")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Combining Diamond-Tip Dermabrasion Treatments and Topical Skincare in Participants with Dry, Hyperpigmented, Photodamaged or Acne-Prone/Oily Facial Skin: A Clinical Usage Study
Authors Goberdhan LT, Schneider K, Makino ET, Mehta RC
Received 29 June 2023
Accepted for publication 20 September 2023
Published 25 September 2023 Volume 2023:16 Pages 2645—2657
DOI https://doi.org/10.2147/CCID.S423688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Lisa T Goberdhan, Katie Schneider, Elizabeth T Makino, Rahul C Mehta
SkinMedica; Allergan Aesthetics, an AbbVie Company, Irvine, CA, USA
Correspondence: Katie Schneider, SkinMedica – Allergan Aesthetics, an AbbVie Company, 2525 Dupont Dr, Irvine, CA, 92612, USA, Tel +1 714 246-2573, Email [email protected]
Purpose: An in-office diamond tip microdermabrasion device (DG) was designed to simultaneously exfoliate, extract, and infuse topical cosmetic serums into the skin to improve its appearance. Combining in-office procedures with take-home skincare may enhance treatment outcomes. This study aimed to assess the efficacy of a novel combination of DG treatments with a take-home cosmetic skincare regimen (DGR) to address facial dryness, hyperpigmentation, photodamage, or acne-prone/oily skin.
Patients and Methods: In this 12-week, open-label, single-center study, participants were assigned to 1 of 4 groups according to skin presentation: dry, hyperpigmented, photodamaged, or acne-prone/oily. All participants received 6 bi-weekly DG treatments with tailored DGR topical products. During the DG treatment, the dry, hyperpigmented, photodamaged, and acne-prone/oily groups received hydrating, brightening, antioxidant, and pore-clarifying serums, respectively. Study endpoints included investigator grading, standardized photography, and participant questionnaires.
Results: Sixteen participants aged 22 to 70 years with Fitzpatrick Skin Types I–V completed the study. Immediately after the first DG treatment, significant improvements in dryness, radiance, texture, photodamage, and fine lines were achieved (P< 0.01). At 72 hours, significant improvements were maintained in all these parameters except fine lines (P< 0.05). The DG and DGR combination provided significant long-term improvements at week 12 compared to baseline for dryness, radiance, texture, hyperpigmentation, photodamage, skin tone unevenness, and periocular/perioral fine lines (P< 0.05).
Conclusion: The combination of DG and DGR showed significant immediate and long-term improvements in skin appearance. These results show that the DG and DGR combination is a well-tolerated and effective intervention to enhance different aspects of facial skin quality.
Keywords: microdermabrasion, growth factors, antioxidants, photodamage, brightening, hydrating, DiamondGlow
Introduction
Facial skin quality can decline over time due to the combination of intrinsic chronological aging and extrinsic aging induced by environmental factors, such as exposure to solar radiation, air pollution, and tobacco smoke.1 The combination of these factors results in structural and functional alterations in the skin, leading to changes in its overall appearance. Characteristics of intrinsically aged skin include fine lines and uniform hyperpigmentation. In contrast, extrinsically aged skin, sometimes referred to as photoaged skin, displays coarse wrinkles and mottled hyperpigmentation and may appear rough, sallow, or dry.2
Microdermabrasion is a widely used nonablative skin resurfacing technique that can address several facial skin concerns, including fine lines, photodamage, and hyperpigmentation.3–5 During microdermabrasion procedures, an abrasive component is propelled on the skin’s surface with a simultaneous vacuum to remove debris, causing exfoliation and disruption of the stratum corneum.6 This triggers a cascade of molecular changes that promote dermal and epidermal remodeling, which are thought to lead to the improvements observed in the appearance of aged or damaged skin after microdermabrasion.7,8 The procedure is non-invasive, well-tolerated, and has no associated downtime, making it a popular choice for skin rejuvenation. Moreover, the temporary barrier disruption induced by microdermabrasion can increase the transdermal delivery of topical drugs and cosmetics.9–11 It has been shown that combining microdermabrasion treatments with the application of topical antioxidants can provide greater improvements in skin appearance compared to microdermabrasion alone.12
Combining take-home skincare with in-office facial rejuvenation procedures has been proposed as a means to improve overall patient outcomes. However, no clinical studies have evaluated a tailored daily long-term skincare regimen to complement microdermabrasion. A proprietary crystal-free microdermabrasion device (DG) was designed with a precision diamond-tip handpiece that can simultaneously exfoliate the skin, extract debris, and infuse the skin with cosmetic serums.13 This allows the serums to permeate the skin when the pores are open and the most receptive. It was hypothesized that pre-, inter-, and post-treatment products tailored to particular skin concerns would complement the DG procedure to improve different aspects of skin quality. This study aimed to assess the efficacy and tolerability of a series of bi-weekly DG treatments combined with targeted take-home cosmetic product regimens to improve the appearance of dry, hyperpigmented, photodamaged, or acne-prone/oily skin.
Materials and Methods
Participants
This study was conducted per all applicable guidelines for the protection of human subjects for research as outlined in 21 CFR 50, the accepted standards for Good Clinical Practice (GCP), and consistent with the guidelines in the Declaration of Helsinki. All participants completed the informed consent process before participating in the study and provided permission to have their photos published.
This single-center, open-label study enrolled men and women between the ages of 18–70 years with Fitzpatrick skin types I to VI from a variety of ethnic backgrounds. Eligible participants presented with dry (mild to severe, 1–3 Overall Dryness Scale), hyperpigmented (moderate-severe, 4–9 Overall Hyperpigmentation scale), photodamaged (Moderate-Severe, 4–9 Overall Photodamage Scale), or acne-prone/oily skin (Mild-Moderate, 2–3 Overall Acne Severity Scale) facial skin as determined by clinical examination or self-reported oiliness. Participants had to be willing to abstain from any other topical products (eg, skin lightening, retinoids, benzoyl peroxide, α/β hydroxy acids) on the facial area throughout the 12-week study. If taking hormone replacement or hormones for birth control, they would not need to stop or change their medication for the duration of the study. Participants were also advised to avoid extended periods of sun exposure.
Treatment Regimen
At the baseline visit, participants were assigned to 1 of 4 groups according to skin presentation: dry, hyperpigmented, photodamaged, or acne-prone/oily. Participants in all groups were to receive a series of 6 DG procedures (DiamondGlow®, Allergan Aesthetics, Irvine, CA, USA) every 2 weeks (baseline, week 2, week 4, week 6, week 8 and week 10) during the 12-week evaluation period. The DG treatment consisted of 2 passes across the face with a vacuum setting of 4–5 PSI, and 1 pass on the neck with a vacuum setting of 3–4 PSI. Based on their assigned group, participants received a customized infusion for their in-office DG procedure, customized immediate post-procedure skincare products that were applied to the participant’s face (note: the neck received an application of physical sunscreen [SPF 35] only), and a take-home skincare regimen (DGR) for use during the study (Table 1). The following products have been previously described: HA5,14 TNS A+,15 TNS Recovery,16 LVS day and night,17,18 and LYT2.19 All regimens contained a growth-factor-based serum (TNS A+ or TNS Recovery). The participants were instructed to use the take-home regimen daily as instructed in Table 1, except those that were enrolled in the hyperpigmented and acne-prone/oily groups were advised to stop the use of the provided topical retinol (0.25%)20 3 days prior to receiving each DG treatment, and to resume application of the retinol 3 days after the DG treatment. Unless otherwise indicated, all products were manufactured by SkinMedica (Allergan Aesthetics, Irvine, CA, USA).
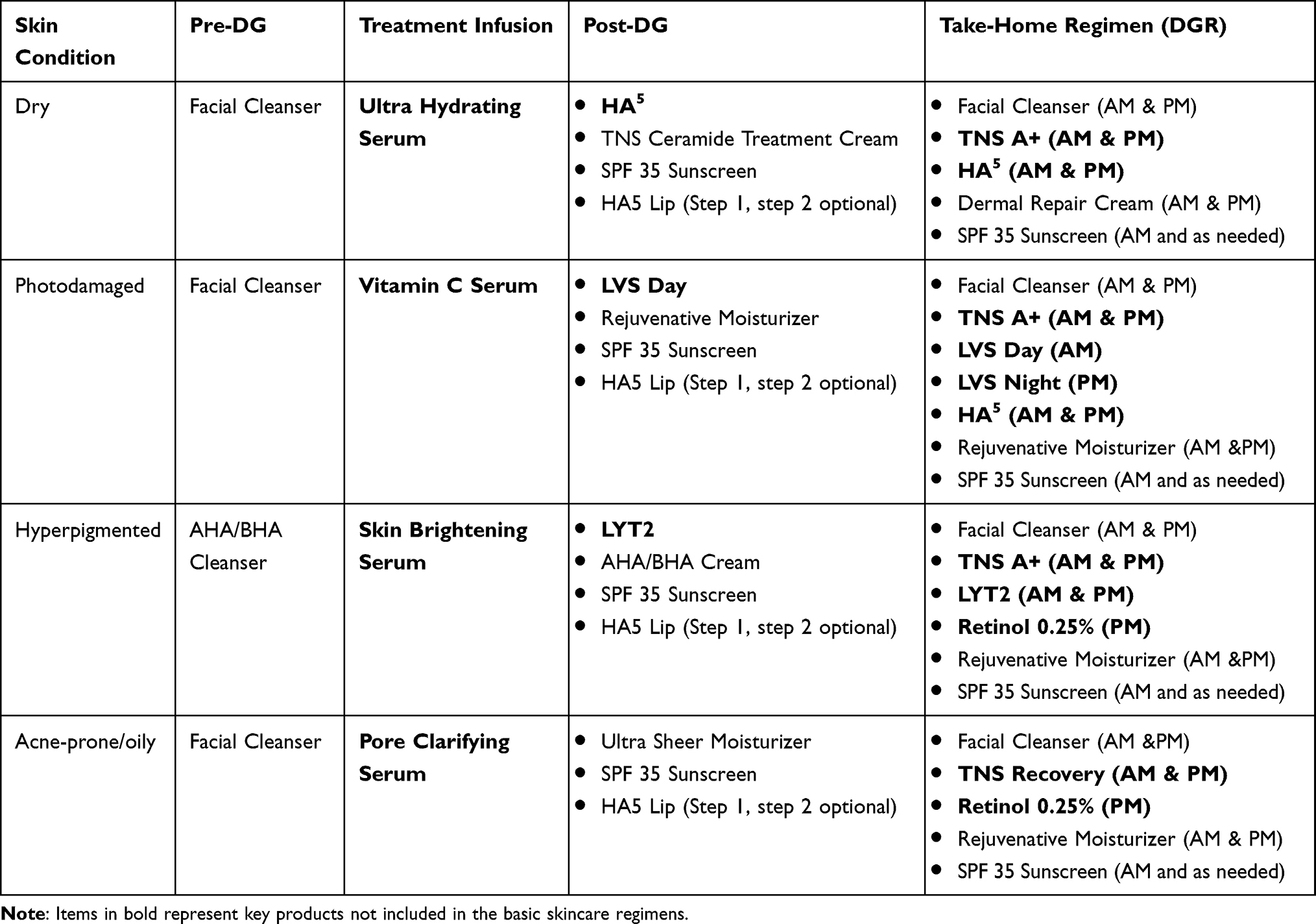 |
Table 1 Treatment Groups and Product Regimen |
Study Assessments
At the beginning of each visit, the face and neck were cleansed, and all makeup was removed at least 15 minutes prior to investigator assessments and photograph acquisition. Live investigator assessments regarding efficacy and tolerability were conducted at the baseline visit (both before and within 15 minutes immediately after the DG treatment) and before each DG treatment at weeks 2, 4, 6, 8, and 10. The following efficacy parameters were assessed using a 10-point grading scale where 0 corresponds to no appearance of the condition, 1–3 is mild, 4–6 is moderate, and 7–9 is severe:
Overall Hyperpigmentation: 0 indicates even skin color with no hyperpigmentation; 9 indicates many large spots with increased pigmentation.
Overall Photodamage: 0 indicates facial skin is smooth to the touch without skin tone unevenness (red/brown), no facial sagging, and significant fine or coarse lines in periocular, cheeks, forehead, or perioral areas; 9 indicates facial skin has significant roughness, skin tone unevenness, may have facial sagging, and shows fine/coarse lines in 3 facial areas.
Skin Tone Unevenness: 0 indicates no red/brown patches or spots, and skin is completely even in color; 9 indicates marked areas of skin tone unevenness.
Radiance: 0 indicates radiant, luminous, or glowing appearance; 9 indicates a dull/matte and/or sallow skin appearance.
Fine Lines/Wrinkles (Forehead, Periocular, Cheeks, Perioral-Individually Assessed): 0 indicates no fine lines/wrinkles present; 9 indicates many fine lines/wrinkles densely packed together in the treatment area.
Coarse Lines/Wrinkles (Forehead, Periocular, Cheeks, Perioral-Individually Assessed): 0 indicates no coarse lines/wrinkles present; 9 indicates many coarse lines/wrinkles densely packed together in the treatment area.
Tactile Roughness: 0 indicates smooth and even feeling skin texture; 9 indicates rough and uneven feeling skin texture.
Additional investigator-graded efficacy and tolerability measures included:
Allergan Skin Roughness Scale21 (0–4 scale): 0 indicates smooth visual skin texture; 4 indicates extremely coarse visual skin texture, deep creases, extreme elastosis.
Overall Dryness/Scaling (0–3 scale): 0 indicates no dryness or scaling; 3 indicates severe with marked roughness.
Clinical Tolerability Assessment for Erythema (0–9 scale): 0 indicates no redness; 9 indicates marked redness.
Immediately post-treatment and at follow-up visits, participants completed the following tolerability assessments:
Burning/Stinging or Itching (0–3 scale): 0 indicates no burning/stinging or itching; 3 indicates marked burning/stinging or itching that causes discomfort and may interrupt daily activities or sleep.
Digital Photography and Skin Imaging
Standardized digital photography and 3D imaging were conducted at all visits using the Canfield VISIA-CR 4.3 Blue® camera system (Parsippany-Troy Hills, NJ). Images were taken from frontal and 45° lateral left and right views with standard 2, cross-polarized, parallel polarized, red channel, and brown channel lighting conditions to document any changes in facial dryness/scaling, hyperpigmentation, photodamage, and acne and/or oiliness.
Miravex Limited, Antera 3D® (Dublin, Ireland) was used to acquire high-resolution 3D images. Triplicate images of the left cheek region were captured for the hyperpigmented and acne-prone/oily groups, while triplicate images of the left cheek and left eye region were captured for the photodamage and dry skin groups.
Participant Self-Assessment Questionnaires
Participants completed self-assessment questionnaires regarding their experience with the DG treatment on the face and neck immediately after the baseline treatment. Additional questionnaires were completed at follow-up visits regarding the DGR products combined with the DG treatments, overall improvement, overall satisfaction, and overall experience with the DG treatments and DGR. Participants were also encouraged to complete a free-text comment section regarding their experience with the DG treatment on the face and neck as well as the DGR products.
Statistical Analysis
All patients that completed at least 1 follow-up visit were included in all analyses. Student’s T-tests were performed using Microsoft Excel and were used to assess any significant changes compared to baseline in investigator-reported parameters. P < 0.05 was deemed statistically significant.
Results
Study Participants
Nineteen women and one man, aged 22–70 years, enrolled in the study and completed the baseline visit (Table 2). The majority were Caucasian (n = 12, 60%), and the most frequent Fitzpatrick skin type was II (n = 6, 30%). At baseline, the 20 enrolled participants were assigned a take-home product regimen (DGR) by skin presentation as dry (n = 4), photodamaged (n = 5), hyperpigmented (n = 7) or acne-prone/oily (n = 4, Table 2). Sixteen participants completed the 12-week study. The 4 participants who did not complete the study were due to a loss to follow-up (n = 1 from acne-prone/oily), non-compliance (n = 1 from acne-prone/oily), requested withdrawal (n = 1 from acne-prone /oily), and a non-related adverse event (n = 1 from photodamaged).
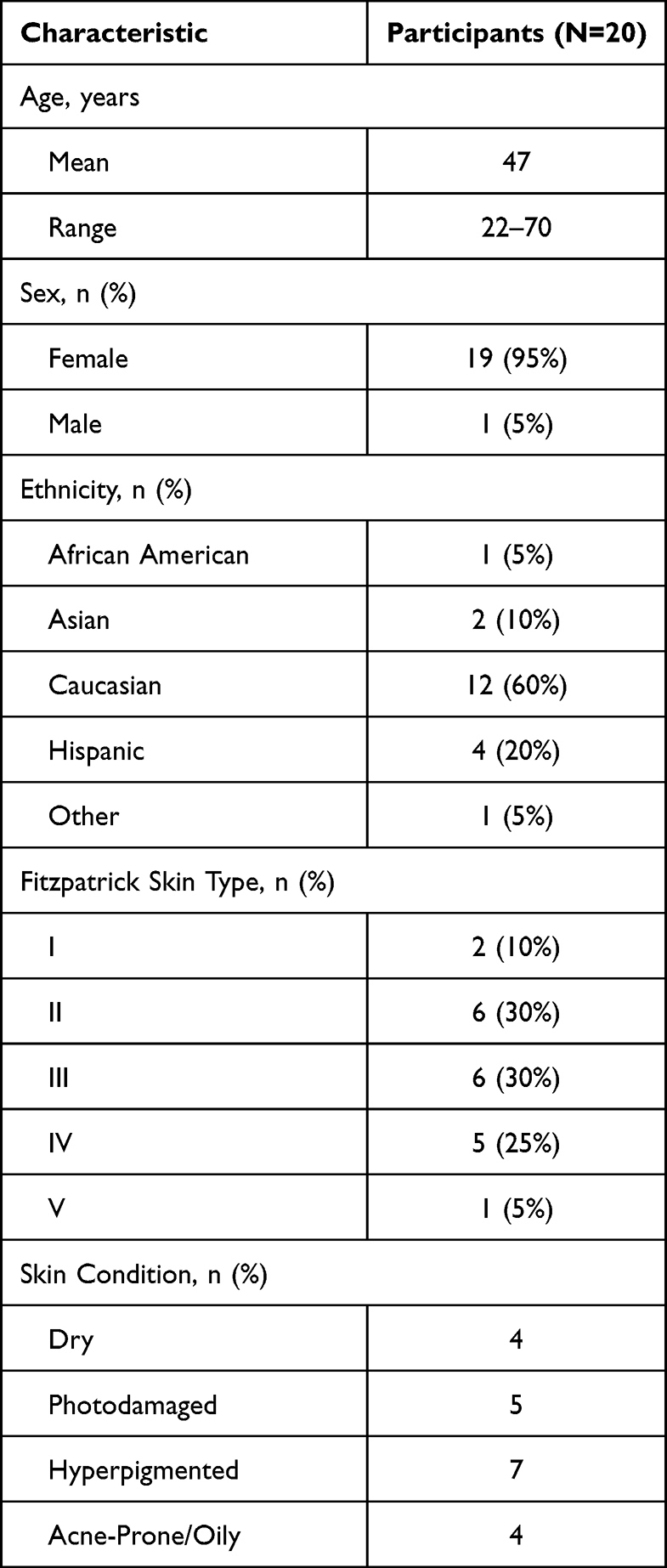 |
Table 2 Participant Demographics and Baseline Disposition |
Efficacy
The instant effects of DG were determined at the baseline visit by comparing the skin after the initial treatment. Immediate significant improvements in overall dryness/scaling, photodamage, visible and tactile roughness, and radiance were observed that persisted for 72 hours after the procedure (P<0.01, Figure 1A). The appearance of forehead, periocular, perioral, and cheek fine lines also showed immediate significant improvements (P<0.01), although these effects lessened after 72 hours (Figure 1B). There was a noticeable reduction in the severity of cheek fine lines but this effect was not significant. However, 2 weeks after the 6th DG treatment, there was a significant, sustained reduction in the severity of perioral and periocular fine lines as compared to baseline (P<0.05, Figure 1B). Benefits on overall hyperpigmentation and skin tone unevenness were seen starting in week 4 (P<0.01, Figure 1C). With continued adherence to DGR, progressive improvements were observed in overall photodamage, overall hyperpigmentation, skin tone unevenness, tactile roughness, and radiance (Figure 1C). Standardized digital photography supports these improvements in multiple different skin types (Figures 2–7).
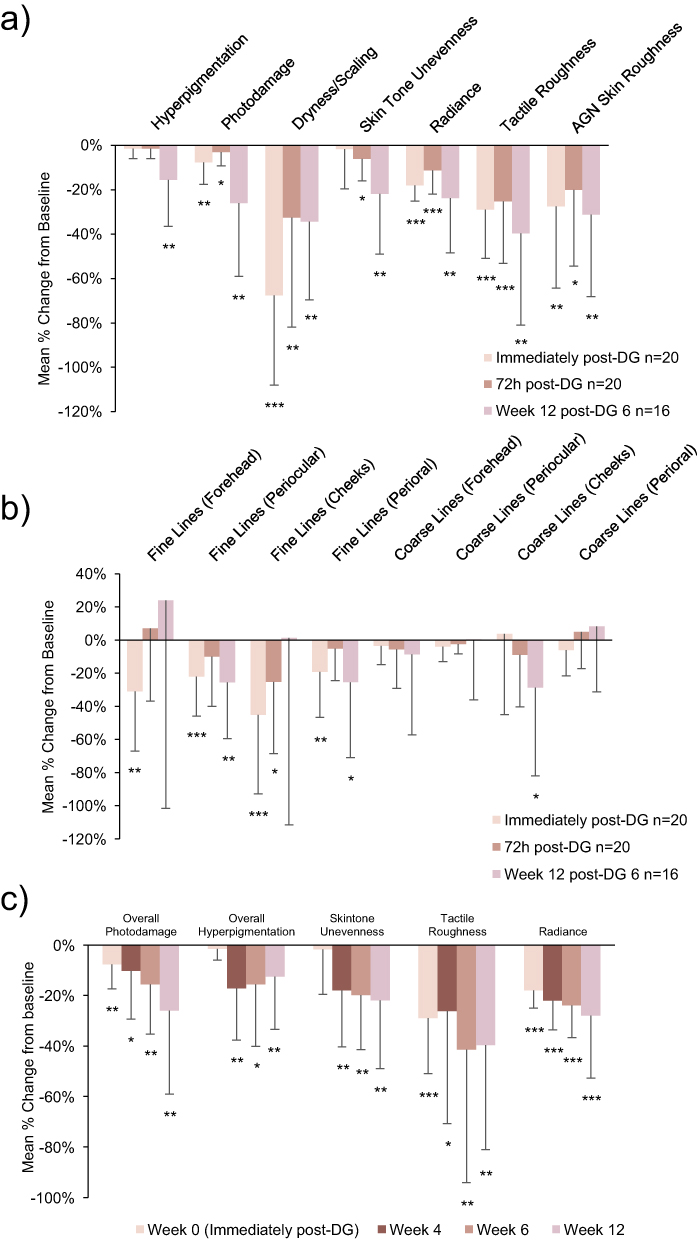 |
Figure 1 Mean percent change from baseline in skin quality attributes as assessed by the investigator with repeated DG treatments and continuous DGR use. (a and b) short and long-term improvements in general attributes (a) and fine and coarse lines (b). (c) Progressive improvements in skin quality. Error bars represent negative SD. P-values were from comparison to baseline using Student’s t-test; *P ≤.05; **P ≤.01; ***P ≤.001. |
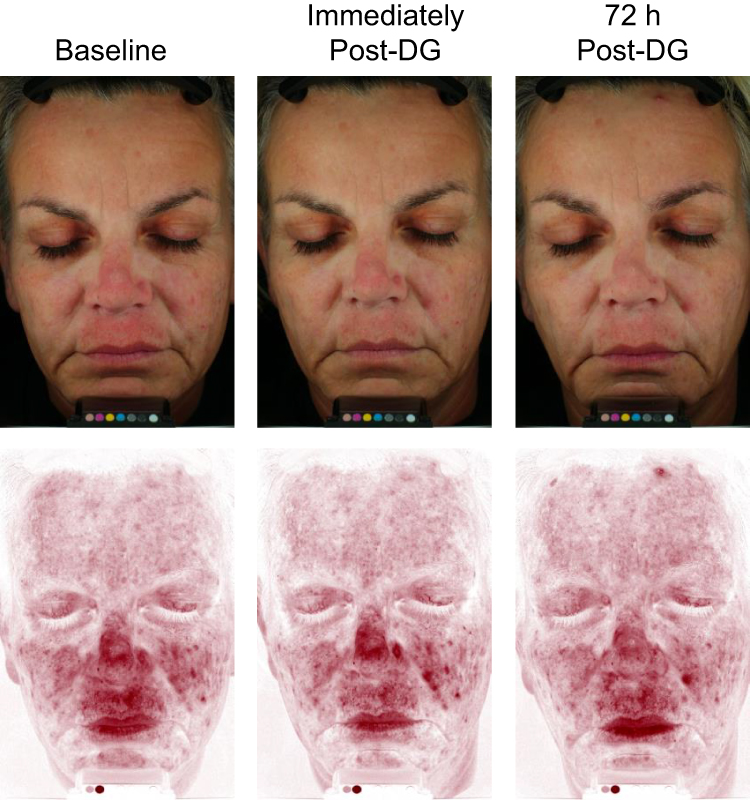 |
Figure 2 Short-term improvements observed in dry skin 72 hours after DG treatment. Participant pictured was a 55-year-old woman with Fitzpatrick Skin Type II. Photographs under cross-polarized lighting (top) or red channel lighting (bottom) showing improvements in visible redness and skin tone unevenness immediately and 72 hours after DG treatment. |
 |
Figure 3 Improvements observed in hyperpigmented skin after 12 weeks of DGR. Participant pictured was a 49-year-old woman with Fitzpatrick Skin Type IV. (a) Photographs under cross-polarized lighting showing improvements in the appearance of dark spots and skin tone unevenness. (b) 3D images showing marked improvements in skin texture and overall discoloration. |
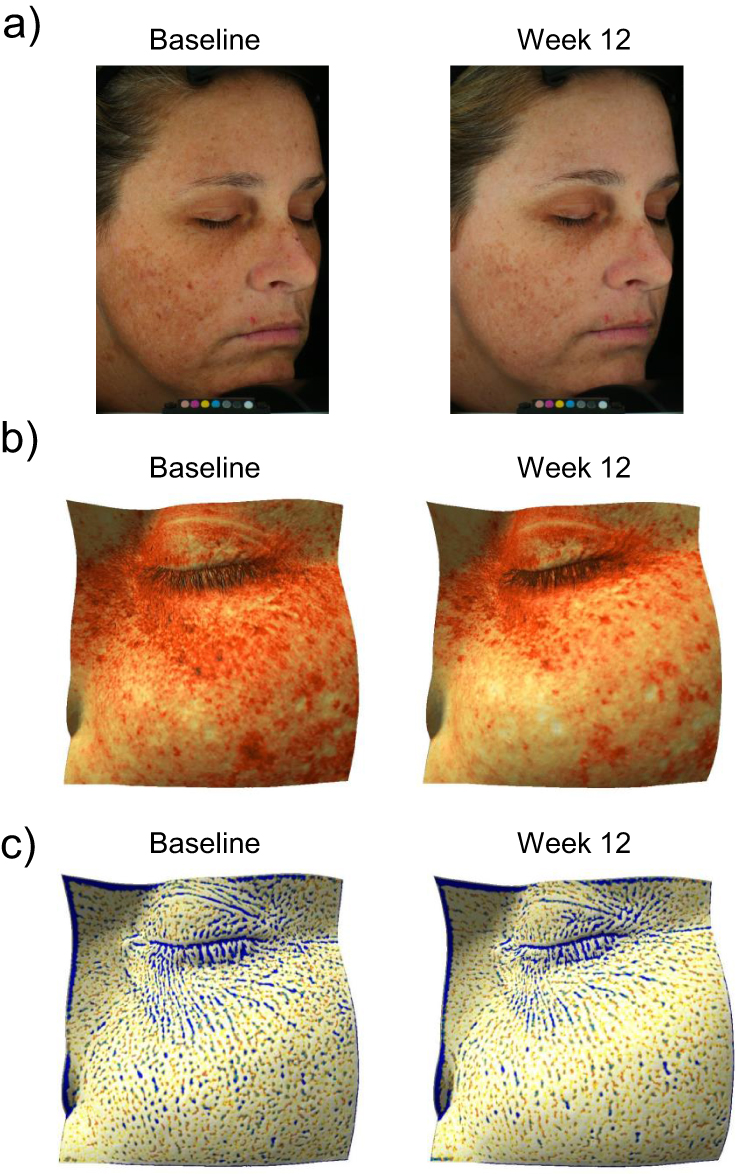 |
Figure 4 Improvements observed in photodamaged skin after 12 weeks of DGR. Participant pictured was a 36-year-old woman with Fitzpatrick Skin Type III. (a) Photographs under cross-polarized lighting showing improvements in overall photodamage, fine lines, discoloration, and texture. (b) 3D images showing reductions in the appearance of dark spots and improvements in skin tone. (c) 3D images showing marked improvements in the appearance of fine lines/wrinkles. |
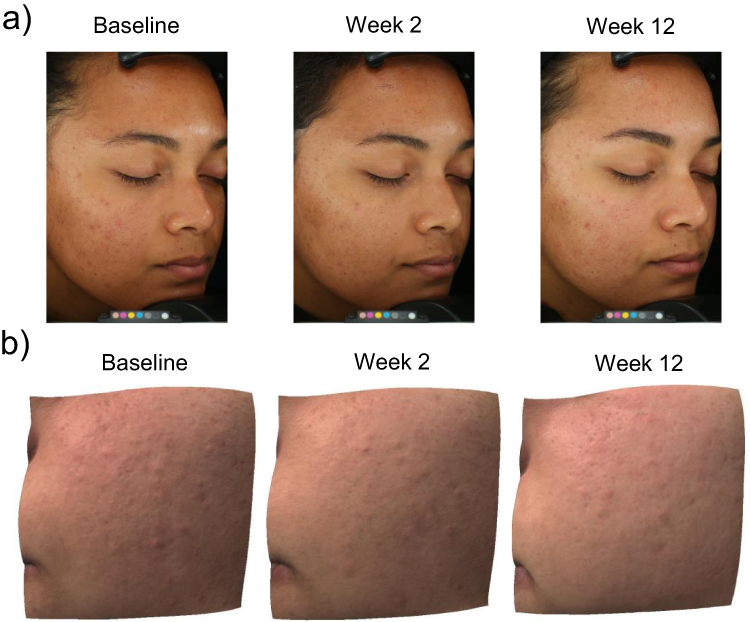 |
Figure 5 Improvements observed in acne-prone/oily skin after 12 weeks of DGR. The participant pictured was a 22-year-old woman with Fitzpatrick Skin Type IV. (a) Photographs under Standard lighting showing improvements in skin texture and skin tone unevenness. (b) 3D images showing visible improvements in skin texture and blemish appearance. |
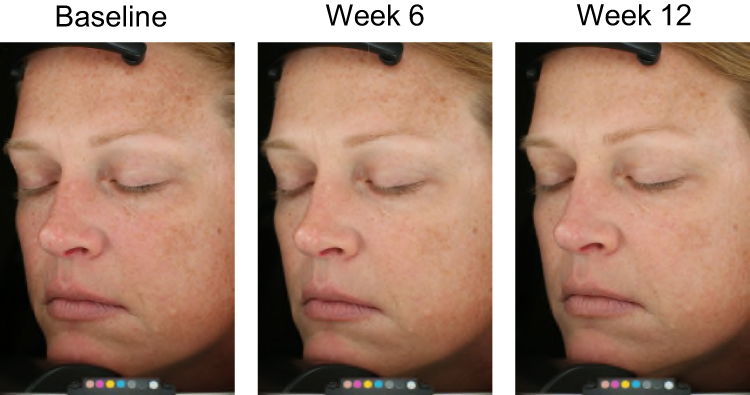 |
Figure 6 Improvements in appearance of hyperpigmented skin after 6 and 12 weeks of DGR. The participant pictured was a 43-year-old woman with Fitzpatrick Skin Type I, under Standard lighting. |
 |
Figure 7 Improvements in appearance of photodamaged skin after 6 and 12 weeks of DGR. The participant pictured was a 48-year-old woman with Fitzpatrick Skin Type I, under parallel-polarized lighting. |
Throughout the study, participant satisfaction consistently remained high. Immediately after the first DG treatment up until week 12, a majority of participants (> 80%) agreed with most questionnaire items regarding self-assessed efficacy (Figure 8). Immediately after the first treatment, 95% of participants agreed or strongly agreed that DG “made me like the way my skin looked after treatment”. At week 12, 82% of participants agreed or strongly agreed that DG “produced short-term results on my skin (1–2 days)”, and 94% agreed or strongly agreed that it “produced long-term results on my skin (3+ days-weeks)”. After 1 or 2 DG treatments with DGR, ≥94% of participants rated their overall satisfaction with the treatments as “excellent” or “good”. After 3 DG treatments + DGR, 100% satisfaction was achieved, which was maintained throughout the 12-week study period.
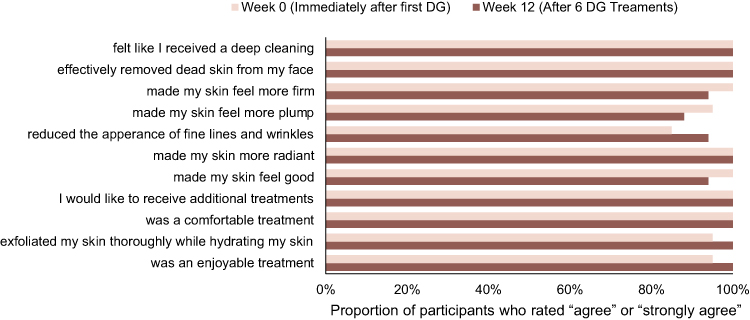 |
Figure 8 Participant self-perceived efficacy and satisfaction immediately after the first DG treatment and after 12 weeks of DGR. |
Safety
The mean tolerability scores for itching, and erythema remained mild or below throughout the 12-week study. Fourteen participants experienced treatment-related adverse events of facial burning/stinging post-DG (n = 5), facial burning/stinging post-DG+DGR (n = 1), DGR-related facial burning and stinging (n = 6), DGR-related raised bumps and discomfort (n = 1), and facial breakout (n = 2). All adverse events were mild, except for 1 instance of moderate facial burning/stinging post-DG + DGR, and 1 instance of DGR-related facial burning due to product getting into eyes. No participants dropped out of the study due to treatment-related adverse events.
Discussion
Both non-invasive procedures and topical skincare products are popular interventions to address facial skin concerns and combining these 2 modalities may lead to improved results and patient satisfaction. The proprietary DG handpiece incorporates concurrent exfoliation from diamond-tip dermabrasion with the targeted delivery of topical products, taking advantage of the temporary disruption of the stratum corneum for enhanced permeation of active ingredients to the epidermis.9,10 This single-center, open-label study showed that combining a customized DG procedure with a targeted take-home skincare regimen leads to significant improvements in multiple aspects of skin quality in individuals with dry, photodamaged, hyperpigmented, or acne-prone/oily skin.
Each DGR consisted of a basic skincare regimen combined with supporting topical products specific to each skin condition that were hypothesized to complement the DG procedure. All regimens contained a growth-factor-based serum (TNS A+ or TNS Recovery) intended for its broad benefits for skin rejuvenation.15,16 The dry skin regimen included HA5 a serum formulated with 5 forms of hyaluronic acid and a blend of ingredients that support healthy hydration and epidermal barrier function.14 The photodamaged DGR contained the LVS dual day/night serum system, consisting of a blend of antioxidants and peptides that defend against extrinsic and intrinsic stressors and support the skin’s reparative processes.18 Hyperpigmented skin received a comprehensive brightening serum, LYT2, that has been shown to reduce hyperpigmentation in many different skin types.19 Finally, the DGR for the acne-prone/oily skin group included nightly retinol to aid with exfoliation, as well as address the appearance of post-inflammatory hyperpigmentation and post-inflammatory erythema that often occur with acne.20,22
Immediate improvements in overall photodamage, skin dryness, roughness, and radiance were observed after a single DG treatment. The improvement in texture is an established benefit associated with microdermabrasion procedures. Diamond-tip dermabrasion has previously been reported to lead to a transient increase in hydration, as measured by skin capacitance, that returned to baseline within 1 day.23 This observation could explain the visible improvements seen here in skin dryness and radiance because both are attributes that reflect overall skin hydration.24 The changes seen in the present study persisted longer than in prior reports, which suggests an additional benefit of the hydrating serum infusion and the accompanying topical regimen in maintaining the short-term visible results from the DG procedure.
Notably, both the investigators and participants observed an immediate reduction in the appearance of fine lines. These immediate effects could be explained by the hydration of keratinocytes from the procedural serum infusions and skincare, as has been histologically observed previously.25 The long-term beneficial effects of microdermabrasion on wrinkles may be attributed to dermal remodeling and increased collagen deposition that occurs over time.6,7 Consistent with this hypothesis, there was a significant and lasting improvement in both periocular and perioral fine lines by week 12. Continued bi-weekly DG treatments accompanied by the targeted take-home product regimens also provided significant long-term improvements in skin dryness, roughness, and radiance. Benefits on overall hyperpigmentation and skin tone unevenness were seen starting in week 4. By both stimulating reorganization of melanin and enhancing the permeability of applied topical brighteners, the DG and DGR combination may be a superior treatment for hyperpigmentation than either treatment alone. Altogether, the DG + DGR regimens produced significant improvements in global skin quality as well as many individual skin quality parameters.
Almost all participants gave high ratings for self-efficacy and satisfaction from the initial treatment onward. Notably, the treatment was well-tolerated among participants; the average tolerability scores for erythema, itching, and burning/stinging remained at mild or below throughout the study, and no participants withdrew from the study due to adverse events. In summary, the DG + DGR treatments provided meaningful improvements in multiple skin quality parameters and high satisfaction from the participants’ perspective.
Limitations of this study include the open-label study design that did not include a control group. This design was chosen because of the known benefits of microdermabrasion and previous studies describing the effects of the targeted topical products. However, any additive or synergistic benefits of DG and the take-home regimens cannot be interpreted. Additionally, the sample size was small and only one male was included. Because of the small sample size, all the participants were pooled into a single group regardless of their customized treatment. Moreover, there was considerable variability in the level of improvement seen for the different skin attributes. To discern significant trends, the data were normalized to baseline to account for the heterogeneity of the initial scores for skin quality parameters. Despite this limitation, the trends observed across skin attributes suggest that the DG regimens can be broadly applicable to any individual seeking to target specific aesthetic concerns or improve overall skin appearance. Further studies should be conducted across multiple centers and in a more diverse population to validate these findings.
Conclusion
This study showed that bi-weekly DG diamond-tip dermabrasion procedures combined with a curated take-home product regimen is a well-tolerated intervention that can address multiple facial skin concerns to improve overall skin appearance and quality. The results presented here highlight the aesthetic benefits and high participant satisfaction that can be gained from combining in-office procedures with targeted topical skincare products.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications.
These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: https://vivli.org/ourmember/abbvie/. Then select “Home.
Ethics Approval
This study was conducted per all applicable guidelines for the protection of human subjects for research as outlined in 21 CFR 50, the accepted standards for Good Clinical Practice (GCP), and consistent with the guidelines in the Declaration of Helsinki. As all products tested were commercially available cosmetics and not investigational drug, biologic, or device products, no IRB approval was required for the study. All participants completed the informed consent process before participating in the study and provided permission to have their photos published.
Acknowledgments
Writing assistance was provided to the authors by Elizabeth Selwan-Lewis, PhD, of AbbVie Inc, and funded by AbbVie Inc. This study was sponsored by Allergan Aesthetics, an AbbVie company.
Disclosure
LT Goberdhan, K Schneider, ET Makino, and RC Mehta are employees of AbbVie, Inc, and may hold AbbVie stock.
References
1. Krutmann J, Bouloc A, Sore G, Bernard BA, Passeron T. The skin aging exposome. J Dermatol Sci. 2017;85(3):152–161. doi:10.1016/j.jdermsci.2016.09.015
2. Farage MA, Miller KW, Elsner P, Maibach HI. Intrinsic and extrinsic factors in skin ageing: a review. Int J Cosmetic Sci. 2008;30(2):87–95. doi:10.1111/j.1468-2494.2007.00415.x
3. Spencer JM, Kurtz ES. Approaches to document the efficacy and safety of microdermabrasion procedure. Dermatol Surg. 2006;32(11):1353–1357. doi:10.1111/j.1524-4725.2006.32305.x
4. El‐Domyati M, Hosam W, Abdel‐Azim E, Abdel‐Wahab H, Mohamed E. Microdermabrasion: a clinical, histometric, and histopathologic study. J Cosmet Dermatol. 2016;15(4):503–513. doi:10.1111/jocd.12252
5. Shim EK, Barnette D, Hughes K, Greenway HT. Microdermabrasion: a clinical and histopathologic study. Dermatol Surg. 2001;27(6):524–530. doi:10.1046/j.1524-4725.2001.01001.x
6. Karimipour DJ, Karimipour G, Orringer JS. Microdermabrasion: an evidence-based review. Plast Reconstr Surg. 2010;125(1):372–377. doi:10.1097/PRS.0b013e3181c2a583
7. Karimipour DJ, Rittié L, Hammerberg C, et al. Molecular analysis of aggressive microdermabrasion in photoaged skin. Arch Dermatol. 2009;145(10):1114–1122. doi:10.1001/archdermatol.2009.231
8. Freedman BM, Rueda-Pedraza E, Waddell SP. The epidermal and dermal changes associated with microdermabrasion. Dermatol Surg. 2001;27(12):1031–1034. doi:10.1046/j.1524-4725.2001.01031.x
9. Zhou Y, Banga AK. Enhanced delivery of cosmeceuticals by microdermabrasion. J Cosmet Dermatol. 2011;10(3):179–184. doi:10.1111/j.1473-2165.2011.00565.x
10. Freedman BM. Hydradermabrasion: an innovative modality for nonablative facial rejuvenation. J Cosmet Dermatol. 2008;7(4):275–280. doi:10.1111/j.1473-2165.2008.00406.x
11. Lee WR, Shen SC, Wang KH, Hu CH, Fang JY. Lasers and microdermabrasion enhance and control topical delivery of vitamin C. J Invest Dermatol. 2003;121(5):1118–1125. doi:10.1046/j.1523-1747.2003.12537.x
12. Freedman BM. Topical antioxidant application enhances the effects of facial microdermabrasion. J Dermatol Treat. 2009;20(2):82–87. doi:10.1080/09546630802301818
13. Makino ET, Huang PC, Emmerich T, Jiang LI, Mehta RC. Efficacy and tolerability of cosmetic serums enriched with five forms of hyaluronic acid as part of biweekly diamond tip microdermabrasion treatments for facial skin dryness and age-associated features. Clin Cosmet Investig Dermatol. 2023;16:1123–1134. doi:10.2147/ccid.s399846
14. Narurkar VA, Fabi SG, Bucay VW, et al. Rejuvenating hydrator: restoring epidermal hyaluronic acid homeostasis with instant benefits. J Drugs Dermatol. 2016;15(1 Suppl 2):s24–37.
15. Naughton GK, Jiang LI, Makino ET, et al. Targeting multiple hallmarks of skin aging: preclinical and clinical efficacy of a novel growth factor-based skin care serum. Dermatology Ther. 2023;13(1):169–186. doi:10.1007/s13555-022-00839-2
16. Mehta RC, Smith SR, Grove GL, et al. Reduction in facial photodamage by a topical growth factor product. J Drugs Dermatol. 2008;7(9):864–871.
17. Makino ET, Jain A, Tan P, et al. Clinical efficacy of a novel two-part skincare system on pollution-induced skin damage. J Drugs Dermatol. 2018;17(9):975–981.
18. Draelos Z, Makino E, Kadoya K, Nguyen A, Jiang L, Mehta R. Clinical benefits of circadian-based antioxidant protection and repair. J Drugs Dermatol. 2020;19(12):1209–1214. doi:10.36849/JDD.2020.5355
19. Makino ET, Kadoya K, Sigler ML, Hino PD, Mehta RC. Development and clinical assessment of a comprehensive product for pigmentation control in multiple ethnic populations. J Drugs Dermatol. 2016;15(12):1562–1570.
20. Babcock M, Mehta RC, Makino ET. A randomized, double-blind, split-face study comparing the efficacy and tolerability of three retinol-based products vs. three tretinoin-based products in subjects with moderate to severe facial photodamage. J Drugs Dermatol. 2015;14(1):24–30.
21. Donofrio L, Carruthers A, Hardas B, et al. Development and validation of a photonumeric scale for evaluation of facial skin texture. Dermatol Surg. 2016;42(1):S219–S226. doi:10.1097/DSS.0000000000000852
22. Leyden J, Stein-Gold L, Weiss J. Why topical retinoids are mainstay of therapy for acne. Dermatology Ther. 2017;7(3):293–304. doi:10.1007/s13555-017-0185-2
23. Kim HS, Lim SH, Song JY, et al. Skin barrier function recovery after diamond microdermabrasion. J Dermatology. 2009;36(10):529–533. doi:10.1111/j.1346-8138.2009.00695.x
24. Humphrey S, Brown SM, Cross SJ, Mehta R. Defining skin quality: clinical relevance, terminology, and assessment. Dermatol Surg. 2021;47(7):974–981. doi:10.1097/DSS.0000000000003079
25. Kirkland EB, Hantash BM. Microdermabrasion: molecular mechanisms unraveled, part 2. J Drugs Dermatol. 2012;11(9):e10–7.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.