Western Europe offering a broader set of yet regulated service options, while structural barriers continue to limit implementation across much of EECA.1,3,17
Structural and social determinants such as stigma, fear of criminalisation, administrative barriers, or lack of healthcare entitlements for undocumented migrants, remain key drivers of delayed diagnosis and inconsistent engagement in prevention and care.2,3,12,14,17,78,79,119 Overall, these dynamics emphasise the importance of community-led, culturally competent, low-threshold approaches that can build trust, ensure confidentiality, and reduce bureaucratic and psychological obstacles to testing.1,18,26,34,62,79
An important gap identified in this review is the limited integration of community-generated data into national HIV surveillance systems.1,13,30 Despite progress through harmonised indicators, digital tools, and EU-funded projects, such as INTEGRATE, only a subset of countries have established routine mechanisms to incorporate CBT indicators into national monitoring frameworks.1,2,13 This lack of systematic data integration means that community-generated data are not consistently captured, impeding accurate assessments of testing coverage, positivity yields, linkage to care, and trends among key populations, ultimately limiting the evidence available for policymaking and resource allocation.12,14,121 Strengthening interoperability, digital infrastructure, and standardised monitoring systems is essential for the consolidation of CBT within national testing systems.12,22
This review also highlights the increasing relevance of accelerated linkage pathways, including peer navigation, proactive referral systems, and in some settings point-of-care confirmatory PCR.26,34,73 These models reduce loss to follow-up after a reactive result and support faster initiation of ART, aligning with emerging European practices and WHO recommendations.7,13 The integration of multiple infections (HIV, HBV, HCV, syphilis, STIs, and tuberculosis) in CBT further enhances efficiency, reduces missed opportunities for diagnosis, and reflects a shift toward more comprehensive, people-centred care.7,13,17,18,22,30
From an economic standpoint, CBT has been shown to be cost-effective, particularly through the early diagnosis of HIV, which reduces long-term treatment costs, and through service models that help decongest facility-based health systems.7,8,29,74 However, long-term sustainability requires transitioning from donor-dependent initiatives to stable domestic financing, including social contracting mechanisms in which governments fund community-led organisations to deliver testing, outreach, and linkage services.17
The COVID-19 pandemic and war in Ukraine have further exposed the vulnerability of HIV services while also creating opportunities for innovation. Disruptions in testing volumes were accompanied by rapid expansion of self-testing, digital counselling, remote distribution of test kits, and adaptive models to ensure continuity of care in the country and for displaced populations.17,18,22,87 These experiences demonstrate both the resilience and adaptability of community-based approaches and highlighting the need for crisis-responsive frameworks capable of sustaining testing and linkage services during emergencies.
This narrative review has several limitations that should be acknowledged. First, the available evidence is unevenly distributed across the region, with a marked predominance of studies and programme examples from Western Europe. This reflects gaps in the published literature and may restrict the transferability of some findings to other contexts. In addition, a proportion of the cited work derives from projects in which the author has been directly involved, some of which were developed within the COBATEST Network, which the author leads. This has resulted in a relatively high level of self-citation rate and raises the possibility of bias associated with reviewing evidence from one’s own professional sphere. This potential limitation is acknowledged, and efforts were made to situate those findings within the wider body of available literature and to reflect the range of approaches reported across different settings.
Implications for Practice and Policy
Overall, the findings underscore that CBT is fundamental to achieving early diagnosis, advancing equity, and strengthening HIV response across ECA. To fully realise the impact of CBT, national strategies must prioritise an enabling policy, financial, and structural environment that allows these services to operate at scale.
The first priority is to remove regulatory barriers by updating national policies to align with WHO/ECDC standards. This includes authorising trained lay providers to perform HIV testing, eliminating unnecessary written consent requirements, and removing legal and punitive frameworks that discourage key populations from seeking testing and care. Such reforms are essential for expanding access and ensuring that CBT models function effectively.
Second, countries should prioritise strategic integration by scaling up person-centred models that combine HIV, hepatitis B/C, syphilis, and STI testing, supported by robust referral pathways, peer navigation, and timely linkage to care. Incorporating HIVST and multiplex diagnostics across community settings can further enhance uptake and diagnostic efficiency.
Third, strengthening monitoring and evaluation systems is critical. Supporting networks, such as COBATEST, and investing in interoperable digital infrastructure will enable the systematic incorporation of community-generated data into national surveillance. High-quality data are critical for improving programmes, guiding, targeted resource allocation, and monitoring progress toward the 2030 goals.
Fourth, securing sustainable financing, particularly through social contracting, will reduce reliance on donor support and ensure long-term operational stability, allowing community-led organisations to expand their reach and maintain service continuity.
Finally, countries must actively address structural inequities, including stigma, criminalisation, migration-related barriers, and gender disparities, through targeted interventions and legal reforms.
Future Research Priorities
Future studies should focus on implementation science for integrated testing models, evaluation of digital and hybrid service modalities, optimisation of post-self-testing linkage pathways, and deeper investigation into structural and legal barriers that continue to limit reach among populations at the highest risk. Advancements in multiplex rapid diagnostics, remote sampling, and real-world economic evaluations are also essential for scaling-up.
Overall Conclusion
This review shows that CBT has become an essential component of HIV responses in ECA, particularly for reaching populations that remain insufficiently served by standard healthcare settings.
Further progress will depend less on generating additional evidence of effectiveness than on creating the conditions for long-term integration, including supportive regulation, stable financing, and routine inclusion of community-generated data in national surveillance. Without these changes, the contribution of community-led testing to ending AIDS as a public health threat by 2030 is likely to remain constrained.
Use of Artificial Intelligence Tools
Artificial intelligence tools Notebook LM (google.com) and Microsoft Copilot (microsoft.com) were used as supportive platforms during the preparation of this narrative review. NotebookLM was employed to synthesise evidence and cross-reference data from the provided primary sources, whereas Microsoft Copilot assisted in summarising complex texts and drafting specific sections to enhance clarity. All AI-generated content was subsequently reviewed, expanded, and validated by the author to ensure scientific accuracy, integrity, and strict adherence to the original source material.
Disclosure
Laura Fernàndez-López reports grants from Gilead Sciences Inc., personal fees from Abbot, outside the submitted work; coordinates and leads the COBATEST Network, which is discussed extensively in this review, and has contributed to several of the initiatives referenced. The author reports no other conflicts of interest in this work.
References
1. European Centre for Disease Prevention and Control/WHO Regional Office for Europe. HIV/AIDS Surveillance in Europe 2025 – 2024 Data. 2025. Available from: https://www.ecdc.europa.eu/en/publications-data/hivaids-surveillance-europe-2025-2024-data.
2. Černý M, Tomšej J. Review of legal/regulatory barriers to community-led and community-based service delivery. CORE Project; 2025. Available from: https://core-action.eu/knowledge-hub.
3. Parczewski M, Gökengin D, Sullivan A, et al. Control of HIV across the WHO European region: progress and remaining challenges. Lancet Reg Health Eur. 2025;52:101243. doi:10.1016/j.lanepe.2025.101243
4. European Centre for Disease Prevention and Control. HIV Testing in Europe and Central Asia - monitoring implementation of the dublin declaration on partnership to fight HIV/AIDS in Europe and Central Asia: 2022 progress report. 2023. Available from: https://www.ecdc.europa.eu/en/publications-data/hiv-testing-europe-and-central-asia.
5. WHO Regional Office for Europe EC for DP and C. HIV/AIDS Surveillance in Europe 2024 – 2023 Data. 2024. Available from: https://www.ecdc.europa.eu/en/publications-data/hiv-aids-surveillance-europe-2024-2023-data.
6. European Centre for Disease Prevention, Control. Progress report on the continuum of HIV care, 2025 (2024 data): monitoring implementation of the Dublin Declaration on partnership to fight HIV/AIDS in Europe and Central Asia. 2025. doi:10.2900/130505.
7. World Health Organization. Consolidated Guidelines on Differentiated HIV Testing Services. 2024. Available from: https://www.who.int/publications/i/item/9789240096394.
8. Brescia V, Ragusa P, Miserere E, Bert F. Assessing the efficiency and effectiveness of community-based voluntary counseling and testing for HIV in Turin: insights from the fast-track cities initiative - a cross-sectional study. BMC Health Serv Res. 2025;25(1):820. doi:10.1186/s12913-025-12865-9
9. Croxford S, Tavoschi L, Sullivan A, et al. HIV testing strategies outside of health care settings in the European Union (EU)/European Economic Area (EEA): a systematic review to inform European Centre for Disease Prevention and Control guidance. HIV Med. 2020;21(3):142. doi:10.1111/HIV.12807
10. Suthar AB, Ford N, Bachanas PJ, et al. Towards universal voluntary HIV testing and counselling: a systematic review and meta-analysis of community-based approaches. PLoS Med. 2013;10(8):e1001496. doi:10.1371/journal.pmed.1001496
11. Terlikbayeva A, Zhussupov B, Primbetova S, et al. Access to HIV counseling and testing among people who inject drugs in Central Asia: strategies for improving access and linkages to treatment and care. Drug Alcohol Depend. 2013;132(1):S61–22. doi:10.1016/j.drugalcdep.2013.07.007
12. European Centre for Disease Prevention and Control. Testing of HIV, Hepatitis B and Hepatitis C in the European Union/European Economic Area (EU/EEA). 2025. doi:10.2900/1359529.
13. European Centre for Disease Prevention and Control. European standards of HIV prevention and care: module on HIV testing. 2025. Available from: https://www.ecdc.europa.eu/en/publications-data/european-standards-hiv-prevention-and-care-module-hiv-testing.
14. Evidence brief: HIV Testing in Europe and Central Asia - monitoring implementation of the Dublin Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia – 2021 Progress Report. 2022. Available from: https://www.ecdc.europa.eu/en/publications-data/evidence-brief-hiv-testing-europe-and-central-asia-monitoring-implementation.
15. Reyes-Urueña J, Breveglieri M, Furegato M, Fernàndez-López L, Agusti C, Casabona J. Heterogeneity of community-based voluntary, counselling and testing services for HIV in Europe: the HIV-COBATEST survey. Int J STD AIDS. 2015;28(1):28–38. doi:10.1177/0956462415623402
16. Freeman-Romilly N, Sheppard P, Desai S, Cooper N, Brady M. Does community-based point of care HIV testing reduce late HIV diagnosis? A retrospective study in England and Wales. Int J STD AIDS. 2017;28(11):1098–1105. doi:10.1177/0956462416688573
17. Joint United Nations Programme on HIV/AIDS. 2024 Global AIDS Report — the Urgency of Now: AIDS at a Crossroads. UNAIDS; 2024. Available from: https://www.unaids.org/en/resources/documents/2024/global-aids-update-2024.
18. Global AIDS strategy 2021–2026 — end inequalities. end AIDS. UNAIDS; 2021. Available from: https://www.unaids.org/en/resources/documents/2021/2021-2026-global-AIDS-strategy.
19. Consolidated guidelines on HIV testing services, 2019. World Health Organization; 2020.
20. Consolidated guidelines on HIV, viral hepatitis and STI prevention, diagnosis, treatment and care for key populations. World Health Organization; 2022.
21. Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations. 2016. Available from: https://www.who.int/publications/i/item/9789241511124.
22. Regional action plans for ending AIDS and the epidemics of viral hepatitis and sexually transmitted infections 2022–2030. 2023. Available from: https://www.who.int/europe/publications/i/item/9789289058957.
23. Sullivan AK, Sperle I, Raben D, et al. HIV testing in Europe: evaluating the impact, added value, relevance and usability of the European Centre for Disease Prevention and Control (ECDC)’s 2010 HIV testing guidance. Eurosurveillance. 2017;22(48):17–00323. doi:10.2807/1560-7917.ES.2017.22.48.17-00323
24. Fernàndez-López L, Reyes-Urueña J, Conway A, et al. The contribution of HIV point-of-care tests in early HIV diagnosis: community-based HIV testing monitoring in Catalonia, 1995 to 2018. Eurosurveillance. 2020;25(43):1900424. doi:10.2807/1560-7917.ES.2020.25.43.1900424
25. Fernàndez-López L, Reyes-Urueña J, Agustí C, et al. The COBATEST network: monitoring and evaluation of HIV community-based practices in Europe, 2014–2016. HIV Med. 2018;19:21–26. doi:10.1111/hiv.12592
26. Compendium of good practices in the health sector response to HIV in the WHO European Region. 2018. Available from: http://www.euro.who.int/pubrequest.
27. World Health Organization. Consolidated guidelines on HIV testing services. 2015. Available from: https://iris.who.int/server/api/core/bitstreams/035ab4d6-a21b-46cb-a838-11871e75b5e4/content.
28. COBATEST Network. COBATEST membership terms of reference. Available from: https://cobatest.org/wp-content/uploads/2024/10/COBATEST-Membership-ToR-2023-3.pdf.
29. Croxford S, Tavoschi L, Sullivan A, et al. Community-based HIV testing in Europe: a systematic review. In:
30. European Centre for Disease Prevention and Control. Public health guidance on HIV, Hepatitis B and C testing in the EU/EEA. 2018. doi:10.2900/424242.
31. Fonner VA, Denison J, Kennedy CE, O’Reilly K, Sweat M. Voluntary counseling and testing (VCT) for changing HIV-related risk behavior in developing countries. Cochrane Database Syst Rev. 2012;2012(9):CD001224. doi:10.1002/14651858.cd001224.pub4
32. Marano-Lee M, Williams W, Uhl G, et al. Contributions of community-based organizations funded by the centers for disease control and prevention’s HIV testing program. J Public Health Manag Pract. 2022;28(2):E461–E466. doi:10.1097/PHH.0000000000001446
33. Spire B, Di Ciaccio M. Community aspects of HIV biomedical prevention. Annu Rev Pharmacol Toxicol. 2026;66(1):113–127. doi:10.1146/annurev-pharmtox-062124-044855
34. European Centre for Disease Prevention and Control. Models of good practice for community-based testing, linkage to care and adherence to treatment for Hepatitis B and C, HIV, and tuberculosis and for health promotion interventions to prevent infections among people who inject drugs. 2022. Available from: https://www.ecdc.europa.eu/en/publications-data/models-good-practice-community-based-testing-linkage-care-and-adherence-treatment.
35. Lorente N, Preau M, Vernay-Vaisse C, et al. Expanding access to non-medicalized community-based rapid testing to men who have sex with men: an urgent HIV prevention intervention (the ANRS-DRAG study). PLoS One. 2013;8(4):e61225. doi:10.1371/journal.pone.0061225
36. Parczewski M, Boesecke C, Khaykin P, et al. Provision of care for people with HIV migrating from Ukraine: preparing for a long-term response. AIDS. 2025;39(6):629–638. doi:10.1097/QAD.0000000000004147
37. Lorente N, Folch C, Aussò S, et al. European Community Health Worker Online Survey (ECHOES): final report. CEEISCAT. 2019. Available from: https://cris.brighton.ac.uk/ws/portalfiles/portal/6689651/D8_5_ECHOES_REPORT_FINAL_APPROVED_CHAFEA.pdf.
38. Marcus U, Ort J, Grenz M, Eckstein K, Wirtz K, Wille A. Risk factors for HIV and STI diagnosis in a community-based HIV/STI testing and counselling site for men having sex with men (MSM) in a large German city in 2011–2012. BMC Infect Dis. 2015;15(1):14. doi:10.1186/s12879-014-0738-2
39. Schmidt AJ, Sandel D, Noori T. From HIV-testing to Gay Health Centres: a Mapping of European “Checkpoints”. In:
40. Fernàndez-Lopez L, Rifà B, Pujol F, et al. Impact of the introduction of rapid HIV testing in the Voluntary Counselling and Testing sites network of Catalonia, Spain. Int J STD AIDS. 2010;21(6):388–391. doi:10.1258/ijsa.2008.008459
41. Falanga C, Marotta C, Negri S, et al. HIV rapid test in a community setting as a strategy to improve access to HIV testing: data from a multicentre experience in Italy. Le Infez Med. 2019;27(4):415–421.
42. Bosa M, Costa S, Gottero M, et al. Analysis of organisational elements in the provision of rapid HIV testing. The case of the Odv Casa Arcobaleno Association. Eur J Volunt Community-Based Proj. 2020;1(1).
43. MacPherson P, Chawla A, Jones K, et al. Feasibility and acceptability of point of care HIV testing in community outreach and GUM drop-in services in the North West of England: a programmatic evaluation. BMC Public Health. 2011;11(1):419. doi:10.1186/1471-2458-11-419
44. Fernandez-Lopez L, Folch C, Majo X, Gasulla L, Casabona J. Implementation of rapid HIV and HCV testing within harm reduction programmes for people who inject drugs: a pilot study. AIDS Care. 2016;28(6):712–716. doi:10.1080/09540121.2016.1164290
45. Fernàndez-López L, Reyes-Urueña J, Egea L, et al. A clinical utility evaluation of dual HIV/Syphilis point-of-care tests in non-clinical settings for screening for HIV and syphilis in men who have sex with men. BMC Infect Dis. 2024;24(S1):264. doi:10.1186/s12879-024-09017-5
46. Twisk DE, Watzeels A, Götz HM. Community-based HIV testing through a general health check event in a high HIV-prevalent multicultural area in Rotterdam, The Netherlands: a pilot study on feasibility and acceptance. Pilot Feasibility Stud. 2023;9(1):101. doi:10.1186/s40814-023-01327-w
47. Cearanovski C, Poverga R. eP.LB024 | Embedding a community-led mobile app within a national HIV digital ecosystem: the case of Moldova. Abstracts of the 20th European AIDS Conference 2025, October 15–18, 2025, Paris, France. HIV Med. 2025;26:754–755. doi:10.1111/hiv.70131
48. Cosmaro L. Lessons Learnt from the Pilot Italian Campaign on HIV Self-Testing, Fondazione LILA Milano. Webinar «Self-Testing on HIV». 2023. Available from: https://aidsactioneurope.org/sites/default/files/2023-09/JUSTLila.%20lessons%20learnt%20from%20the%20pilot%20Italian%20campaign%20on%20HIV%20self-testing_0.pdf.
49. Test order - Zamów Test Na HIV - FES. Available from: https://zamowtestnahiv.pl/en/test-order/.
50. Raccagni AR, Soldini L, Nozza S, et al. eP419 | expanding HIV screening beyondhospital walls in Milan: 18 years of the “EasyTest”project. Abstracts of the 20th European AIDS Conference 2025, October 15–18, 2025, Paris, France. HIV Med. 2025;26:5–701. doi:10.1111/hiv.70104
51. Kirtadze I, Mgebrishvili T, Tabatadze M, et al. eP343 | enhancing HIV self-testing uptakethrough syringe vending machines: a case study inTbilisi, Georgia. Abstracts of the 20th European AIDS Conference 2025, October 15–18, 2025, Paris, France. HIV Med. 2025;26:565. doi:10.1111/hiv.70104
52. Scognamiglio P, Chiaradia G, Giovanetti M, et al. HIV rapid testing in community and outreach sites: results of a nationwide demonstration project in Italy. BMC Public Health. 2018;18(1):748. doi:10.1186/s12889-018-5680-6
53. Schaffer DH, Sawczuk LM, Zheng H, Macias-Konstantopoulos WL. Community-based, rapid HIV screening and pre-exposure prophylaxis initiation: findings from a pilot program. Cureus. 2022;14(1). doi:10.7759/cureus.20877
54. Sophocles C, Stergios M, Georgios G, et al. The Greek Checkpoint “success story” in safeguarding public health: first community-based prevention and testing center in Greece diagnoses 30% of the national 2017 HIV cases. In:
55. Rocha M, Pujol Roca F, Saz Berges J, et al. High contribution, low public funding: Southern European Checkpoints’ role in HIV detection in 4 countries. 2018. Available from: http://hephiv2019abstracts.hiveurope.eu/Abstract_Oral_PS1_01.pdf.
56. Meulbroek M, Dalmau-Bueno A, Saz J, et al. Falling HIV incidence in a community clinic cohort of men who have sex with men and transgender women in Barcelona, Spain. Int J STD AIDS. 2020;31(9):841–848. doi:10.1177/0956462420932424
57. Fernàndez-López L, Reyes-Urueña J, Agustí C, Kustec T, Klavs I, Casabona C. The COBATEST network: a platform to perform monitoring and evaluation of HIV community-based testing practices in Europe and conduct operational research. AIDS Care. 2016;0121:1–5. doi:10.1080/09540121.2016.1146218
58. Fernández-Balbuena S, de la Fuente L, Hoyos J, Rosales-Statkus ME, Barrio G, Belza MJ. Highly visible street-based HIV rapid testing: is it an attractive option for a previously untested population? A cross-sectional study. Sex Transm Infect. 2014;90(2):112–118. doi:10.1136/sextrans-2013-051234
59. Shawe J, McGregor F, Stretch R, Robinson A, Cannon E. Improving the sexual health of homeless people: does providing care within hostels improve contraceptive use and uptake of sexual health screening? Nurs Times. 2018.
60. Lisa Power for OptTEST by HIV in Europe. OptTEST: literature review of legal and regulatory barriers to HIV Testing and Access to Treatment & Care in Europe. 2017. Available from: https://www.eurotest.org/media/pmljhvcc/wp7_literature_review_final.pdf.
61. Europe Centre for Disease Prevention and Control. HIV and sex workers: monitoring implementation of the Dublin Declaration on partnership to fight HIV/AIDS in Europe and Central Asia: 2022 progress report. 2024. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/HIV-and-sex-workers-2022.pdf.
62. Bird PW, Pan D, Trerattanavong K, et al. A systematic review on community-based screening of newly arrived migrants in Europe for tuberculosis, human immunodeficiency virus, and hepatitis B and C. Eur J Public Health. 2026. doi:10.1093/eurpub/ckaf234
63. JLlenas-García J, Navarro M, Ventero M, et al. PS13.1 | community-based screening for HIV and viral hepatitis using dried blood spots in a migrant population in Spain: the HEPINMIGRA study. Abstracts of the 20th European AIDS Conference 2025, October 15–18, 2025, Paris, France. HIV Med. 2025;26:64–66. doi:10.1111/hiv.70104
64. Deblonde J, Sasse A, Del Amo J, et al. Restricted access to antiretroviral treatment for undocumented migrants: a bottle neck to control the HIV epidemic in the EU/EEA. BMC Public Health. 2015;15(1):1–13. doi:10.1186/s12889-015-2571-y
65. Fakoya I, Álvarez-Del Arco D, Monge S, et al. HIV testing history and access to treatment among migrants living with HIV in Europe. J Int AIDS Soc. 2018;21(Suppl 4):e25123. doi:10.1002/jia2.25123
66. Croxford S, Yin Z, Burns F, et al. Linkage to HIV care following diagnosis in the WHO European Region: a systematic review and meta-analysis, 2006–2017. PLoS One. 2018;13(2):e0192403. doi:10.1371/journal.pone.0192403
67. Koenig SP, Dorvil N, Dévieux JG, et al. Same-day HIV testing with initiation of antiretroviral therapy versus standard care for persons living with HIV: a randomized unblinded trial. PLoS Med. 2017;14(7):e1002357. doi:10.1371/journal.pmed.1002357
68. Mateo-Urdiales A, Johnson S, Smith R, Nachega JB, Eshun-Wilson I. Rapid initiation of antiretroviral therapy for people living with HIV. Cochrane Database Syst Rev. 2019. doi:10.1002/14651858.CD012962.pub2
69. Ford N, Migone C, Calmy A, et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS. 2018;32(1):17–23. doi:10.1097/QAD.0000000000001671
70. Lebelonyane R, Bachanas P, Block L, et al. Rapid antiretroviral therapy initiation in the Botswana Combination Prevention Project: a quasi-experimental before and after study. Lancet HIV. 2020;7(8):e545–e553. doi:10.1016/S2352-3018(20)30187-9
71. Micheli G, Caioli A, Esvan R, et al. eP080 | implementation of a same-day ART startmodel in a real-life setting in Italy.Abstracts of the 20th European AIDS Conference 2025, October 15–18, 2025, Paris, France. HIV Med. 2025;26:301–302. doi:10.1111/hiv.70104
72. Krulic T, Brown G, Bourne A. A scoping review of peer navigation programs for people living with HIV: form, function and effects. AIDS Behav. 2022;26(12):4034–4054. doi:10.1007/s10461-022-03729-y
73. Meulbroek M, Pujol F, Pérez F, et al. BCN Checkpoint: same-day confirmation of reactive HIV rapid test with Point of Care HIV-RNA accelerates linkage to care and reduces anxiety. HIV Med. 2018;19(S1):63–65. doi:10.1111/hiv.12595
74. Perelman J, Rosado R, Amri O, et al. Economic evaluation of HIV testing for men who have sex with men in community-based organizations–results from six European cities. AIDS Care. 2017;29(8):985–989. doi:10.1080/09540121.2016.1271392
75. Brescia V, Scavia M, Trentini L, et al. Relazione finale Progetto Torino Fast Track City. Eur J Volunt Community-Based Proj. 2022;1(4):1A–15A.
76. Cremer A, Reintjes R, Schulte B, Kantwerk C, Schmidt AJ. Auswirkungen der Aufhebung des Arztvorbehaltes für HIV-, Hepatitis-C- und Syphilis-Schnelltests in Einrichtungen der Aids- und Drogenhilfe sowie des öffentlichen Gesundheitsdienstes. Bundesgesundheitsblatt Gesundheitsforsch Gesundheitsschutz. 2025;68(10):1194–1203. doi:10.1007/s00103-025-04113-6
77. Hoyos J, Belza MJ, Fernández-Balbuena S, Rosales-Statkus ME, Pulido J, de la Fuente L. Preferred HIV testing services and programme characteristics among clients of a rapid HIV testing programme. BMC Public Health. 2013;13:791. doi:10.1186/1471-2458-13-791
78. European Centre for Disease Prevention and Control. HIV stigma in the healthcare setting: monitoring implementation of the Dublin Declaration on partnership to fight HIV/AIDS in Europe and Central Asia. 2024. doi:10.2900/255834.
79. Bremer V, Pharris A. Five years to 2030: reaching underserved populations is key to ending the AIDS epidemic in Europe. Eurosurveillance. 2024;29(48):2400778. doi:10.2807/1560-7917.ES.2024.29.48.2400778
80. Fernàndez-López L, Simões D, Casabona J. Impact of the COVID-19 pandemic on community-based testing for HIV, viral hepatitis and sexually transmitted infections in the WHO European Region, March to August 2020. Eur J Public Health. 2023;33(3):528–535. doi:10.1093/eurpub/ckad010
81. Simões D, Stengaard AR, Combs L, Raben D; The EuroTEST COVID-19 impact assessment consortium of partners. Impact of the COVID-19 pandemic on testing services for HIV, viral hepatitis and sexually transmitted infections in the WHO European Region, March to August 2020. Eurosurveillance. 2020;25(47):2001943. doi:10.2807/1560-7917.ES.2020.25.47.2001943
82. European Centre for Disease Prevention and Control. The Impact of the COVID-19 Pandemic on the HIV Response in Europe and Central Asia Monitoring Implementation of the Dublin Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia. 2024. doi:10.2900/438904.
83. World Health Organization Regional Office for Europe. Standardized protocol for clinical management and medical data-sharing for people living with HIV among refugees from Ukraine. 2022. (WHO/EURO:2022-5288-45052-64211). Available from: https://iris.who.int/server/api/core/bitstreams/688778c8-26a9-40c1-8004-5cd603a9045e/content.
84. European Centre for Disease Prevention, Control, World Health Organization. Ensuring high-quality HIV care for displaced people from Ukraine. 2022. Available from: https://iris.who.int/server/api/core/bitstreams/688778c8-26a9-40c1-8004-5cd603a9045e/content.
85. Nikitin BM, Bromberg DJ, Ivasiy R, et al. Disruptions to HIV Prevention During Armed Conflict in Ukraine and Other Settings. Curr HIV/AIDS Rep. 2025;22(1):10. doi:10.1007/s11904-024-00716-x
86. Vasylyev M, Skrzat-Klapaczyńska A, Bernardino JI, et al. Unified European support framework to sustain the HIV cascade of care for people living with HIV including in displaced populations of war-struck Ukraine. Lancet HIV. 2022;9(6):e438–e448. doi:10.1016/S2352-3018(22)00125-4
87. Friedman SR, Smyrnov P, Vasylyeva TI. Will the Russian war in Ukraine unleash larger epidemics of HIV, TB and associated conditions and diseases in Ukraine? Harm Reduct J. 2023;20(1):119. doi:10.1186/S12954-023-00855-1
88. Gasbarrini N, Dubravić D, Combs L, et al. Increasing integrated testing in community settings through interventions for change, including the Spring European Testing Week. BMC Infect Dis. 2021;21(S2):874. doi:10.1186/s12879-021-06555-0
89. Matulionytė R, Jakobsen ML, Grecu VI, et al. Increased integrated testing for HIV, hepatitis C and sexually transmitted infections in health care facilities: results from the INTEGRATE Joint Action pilots in Lithuania, Romania and Spain. BMC Infect Dis. 2021;21(S2):845. doi:10.1186/s12879-021-06537-2
90. Valkovičová Staneková D, Wimmerová S, Fernàndez-López L, et al. Piloting an integrated HIV, HCV and syphilis testing approach in community-based voluntary counselling and testing services in Slovakia. Epidemiol Mikrobiol Imunol. 2024. doi:10.61568/emi/11-6352/20240726/138062
91. INTEGRATE Joint Action. Integrated testing in community and low-threshold settings. Available from: https://iris.who.int/server/api/core/bitstreams/035ab4d6-a21b-46cb-a838-11871e75b5e4/content.
92. Fernàndez-López L, Gogishvili M, Vicente M, et al. PS02.3 | strengthening community-based integrated HIV/STI/VH prevention, testing, and linkage-to-care: first-year outcomes of the CORE project. Abstracts of the 20th European AIDS Conference 2025. HIV Med. 2025:12–13. doi:10.1111/hiv.70104
93. Karellis A, Naeem F, Nair S, et al. Multiplexed rapid technologies for sexually transmitted infections: a systematic review. Lancet Microbe. 2022;3(4):e303–e315. doi:10.1016/S2666-5247(21)00191-9
94. World Health Organization. Dual HIV/Syphilis rapid diagnostic tests can be used as the first test in antenatal care: policy brief. 2019. Available from: https://www.who.int/.
95. Van Den Heuvel A, Smet H, Prat I, et al. Laboratory evaluation of four HIV/syphilis rapid diagnostic tests. BMC Infect Dis. 2019;19(1):1. doi:10.1186/s12879-018-3567-x
96. HIV-COBATEST Project. Core Indicators to Monitor Community Based Voluntary Counselling and Testing (CBVCT) for HIV Guidelines for CBVCT Services, Field-Test Version. 2012. Available from: https://cobatest.org/wp-content/uploads/2023/04/ehe_cdocsmenu_cdocsmenu_doc_3-CBVCT_core_indicators_field_test_version.pdf.
97. Gogishvili M, Aceitón J, Alarcón Gutiérrez M, Casabona J, Fernàndez-López L; COBATEST Steering Comitee. COBATEST Network 2022 Report: monitoring and Evaluation. 2024.
98. Fernàndez-López L, Baros S, Niedźwiedzka-Stadnik M, et al. Integration of community-based testing data into national HIV surveillance in Poland, Serbia and Slovakia within the framework of INTEGRATE project. BMC Infect Dis. 2021;21(Suppl 2):800. doi:10.1186/S12879-021-06498-6
99. Fernàndez-López L, Klavs I, Conway A, et al. Recommendations for collection and integration of community-based testing and linkage to care data into national surveillance, monitoring and evaluation systems for HIV, viral hepatitis and sexually transmitted infections: results from the INTEGRATE Joint Action. BMC Infect Dis. 2021;21(Suppl 2):794. doi:10.1186/S12879-021-06499-5
100. Reyes-Urueña J, Fernàndez-Lopez L, Montoliu A, et al. Assessing the quality of routine HIV testing data in the community setting “COBATEST Network. Int J STD AIDS. 2019;30(10):999–1008. doi:10.1177/0956462419857572
101. European Centre for Disease Prevention and Control. HIV testing, monitoring implementation of the dublin declaration on partnership to fight HIV/AIDS in Europe and Central Asia: 2018 progress report. 2019. Available from: https://www.ecdc.europa.eu/en/publications-data/hiv-testing-monitoring-implementation-dublin-declaration-partnership-fight.
102. Meireles P, Barros H, Aguiar A, Simões D, Freitas R, Mendão L. The Community Screening Network project - Surveillance of HIV, viral hepatitis and sexually transmitted infections in the community in Portugal. Rev Epidemiol Sante Publique. 2018;66:S396. doi:10.1016/j.respe.2018.05.437
103. Brady M, Shanley A, Hurley C, et al. Establishment of a national surveillance system to monitor community HIV testing, Ireland, 2018. Irish J Med Sci. 2020;189(4):1507–1514. doi:10.1007/s11845-020-02217-3
104. División de Control de VIH ITS Hepatitis Virales y Tuberculosis. Red Comunitaria de Programas de Cribado de Infección Por VIH (RedCoVIH). Informe Anual 2024. 2025. Available from: https://www.sanidad.gob.es/en/areas/DCVIHT/vihSida/REDCOVIH/docs/Informe_pruebas_RedCoVIH_2024_v2_definitivos.pdf.
105. EURO HIV EDAT outputs. Available from: https://cobatest.org/en/conferences-and-publications/.
106. BMC Infectious Diseases. Results from INTEGRATE - the EU joint action on integrating prevention, testing and linkage to care strategies across HIV, viral hepatitis, TB and STIs in Europe. Available from: https://bmcinfectdis.biomedcentral.com/articles/supplements/volume-21-supplement-2.
107. AIDS ACTION EUROPE. CORE – community Response to End Inequalities. 2023. Available from: https://core-action.eu/core-home.
108. Correlation – European Harm Reduction Network. BOOST – strengthening community-based and community-led organisations in providing communicable diseases services. 2025. Available from: https://community-boost.eu/.
109. EXPAND – expanding access to community-based testing for HIV, viral hepatitis and STIs in Slovenia. 2023. Available from: https://www.filantropija.org/expand/.
110. Reach Out Europe. REACH-OUT – integrated community healthcare and outreach services for hard-to-reach populations. 2023. Available from: https://reachouteurope.eu/.
111. Médecins du Monde Greece. 4C – crossing Countries, Crossing Communities. 2026. Available from: https://www.mdmgreece.gr/en/action/4c-rapid-test/.
112. Meireles P, Lucas R, Carvalho C, et al. Incident risk factors as predictors of HIV seroconversion in the Lisbon cohort of men who have sex with men: first results, 2011–2014. Eurosurveillance. 2015;20(14):45–56. doi:10.2807/1560-7917.ES2015.20.14.21091
113. Meireles P, Lucas R, Martins A, et al. The Lisbon Cohort of men who have sex with men. BMJ Open. 2015;5(5):e007220. doi:10.1136/bmjopen-2014-007220
114. Ferrer L, Loureiro E, Meulbroek M, et al. High HIV incidence among men who have sex with men attending a community-based voluntary counselling and testing service in Barcelona, Spain: results from the ITACA cohort. Sex Transm Infect. 2016;92(1):70–75. doi:10.1136/sextrans-2015-052042
115. Nikolopoulos GK, Chanos S, Tsioptsias E, Hodges-Mameletzis I, Paraskeva D, Dedes N. HIV incidence among men who have sex with men at a community-based facility in Greece. Cent Eur J Public Health. 2019;27(1):54–57. doi:10.21101/cejph.a4856
116. Lorente N, Fernàndez-López L, Fuertes R, et al. COBA-Cohort: a prospective cohort of HIV-negative men who have sex with men, attending community-based HIV testing services in five European countries (a study protocol). BMJ Open. 2016;6(7):e011314. doi:10.1136/bmjopen-2016-011314
117. Lorente N, Fuertes R, Rocha M, et al. Report on the Determinants of HIV Test-Seeking Behaviour among MSM in Europe. 2018. Available from: https://cobatest.org/wp-content/uploads/2019/03/ehe_docsmenu_docsmenu_doc_162-Final_report_WP5_Euro_HIV_EDAT1.pdf.
118. Fernàndez-López L, Alarcón M, Escaramís G, et al. eP397 | estimating HIV incidence and associated risk factors using longitudinal community-based testing data across the WHO European Region: insights from the COBATEST Network. Abstracts of the 20th European AIDS Conference 2025. HIV Med. 2025;26(S4):604–605. doi:10.1111/hiv.70104
119. European Centre for Disease Prevention and Control. HIV and Migrants in the EU/EEA - Monitoring the Implementation of the Dublin Declaration on Partnership to Fight HIV/AIDS in Europe and Central Asia: 2024 Progress Report (2023 Data). 2024. Available from: https://www.ecdc.europa.eu/en/publications-data/hiv-and-migrants-eueea-monitoring-implementation-dublin-declaration-partnership.
120. Kadye T, Jamil MS, Johnson C, Baggaley R, Barr-DiChiara M, Cambiano V. Country uptake of WHO recommendations on differentiated HIV testing services approaches: a global policy review. BMJ Open. 2024;14(3):e058098. doi:10.1136/bmjopen-2021-058098
121. European Centre for Disease Prevention and Control. HIV testing in Europe evaluation of the impact of the ECDC guidance on HIV testing: increasing uptake and effectiveness in the European Union HIV testing in Europe. 2016. doi:10.2900/818448.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.