Back to Journals » Clinical Ophthalmology » Volume 17
Combined Phacoemulsification and STREAMLINE Surgical System Canal of Schlemm Transluminal Dilation in Eyes of Hispanic Patients with Mild to Moderate Glaucoma
Authors Lazcano-Gomez G ![]() , Antzoulatos GL, Kahook MY
, Antzoulatos GL, Kahook MY
Received 1 March 2023
Accepted for publication 8 June 2023
Published 4 July 2023 Volume 2023:17 Pages 1911—1918
DOI https://doi.org/10.2147/OPTH.S409164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Gabriel Lazcano-Gomez,1,2 George Luis Antzoulatos,1 Malik Y Kahook3
1Department of Glaucoma, Clinica Laser y Ultrasonido Ocular, Puebla City, Puebla, Mexico; 2Hospital Angeles Puebla, Puebla City, Puebla, Mexico; 3Department of Ophthalmology, University of Colorado School of Medicine, Aurora, CO, USA
Correspondence: Malik Y Kahook, Tel +1 720 848 2500, Email [email protected]
Purpose: To characterize clinical outcomes of transluminal dilation of the canal of Schlemm using the STREAMLINE Surgical System combined with phacoemulsification in eyes of Hispanic patients diagnosed with mild to moderate primary open-angle glaucoma.
Methods: This was a prospective analysis of all cases performed and followed up to 12 months. All eyes underwent medication washout preoperatively. Reduction in intraocular pressure (IOP) from unmedicated baseline, as well as medications from pre-washout baseline, were analyzed at postoperative Day 1, Week 1, and Months 1, 3, 6, 9, and 12.
Results: All 37 patients were Hispanic, 83.8% were female, and mean (standard deviation) age was 66.0 (10.5) years. Mean medicated preoperative IOP was 16.9 (3.2) mmHg using a mean of 2.1 (0.9) medications, unmedicated baseline IOP (after washout) was 23.2 (2.3) mmHg, and mean IOP at every postoperative study visit was significantly lower (p< 0.0002). Mean IOP from month 1 through the first postoperative year ranged from 14.7– 16.2 mmHg, representing a reduction of 7.0– 8.5 mmHg (30.7– 36.5%). At month 12, 80% of all eyes (28/35) and 77.8% of medication-free eyes (14/18) had IOP reduction ≥ 20% from unmedicated baseline, and 51.4% of eyes (18/35) were medication-free. Mean medication use was significantly reduced (by 59.9– 74.6%, p< 0.0001) at every postoperative study visit. The only adverse event occurring in > 1 eye was high IOP (n=4) which was responsive to topical medical therapy; no adverse events were attributed to the transluminal dilation procedure.
Conclusion: Transluminal dilation of the canal of Schlemm using the STREAMLINE Surgical System combined with phacoemulsification safely and effectively reduced both IOP and dependence on IOP-lowering medications in a Hispanic population diagnosed with POAG and should be considered at the time of phacoemulsification in Hispanic patients who have a need for IOP reduction, medication reduction, or both.
Keywords: glaucoma, intraocular pressure, STREAMLINE surgical system, goniotomy, viscodilation
Introduction
The past decade has seen a significant expansion of surgical options for the management of glaucoma. Novel bleb-based subconjunctival filtering procedures, trabecular meshwork (TM) bypass procedures, suprachoroidal filtration procedures, and viscodilation procedures of the canal of Schlemm have all been developed and evaluated for the treatment of various forms of glaucoma.1–3 The impetus for this innovation is the desire for a glaucoma procedure that can achieve therapeutic goals without the risks of traditional trabeculectomy or tube-shunt surgeries.4,5
The TM is considered the primary site of aqueous humor outflow obstruction leading to elevated intraocular pressure (IOP) and the development of glaucomatous optic neuropathy.6,7 In glaucomatous eyes, additional outflow resistance is found distal to the TM, in the canal of Schlemm and collector channels.8,9 Various techniques for transluminal dilation of the canal of Schlemm have been developed as a means of enhancing outflow in post-TM structures.
The STREAMLINE™ Surgical System (New World Medical, Rancho Cucamonga, CA) is an FDA-cleared instrument for delivering small volumes of viscoelastic during ocular surgery. The single-use, disposable instrument consists of a polymer handset tipped with a surgical grade stainless-steel cannula comprised of a long thin neck that accesses the TM through a clear corneal incision. An actuator button on the handset, when depressed, retracts a polymer outer sleeve to facilitate positioning of the inner cannula into the canal of Schlemm and allowing the internal pump to deliver a small amount of ophthalmic viscoelastic fluid (approximately 7 uL per actuation). The product is designed to provide a maximum of 8 total deliveries of ophthalmic viscoelastic. The procedure can be performed either as a standalone surgery or in combination with cataract surgery.
Glaucoma related-health disparities exist in the Hispanic population. Glaucoma is a leading cause of blindness in Hispanics.10 Its prevalence is approximately twice as common in Hispanics compared with whites, and increases more rapidly with age than any other ethnic group.11 Hispanics are less likely to undergo glaucoma testing12 and less likely to be treated for glaucoma than whites.13
In this report, we characterize 12-month efficacy and safety of transluminal dilation of the canal of Schlemm using the STREAMLINE Surgical System combined with cataract surgery in eyes of Hispanic patients diagnosed with mild to moderate primary open-angle glaucoma (POAG).
Methods
This was a 12-month prospective, interventional case series conducted at a single center in Mexico (two sites were activated but only one enrolled subjects). The study protocol and the consent form underwent review and approval by the Comites de Investigacion y Etica en Investigacion del Hospital Angeles Puebla. All participants provided written informed consent to enter the study. The trial was registered on www.ClinicalTrials.gov (NCT04700189) and conducted in accordance with the tenets of the Declaration of Helsinki. Reasonable requests for sharing of deidentified data will be considered by the investigators.
Subjects were eligible to participate if they were at least 22 years old, with mild to moderate POAG in one or both eyes, under treatment with at least 1 and up to 3 topical glaucoma medications and scheduled to undergo elective cataract surgery. One subject was previously classified in an interim report as having severe POAG.14 Analysis of visual field testing at the time of writing this article established that a classification of moderate glaucoma was more appropriate and the patient was reclassified accordingly. Prior to surgery, IOP-lowering medication washout was undertaken, and subjects whose preoperative unmedicated IOP was between 21–36 mmHg, inclusive, were enrolled. Exclusion criteria comprised women with the potential to become pregnant, patients with closed or potentially occludable angles, advanced glaucoma (visual field mean deviation worse than −12 dB; sensitivity less than or equal to 10 dB in two or more of the four central test points; cup-disc ratio greater than 0.8; inability to safely undergo IOP-lowering medication washout, any recent intraocular surgery (within the six months preceding study entry) or laser surgery in the three months prior (or any prior history of laser iridotomy), best-corrected visual acuity (BCVA) worse than 20/80 in either eye, or recent ocular inflammation or infection in the preceding six months.
Potential participants received a full ocular examination including recording of prior medical and ocular history, BCVA, examination of the anterior and posterior segments, IOP measurement with Goldmann tonometry (mean of 2 measurements or 3 if the first 2 differed by more than 3 mmHg), gonioscopy, and automated visual field assessment. Qualifying subjects ceased using IOP-lowering medications for a washout period (a minimum of 28 days for prostaglandin analogues and beta-blockers, 14 days for alpha agonists, and 5 days for miotics and carbonic anhydrase inhibitors; washout of combination products was based on the component with the longer washout). Unmedicated baseline IOP was established after completion of the washout. If both eyes met eligibility criteria, the study eye was the eye with higher baseline unmedicated IOP (or, if equal, the right eye was the study eye). The surgical procedure is described below. Postoperatively, subjects were reassessed at 1 day, 1 week, and 1, 3, 6, 9, and 12 months after surgery. At all visits, IOP-lowering medication use, BCVA, IOP, and anterior segment examination were recorded; at months 3 and 12, gonioscopy and posterior segment examination were repeated.
All glaucoma procedures were performed by a single surgeon. The transluminal dilation procedure was performed as described in the manufacturer’s instructions for use15 and followed cataract extraction by phacoemulsification cataract surgery and intraocular lens implantation. Before use, the device was loaded with ophthalmic viscoelastic fluid. Head and microscope position were adjusted such that the patient’s head was tilted 45° from the surgeon and the microscope tilted 45° toward the surgeon. Using intraoperative gonioscopy for visualization, the STREAMLINE Surgical System device tip was advanced through the phacoemulsification incision to the nasal drainage angle. The device’s outer sleeve was placed adjacent to the TM without indenting the anterior wall of the canal. The actuator button was depressed, which retracted the outer sleeve and positioned the inner cannula within the canal of Schlemm and held for 2 seconds to deliver viscoelastic fluid into the canal. The device’s tip was then removed from the TM, the actuator button was released, and the procedure repeated over several clock hours of the drainage angle until 5–8 applications were administered per eye. Postoperatively, a fixed combination of prednisolone and either gatifloxacin or tobramycin was prescribed for use every 2 hours with a 4-week taper.
The study’s primary outcome was the percentage of eyes with IOP reduction of 20% or greater from baseline to month 12. Other outcome measures were the mean change from post-washout baseline in IOP and the mean change from pre-washout screening in IOP-lowering medication use. All outcomes were analyzed by two-tailed paired t-tests with alpha of 0.05 taken as the level of significance. The percentage of eyes achieving target IOP of less than 18 mmHg and less than 15 mmHg, as well as the percentage of eyes using fewer medications and no medications, were calculated at the 12-month time point. Safety assessment was characterized by tabulating the incidence of intra- and postoperative adverse events. Consistent with first-in-human trials, the analyses undertaken in this study were exploratory and not intended to test any prespecified hypotheses. Therefore, an arbitrary sample size was enrolled to ensure adequate estimation of the primary outcome.
Results
A total of 37 eyes of 37 patients were included in this analysis. Demographic and glaucoma status data are shown in Table 1. All 37 patients were Hispanic, 83.8% were female, and mean (standard deviation) age was 66.0 (10.5) years. All had POAG, which was mild (70.3%) or moderate (29.7%), and approximately equal numbers of patients were using 1, 2, or 3 medications at the time of washout.
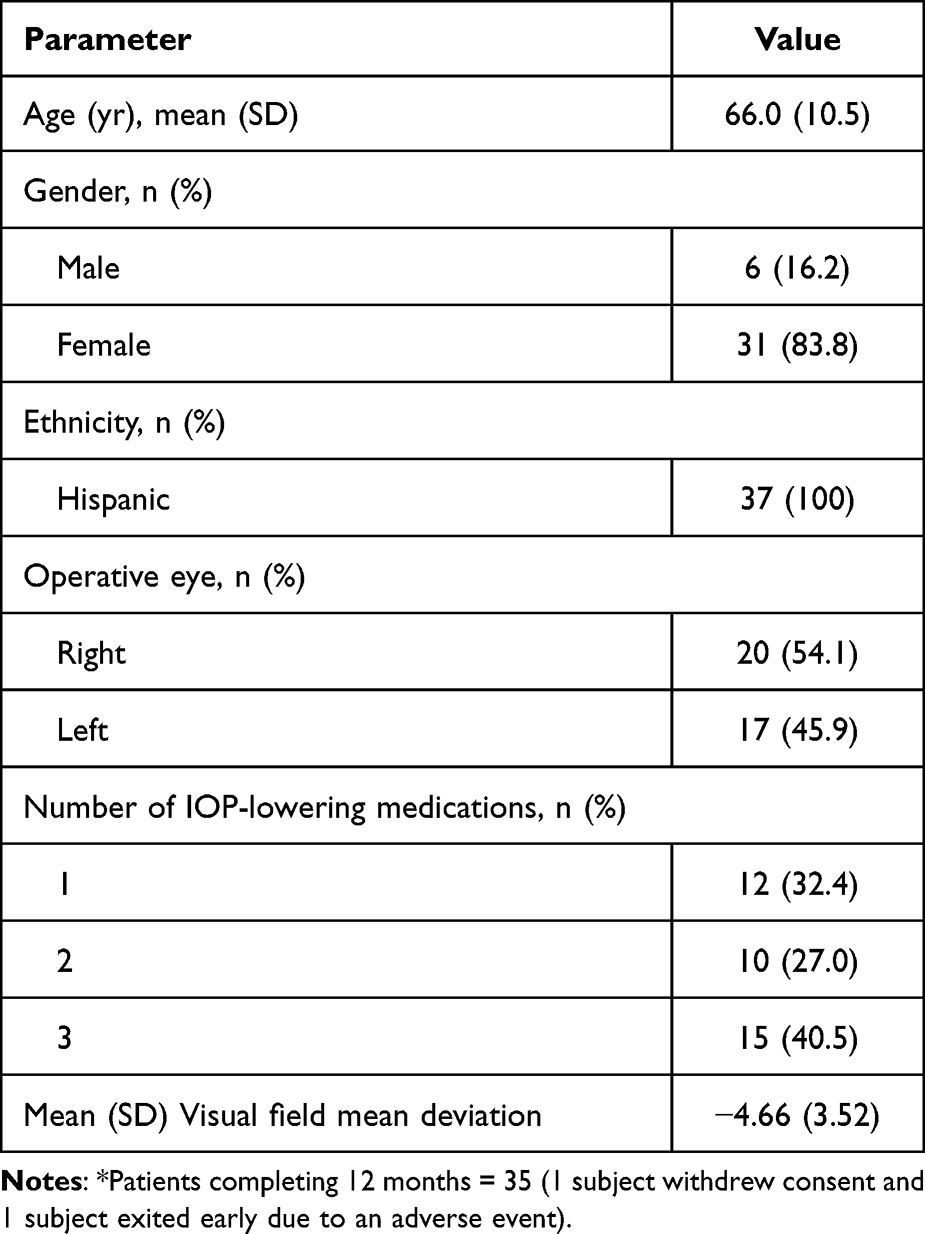 |
Table 1 Demographic and Baseline Glaucoma Status Data for the Study Sample (n=37*) |
Figure 1 illustrates the distribution of IOP reduction at month 12, with 28 eyes (80%) reaching an IOP reduction from baseline of 20% or greater and nearly half of eyes (48.6%; 17/35) reaching an IOP reduction of 30% or greater. Among the 18 eyes using no medications at month 12, the responder analysis was very similar (Figure 1), and 77.8% achieved an IOP reduction ≥20% at month 12. Mean IOP data at each time point are given in Table 2. Mean IOP was 16.9 (3.2) mmHg at screening and increased to 23.2 (2.3) after washout of all IOP-lowering medications. Postoperatively, mean IOP was significantly reduced (p≤0.0002) at all time points. Mean IOP at the first postoperative day was 15.0 (3.9) mmHg, a reduction of 8.2 mmHg from baseline, and at week 1 was 18.4 (6.5) mmHg. Mean IOP from month 1 through month 12 ranged from 14.7–16.2 mmHg, representing mean IOP reductions of 7.0–8.5 mmHg (p<0.0001 at all time points) and percent IOP reductions of 30.2–36.5%. At month 12 (n=35), mean IOP was 16.2 (2.2) mmHg, a reduction of 7.0 mmHg (30.2%) from post-washout baseline. IOP ≤18 mmHg was achieved in 85.7% of eyes (29/35), and IOP ≤ 15 mmHg was achieved in 28.6% of eyes (10/35) at month 12.
 |
Table 2 Mean Intraocular Pressure (IOP) and Medication Use and Changes from Baseline at Each Study Time Point. Baseline for IOP Was After Medication Washout, While Baseline for Medications Was Before Washout |
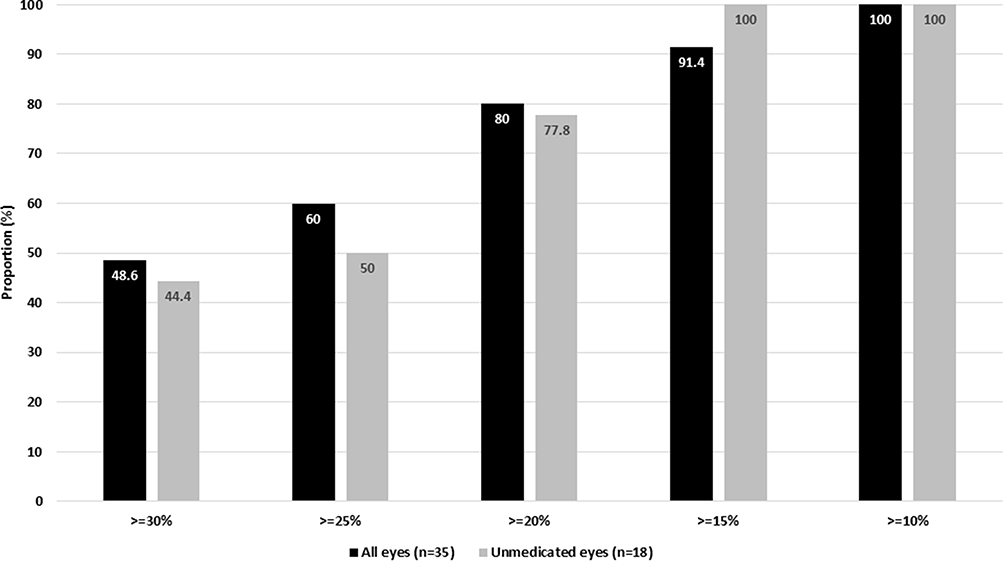 |
Figure 1 Responder analysis of percent reduction in intraocular pressure at 12 months in all eyes and those unmedicated at month 12. |
Mean medication use data at each time point are given in Table 2. The mean number of medications per eye was 2.1 (0.9) at screening baseline. Postoperatively, mean medication use was significantly reduced (p<0.0001) from screening baseline at all time points. Mean medication use was low at postoperative day 1 and week 1, with 1 and 3 eyes, respectively, requiring medications at these visits. At month 12 (n=35) the number of medications used was 0.8 (a reduction of 1.3 medications or 60.5% from pre-washout baseline), 51.4% of eyes (18/35) were medication-free, and 71.4% (25/35) were using fewer medications than preoperatively, and all but one eye (34/35, 97.1%) were using the same or fewer medications. Mean medication use from month 1 through month 12 ranged from 0.5–0.8 medications, representing a reduction of 1.2–1.6 medications (p<0.0001) at all time points and percent medication reduction of 59.9–74.6%.
The procedure was safe and well tolerated in all eyes. There were no adverse events attributable to the transluminal dilation procedure or the STREAMLINE Surgical System device. The only adverse event occurring in more than 1 eye was high IOP (n=4). All of these were responsive to short-term topical medical therapy. Adverse events occurring in only single patients included choroidal detachment, cortical remnants in the visual axis, predisposing lesion in the retina, dry eye, red eye, conjunctivitis, skin infection, and corneal abrasion. One patient experienced an accidental chemical exposure to the face during the first postoperative week leading to study withdrawal. A single serious adverse event, posterior capsule rupture, was not attributable to the STREAMLINE procedure or device. Mean endothelial cell density showed a slight mean reduction by month 3 that remained stable thereafter, with a 16.8% reduction seen at month 12 (Figure 2).
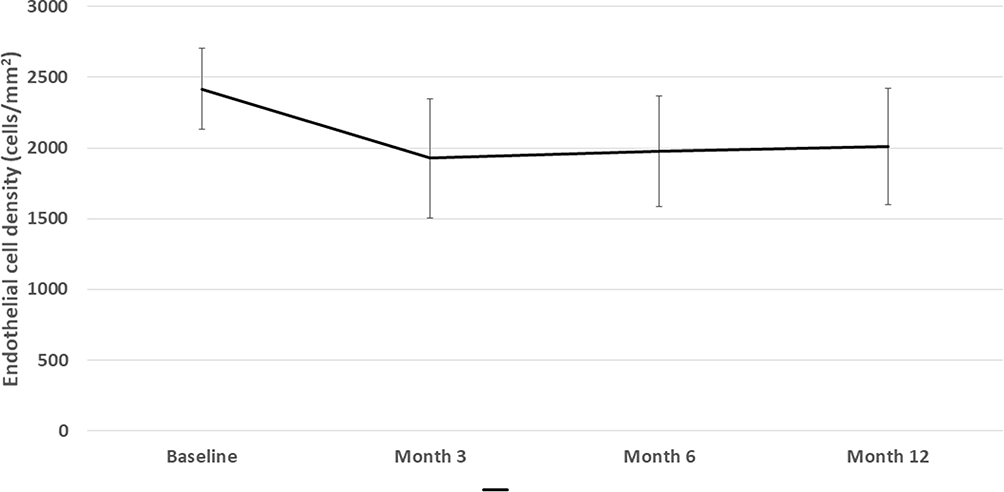 |
Figure 2 Endothelial cell density over time. Error bars represent standard deviation. |
Discussion
In this first-in-human case series, transluminal dilation of the canal of Schlemm using the STREAMLINE Surgical System, combined with phacoemulsification, safely and significantly decreased both IOP and the need for IOP-lowering medications. Mean IOP was reduced by 30.2% and medication use by 60.5% at 12 months, with 80% of eyes achieving a ≥20% IOP reduction from baseline and more than half (51.4%) were medication-free.
These results compare favorably with 6-month outcomes previously reported in a subset of the current study population.14 In that interim analysis, mean IOP reduction at 6 months was 36.9%, with 89.5% of eyes achieving a ≥20% reduction in IOP from baseline; medication use was reduced by 49.1%, and 42.1% of eyes were medication-free. Comparing these values with those observed in the current 12-month analysis, the procedure’s efficacy remained consistent between 6 and 12 months. Comparing these results with other MIGS procedures is made challenging by significant differences in study designs within the MIGS literature. Some devices have undergone prospective randomized trials for regulatory approval while others have been cleared via the 510(k) pathway in which randomized trials are not required. Also, some studies have implemented washout IOP assessments at study entry and at the primary time point of interest, while others have not. With these caveats in mind, the results obtained with the STREAMLINE Surgical System compare favorably with outcomes of randomized clinical trials evaluating phacoemulsification combined with TM bypass devices16–19 and with outcomes of other transluminal dilation procedures20–30 (Table 3).
 |
Table 3 Comparison of Outcomes in the Current Study Compared with Those Reported in Studies of Trabecular Meshwork Bypass Devices and Other Transluminal Dilation Procedures in Combination with Phacoemulsification |
The primary outcome of this study was the proportion of eyes with IOP reduction ≥20% from post-washout baseline at month 12. This was achieved in 80% of eyes. Of note, nearly half of eyes (48.6%) achieved an IOP reduction from baseline of ≥30%. Also of note, all eyes manifested at least a 10% reduction in IOP (Figure 1). This is significant given that the pre-washout IOP of the study population was 16.9 mmHg, suggesting that medication reduction was an important individualized goal for some eyes. Such a decrease in medication—71.4% of eyes were on fewer medications at month 12 than at baseline and more than half (51.4%) were medication-free—was achieved without a rise in IOP compared with unmedicated baseline in any eye. This was accomplished with a favorable safety profile similar to other angle-based IOP lowering procedures summarized in Table 3. The slight mean change in ECD was seen by month 3 and remained stable thereafter (Figure 2) similar to what is seen with phacoemulsification alone. The magnitude of this change—16.8% at month 12—is somewhat similar to what has been reported for phacoemulsification alone in the control arms of recent combined MIGS trials (~9–12%)18,31–33 and consistent with outcomes of combined MIGS-phacoemulsification (13–15.5%)18,34,35 allowing for differences in study populations. Importantly, there was no progressive reduction in ECD over time illustrating safety of this approach for long-term corneal endothelial health.
This report complements the interim analysis14 by adding more eyes and longer-term data to this first-in-human study. The study’s strengths include a prospective design, the use of a standard primary outcome measure (≥20% IOP reduction from baseline), and a medication washout preoperatively to more robustly characterize surgical IOP reduction. An additional strength is the inclusion of a uniformly Hispanic subject sample. As discussed in the Introduction, multiple glaucoma-related health disparities and health-care disparities exist in the Hispanic population.10–13 However, when treated, outcomes in Hispanics are typically similar to those of other ethnicities.36–38 Limitations include a relatively small sample size, which is appropriate for first-in-human studies. Also, the study duration is short relative to the chronic lifelong nature of glaucoma; however, intermediate-term data are of value to surgeons when selecting from among the various glaucoma procedures available. Further, the inclusion of a single surgeon limits generalizability of results. An additional limitation is the lack of a phacoemulsification-only control group, as phacoemulsification alone is known to reduce both IOP and the need for IOP-lowering medications in glaucomatous eyes.39 However, the reduction in IOP and medications observed at 12 months in this study exceed what would be expected from phacoemulsification alone, supporting the additive advantage of this combination procedure. Finally, while baseline IOP was assessed after medication washout, 12-month IOP outcomes were not.
Conclusion
In summary, canal of Schlemm transluminal dilation at the time of cataract extraction safely and effectively reduced IOP and the need for IOP-lowering medications by both clinically and statistically significant magnitudes in eyes of Hispanic patients with medically controlled mild to moderate POAG.
Disclosure
Dr Malik Y Kahook is a consultant to New World Medical and his university receives fees on his behalf for this consultancy. In addition, Dr Kahook has a patent (No. 10,729,584) issued related to STREAMLINE Surgical System technology and a patent US 2021/0322218 A1 owned by New World Medical. Funding for the conduct of this study was provided by New World Medical. The authors report no other conflicts of interest in this work.
References
1. Lim R. The surgical management of glaucoma: a review. Clin Exp Ophthalmol. 2022;50:213–231. doi:10.1111/ceo.14028
2. Birnbaum FA, Neeson C, Sola-Del Valle D. Microinvasive glaucoma surgery: an evidence-based review. Semin Ophthalmol. 2021;36(8):772–786. doi:10.1080/08820538.2021.1903513
3. Pereira ICF, van de Wijdeven R, Wyss HM, Beckers HJM, den Toonder JMJ. Conventional glaucoma implants and the new MIGS devices: a comprehensive review of current options and future directions. Eye. 2021;35:3202–3221. doi:10.1038/s41433-021-01595-x
4. Gedde SJ, Feuer WJ, Lim KS, et al. Treatment outcomes in the primary tube versus trabeculectomy study after 3 years of follow-up. Ophthalmology. 2020;127:333–345. doi:10.1016/j.ophtha.2019.10.002
5. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153:804–814. doi:10.1016/j.ajo.2011.10.024
6. Grant WM. Experimental aqueous perfusion in enucleated human eyes. Arch Ophthalmol. 1963;69:783–801. doi:10.1001/archopht.1963.00960040789022
7. Maepea O, Bill A. Pressures in the juxtacanalicular tissue and Schlemm’s canal in monkeys. Exp Eye Res. 1992;54:879–883. doi:10.1016/0014-4835(92)90151-H
8. Allingham RR, de Kater AW, Ethier CR. Schlemm’s canal and primary open angle glaucoma: correlation between Schlemm’s canal dimensions and outflow facility. Exp Eye Res. 1996;62:101–109. doi:10.1006/exer.1996.0012
9. Battista SA, Lu Z, Hofmann S, Freddo T, Overby DR, Gong H. Reduction of the available area for aqueous humor outflow and increase in meshwork herniations into collector channels following acute IOP elevation in bovine eyes. Invest Ophthalmol Vis Sci. 2008;49:5346–5352. doi:10.1167/iovs.08-1707
10. Rodriguez J, Sanchez R, Munoz B, et al. Causes of blindness and visual impairment in a population-based sample of U.S. Hispanics. Ophthalmology. 2002;109:737–743. doi:10.1016/S0161-6420(01)01008-9
11. Kapetanakis VV, Chan MP, Foster PJ, Cook DG, Owen CG, Rudnicka AR. Global variations and time trends in the prevalence of primary open angle glaucoma (POAG): a systematic review and meta-analysis. Br J Ophthalmol. 2016;100:86–93. doi:10.1136/bjophthalmol-2015-307223
12. Stein JD, Talwar N, Laverne AM, Nan B, Lichter PR. Racial disparities in the use of ancillary testing to evaluate individuals with open-angle glaucoma. Arch Ophthalmol. 2012;130(12):1579–1588. doi:10.1001/archophthalmol.2012.1325
13. Stein JD, Ayyagari P, Sloan FA, Lee PP. Rates of glaucoma medication utilization among persons with primary open-angle glaucoma, 1992 to 2002. Ophthalmology. 2008;115(8):1315–9, 9 e1. doi:10.1016/j.ophtha.2007.12.017
14. Lazcano-Gomez G, Garg SJ, Yeu E, Kahook MY. Interim analysis of STREAMLINE((R)) surgical system clinical outcomes in eyes with glaucoma. Clin Ophthalmol. 2022;16:1313–1320. doi:10.2147/OPTH.S358871
15. New World Medical. Streamline Surgical System Instructions for Use. Rancho Cucamonga, CA: New World Medical; 2021.
16. Samuelson TW, Katz LJ, Wells JM, Duh YJ, Giamporcaro JE. Randomized evaluation of the trabecular micro-bypass stent with phacoemulsification in patients with glaucoma and cataract. Ophthalmology. 2011;118:459–467. doi:10.1016/j.ophtha.2010.07.007
17. Ahmed IIK, Fea A, Au L, et al. A prospective randomized trial comparing Hydrus and iStent microinvasive glaucoma surgery implants for standalone treatment of open-angle glaucoma: the COMPARE study. Ophthalmology. 2020;127:52–61. doi:10.1016/j.ophtha.2019.04.034
18. Samuelson TW, Sarkisian SR Jr, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126:811–821. doi:10.1016/j.ophtha.2019.03.006
19. Samuelson TW, Chang DF, Marquis R, et al. A schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: the HORIZON study. Ophthalmology. 2019;126:29–37. doi:10.1016/j.ophtha.2018.05.012
20. Hughes T, Traynor M. Clinical results of ab interno canaloplasty in patients with open-angle glaucoma. Clin Ophthalmol. 2020;14:3641–3650. doi:10.2147/OPTH.S275087
21. Ondrejka S, Korber N. 360 degrees ab-interno Schlemm’s canal viscodilation in primary open-angle glaucoma. Clin Ophthalmol. 2019;13:1235–1246. doi:10.2147/OPTH.S203917
22. Tracer N, Dickerson JE Jr, Radcliffe NM. Circumferential viscodilation ab interno combined with phacoemulsification for treatment of open-angle glaucoma: 12-month outcomes. Clin Ophthalmol. 2020;14:1357–1364. doi:10.2147/OPTH.S252965
23. Gillmann K, Aref A, Niegowski LJ, Baumgartner JM. Combined ab interno viscocanaloplasty (ABiC) in open-angle glaucoma: 12-month outcomes. Int Ophthalmol. 2021;41:3295–3301. doi:10.1007/s10792-021-01891-1
24. Kazerounian S, Zimbelmann M, Lortscher M, Hommayda S, Tsirkinidou I, Muller M. Canaloplasty ab interno (AbiC) - 2-year-results of a novel Minimally Invasive Glaucoma Surgery (MIGS) technique. Klin Monbl Augenheilkd. 2021;238(10):1113–1119. doi:10.1055/a-1250-8431
25. Davids AM, Pahlitzsch M, Boeker A, Winterhalter S, Maier-Wenzel AK, Klamann M. Ab interno canaloplasty (ABiC)-12-month results of a new minimally invasive glaucoma surgery (MIGS). Graefes Arch Clin Exp Ophthalmol. 2019;257:1947–1953. doi:10.1007/s00417-019-04366-3
26. Gallardo MJ, Supnet RA, Ahmed IIK. Circumferential viscodilation of Schlemm’s canal for open-angle glaucoma: ab-interno vs ab-externo canaloplasty with tensioning suture. Clin Ophthalmol. 2018;12:2493–2498. doi:10.2147/OPTH.S178962
27. Gallardo MJ, Supnet RA, Ahmed IIK. Viscodilation of Schlemm’s canal for the reduction of IOP via an ab-interno approach. Clin Ophthalmol. 2018;12:2149–2155. doi:10.2147/OPTH.S177597
28. Gallardo MJ. 24-month efficacy of viscodilation of Schlemm’s Canal and the distal outflow system with iTrack ab-interno canaloplasty for the treatment of primary open-angle glaucoma. Clin Ophthalmol. 2021;15:86–89. doi:10.2147/OPTH.S272506
29. Gallardo MJ. 36-month effectiveness of ab-interno canaloplasty standalone versus combined with cataract surgery for the treatment of open-angle glaucoma. Ophthalmol Glaucoma. 2022;5(5):476–482. doi:10.1016/j.ogla.2022.02.007
30. Koerber N, Ondrejka S. Four-year efficacy and safety of iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery in open-angle glaucoma. Klin Monbl Augenheilkd. 2022. doi:10.1055/a-1737-4149
31. Ahmed IIK, Rhee DJ, Jones J, et al. Three-year findings of the HORIZON trial: a schlemm canal microstent for pressure reduction in primary open-angle glaucoma and cataract. Ophthalmology. 2021;128(6):857–865.
32. Lass JH, Benetz BA, He J, et al. Corneal endothelial cell loss and morphometric changes 5 years after phacoemulsification with or without CyPass micro-stent. Am J Ophthalmol. 2019;208:211–218. doi:10.1016/j.ajo.2019.07.016
33. Ianchulev T, Lane S, Masis M, et al. Corneal endothelial cell density and morphology after phacoemulsification in patients with primary open-angle glaucoma and cataracts: 2-year results of a randomized multicenter trial. Cornea. 2019;38:325–331. doi:10.1097/ICO.0000000000001826
34. Jones J, Koch DD, Vold S, et al. Results from the United States cohort of the HORIZON trial of a Schlemm canal microstent to reduce intraocular pressure in primary open-angle glaucoma. J Cataract Refract Surg. 2019;45:1305–1315. doi:10.1016/j.jcrs.2019.03.024
35. Gillmann K, Bravetti GE, Rao HL, Mermoud A, Mansouri K. Impact of combined XEN gel stent implantation on corneal endothelial cell density: 2-year results. J Glaucoma. 2020;29:155–160. doi:10.1097/IJG.0000000000001430
36. Coleman AL, Lum FC, Velentgas P, Su Z, Gliklich RE, GORSG R. Impact of treatment strategies for open angle glaucoma on intraocular pressure: the RiGOR study. J Comp Eff Res. 2016;5:87–98. doi:10.2217/cer.15.58
37. Jung JL, Isida-Llerandi CG, Lazcano-Gomez G, SooHoo JR, Kahook MY. Intraocular pressure control after trabeculectomy, phacotrabeculectomy and phacoemulsification in a Hispanic population. J Curr Glaucoma Pract. 2014;8:67–74. doi:10.5005/jp-journals-10008-1164
38. Gallardo MJ, Supnet RA, Giamporcaro JE, Hornbeak DM. Outcomes of combined trabecular micro-bypass and phacoemulsification in a predominantly Hispanic patient population. Clin Ophthalmol. 2016;10:1931–1937. doi:10.2147/OPTH.S117403
39. Armstrong JJ, Wasiuta T, Kiatos E, Malvankar-Mehta M, Hutnik CM. The effects of phacoemulsification on intraocular pressure and topical medication use in patients with glaucoma: a systematic review and meta-analysis of 3-year data. J Glaucoma. 2017;26:511–522. doi:10.1097/IJG.0000000000000643
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.