Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 14
Combined GSTT1 Null, GSTM1 Null and XPD Lys/Lys Genetic Polymorphisms and Their Association with Increased Risk of Chronic Myeloid Leukemia
Authors Abdalhabib EK ![]() , Jackson DE
, Jackson DE ![]() , Alzahrani B, Elfaki EM
, Alzahrani B, Elfaki EM ![]() , Hamza A
, Hamza A ![]() , Alanazi F, Ali EI, Algarni A
, Alanazi F, Ali EI, Algarni A ![]() , Ibrahim IK
, Ibrahim IK ![]() , Saboor M
, Saboor M ![]()
Received 21 October 2021
Accepted for publication 9 December 2021
Published 22 December 2021 Volume 2021:14 Pages 1661—1667
DOI https://doi.org/10.2147/PGPM.S342625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Ezeldine K Abdalhabib,1 Denise E Jackson,2 Badr Alzahrani,1 Elyasa M Elfaki,1 Alneil Hamza,1 Fehaid Alanazi,1 Elryah I Ali,3 Abdulrahman Algarni,3 Ibrahim Khider Ibrahim,4 Muhammad Saboor5,6
1Department of Clinical Laboratory Sciences, College of Applied Medical Sciences-Al Qurayyat, Jouf University, Sakaka, Saudi Arabia; 2Thrombosis and Vascular Diseases Laboratory, School of Health and Biomedical Sciences, RMIT University, Victoria, Australia; 3Department of Medical Laboratory Technology, College of Applied Medical Sciences, Northern Border University, Arar, Saudi Arabia; 4Department of Hematology, Faculty of Medical Laboratory Sciences, Al Neelain University, Khartoum, Sudan; 5Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 6Medical Research Center (MRC), Jazan University, Jazan, Saudi Arabia
Correspondence: Muhammad Saboor
Department of Medical Laboratory Technology, Faculty of Applied Medical Science, Jazan University, Jazan, Saudi Arabia
Tel +966 54 495 9029
Email [email protected]
Purpose: Glutathione S-transferases (GSTT1 and GSTM1) are instrumental in detoxification process of activated carcinogens. Nucleotide excision repair is carried out by DNA helicase encoded by xeroderma pigmentosum group D (XPD) genes and aberrations in the XPD gene predisposes to increased risk of cancer. The present study aimed to investigate GSTT1, GSTM1 and XPD polymorphisms in newly diagnosed chronic myeloid leukemia (CML) patients and to examine the association of these polymorphisms with the risk of developing CML.
Patients and Methods: This case–control study was carried out from June 2019 to August 2021 involving 150 newly diagnosed patients with CML and an equal number of randomly selected age- and sex-matched healthy individuals. A multiplex-PCR assay was used to genotype GSTT1 null and GSTM1 null polymorphisms. XPD gene polymorphism was detected by PCR-RFLP using predesigned gene-specific primers.
Results: GSTT1 and GSTM1 null polymorphisms were detected in 42.7% and 61.3% of cases, respectively, compared to 18% and 35.3% for controls. The combination of both GST null polymorphisms revealed a significant association with CML. Frequencies of XPD Lys751Gln genotypes in cases were 62.7% heterozygous Lys/Gln, 24% homozygous Lys/Lys and 13.3% homozygous Gln/Gln, while in the controls were 74.7%, 20%, and 5.3%, respectively. Significant differences were also noted regarding the combination of GSTT1/GSTM1 null with XPD Lys/Lys, and GSTM1 null with XPD Lys/Lys.
Conclusion: In conclusion, GSTT1 null, GSTM1 null and XPD polymorphisms showed positive association with the risk of development of CML. Furthermore, age and gender did not exhibit any association with the studied polymorphisms, while CML phases were associated with GSTT1 null polymorphism.
Keywords: GSTT1 null polymorphism, GSTM1, XPD, chronic myeloid leukemia
Introduction
Chronic myeloid leukemia (CML) is a clonal neoplastic hematological stem cell disorder typically results from specific reciprocal chromosomal translocation t (9;22) (q34;q11), which produces BCR‐ABL aberrant oncogene.1 Expression of BCR-ABL aberrant gene plays a critical role in transformation of hematopoietic stem cells, which results in relentless neoplastic proliferation of myeloid cells.2 Various genetic disorders are known to be associated with cancer predisposition. Additionally, neoplastic cells are predisposed to acquire a number of genetic abnormalities over time, resulting in disease progression.3 It has been suggested that cancer susceptibility and carcinogen metabolism are associated with polymorphisms in detoxification enzymes, which are essential for the elimination of these toxic substances and protect the cells from developing cancers by hydrolysis, reduction, and/or oxidation of activated carcinogens.4–6
Glutathione S-transferases (GSTs) are oxidative stress detoxification metabolic enzymes that carry out a wide range of functions in cell proliferation, apoptosis, neoplastic transformation, and tumor metastasis.7 In order to attain the xenobiotic detoxification function, GSTs catalyze the conjugation of xenobiotic substrates to the reduced glutathione (GSH).8,9 In the human genome, the GST encoding genes have been categorized into eight classes, including GSTT1 which encodes GST theta 1 and GSTM1 that encodes GST mu 1.10 Polymorphism GST encoding genes have been associated with reduced GST activity, which is implicated in developing different cancers, including hematologic malignancies and varied anti-neoplastic drug resistance.11
Defect in the DNA repair system is considered a crucial event in leukemogenesis, which causes chromosomal aberrations and genomic instability.12,13 The xeroderma pigmentosum group D (XPD) gene also known as ERCC2 which encodes a DNA helicase, functionally involved in the nucleotide excision repair (NER) pathway, is instrumental for nucleotide excision repair. Mutations in the XPD gene lessen the activity of DNA helicase, consequently causing defects in the NER pathway.14 XPD Lys751Gln (XPD 2251A>C, rs13181) polymorphisms in homozygous form downregulate the DNA repair capacity for UV DNA damage and benzo(a)pyrene adducts.15,16 Polymorphism’s status of DNA repair genes is varied in ethnic and geographic distanced populations.17 Several studies have explored the effects of XPD Lys751Gln polymorphism in different hematological malignancies, including CML.18–21 However, these results are inconsistent in different populations. It is interesting to note that while some studies suggest strong association of leukemia with XPD gene polymorphism, others found relatively weak correlation; yet some negate this association.22 The present study aimed to investigate GSTT1, GSTM1 and XPD polymorphisms in newly diagnosed CML patients and to examine the association of these polymorphisms with the risk of developing CML.
Materials and Methods
This case–control study involving 150 patients with CML and an equal number of randomly selected healthy individuals was carried out from June 2019 to August 2021. Newly diagnosed patients with CML were recruited from the Radiation and Isotope Centre Khartoum (RICK), Khartoum, Sudan. Patients were diagnosed by at least two hematopathologists according to WHO guidelines. All patients were positive for Ph chromosome. Patients with a history of other malignancies were excluded from the study. Age- and gender-matched healthy controls were recruited during their regular examination. All subjects were Sudanese and older than 18 years. Ethic committee of Alneelain University, Khartoum, Sudan, gave the ethical approval of this study. Guidelines of the Declaration of Helsinki were followed in this study. Written informed consents were signed by all study participants.
Venous blood samples were collected in EDTA-anticoagulated vacutainers from all participants. QIAamp® DNA Mini kit (Qiagen GmbH, Hilden, Germany) was used for the extraction of genomic DNA from the peripheral blood samples of patients and controls according to the manufacturer’s instructions. Aliquots of the extracted DNA samples were stored at –20°C until molecular analysis. A multiplex-PCR assay was used to genotype GSTT1 and GSTM1 null polymorphisms. Briefly, for each 25 µL of reaction volume of genomic DNA (100–150 ng) a 10× PCR buffer of 1.5 µM MgCl2, 0.5 units of Taq polymerase, and 200 µM dNTPs were mixed. The primers and PCR conditions were the same as described by Agrawal et al.23 The β-Globin primers were used as a positive control (5′-CAA CTT CAT CCA CGT TCA CC-3′ and 5′-GAA GAG CCA AGG ACA GGT AC-3′). The amplified products were analyzed by banding patterns on agarose gels electrophoresis. PCR product at 268 bp indicated a successful amplification. Genotyping of the GSTT1 and GSTM1 is revealed by the presence or absence of a band at 480 and 215 bp, respectively. XPD gene polymorphism was detected by PCR-RFLP using predesigned gene-specific primers. The primers and PCR conditions for XPD polymorphism were the same as described by Mervat et al.24 The amplified PCR products of XPD were subjected to restriction digestion with respective enzyme (PstI). The digested products were run on 3% agarose gel electrophoresis and stained using ethidium bromide. The identification of genotypes was based on the banding patterns. PCR product of XPD polymorphism contained an internal PstI site, resulting in products of 290 and 146 bp in the 751 Lys/Lys (AA) allele. While the PstI site in the Gln allele, results in 272/146/63 bp for Gln/Gln (CC), and 290/227/146/63 bp products for Lys/Gln (AC) genotypes.
Statistical Analysis
Standard statistical tests were carried out using the Statistical Package for Social Sciences (SPSS) version 25 (SPSS for Windows, Chicago, IL, USA) to compute descriptive parameters including mean and frequencies. Inferential statistics including Student’s t-test was used to evaluate the significance of the difference between the mean values of two continuous variables. Chi-square test (X2) test and Fisher-Freeman-Halton test were used to verify statistical significance in proportions categorical variables. Odds ratios (OR) with 95% confidence intervals (CI) calculated by logistic regression analyses were conducted to determine the relationship between the studied genotypes and the risk for CML. The level of confidence (P˂0.05) was considered as cutoff value for statistical significance.
Results
In this study, GSTT1 null, GSTM1 null and XLD Lys 751Gln polymorphisms were investigated in patients with CML and healthy controls. Demographic features including age, gender, and phase of CML are presented in Table 1. Similar distribution of age and gender existed between cases and controls as depicted in Table 1. The male group constituted 66% (n=99), and 68.7% (n=103) of cases and controls, respectively. Among cases, 86% were diagnosed in the chronic phase, 8% accelerated phase, while 6% in the blast crisis phase.
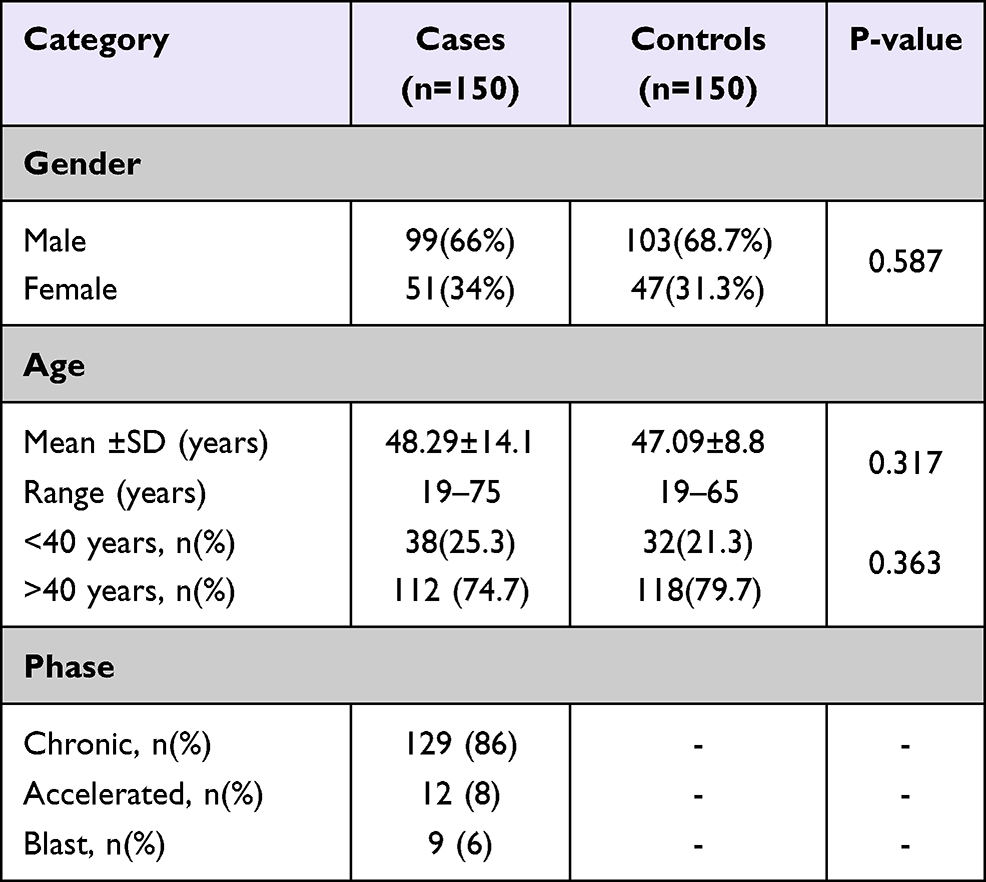 |
Table 1 Demographic Characteristics of the Studied Subjects |
In this study, GSTT1 null and GSTM1 null showed positive association with CML (Table 2). Genotype frequency of GSTT1 null polymorphism in cases was 42.7%, and for controls, it was 18%. Statistically significant difference was observed in the variant genotype frequencies between the cases and controls (OR=3.39, P < 0 0.001). Frequencies of GSTM1 null polymorphism in cases were 61.3% and, 35.3% for the controls. Statistically significant difference was observed in the variant genotype frequencies between the cases and controls (OR=2.9, P < 0 0.001).
 |
Table 2 Genotypes and Alleles Distribution in the CML Cases and Control Groups |
The observed genotype frequencies of XPD Lys751Gln polymorphism in cases were 62.7% heterozygous Lys/Gln, 24% homozygous Lys/Lys and 13.3% homozygous Gln/Gln. As for the controls, genotype frequencies were 74.7%, 20%, and 5.3%, respectively, which revealed significant association between CML patients and controls (Lys/Lys; OR=1.43, P = 0.027, Gln/Gln; OR=2.98, P = 0.013).
We analyzed the combination of the studied polymorphism and their association with CML as shown in Table 3. The combination of both GSTs null polymorphism revealed a significant association with CML (P < 0 0.001), in which the frequency of GSTT1null/GSTM1 null/Gln/Lys was 29.3% in cases, and 6.7% in control group. Also, significant differences were noted regarding the combination of GSTT1 Null/GSTM1 null with XPD Lys/Lys (P = 0.034), and GSTM1 with XPD Lys/Lys (P = 0.023). However, the combinations of GSTT1 null/GSTM1 null with XPD Gln/Gln, GSTT1 with XPD Gln/Gln, and GSTM1 null with XPD Gln/Gln did not show statistically significant difference between cases and control groups (P > 0.05).
 |
Table 3 Combination Effect of Studied Polymorphisms on the Risk of CML |
Distribution of XPD variants and GSTs null polymorphisms in patients stratified by age groups, gender, and CML phases is illustrated in Table 4. No statistically significant difference was found between the distribution of studied polymorphisms and age of CML patients at diagnosis. (P-values were >0.05). The studied polymorphisms also had no impact on the risk of CML with respect to patient’s gender. No statistically significant differences were observed in genotypes frequencies within CML patients (p > 0.05). Statistically significant difference was observed in GSTT1 null genotype and phases of CML (p = 0.012) as shown in Table 4.
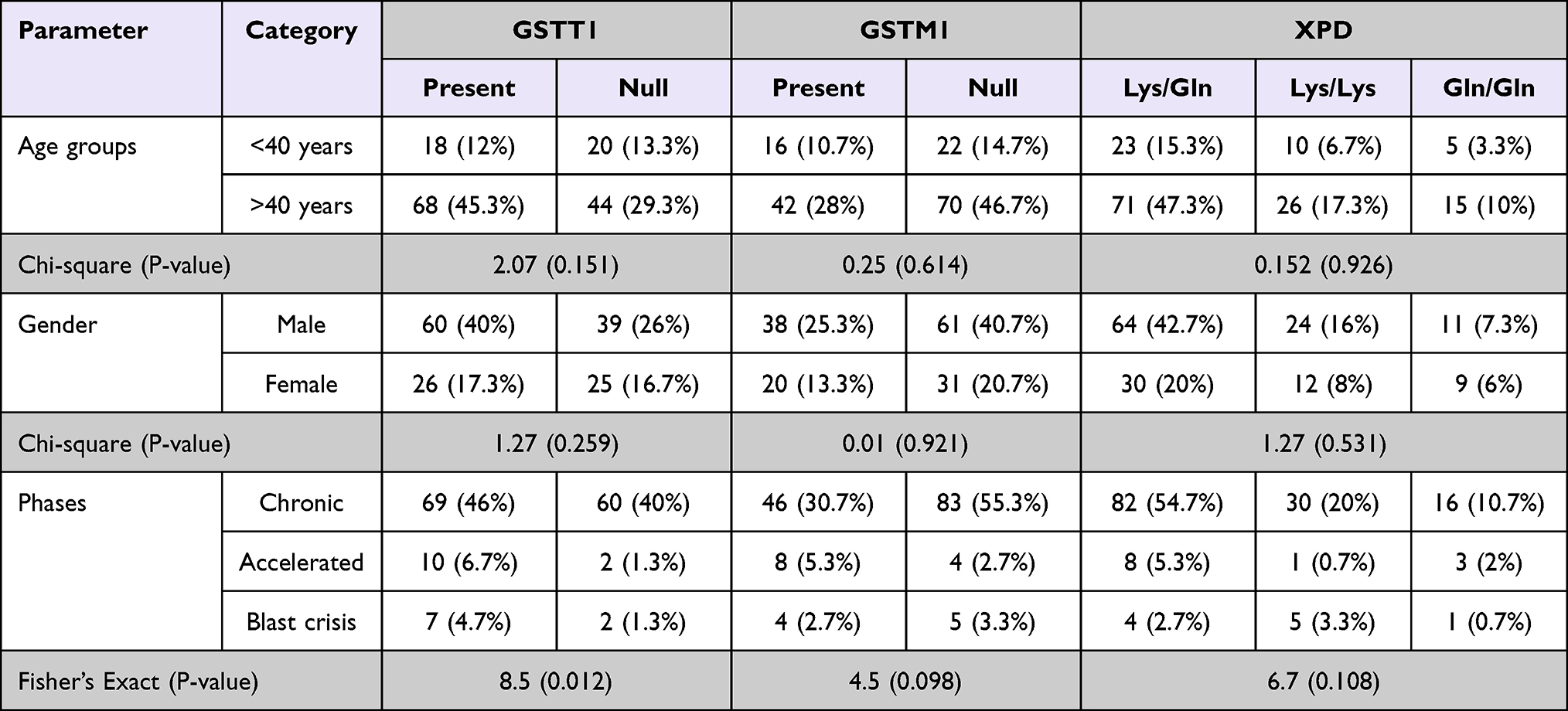 |
Table 4 Distribution of the Studied Polymorphisms Among CML Patients According to Age Group, Gender, and CML Phase |
Discussion
GSTs are categorized into two families: membrane bound and the soluble or cytosolic GSTs. Cytosolic GSTs including GSTT1 and GSTM1 are instrumental in detoxification process of activated carcinogens.25 Nucleotide excision repair and basal transcription are carried out by helicase encoded by XPD genes and aberrations in the XPD gene predisposes to increased risk of cancer.26
In this case–control study, genetic polymorphisms of GSTT1, GSTM1, and XPD Lys751Gln polymorphisms as risk for CML were investigated in Sudanese population. Literature shows contradictory results of these polymorphisms in a number of studies in different ethnicities and populations. In the current study, GSTT1 null polymorphism was observed in 42.7% patients with CML (OR = 3.39, 95% CI = 2.0 to 5.74, p < 0.001) as compared to control group (18%). Almost the same frequency of GSTT1 null polymorphism has also been reported in a local study,25 while another has reported lower rate (34%) of GSTT1 in Sudanese population with CML.27 Similarly, the frequency of GSTT1 null phenotype has been found to be lower in other populations including India (9%),28 Syria (17%),29 Turkey (18%),30 Brazil (23.8%),31 and Romania (24%).32 Frequencies of GSTM1 null polymorphism in cases were 61.3% and, 35.3% in controls. Statistically significant difference was observed in the variant genotype frequencies between the cases and controls (OR= 2.9, P = <0 0.001). Our results revealed a strong association between GSTT1 null and GSTM1 null polymorphisms and CML susceptibility. Similar results have been also reported in a local study27 and, other populations as well.28,33 However, in contrast, other studies also suggest that GSTT1 null, and GSTM1 null may not be a predisposing risk factor for CML.32,34 Additionally, a local study also presents contradictory results reporting no association of GSTM1 null phenotype and risk of CML (OR = 0.975, P = 0.836).25 Furthermore, several studies have described the influence of isolated GSTM1 gene polymorphism on CML risk, but no association of GSTT1 gene polymorphism was found in the same patients.35,36 Contrary to this, some reports show that GSTT1 gene polymorphism has association with increased risk for CML, whereas no association was observed in regards to GSTM1 gene polymorphism.6,37 The reasons for these contradictions and inconsistencies might depend on geographic and ethnic variations, among others.35
The combined analysis performed in the current study illustrates that GSTT1 null genotype in combination with GSTM1 null genotype are considerable risk factors for CML development. A similar pattern of results have also been observed.25,30 The increased risk could be correlated with the synergistic effect of the enzymes encoded by GSTT1 and GSTM1 genes; instrumental in the cellular detoxification process. Genetic aberrations affecting the enzymatic activity of GSTT1 and GSTM1 make the DNA prone to damages leading to increased risk of developing CML.
Increased risk of cancer among individuals with XPD polymorphisms or other genes involved in the NER pathway has been observed.38 Literature shows conflicting results of XPD polymorphism in patients with neoplasia. Some studies have reported a strong association between the XPD Lys751Gln polymorphism and increased leukemia risk,20,21,39 while one study found decreased risk of the leukemia.26 In the current study, XPD Lys751Gln polymorphism was found to be associated with increased risk for CML. These results are in agreement with Bănescu et al.39 To examine the effect of gene–gene interactions as an estimation for CML risk in the present study, the relationship between dual gene–gene combinations was also analyzed. The results indicate that XPD Lys/Lys genotypes and GSTM1null polymorphisms have an impact together on CML development and risk. No previous study has used this to investigate the effects of these polymorphisms on CML.
Distribution of XPD variants and GSTs null polymorphisms in patients stratified by age group and gender did not show statistically significant difference between the distribution of studied polymorphisms and age of CML patients at diagnosis (P > 0.05). The studied polymorphisms also had no impact on the risk of CML with respect to patient’s gender. No statistically significant differences were observed in genotypes frequencies within CML patients (P > 0.05); this finding is also supported by other studies.27,35,40 However, these findings are contradictory to previous reports where the frequency of GSTM1 null genotype was lower in patients in the accelerated and/or blast crisis phase as compared to patients in chronic phase.41 Moreover, findings of this study show that GSTT1 polymorphism is associated with phase of CML. In the light of the above results and discussion, it is concluded GSTT1, GSTM1 and XPD null polymorphisms showed positive association with the risk of development with CML. Furthermore, age and gender did not exhibit any association with the studied polymorphisms, while CML phases were associated with GSTT1 null polymorphism.
Acknowledgments
The authors extend their appreciation to the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this work through the grant number “375213500”. The authors would like to extend their sincere appreciation to the central laboratory at Jouf University for support this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shibata N, Miyamoto N, Nagai K, et al. Development of protein degradation inducers of oncogenic BCR-ABL protein by conjugation of ABL kinase inhibitors and IAP ligands. Cancer Sci. 2017;108(8):1657–1666. doi:10.1111/cas.13284
2. Zhang B, Li L, Ho Y, et al. Heterogeneity of leukemia-initiating capacity of chronic myelogenous leukemia stem cells. J Clin Invest. 2016;126(3):975–991. doi:10.1172/JCI79196
3. Ales M, Scaramucci L, Niscola P, et al. IgG secreting lymphoplasmacytoid leukemia with massive skin involvement and very aggressive clinical course: an exceptionally rare observation. Leuk Res. 2010;34(2):2009–2010. doi:10.1016/j.leukres.2009.07.014
4. Yaya K, Hind D, Meryem Q, Asma Q, Said B, Sellama N. Single nucleotide polymorphisms of multidrug resistance gene 1 (MDR1) and risk of chronic myeloid leukemia. Tumor Biol. 2014;35(11):10969–10975. doi:10.1007/s13277-014-2400-4
5. Laborde E. Glutathione transferases as mediators of signaling pathways involved in cell proliferation and cell death. Cell Death Differ. 2010;17(9):1373–1380. doi:10.1038/cdd.2010.80
6. Dusinska M, Staruchova M, Horska A, et al. CYP1A1, GST gene polymorphisms and risk of chronic myeloid leukaemia. Tumor Biol. 2014;7(7):130–137. doi:10.1016/j.tips.2012.09.007
7. Wu B, Dong D. Human cytosolic glutathione transferases: structure, function, and drug discovery. Trends Pharmacol Sci. 2012;33(12):656–668. doi:10.1016/j.tips.2012.09.007
8. Cummins I, Dixon DP, Freitag-Pohl S, Skipsey M, Edwards R. Multiple roles for plant glutathione transferases in xenobiotic detoxification. Drug Metab Rev. 2011;43(2):266–280. doi:10.3109/03602532.2011.552910
9. Board PG, Menon D. Structure, function and disease relevance of Omega-class glutathione transferases. Arch Toxicol. 2016;90(5):1049–1067. doi:10.1007/s00204-016-1691-1
10. He HR, Zhang XX, Sun JY, et al. Glutathione S-transferase gene polymorphisms and susceptibility to chronic myeloid leukemia. Tumor Biol. 2014;35(6):6119–6125. doi:10.1007/s13277-014-1810-7
11. Duvoix A, Delhalle S, Blasius R, et al. Effect of chemopreventive agents on glutathione S-transferase P1-1 gene expression mechanisms via activating protein 1 and nuclear factor kappaB inhibition. Biochem Pharmacol. 2004;68(6):1101–1111. doi:10.1016/j.bcp.2004.05.032
12. Pawlowska E, Blasiak J. DNA repair—a double-edged sword in the genomic stability of cancer cells—the case of chronic myeloid leukemia. Int J Mol Sci. 2015;16(11):27535–27549. doi:10.3390/ijms161126049
13. Esposito MT, So CWE. DNA damage accumulation and repair defects in acute myeloid leukemia: implications for pathogenesis, disease progression, and chemotherapy resistance. Chromosoma. 2014;123(6):545–561. doi:10.1007/s00412-014-0482-9
14. Catana A, Popp RA, Pop M, Porojan MD, Petrisor FM, Pop IV. Genetic polymorphism of DNA repair gene ERCC2/XPD (Arg 156 Arg) (A22541C) and lung cancer risk in Northern Romania. Revista Română de Medicină de Laborator. 2012;20(2):4–6.
15. Mitra AK, Singh N, Garg VK, Chaturvedi R, Sharma M, Rath SK. Statistically significant association of the single nucleotide polymorphism (SNP) rs13181 (ERCC2) with predisposition to Squamous Cell Carcinomas of the Head and Neck (SCCHN) and Breast cancer in the north Indian population. J Exp Clin Cancer Res. 2009;28(1):104. doi:10.1186/1756-9966-28-104
16. Douzi K, Ouerhani S, Menif S, Safra I, Abbes S. Polymorphisms in XPC, XPD and XPG DNA repair genes and leukemia risk in a Tunisian population. Leuk Lymphoma. 2015;56(6):1856–1862. doi:10.3109/10428194.2014.974045
17. Yetgin S, Yalçin SS. The effect of vitamin D3 on CD34 progenitor cells in vitamin D deficiency rickets. Turk J Pediatr. 2004;46(2):164–166.
18. Sorour A, Ayad MW, Kassem H. The genotype distribution of the XRCC1, XRCC3, and XPD DNA repair genes and their role for the development of acute myeloblastic leukemia. Genet Test Mol Biomarkers. 2013;17(3):195–201. doi:10.1089/gtmb.2012.0278
19. Özcan A, Pehlivan M, Tomatir AG, et al. Polymorphisms of the DNA repair gene XPD (751) and XRCC1 (399) correlates with risk of hematological malignancies in Turkish population. Afri J Biotechnol. 2011;10(44):8860–8870. doi:10.5897/ajb10.1839
20. Bănescu C, Iancu M, Trifa AP, et al. Influence of XPC, XPD, XPF, and XPG gene polymorphisms on the risk and the outcome of acute myeloid leukemia in a Romanian population. Tumor Biol. 2016;37(7):9357–9366. doi:10.1007/s13277-016-4815-6
21. Shi JY, Ren ZH, Jiao B, et al. Genetic variations of DNA repair genes and their prognostic significance in patients with acute myeloid leukemia. Int J Cancer. 2011;128(1):233–238. doi:10.1002/ijc.25318
22. Wen M, Zhou B, Lin X, et al. Associations between XPD Lys751Gln polymorphism and leukemia: a meta-analysis. Front Genet. 2018;9:1–11. doi:10.3389/fgene.2018.00218
23. Agrawal D, Gupta S, Agarwal D, Gupta OP, Agarwal M. Role of GSTM1 and GSTT1 polymorphism: susceptibility to oral submucous fibrosis in the north Indian population. Oncology. 2011;79(3–4):181–186. doi:10.1159/000318533
24. El-Tokhy MA, Hussein NA, Bedewy AML, Barakat MR. XPD gene polymorphisms and the effects of induction chemotherapy in cytogenetically normal de novo acute myeloid leukemia patients. Hematology. 2014;19(7):397–403. doi:10.1179/1607845413Y.0000000144
25. Idris HME, Elderdery AY, Khalil HB, Mills J. Genetic polymorphism of GSTP1, GSTM1 and GSTT1 genes and susceptibility to chronic myeloid leukaemia. Asian Pacific J Cancer Prev. 2020;21(2):499–503. doi:10.31557/APJCP.2020.21.2.499
26. Dincer Y, Yüksel S, Batar B, Güven M, Onaran I, Celkan T. DNA repair gene polymorphisms and their relation with DNA damage, DNA repair, and total antioxidant capacity in childhood acute lymphoblastic leukemia survivors. J Pediatr Hematol Oncol. 2015;37(5):344–350. doi:10.1097/MPH.0000000000000133
27. Muddathir ARM, Abdallah EI, Khabour OF, Abdelgader RE, Elgari MM. Age- and gender-independent association of glutathione S-transferase null polymorphisms with chronic myeloid leukemia. Bosn J Basic Med Sci. 2019;19(4):350–354. doi:10.17305/bjbms.2019.4176
28. Bajpai P, Tripathi AK, Agrawal D. Increased frequencies of glutathione-S-transferase (GSTM1 and GSTT1) null genotypes in Indian patients with chronic myeloid leukemia. Leuk Res. 2007;31(10):1359–1363. doi:10.1016/j.leukres.2007.02.003
29. Al-Achkar W, Azeiz G, Moassass F, Wafa A. Influence of CYP1A1, GST polymorphisms and susceptibility risk of chronic myeloid leukemia in Syrian population. Med Oncol. 2014;31(5):889. doi:10.1007/s12032-014-0889-4
30. Özten N, Sunguroǧlu A, Bosland MC. Variations in glutathione-S-transferase genes influence risk of chronic myeloid leukemia. Hematol Oncol. 2012;30(3):150–155. doi:10.1002/hon.1018
31. Lordelo GS, Miranda-Vilela AL, Akimoto AK, et al. Association between methylene tetrahydrofolate reductase and glutathione S-transferase M1 gene polymorphisms and chronic myeloid leukemia in a Brazilian population. Genet Mol Res. 2012;11(2):1013–1026. doi:10.4238/2012.April.19.6
32. Benescu C, Trifa AP, Voidezan S, et al. CAT, GPX1, MnSOD, GSTM1, GSTT1, and GSTP1 genetic polymorphisms in chronic myeloid leukemia: a case-control study. Oxid Med Cell Longev. 2014;2014. doi:10.1155/2014/875861
33. Taspinar M, Aydos SE, Comez O, Elhan AH, Karabulut HG, Sunguroglu A. CYP1A1, GST gene polymorphisms and risk of chronic myeloid leukaemia. Swiss Med Wkly. 2008;138(1–2):12–17. doi:10.4414/smw.2008.12036
34. Hishida A, Terakura S, Emi N, et al. GSTT1 and GSTM1 deletions, NQO1 C609T polymorphism and risk of chronic myelogenous leukemia in Japanese. Asian Pacific J Cancer Prev. 2005;6(3):251–255.
35. Weich N, Ferri C, Moiraghi B, et al. GSTM1 and GSTP1, but not GSTT1 genetic polymorphisms are associated with chronic myeloid leukemia risk and treatment response. Cancer Epidemiol. 2016;44:16–21. doi:10.1016/j.canep.2016.07.008
36. Rostami G, Assad D, Ghadyani F, et al. Influence of glutathione S-transferases (GSTM1, GSTT1, and GSTP1) genetic polymorphisms and smoking on susceptibility risk of chronic myeloid leukemia and treatment response. Mol Genet Genomic Med. 2019;7(7):1–10. doi:10.1002/mgg3.717
37. Shahrokhzadeh S, Soleimani A, Kordi-Tamandani DM, Sangtarash MH, Nejati O, Taheri M. Association of genetic polymorphisms in GSTP1, GSTM1, and GSTT1 genes with vesicoureteral reflux susceptibility in the children of southeast Iran. Iran J Public Health. 2020;49(7):1364–1371. doi:10.18502/ijph.v49i7.3591
38. He BS, Xu T, Pan YQ, et al. Nucleotide excision repair pathway gene polymorphisms are linked to breast cancer risk in a Chinese population. Oncotarget. 2016;7(51):84872–84882. doi:10.18632/oncotarget.12744
39. Bănescu C, Trifa AP, Demian S, et al. Polymorphism of XRCC1, XRCC3, and XPD genes and risk of chronic myeloid leukemia. Biomed Res Int. 2014;2014:213790. doi:10.1155/2014/213790
40. Mondal BC, Paria N, Majumdar S, et al. Glutathione S-transferase M1 and T1 null genotype frequency in chronic myeloid leukaemia. Eur J Cancer Prev. 2005;14(3):281–284. doi:10.1097/00008469-200506000-00014
41. Lourenc¸ GJ, Ortega MM, Nascimento H, et al. Polymorphisms of glutathione S -transferase in chronic myeloid leukaemia. Eur J Haematol. 2005;75:530–531. doi:10.1111/j.0902-4441.0000.t01-1-EJH2337.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.