Back to Journals » Risk Management and Healthcare Policy » Volume 16
Combining the Real-Time Vial Sharing Strategy with Daily-Rate Charge Mode for Antimicrobial Drugs of Inpatients: An Economical and Practical Method for Patients and Hospitals
Authors Li J, He Y, Lei X, Cao Z, Liao Y, Wang G, Chen Z, Li X ![]() , Liu X
, Liu X ![]()
Received 28 April 2023
Accepted for publication 11 August 2023
Published 14 August 2023 Volume 2023:16 Pages 1521—1530
DOI https://doi.org/10.2147/RMHP.S418886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Jianquan Li, Yongyang He, Xi Lei, Zhongqiang Cao, Yuwei Liao, Guoqiang Wang, Zebin Chen, Xuejuan Li, Xiaoya Liu
Department of Pharmacy, Shenzhen Children’s Hospital, Shenzhen, Guangdong Province, People’s Republic of China
Correspondence: Xiaoya Liu, Department of Pharmacy, Shenzhen Children’s Hospital, Shenzhen, 518026, Guangdong Province, People’s Republic of China, Tel +86 075583008256, Email [email protected]
Background: Antimicrobial agents’ wastage is a huge problem, especially for pediatric patients, resulting in excessive drug expenditure and increasing the economic burden on patients’ families. Moreover, the cost of disposing of antimicrobial agents’ waste and the risk of environmental and occupational exposure also increased. This study aimed to explore the cost-effectiveness of the vial-sharing strategy combined with the daily-rate charge mode for pediatric inpatients to provide a strategy for reducing patients’ expenditures, saving medical costs, and reducing drug proportion.
Methods: This retrospective study was conducted at Pharmacy Intravenous Admixture Service (PIVAS), Shenzhen Children’s Hospital, Guangdong Province, China, in 2022. Data on prescription drugs were collected from the PIVAS system. Ten antimicrobial drugs with a frequency of prescriptions no less than twice once daily were selected, and the drug costs, drug weight, and drug saved were further analyzed according to the combination of real-time vial sharing strategy and daily-rate charge mode. Traditional single vial charge mode without vial sharing was set as a control strategy. The actual expenditure of the hospital was also calculated and analyzed.
Results: During 2022, ¥ 4,122,099 (34.4%) was saved for inpatients by applying a vial-sharing strategy on ten antibacterial agents, and more than 46,343,750 mg (24.6%) of drugs were totally saved. The top 5 drugs saved by the real-time vial-sharing strategy were cefoperazone-sulbactam, vancomycin, amoxicillin-sulbactam, ceftazidime, and meropenem. Taken the price into consideration, the top five payment-saved drugs were vancomycin (¥ 1,522,385), meropenem (¥ 1,311,475), cefoperazone-sulbactam (¥ 736,697), imipenem-cilastatin (¥ 406,092), and amoxicillin-sulbactam (¥ 51,394). Moreover, the account balance of the hospital was up to ¥ 426,499.
Conclusion: The real-time vial sharing strategy combined with the daily-rate charge mode greatly reduces drug wastage and patients’ payments. It may be useful for hospitals with PIVAS to achieve vial-sharing while protecting the best interest of inpatients.
Keywords: real-time vial sharing strategy, daily-charge mode, antimicrobial drugs, inpatients, PIVAS
Introduction
Antimicrobials are the most commonly prescribed medicines in pediatrics. It is estimated that between 37% and 61% of infants and children are treated with antibiotics during hospitalization.1–3 However, limited by the shortage of children-specific dosage forms, clinicians have to prescribe large specifications for children. As a result, it is common for the residual drug to be left over in vials due to patient-specific dosages. Drug wastage is defined as the amount of drug dispensed but discarded without administration.4 MacBrayne et al analyzed the anti-infective waste in the Children’s Hospital Colorado and found that significant quantities of anti-infective drugs are unused, incurring roughly $100,000 in waste annually.5 Drug wastage increases the excessive economic burden on patients, raises healthcare costs, and contributes significantly to the global emergency of antimicrobial resistance.6,7 Therefore, it is necessary to reduce antibiotic waste for resource and cost savings.
Vial sharing has become common in large hospitals, especially for expensive drugs.8,9 By using quantities of drugs that would have previously been discarded, cytotoxic and biological waste production is also reduced. A study retrospectively analyzed the wastage of cancer chemotherapeutic drugs in an oncology unit and found that vial sharing showed a 9% reduction in 1 year.4 Similarly, another study performed in a Dutch hospital estimated the cost savings by implementing a vial-sharing strategy between 2017 and 2021, resulting in savings of € 280,000. Despite the effectiveness of the vial-sharing strategy in cost savings, there are regulatory, safety, stability, and microbiological concerns regarding the reuse of the drug vials. It means that alternative compounding strategies that reduce drug waste are urgently needed.
As stated in United States Pharmacopeia, the sterile products packaged as a single-use vial should be used within 6h of opening if maintained in an ISO 5 environment or within 1 hour if not kept under these conditions.10 To accommodate vial sharing, some hospitals or disease research centers use Closed System Drug Transfer Devices (CSTD) to extend the shelf life of drugs after opening. However, most hospitals in China, our hospital included, cannot afford CSTD. Therefore, a real-time vial-sharing strategy was implemented in Pharmacy Intravenous Admixture Services (PIVAS) in our hospital to avoid unnecessary risk caused by the storage of opened vials. The real-time vial sharing means that the preparation of all prescription doses of the same drug is done at once based on the pre-classification of the same drug in different prescriptions in one batch. Few investigations on the real-time vial-sharing strategy have been conducted outside of China.11 Accompanying the real-time vial sharing strategy, we introduced the daily-rate charge mode to reduce patient payments as much as possible. Since vial-sharing means less than a vial of drug was administrated to one patient, it is unreasonable to charge on a per vial basis. Daily-rate charge mode implies that patients pay for the required drug quantity rather than for each prescription, which permits significant cost savings. These strategies were approved after consultation with clinicians, pharmacists and administrators. Currently, twenty medications are included and dispensed by the vial-sharing strategy.
This study was conducted to compare and analyze the difference in drug cost and drug wastage between the traditional charge mode and the new charge system in PIVAS for antibiotic prescriptions of inpatients. In addition, the benefit for both inpatients and hospitals were analyzed and summarized.
Methods
Data Sources and Workflow of PIVAS
This retrospective study was conducted at Pharmacy Intravenous Admixture Services of the Shenzhen Children’s Hospital, Guangdong Province, China. Data were extracted from the PIVAS system for preparations in 2022. Figure 1 illustrates the main workflow of PIVAS in our hospital. Except for the routine steps in PIVAS, the classification step was added as preparation work for vial-sharing to improve the effectiveness of the real-time vial sharing strategy. Drugs that can be shared in vials were previously set up in PIVAS. The PIVAS system informs the medical worker when multiple two-dimensional prescription information is used as code for the same drug. Next, the medical staff can put these prescriptions into one batch for further compounding to achieve real-time vial-sharing. Furthermore, the prescriptions were dispensed every two hours during the day. Prescriptions with the same drug in the same periods were automatically classified by the PIVAS system to reduce drug wastage. We did not share vials among different working periods to decrease contamination and confusion.
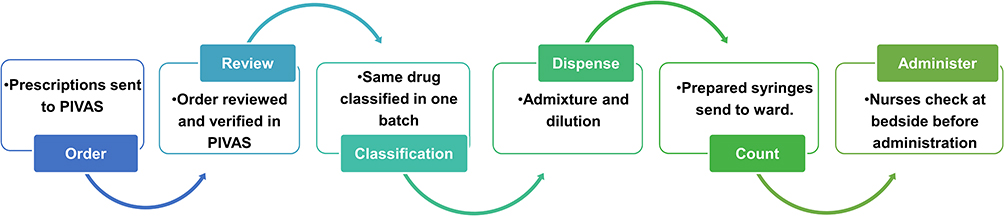 |
Figure 1 Workflow of PIVAS. |
For the traditional single dose preparation method, no batching or vial sharing was implemented and the drug residual was discarded after each preparation. Therefore, the vials of ten drugs prescribed by clinicians were counted and compared with the actual drug consumption.
The Selection of Drugs
To compare drug wastage, patients’ payment, and the cost of the hospital between two different charge modes, we selected several drugs with different characteristics of dosage and administration. After reviewing previous research and discussing with a clinical pharmacist, we selected ten antibiotics that were administrated no less than twice a day. The actual consumption of these selected agents, the theoretically number of vials according to different strategies, and the hypothetical drug wastage were obtained by sending the corresponding instructor to the PIVAS system. To further analyze the cost saving and drug wastage, the price, specification, and usage were recorded.
Charge Mode
This study compared two charge modes: the single vial-charge mode and the daily-rate charge mode. Traditionally, patients have to pay for their drugs by vials. For example, as illustrated in Figure 2, patient 1 prescribed a dosage of 30 mg and patient 2 prescribed a dosage of 50 mg both had to pay for 3 vials of drugs per day because the frequency of their prescription was three times a day. Therefore, a new drug vial was opened for each administration. However, this charging mode was unreasonable when the vial sharing strategy was implemented. As illustrated in Figure 3, only 90 mg drug was used by patient 1. Thus, we introduced the daily-rate charge mode, meaning that patients have to pay for their total drug users in one day rather than for every administration. The dose-rounding strategy was included in the daily charge mode. For example, considering that the total used drug for patient 1 was 90 mg (< 1 vial), we charged for 1 vial only. Similarly, patient 2 who required 150 mg during a day (> 1 vial but < 2 vials), was charged for 2 vials.
 |
Figure 2 Illustration of drug discarded and the actual payment of inpatients prescribed with same drug but without vial sharing and charged in single does mode. |
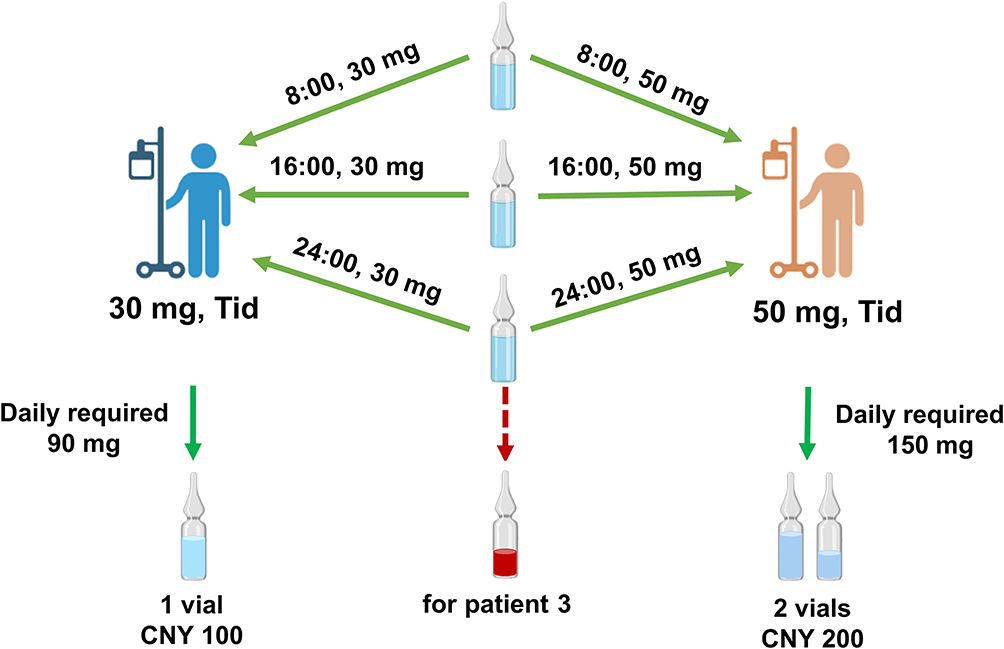 |
Figure 3 Illustration of drug discarded and the actual payment of inpatients prescribed with same drug with real-time vial sharing and daily-rate charged. |
Data Collection and Calculation
The information on ten drugs was collected, including the name of the prescribed drug, a unit price per vial of the drug, drug specification, the actual dose of the drug and the number of vials used. In addition, the amount of drug saved was calculated according to the difference between patient usage and vial specifications.
The payment saved for patients was also analyzed. Furthermore, we also analyzed the hospital’s expenditure for these drugs and verified whether the daily-rate charge mode was cost-effective, combined with the real-time vial sharing strategy.
Results
Amount of Drug Usage
The information on the ten antibacterial agents were compared was illustrated in Table 1 and two bar charts were used to compare the theoretical consumption of drugs (Figure 4). The real-time vial-sharing strategy was able to save drugs for all selected species. The top 5 drugs saved by the real-time vial-sharing strategy were cefoperazone-sulbactam (15,281,000 mg), vancomycin (7,389,500 mg), amoxicillin-sulbactam (7,266,000 mg), ceftazidime (6,056,000 mg), and meropenem (4,682,500 mg) (Figure 4a). The number of cefoperazone-sulbactam needed according to the traditional single dose preparation was 57,978 vials, while only 42,697 vials were actually used in 2022. Similarly, 14,779 vials of vancomycin were saved by the real-time vial-sharing method. Unsurprisingly, the more frequently the drug administration was required, the more drug was saved. The least saved drug was fusidate since only 576 vials were prescribed in 2022, which was less than 1% of cefoperazone-sulbactam (Figure 4b). Overall, 46,343,750 mg antibacterial drugs were saved using a real-time vial sharing strategy, approximately 25% of the originally prescribed.
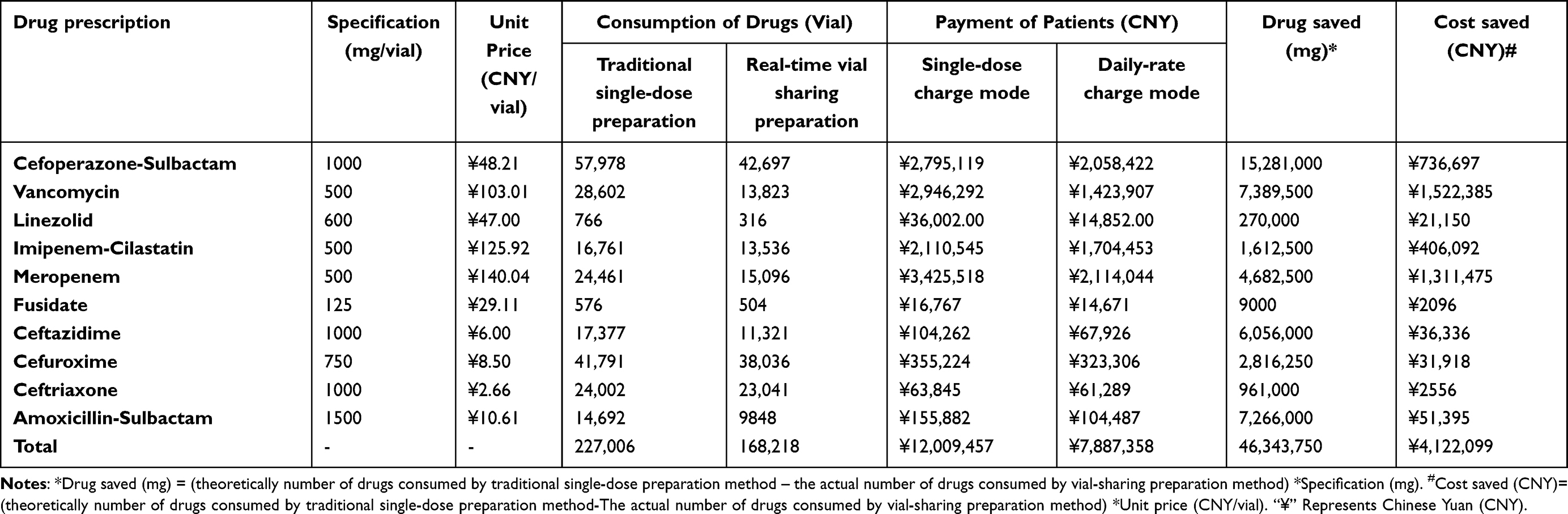 |
Table 1 Summary of Information on ten Antibacterial Drugs in PIVAS |
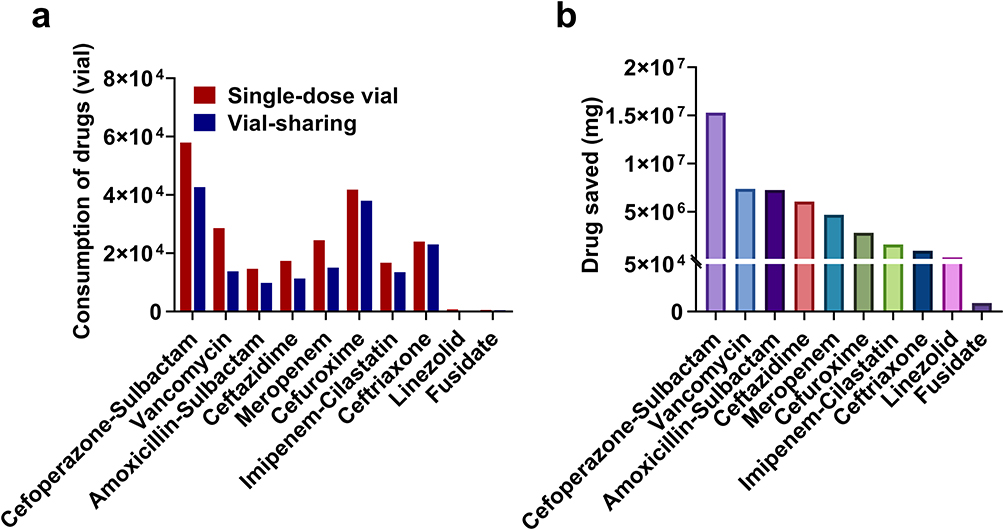 |
Figure 4 The theoretical number of drugs used in 2022 by single-dose vial strategy and real-time vial sharing strategy. (a) The number of antibacterial drugs vials. (b) The total amount of drugs saved by weight. |
Payment Saved for Inpatients
The payments of patients for these drugs in two charge modes are illustrated in Table 1 and Figure 5a. The top five payment-saved drugs were vancomycin (¥1,522,385), meropenem (¥1,311,475), cefoperazone-sulbactam (¥736,697), imipenem-cilastatin (¥406,092), and amoxicillin-sulbactam (¥51,394). Only 2095 yuan was saved by daily charge mode for fusidate. Despite that more ceftriaxone was saved when compared with the amount of linezolid, the daily-charge mode saved more money for patients prescribed with linezolid because of the high unit price of linezolid (Figure 5b).
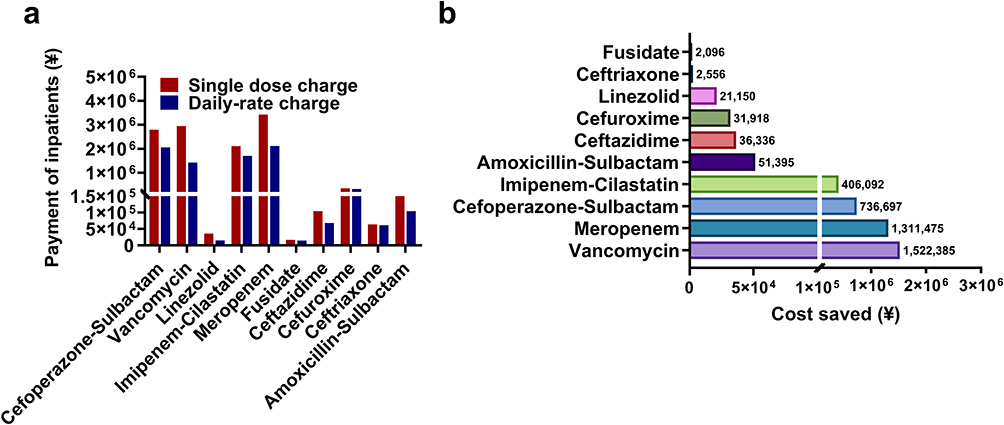 |
Figure 5 The payment of patients for selected drugs by traditional single does charge mode and daily-rate charge mode (a) and the calculated cost saved for inpatients (b). |
The ratio of drugs saved is illustrated in Figure 6. The saved amount of cefoperazone-sulbactam and vancomycin accounts for almost half of the total drug saved (49%) (Figure 6a). The weight of cefoperazone-sulbactam saved accounts for 33% of the total drugs because its clinical use was the highest among the ten drugs. The cost saved for inpatients was highest for vancomycin, followed by meropenem and cefoperazone-sulbactam (Figure 6b). This might be due to the high unit price of vancomycin (¥103.01/vial) and meropenem (¥140.04/vial), while the price of cefoperazone-sulbactam was only ¥48.21 per vial. On the contrary, despite fusidate having a higher price, the cost saved for it was less than ceftazidime (¥2096 vs ¥36,336). Therefore, the financial benefit of the vial-sharing strategies was associated with both the quantity of drugs’ consumption and the unit price.
 |
Figure 6 The ratio of drug saved (a) and cost saved (b) among ten antibacterial drugs. |
The Account Balance of Drugs and Expenditure of PIVAS
The actual expenditure of drugs in PIVAS is summarized and shown in Table 2. Eight of the ten selected drugs were profitable, while two were defective. In addition, 504 vials of fusidate were paid in 2022, but 579 vials were used. Moreover, 1559 vials of linezolid were charged for inpatients, while more than 2500 vials were used. Correspondingly, 46,342 yuan were lost because of the extra consumption of linezolid. However, there was still ¥426,499 in an economic surplus of PIVAS by combining the real-time vial sharing method and daily-charge mode.
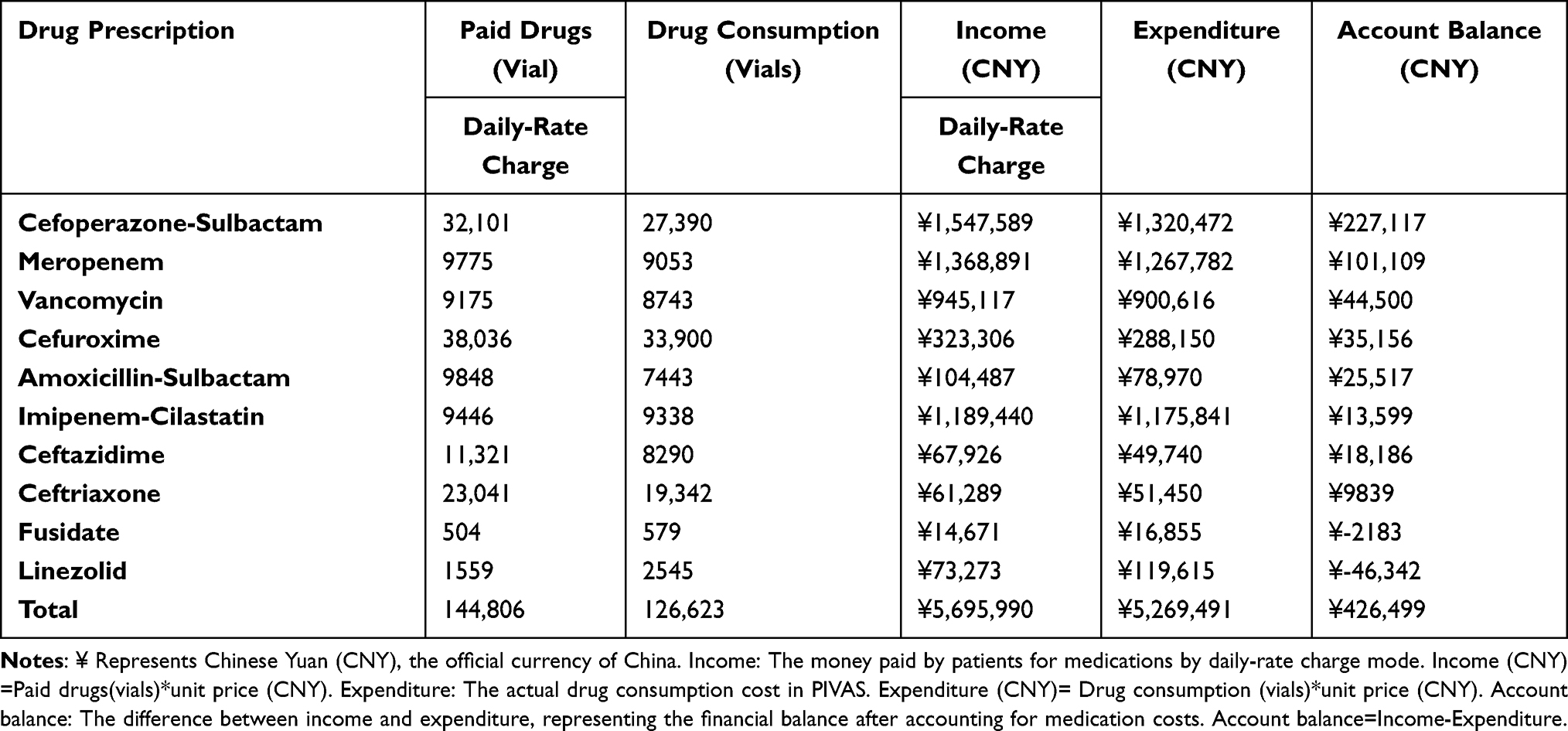 |
Table 2 The Summary of Inpatients’ Paid Drugs and Actual Expenditure of PIVAS |
Discussion
This is the first study reporting on real-world, patient-level data to show the benefit for inpatients and medical service providers by combining the daily-charge mode with the real-time vial-sharing method in PIVAS. In 2022, after applying a vial-sharing strategy on ten antibacterial agents, ¥ 4,122,099 (34.4%) and more than 46,343,750 mg (24.6%) of drugs were saved.
The vial sharing strategy has become common practice globally. Most research about vial sharing was associated with injectable cancer drugs.9,12,13 A survey conducted by Gilbar and Chambers found that vial sharing strategies for frequently used drugs have been employed in more than 10 countries, and cost savings were achieved in 74% of cases.14 The vial-sharing strategy was implemented in our hospital in 2014.15 Previously, the opened vials were left in a safety cabinet to keep them away from contamination until reuse. However, the Good Manufacturing Practice guideline prohibits storing vials with residual drugs in the cabinet. It means these vials must be stored outside the class A environment, which might introduce the risk of microbiological contamination.16 To solve this problem, closed-system drug transfer devices were considered but later given up because of the high price of CSTD. Next, we decided to put forward the concept of “real-time vial sharing”, modifying the PIVAS system automatically matched the prescriptions with the same drug in each dispensing period for inpatients for further vial-sharing. No further storage was needed because the prescriptions with the same medication were dispensed at once. The second problem with the vial-sharing strategy in our hospital was the charge mode. The traditional single-dose charge mode was unsuitable for inpatients who shared the same vial drug with other inpatients. However, paying for the actual quantity of the drug required the medical workers in PIVAS to use up every milligram of the drug in the vial, which was impossible. Next, we came up with the idea of a daily-charge mode for frequently used antibiotics (Figure 3).
As expected, real-time vial-sharing strategies saved a larger amount of drugs, which fluctuated from 31.9% (cefoperazone-sulbactam) to 1.9% (fusidate) and related to the frequency of drug use, the dosage, and the specification. Cefoperazone-sulbactam was the most frequently used antibacterial drug in our hospital. Correspondingly, the amount of saved cefoperazone-sulbactam was significantly higher than in other drugs. Compared with cefoperazone-sulbactam, only 6.1% of cefuroxime was saved, although the consumption of cefuroxime was second among the ten selected drugs. This was due to the dosage of cefuroxime, which does not need further vial-sharing with others. The least saved drug was fusidate because of the minimum clinical use. Amoxicillin-sulbactam was the only drug with a specification of 1500 mg per vial, while most drugs were 500 mg per vial. As a result, more than 51,394 mg of amoxicillin-sulbactam was saved and listed as the third one, which is why specialists call for smaller specifications than larger ones.9 In 2023, amoxicillin-sulbactam with the specification of 500 mg/vial was introduced to Shenzhen Children’s Hospital.
The daily-charge mode was theoretically economical for inpatients and the hospital. However, the fusidate and linezolid in our study witnessed a loss in 2022. The actual consumption of linezolid was 2545 vials, while the number of linezolid paid by patients was only 1559 vials. The reasons were concluded as follows: 1) linezolid was usually prescribed as a temporary order rather than a regular therapeutic medication. As a result, the real-time vial sharing strategy could not be applied. 2) The frequency of linezolid in our hospital was usually prescribed twice a day rather than three times a day. The lower administration frequency of linezolid further diminished the chance of vial-sharing. Although fusidate and linezolid were lost during 2022, the total amount balance of our hospital by combing vial-sharing with daily-charge mode was up to 426,499 yuan. Meanwhile, clinicians reevaluated the clinical utilization rates of fusidate and linezolid and subsequently removed them from the vial-sharing strategy catalog to reduce further possible loss.
Due to differences in the health insurance system, only a few studies in China have studied the economics of vial sharing. In this study, real-time vial sharing was introduced, accompanied by the daily charge mode, to reduce patient’s cost, thus providing a new strategy for those who do not have CSTDs but have a demand for vial-sharing.
Despite the feasibility of the system, this study has a few limitations. Firstly, there is still drug wastage because of inability to collect all drugs from vials, which was defined as systematical consumption. Moreover, drugs prescribed during the different dispensing periods could not achieve vial-sharing to avoid contamination, which might further increase drug wastage. Secondly, manual compounding might lead to professional exposure to antimicrobials.17 Further studies about external contamination of hazardous drugs by vial sharing were necessary. Finally, the daily charge mode was inaccurate and not charged for the actual dose used. The account balance inevitably occurred. The way to manage account balance was debatable.
Conclusion
The use of a real-time vial sharing strategy combined with the daily-rate charge mode resulted in a considerable reduction in drug wastage and patient payments. Our data recommend that medical institutions prioritize scrutinizing drugs in terms of their unit price, frequency of use, prescription dose, and common population dose to determine which medications are appropriate for a real-time vial sharing strategy. Moreover, the actual consumption of drugs should be attended to in case drugs are more prone to be prescribed as temporal orders.
Ethics Statement
This study followed the guidelines outlined in the Declaration of Helsinki and was approved by the Shenzhen Children’s Hospital Ethics Committee. An exemption for informed consent was applied and approved by the Ethics Committee because only clinical data was collected.
Acknowledgment
Guangdong High-level Hospital Construction Fund supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dona D, Barbieri E, Daverio M, et al. Implementation and impact of pediatric antimicrobial stewardship programs: a systematic scoping review. Antimicrob Resist Infect Control. 2020;9(1):3–10. doi:10.1186/s13756-019-0659-3
2. Cho JC, Stovall SH. Need for pediatric antimicrobial stewardship. Am J Health Syst Pharm. 2015;72(5):347. doi:10.2146/ajhp140844
3. Tersigni C, Venturini E, Montagnani C, et al. Antimicrobial stewardship in children: more shadows than lights? Expert Rev Anti Infect Ther. 2019;17(11):871–876. doi:10.1080/14787210.2019.1686355
4. Gopisankar MG, Wahlang J, Jagtap V, et al. Cancer chemotherapy drug wastage in a tertiary care hospital in India-A 3-month prospective and 1-year retrospective study. Br J Clin Pharmacol. 2019;85(10):2428–2435. doi:10.1111/bcp.14064
5. MacBrayne CE, Williams MC, Obermeier H, et al. Anti-infective waste in a pediatric institution: pinpointing problems in the process. Hosp Pharm. 2020;55(4):220–223. doi:10.1177/0018578719844164
6. Smith MJ, Gerber JS, Hersh AL. Inpatient antimicrobial stewardship in pediatrics: a systematic review. J Pediatric Infect Dis Soc. 2015;4(4):e127–35. doi:10.1093/jpids/piu141
7. Liu X, Lu S, Guo W, et al. Antibiotics in the aquatic environments: a review of lakes. China Sci Total Environ. 2018;627:1195–1208. doi:10.1016/j.scitotenv.2018.01.271
8. Baan SD, Geersing TH, Crul M, et al. An economic evaluation of vial sharing of expensive drugs in automated compounding. Int J Clin Pharm. 2022;44(3):673–679. doi:10.1007/s11096-022-01388-6
9. Gilbar PJ, Chambers CR, Musicco F. Preventing drug vial wastage and reducing expenditure associated with injectable cancer drugs: international oncology pharmacy survey. J Oncol Pharm Pract. 2022;28(6):1332–1339. doi:10.1177/10781552211024723
10. Convention, T.U.S.P. USP general 797, in The United States Pharmacopeial; 2021.
11. Liu H, Zou L, Song Y, et al. Cost analysis of implementing a vial-sharing strategy for chemotherapy drugs using intelligent dispensing robots in a tertiary Chinese hospital in Sichuan. Front Public Health. 2022;10:936686. doi:10.3389/fpubh.2022.936686
12. Hall E, Zhang J, Kim EJ, et al. Economics of alternative dosing strategies for pembrolizumab and nivolumab at a single academic cancer center. Cancer Med. 2020;9(6):2106–2112. doi:10.1002/cam4.2888
13. Prasad V, De Jesus K, Mailankody S. The high price of anticancer drugs: origins, implications, barriers, solutions. Nat Rev Clin Oncol. 2017;14(6):381–390. doi:10.1038/nrclinonc.2017.31
14. Gilbar PJ, Chambers CR. How can we ensure value for money from expenditure on injectable cancer drugs? J Oncol Pharm Pract. 2018;24(6):473–476. doi:10.1177/1078155217706195
15. Jang A, Nakashima L, Ng T, et al. A real-world data approach to determine the optimal dosing strategy for pembrolizumab. J Oncol Pharm Pract. 2021;27(3):635–643. doi:10.1177/1078155220929756
16. Gilbar PJ, Chambers CR, Vandenbrouche J, et al. How can the use of closed system transfer devices to facilitate sharing of drug vials be optimised to achieve maximum cost savings? J Oncol Pharm Pract. 2019;25(1):205–209. doi:10.1177/1078155217753890
17. Ml H, T W, Jq Z, et al. Evaluation of external contamination on the vial surfaces of some hazardous drugs that commonly used in Chinese hospitals and comparison between environmental contamination generated during robotic compounding by IV: dispensing robot vs. manual compounding in biological safety cabinet. J Oncol Pharm Pract. 2022;28(7):1487–1498. doi:10.1177/10781552211023571
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.