Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Comment on: “Association Between the Hemoglobin Glycation Index (HGI) and Risk of Diabetic Nephropathy: A Retrospective Cohort Study” [Response to Letter]
Weiyi Zhou,1 Lingyu Zhang,2 Tongqiang Liu1
1Department of Nephrology, The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Changzhou Medical Center, Changzhou, Jiangsu, People’s Republic of China; 2Department of Endocrinology, The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Changzhou Medical Center, Changzhou, Jiangsu, People’s Republic of China
Correspondence: Tongqiang Liu, Department of Nephrology, The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, 68 Middle Gehu Road, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected]
View the original paper by Mr Zhou and colleagues
This is in response to the Letter to the Editor
Dear editor
We have received the correspondence from Ren et al regarding our recently published study and appreciate their insightful comments. Our research was to reveal a significant U-shaped relationship between the Hemoglobin Glycation Index (HGI) and the risk of Diabetic Nephropathy (DN) in patients with Type 2 Diabetes Mellitus.1,2
In response to the two main points raised in the letter, we provide the following clarifications:
First, regarding the potential interaction between HGI and different glucose-lowering treatment regimens, we have conducted supplementary analyses as suggested. We constructed both a base model and an extended model incorporating interaction terms between HGI and specific medications (Table 1). The results show that the association between HGI and DN was not significantly modified by the use of insulin, metformin, or DPP-4 inhibitors (Interaction P-values = 0.3801, 0.1028, and 0.2, respectively). It is important to note that our study was conducted before newer antidiabetic agents with demonstrated renal benefits, such as SGLT-2 inhibitors and GLP-1 receptor agonists, were widely available in China.3,4 Consequently, our study could not evaluate their potential interaction with HGI. Subsequent research should indeed prioritize investigating these novel therapeutic classes.
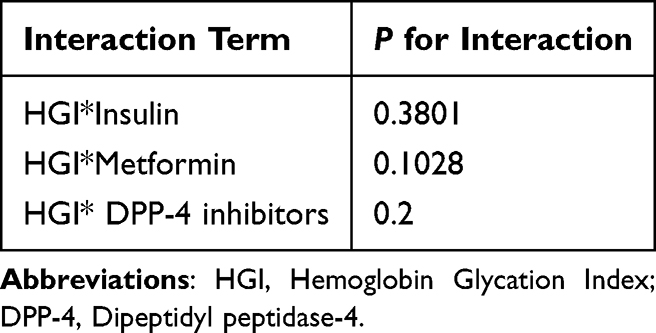 |
Table 1 Interaction Between HGI and Drugs and Its P-value |
Second, concerning the clinical operability and generalizability of HGI, we fully agree with the points raised. While the linear regression model we developed, based on fasting blood glucose and HbA1c, performed well within our cohort, its generalizability across diverse ethnicities, age groups, and comorbid conditions certainly requires further validation. Particularly noteworthy is the strong association between HGI and hypertension, which represents a crucial consideration for clinical application.5 The question of whether the HGI threshold should be adjusted for diabetic patients with comorbidities such as hypertension is a highly relevant clinical direction. We encourage research teams from different centers to utilize prospective designs and more comprehensive clinical data to jointly develop and validate more individualized and universally applicable HGI assessment tools, thereby facilitating its transition from a research indicator to a practical clinical instrument.
We thank the commentators once again for their valuable suggestions, which have significantly enhanced our discussion and provided clear direction for future research.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors approved of the final version accepted for publication; agreed on the journal to which this communication was submitted; and agree to be accountable for all aspects of the work. WZ: Formal analysis, Writing – original draft; LZ: Formal analysis, Writing – review and editing; TL: Conceptualization, Writing – review and editing.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this communication.
Disclosure
The authors declare no competing interests.
References
1. Ren Y, Chen Z, Wang B. Comment on: “association between the hemoglobin glycation index (HGI) and risk of diabetic nephropathy: a retrospective cohort study” [Letter]. Diabetes Metab Syndr Obes 2025;18:3795—3796. doi:10.2147/DMSO.S569377.
2. Zhou W, Zhang L, Liu T. Association between the hemoglobin glycation index (HGI) and risk of diabetic nephropathy: a retrospective cohort study. Diabetes Metab Syndr Obes. 2025;18:1859–1872. doi:10.2147/DMSO.S523442
3. Shokravi A, Seth J, Mancini GBJ. Cardiovascular and renal outcomes of dual combination therapies with glucagon-like peptide-1 receptor agonists and sodium-glucose transport protein 2 inhibitors: a systematic review and meta-analysis. Cardiovasc Diabetol. 2025;24(1):370. doi:10.1186/s12933-025-02900-8
4. Layton JB, Ziemiecki R, Johannes CB, et al. Outcomes in new user cohorts of SGLT2 inhibitors or GLP-1 receptor agonists with type 2 diabetes and chronic kidney disease. Diabetes Ther. 2025;16(8):1597–1614. doi:10.1007/s13300-025-01750-7
5. Wu QY, Mo LR, Nan J, Huang WZ, Wu Q, Su Q. The association between the hemoglobin glycation index and cardiometabolic diseases: a mini-review. J Clin Hypertens. 2025;27(7):e70092. doi:10.1111/jch.70092
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.