")
Back to Journals » Clinical Ophthalmology » Volume 17
Combined Femtosecond Laser-Assisted Keratotomy and Cataract Surgery for Enhancing Refractive Outcomes. An Indonesian Case Study
Authors Viona V , Soebijantoro I, Gondhowiardjo TD
Received 18 July 2023
Accepted for publication 4 October 2023
Published 9 October 2023 Volume 2023:17 Pages 2983—2996
DOI https://doi.org/10.2147/OPTH.S416217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Viona Viona,1,* Iwan Soebijantoro,2,* Tjahjono D Gondhowiardjo3,*
1Department of Research, Jakarta Eye Center (JEC) Eye Hospitals and Clinics, Jakarta, Indonesia; 2Department of Glaucoma, Jakarta Eye Center (JEC) Eye Hospitals and Clinics, Jakarta, Indonesia; 3Department of Corneal and Refractive Surgery, Jakarta Eye Center (JEC) Eye Hospitals and Clinics, Jakarta, Indonesia
*These authors contributed equally to this work
Correspondence: Viona Viona, Jalan Terusan, Jl. Arjuna Utara Jl. Kedoya Raya No. 1, Kedoya Sel., Kec. Kb, Jeruk, West Jakarta, 11520, Jakarta, Email [email protected]
Purpose: We evaluate the reduction of corneal astigmatism and the improvement of visual outcomes of this surgical method in the Indonesian population. We also assess the accuracy and predictability of using femtosecond laser astigmatic keratotomy (FLAK) combined with cataract surgery.
Patients and Methods: In a retrospective study, a total of 275 subjects (78 with against-the-rule (ATR) astigmatism, 178 with with-the-rule (WTR) astigmatism, and 19 with oblique (OBL) astigmatism) with preexisting corneal astigmatism ranging from 0.75D to 3.00D underwent FLAK. All subjects completed a 3-month follow-up. The femtosecond laser used for creating paired AK 2.2 mm, primary incision, and paracentesis incision was the FEMTO Z8 NEO from Ziemer Ophthalmic System, Switzerland. The surgical approach was guided by the “NAPA” nomogram.
Results: The reduction in postoperative astigmatism was 56.90% for the WTR group, 49.46% for the ATR group, and 47.33% for the oblique group. A significant reduction in astigmatism was observed at the 1-week, 1-month, and 3-month follow-up intervals in both the WTR and ATR groups. The reduction in astigmatism was more favorable in cases of moderate astigmatism within the WTR group, as compared to the ATR and oblique groups. Postoperative astigmatism reduction was found to be more predictable in the right eye than in the left eye.
Conclusion: The combination of FLAK can be considered as a potential method for reducing corneal astigmatism ranging from 1.00D to < 3.00D. The highest reduction was observed in the WTR group, along with a higher rate of intended correction without astigmatism meridian shift in the right eye for the WTR group. However, factors such as cyclotorsion resulting from the surgical technique, alignment of docking, incision length, and preoperative astigmatism need to be taken into account for further enhancement and predictability of astigmatism reduction with this method.
Keywords: femtosecond laser-assisted cataract surgery, FLACS, astigmatic keratotomy, AK, femtosecond laser astigmatic keratotomy, FLAK, corneal astigmatism correction
Introduction
Cataract is the leading cause of visual impairment or blindness worldwide. The World Health Organization (WHO) estimates that there are 94 million cataract cases, accounting for 51% of global blindness.1,2 Techniques for cataract surgery have been improved to be less invasive, resulting in more accurate visual outcomes.
Pre-existing astigmatism is not uncommon among cataract patients, with varying degrees. Approximately 30% of cataract patients have 1.25 D astigmatism, and 10% of the population has astigmatism higher than 2.00 D. Previous studies have demonstrated a high prevalence of pre-existing astigmatism that increases with age. The remaining postoperative astigmatism of 0.75 D can significantly impact visual acuity, leading to symptomatic blur, image ghosting, and halos. Therefore, reducing astigmatism to achieve emmetropia may improve visual outcomes, reduce dependence on spectacles, and enhance patient satisfaction after cataract surgery.3,4
Numerous approaches to achieve emmetropic astigmatism include limbal relaxing incisions (LRI), arcuate keratotomies, opposite clear corneal incisions (OCCI), and toric intraocular lens (IOLs) implantation.5–7 Astigmatic keratotomy (AK) is located within the cornea, causing a flattening effect in the incised meridian, which represents the steepest meridian. LRIs, when compared to more central incisions, are more manageable and forgiving, resulting in less postoperative discomfort.8,9 Manual limbal relaxing incisions have inconsistent predictability and outcomes. Complications associated with limbal relaxing incisions include induced irregular astigmatism, induced ocular aberrations, and abnormal wound healing.10 With recent advancements in femtosecond laser technology, there has been a shift in interest from manual LRIs and AK procedures to laser-guided surgeries. Femtosecond laser-assisted cataract surgery (FLACS) has emerged as a new technology over the past decade, offering less invasiveness, improved safety, and more predictable outcomes. The utilization of femtosecond laser technology in corneal surgery has gained popularity due to the potential benefits of increased precision and accuracy when compared to traditional manual methods.11 Studies have demonstrated that femtosecond laser-assisted intrastromal arcuate keratotomy is safer, more reproducible, and more precise in reducing astigmatism. Consequently, there have been suggestions of employing FLACS with limbal relaxing incisions or arcuate keratotomy as a viable alternative to manual techniques. The femtosecond laser allows for the creation of incisions that are more precise in terms of length, depth, and alignment of the keratotomy.12
Toric IOLs are well-known and proven to be effective, offering high precision in correcting astigmatism. However, there are limited options for toric IOLs, as they are only available for correcting astigmatism power greater than 2D in Indonesia. Several published studies have investigated the effectiveness of toric intraocular lenses (IOLs) compared to limbal relaxing incisions or astigmatic keratotomy. While some studies indicate similar outcomes between the approaches, others suggest that toric IOLs provide superior and long-lasting results, enabling patients to achieve spectacle independence. In this study, our focus is to evaluate the use of astigmatic keratotomy in reducing corneal astigmatism and improving outcomes, particularly in situations where toric IOLs are either unavailable or considered prohibitively expensive.13 Therefore, we utilized the femtosecond laser system, which is already available and provides cost-related benefits, and incorporated it with arcuate keratotomy to reduce astigmatism and achieve the emmetropia target for cataract surgery.
Subject and Methods
Ethical Approval
This study was conducted in adherence to the tenets of the Declaration of Helsinki. All patients have given written informed consent. Retrospective case review of patients who underwent femtosecond laser-assisted cataract surgery combined with astigmatic keratotomy between December 2019 and September 2022 by 1 surgeon (IS) at JEC Eye Hospitals and Clinics. The follow-up period was 3 months.
Subject
The inclusion criteria of this study were subjects with subjective visual acuity reduction by significant cataract, astigmatism >0.75 D, and adhered to 3-month follow-up. Patients with irregular astigmatism, a history of refractive surgeries or intraocular surgeries, corneal abnormalities, a history of acute glaucoma attack, uncontrolled diabetes, and pregnancy were excluded. Patients selected in the study attempted to be as ideal as possible in order to describe the results of the astigmatic keratotomy. Corneal astigmatism was measured by IOL master 700 (Carl Zeiss Meditec AG, Jena, Germany) as a routine preoperative examination and analysis.
Procedure
The optical zones for astigmatic keratotomy (AK) in all study subjects were set at 9.0 mm with a depth of 85%, following the Nichamin Age and Pachymetry-adjusted Intralimbal Arcuate Astigmatic (NAPA) Femtosecond nomogram. Astigmatism, according to the Nichamin FLACS “NAPA” nomogram with postoperative astigmatism target <0.5D, was classified as either with-the-rule astigmatism (45 to 135 degrees) or against-the-rule astigmatism (0 to 44 degrees or 136 to 180 degrees). Paired AKs, a primary incision of 2.2 mm, and a paracentesis incision were all created using the femtosecond laser (FEMTO Z8 NEO, Ziemer Ophthalmic System, Switzerland). Topical anesthetics (Pantocain 0.5%) were administered in all cases prior to the procedures. AKs were performed and released before phacoemulsification.
The procedure commenced with the positioning of the suction ring from a disposable liquid–patient interface, carefully centered over the limbus and onto the eye. The femtosecond laser system incorporates a liquid interface that does not exert flattening pressure on the cornea. Once the suction vacuum reached a pressure of 400 mbar, a balanced salt solution was introduced to fill the suction ring. The handpiece, which is securely attached to an articulated arm of the laser system, was then aligned with precision to match the corneal apex. This handpiece features a color camera and an integrated ocular coherence tomography (OCT) system. The laser treatment procedure commenced with an anterior capsulotomy having a diameter of 5.0 mm, followed by lens fragmentation, and clear corneal incisions. In this study, lens fragmentation was omitted based on the surgeon’s preference.
The main incision was positioned at 3 o’clock, while the paracentesis incision was at 6 o’clock, maintaining a 90-degree separation. However, in cases with against-the-rule (ATR) astigmatism, NAPA-assumptions were applied. In such cases, AKs were positioned temporally, and the surgeon adjusted the main incision to be as close as possible (within a 10-degree buffer) to the AK site while still aligning with the surgeon’s preferred incision position. The paracentesis incision was shifted accordingly to maintain a 90-degree separation.
An extended depth focus intraocular lens (TECNIS ICBoo by Johnson & Johnson Surgical Vision, Inc., Santa Ana, USA, or RayOne EMV by Rayner Intraocular Lenses Limited, Worthing, UK) was implanted in all cases. Postoperative assessments of astigmatism using automated keratometry were conducted at 1-day, 1-week, 1-month, and 3-month follow-up intervals. Astigmatism analysis was categorized into against-the-rule (ATR) 0°–30°, with-the-rule (WTR) 60°–120°, and oblique (OBL) 31°–59°; 121°–149° astigmatism groups.
Statistical Analysis
The statistical analysis was conducted using SPSS 23.0 (IBM Corp, NY, USA) and Microsoft Office Excel 2021 (Microsoft, Washington, USA). Follow-up data were measured by Mann–Whitney or dependent t-test with a significance level of P<0.05. In this study, the assessment of surgical outcomes for astigmatism was conducted employing Alpins’ vector analysis method, with graphical representation available at the following link: http://www.lasikmd.com/media/astigmatic. The evaluation of keratometric astigmatism was based on simulated keratometry values. The investigation centered on three key vectors: target-induced astigmatism (TIA), surgically induced astigmatism (SIA), and the difference vector (DV).
Results
Based on the inclusion and exclusion criteria, 275 subjects underwent cataract surgery with limbal relaxing incisions combined with FLACS and had a complete 3-month follow-up. The demographic and clinical characteristics of the patients are shown in Table 1.
 |
Table 1 Patient Characteristics |
All study participants were Indonesian. No significant differences were found in WTW between the against-the-rule (ATR), with-the-rule (WTR), and oblique (OBL) astigmatism groups. However, the widest WTW was found in the WTR group, which had the youngest study participants compared to the ATR and OBL groups. The laterality of the eye also affects the placement of the main port, side port, and arcuate keratotomies in overlapping cases. In our case, we placed the incisions as close as possible to the intended places without overlapping to prevent corneal perforation. ATR and OBL groups had higher subjects in the left eye, and WTR group had more subjects with the right eye. The differences in preoperative astigmatism were assessed by dividing the groups into ATR, WTR, and Oblique shown in Table 2.
 |
Table 2 Preoperative and Postoperative Against-The-Rule (ATR), with-The-Rule (WTR), Oblique (OBL) Astigmatism |
In the ATR group, there was a significant difference between preoperative and postoperative astigmatism in <1.00 D, 1.00–2.00 D, >2.00 D, and >3.00 D groups with P value <0.005. Although the significant decrease, postoperative astigmatism had not reached the desired target (<0.5D). Further analyzed, the highest decrease in astigmatism was found in the astigmatism group >2.00 D (66.87%±16.24%). Subjects with postoperative astigmatism <0.5D were comparable in <3.00D. In five subjects with >3.00 D astigmatism with significant differences in postoperative astigmatism, but no subjects had the target astigmatism (<0.5D).
The largest sample was obtained in WTR astigmatism group with a total of 178 subjects. Similar to ATR astigmatism, most subjects were 1.00D - 2.00 D group, as many as 84 subjects. The highest mean of astigmatism decrease was found in the astigmatism group > 3.00 (69.45%±28.80%). However, the group that achieved the highest postoperative astigmatism within the target range of <0.50 D was the <1.00 D group. Overall, compared with ATR astigmatism, in the WTR astigmatism group, there were more subjects with postoperative astigmatism <0.50D.
A small sample size was obtained in oblique astigmatism group, with the largest number of subject in the 1.00D to 2.00D astigmatism. There was no overall significant decrease in postoperative astigmatism. An increase in astigmatism was observed in four cases within the <1.00D group. There was a significant decrease in astigmatism in >2.00D group (P<0.05). But there were only two subjects in the group. Overall reduction of astigmatism was 56.90% for WTR group, 49.46% for ATR group, and 47.33% for OBL astigmatism.
In the WTR, ATR, and OBL groups, higher astigmatism was found in the right eye (Table 3). These findings indicate that higher astigmatism is more common in the dominant eye, which is typically the right eye in the general population. A significant decrease in astigmatism was observed in both the right and left eyes of the WTR and ATR groups. In contrast, the decrease in astigmatism was not significant in the OBL group. Further analysis was conducted using astigmatism meridian shift analysis to evaluate the predictability of this surgical method.
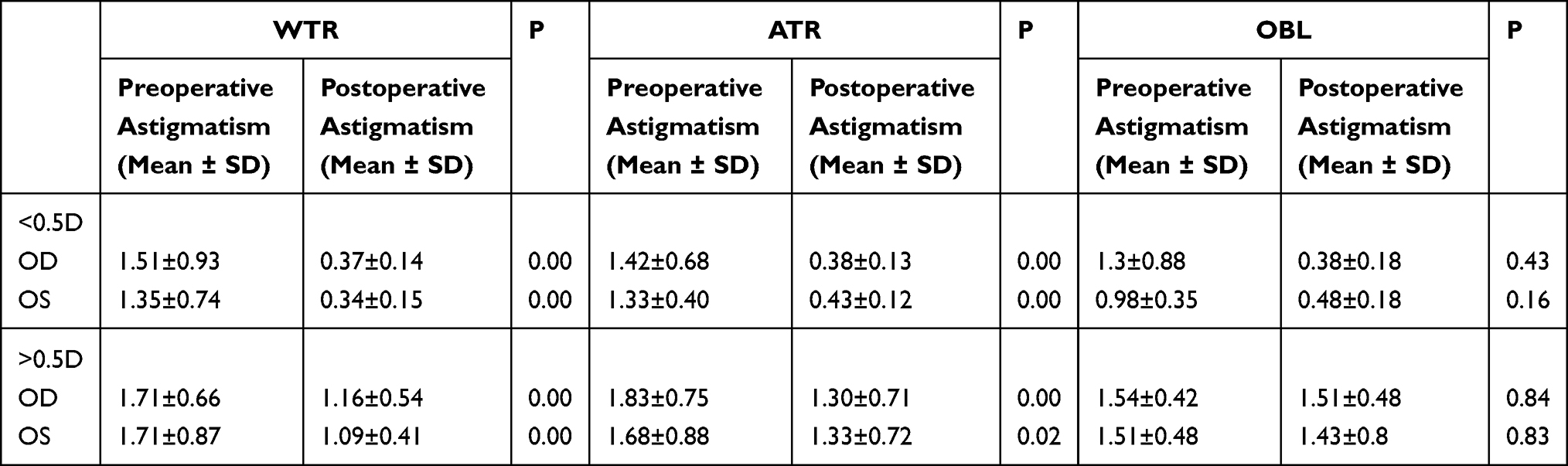 |
Table 3 Comparison of Right and Left Eye Astigmatism |
Vector analysis using Alpin’s Method for target-induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector (DV), and correction index (CI). The differences in preoperative astigmatism were assessed by dividing the groups into ATR (Figure 1), WTR (Figure 2), and Oblique (Figure 3).
 |
Figure 1 Angle plots by Alpin’s Method for target-induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector (DV), correction index (CI) in ATR group. |
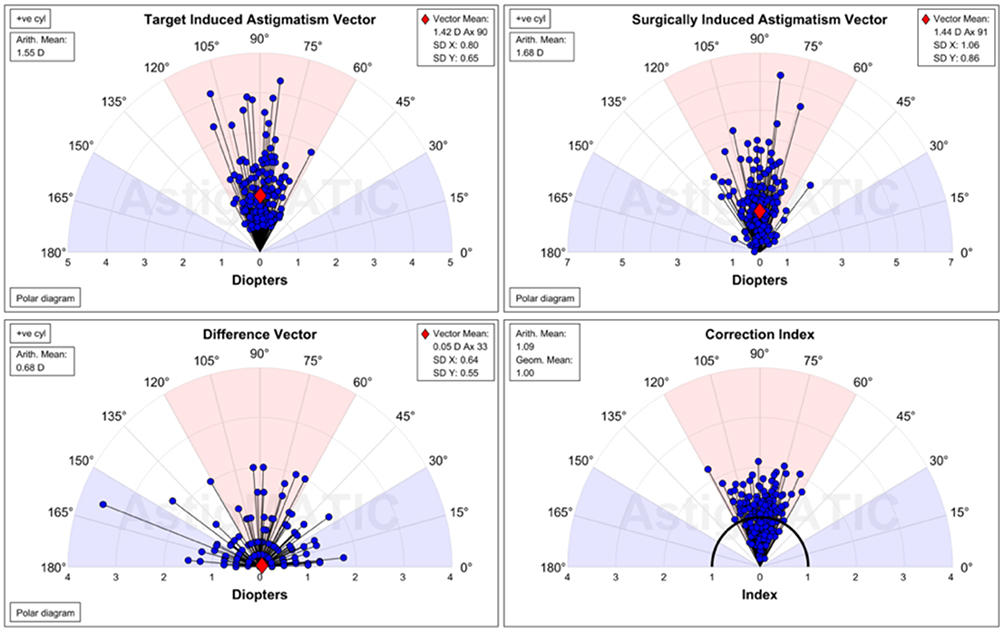 |
Figure 2 Angle plots by Alpin’s Method for target induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector (DV), correction index (CI) in WTR group. |
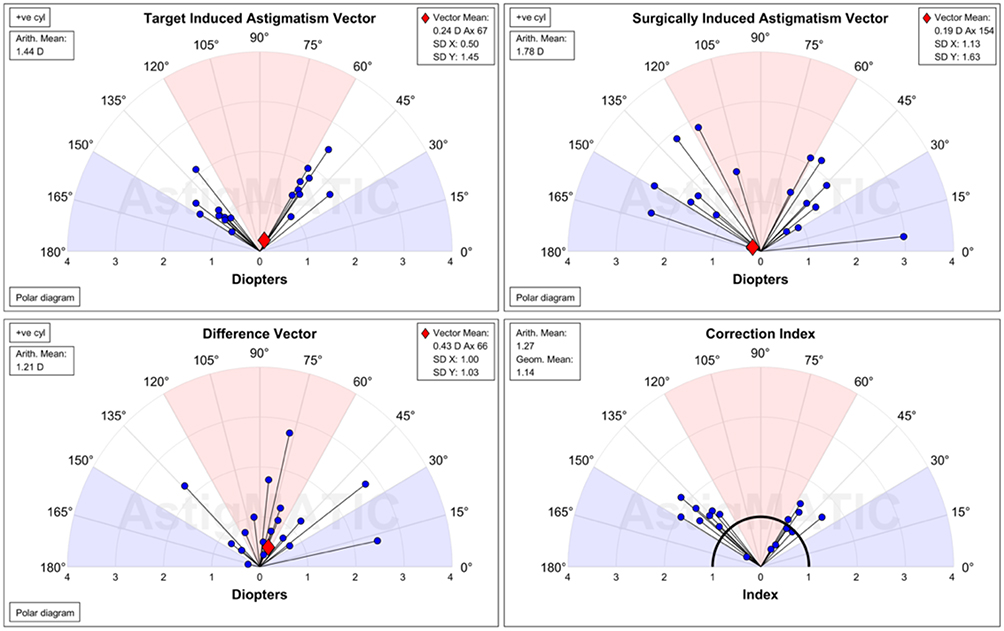 |
Figure 3 Angle plots by Alpin’s Method for target induced astigmatism (TIA), surgically induced astigmatism (SIA), difference vector (DV), correction index (CI) in OBL group. |
SIA magnitude (1.83 D) of the arithmetic mean was higher than the TIA magnitude (1.62 D) in ATR group, indicating overcorrection. The vector mean of SIA (1.57 D) and TIA (1.47 D) also represents overcorrection and is consistent with the arithmetic mean. Vector mean of DV 0.12 D and the arithmetic mean of DV 1.02 D with 11.7% error of 0.82–1.12 D. By dividing DV to TIA, index of success (IOS) is a relative measure of success of treatment. IOS for ATR group was 0.67. Correction index (1.17) indicates overall overcorrection in ATR group.
The arithmetic mean of SIA magnitude (1.68 D) was more than the TIA magnitude (1.55D), which indicates an overall overcorrection in WTR group. Vector mean values of SIA (1.44 D) and TIA (1.42 D) in the WTR group conclude slight overcorrection consistent with the arithmetic mean. The vector mean of difference vector (DV) in the WTR group (0.05 D) and arithmetic mean of 0.68 D. The DV is an absolute measure of success and is preferably by zero. The DV measures the induced astigmatic change by the surgery to achieve its intended target. IOS in WTR (0.50) was more favourable than ATR (0.67). Correction index (CI) of WTR (1.09), the WTR group was the closest to 1.00, indicating neither overcorrection nor under correction. Therefore, LRI in the WTR group has a favourable outcome.
The same overall correction was also found in the oblique group, with SIA magnitude (1.78 D) and TIA magnitude (1.44 D). The vector mean of SIA (0.19 D) was lower than the TIA (0.24 D). The vector mean of DV 0.43 D and arithmetic mean 1.21 D in oblique group have the highest error compared to ATR and WTR (0.7–1.6 D). The correction index was also found to be the highest in the oblique group. In addition to the lowest number of significant decreases in post-op astigmatism, overall correction of oblique groups was found to be ineffective.
Patients with with-the-rule (WTR) astigmatism in the right eye had a higher intended correction rate with no shift in meridian outcomes (38.5%) (Table 4). There was an almost equal proportion of overcorrection, with postoperative shifts to against-the-rule (ATR) astigmatism (30.18%) and unpredictable meridional shifts to oblique (OBL) astigmatism (32.08%). The shift from with-the-rule (WTR) to against-the-rule (ATR) astigmatism was observed to be higher in the right eye (30.18%) compared to the left eye (25.5%). In the left eye of WTR group, a higher percentage of patients achieved the intended postoperative target (25.5%), but this was accompanied by a more unpredictable shift towards oblique astigmatism (49%).
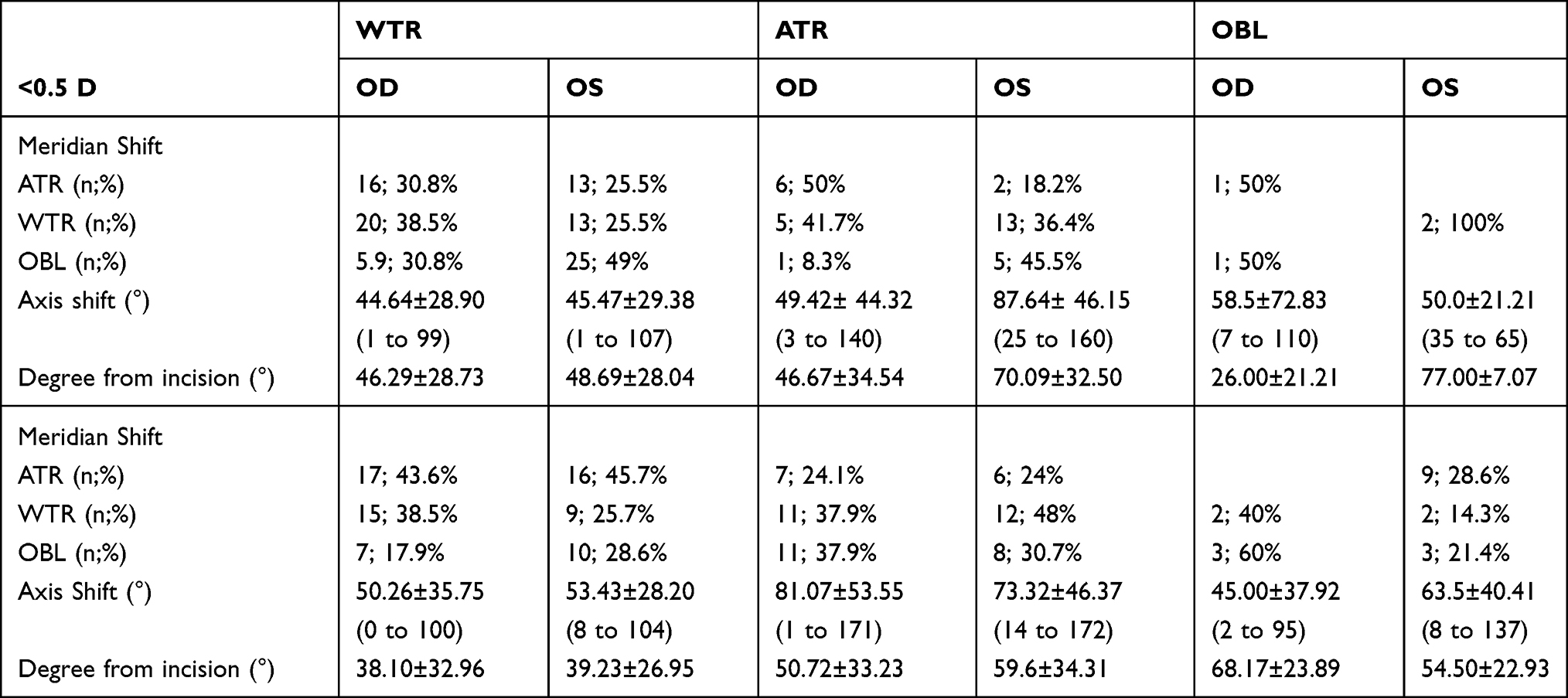 |
Table 4 Postoperative Shift of Astigmatism |
Similar outcome characteristics were observed in against-the-rule (ATR) astigmatism, where the intended postoperative astigmatism meridian was also more common in the right eye (50%) compared to the left eye (18.2%). Overcorrection, which resulted in a shift to WTR, was also higher in the right eye (41.7%) compared to the left eye (36.4%). Unpredictable shifts, resulting in oblique astigmatism, were more common in the left eye (45.5%).
In oblique astigmatism, we found that correction in the intended meridian was only observed in the right eye (50%). Both eyes showed unpredictable postoperative meridian shifts. Astigmatism shifts from oblique were found for the ATR (50%) and WTR (100%) meridian in both the right and left eyes. The group with oblique astigmatism exhibited the smallest sample size, rendering it less amenable to meaningful comparisons with other groups.
Among patients with WTR astigmatism who did not achieve the intended target, there was more overcorrection in the left eye (45.7%), under-correction in the right eye (38.5%), and unpredictable outcomes in the left eye (28.6%). For patients with ATR astigmatism and >0.5D postoperative astigmatism, there was a higher under-correction in the left eye (48%), almost equal overcorrection in the right eye (24.1%) and left eye (24%), and higher unpredictable outcomes in the right eye (37.9%). Patients with oblique astigmatism showed highly unpredictable shifts. All groups exhibited higher rates of overcorrection and unpredictable shifts in both the right and left eyes.
In the right eye, counter clockwise (CCW) rotation was more common in the WTR and ATR groups, while in contrast, clockwise (CW) rotation was more common in the WTR, ATR, and OBL groups in the left eye (Table 5). Compared to previous studies, CW rotation was higher in both the right (60.9%) and left (57.1%) eyes.
 |
Table 5 The Direction of Rotation in Postoperative Astigmatism <0.5D |
Different results were found in patients with >0.5D postoperative astigmatism, where CW rotation was higher in the ATR group for both the left and right eyes, while CCW rotation was higher in the WTR group for both the left and right eyes (Table 6). In oblique astigmatism, CCW rotation was found in all cases in the right eye and CW rotation was higher in the left eye.
 |
Table 6 The Direction of Rotation in Postoperative Astigmatism >0.5D |
Postoperative astigmatism follow-up was performed using an automated keratometry (Table 6). Similar results were observed for the WTR and ATR groups, with a significant reduction in astigmatism observed at the 1-week, 1-month, and 3-month follow-up intervals. However, the oblique group did not show a significant decrease in astigmatism. A significant reduction in postoperative astigmatism was observed in the ATR and WTR groups.
Postoperative visual acuity was assessed in all patients (Table 7). However, it is important to note that not all patients were specifically targeted to achieve emmetropia, as this outcome depended on factors such as the choice of intraocular lens (IOL) and individual patient preferences. Consequently, the impact of residual astigmatism on visual acuity could not be quantified. Nevertheless, there was a notable overall improvement in both best-corrected visual acuity and uncorrected visual acuity across all study groups.
 |
Table 7 Preoperative and Postoperative Visual Acuity in WTR, ATR, and OBL Astigmatism Group |
Multivariate analysis of age, WTW, arc length, axial length, and torque axis were analyzed to determine factors influencing the decrease in astigmatism overall data (Table 8). Age was a significant parameter for ATR astigmatism reduction (p=0.018), arc length (p=0.000), and torque axis (0.000) were significant for WTR astigmatism.
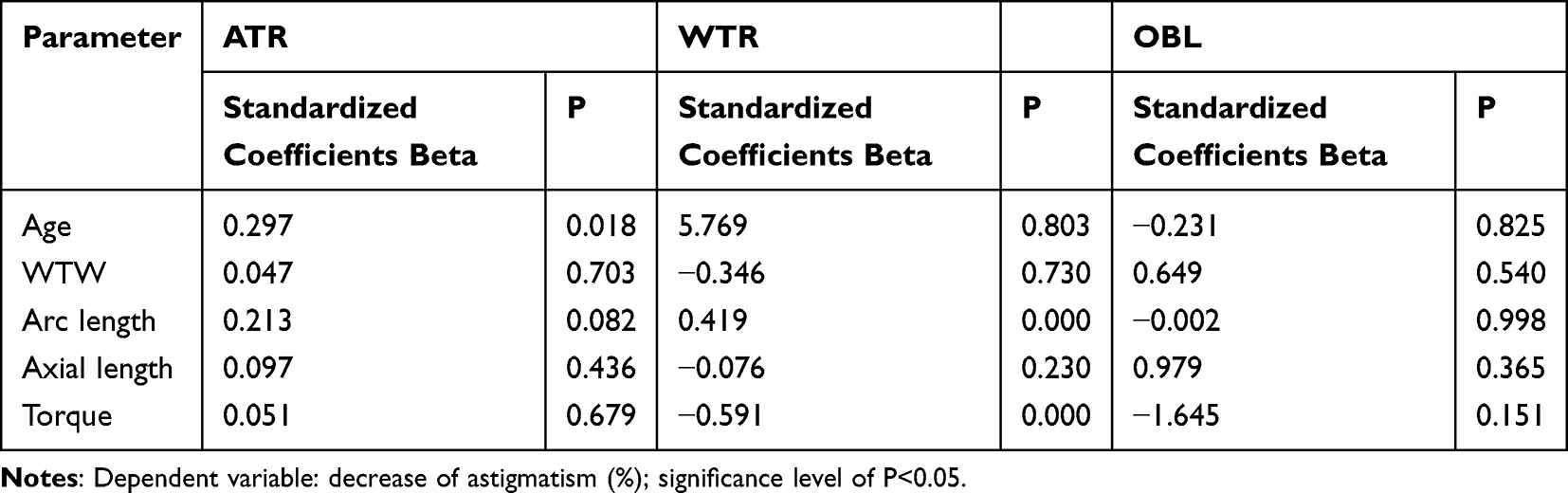 |
Table 8 Multivariate Analysis of Parameters Affecting the Decrease in Astigmatism |
Discussion
Arcus senilis is found to be more frequent in Southeast Asian populations.14 Lin et al conducted a study to examine the effect of arcus senilis on calculating white-to-white (WTW) measurements, as it may impact accuracy.15 Previous research has indicated a shift towards against-the-rule (ATR) astigmatism in older age group due to the aging process.14–16 Furthermore, as part of the aging process, there is a reduction in eyelid pressure, especially in the upper eyelid. These changes have been suggested to contribute to the shift from with-the-rule (WTR) astigmatism to ATR.1,16 Additionally, lid tension is influenced by eye dominance, which varies between the dominant and non-dominant eyes. It has been proposed that the dominant eye, often the right eye in the general population, influences the width of the palpebral fissure.17 While the correlation between eyelid pressure, eye dominance, and aging in relation to the shift in astigmatism has not been determined, this study population exhibited a higher prevalence of ATR in the left eye and WTR in the right eye.
As this study is a retrospective case review, we are unable to precisely determine the effect and correlation of laterality and astigmatism meridian. Sander et al18 stated that only a proportion of subjects with direct astigmatism in their youth change to inverse astigmatism through oblique astigmatism. However, no studies with longitudinal data have been able to support this hypothesis.14 In this study, the oblique group had the fewest subjects, with a minimum age of 47 and a maximum age of 75, which lies between the WTR and ATR groups. Larger data sizes are needed to assess the role of oblique astigmatism as a transition from WTR to ATR. This shift probably needs to be taken into consideration when treating astigmatism in younger populations. We also noted that patients who underwent FLAK in both eyes experienced more complaints in the second eye, which may be due to expectations and pain memory from the first surgery. A previous study also supports our findings, suggesting a correlation between a patient’s anxiety level during their second eye cataract surgery.19 More data regarding patient experiences with FLAK.
Studies have shown that a longer axial length is associated with a steeper cornea, whereas a compensating mechanism of emmetropization causes corneal flattening in low myopia or emmetropia groups. Insufficient emmetropizing capacity can cause the cornea to become steep in moderate myopia, leading to changes in corneal astigmatism, curvature flattening, or steepening, which may impact the eye’s refractive power. An emmetropic state can be achieved through a steep cornea coupled with a relatively short axial length or a flat cornea combined with a relatively long axial length, indicating the presence of coordinated eye growth and an active emmetropization process.20 These findings suggest a correlation between eye growth and an active emmetropization process. No significant differences were found in axial length between groups, which reduced the variability of refractive power and the impact on astigmatism calculation.
Astigmatism corrections aimed to be less than 0.5D have been mentioned to give satisfactory visual acuity.20,21 Based on our data, patients who achieved the intended postoperative astigmatism target experienced various axis shifts in the right or left eye. The same pattern was also found in postoperative astigmatism that did not achieve the intended target. We found similar results regarding oblique astigmatism, which presents a conundrum. Correction of oblique astigmatism yields unfavorable outcomes, with WTR and ATR groups exhibiting more postoperative astigmatism <0.5D. Due to the retrospective nature of this study, we could not distinguish between postoperative astigmatism arising from lenticular or corneal astigmatism. Additionally, we were unable to assess patient spectacles independence with respect to astigmatism correction and the use of extended depth of focus IOLs. In addition to the refraction correction performed during cataract surgery, the patient’s ability to adapt is also an important factor in achieving optimal results. Further studies are needed to assess the effect of astigmatism correction on patient adaptation to achieve spectacle independence.
We further analyzed probable factors. We used the Ziemer Femtosecond Laser System, which is not able to detect cyclotorsion or intraoperative misalignments. One downside of this system is the absence of marking iris to determine the intended correction axis precisely. Femtosecond laser system aims to create accurate and less variable incisions with more consistency in arc length, depth, and position. Precision is one of the parameters for predictable outcomes, which needs to be improved using this laser system. According to Euler’s theorem, an axis deviation of 5, 10, or 15 degrees results in a reduction of 17%, 33%, and 50% in the correction, respectively.4 Theoretical modeling allows the calculation of residual astigmatism resulting from axis error using the formula C = 2F × sinα. In this equation, C represents residual astigmatism, F is the original astigmatic error, and α represents the axis misalignment. Based on this equation, a 10-degree axis misalignment can result in a 34% undercorrection of astigmatism.22,23 Astigmatism deviation after correction was considered tolerable, with good patient satisfaction at 10 degrees. Therefore, to reduce cyclorotation and minimize deviation, the routine use of imaging-guided systems and cyclotorsion correction in modern refractive corneal surgery has been suggested. It is likely that femtosecond laser-assisted cataract surgery with astigmatic keratotomies also involves cyclorotation due to various factors such as the patient lying supine, head positioning, and docking placement. The placement of the docking system may also contribute to misalignment during the procedure, which can be caused by the suction forces of the interface ring and the vertical compressive forces of the laser projector. Previous studies using combined topography and LENSAR found small cyclotorsion (5.81°), and a combination of Verion and Zeimer found 2.66° to 8.08° of cyclotorsion.23,24 It can be concluded that marking with an imaging-guided system may reduce cyclotorsion and aid in achieving greater precision of astigmatism correction during cataract surgery. In our study, we did not use any imaging-guided systems, which resulted in a wide range of astigmatism shifts. We conclude that using both imaging-guided and iris registration systems has the potential to play a crucial role in increasing the accuracy of astigmatic correction.
In addition to laser systems, surgeons face the challenging task of determining which preoperative astigmatic measurements to utilize for surgical planning. In this study, astigmatism measurements were acquired through K and TK from the IOL Master 700, which also presents as this study limitation. According to a previous investigation, the IOL Master 700 tends to underestimate corneal astigmatism compared to manual keratometry and the Pentacam. Moreover, WTW distance calculation by the IOL Master 700 may deviate by up to 0.78 mm in comparison to the Pentacam HR, emphasizing that these two devices should not be employed interchangeably.25,26 Hence, based on our findings, for improved outcomes, it may be advisable to enhance astigmatism measurement and preoperative assessment by conducting two distinct assessments using the IOL Master 700 and Pentacam. Beyond astigmatism values, the imaging provided by the Pentacam can also elucidate corneal curvature and topography. Pentacam employs a rotating Scheimpflug camera to capture multiple images of the anterior eye segment, subsequently amalgamating them to generate a three-dimensional (3D) map of the eye.27 This capability enables precise and comprehensive analysis of the cornea and other anterior eye structures, which can be invaluable when planning limbal relaxing incisions or astigmatic keratotomy.28 A primary advantage of the Pentacam for astigmatism calculations is its capacity to measure the entire cornea, not just the central 3 mm as seen in traditional manual or automated keratometry. This expanded coverage permits a more accurate assessment of the cornea’s true shape, particularly beneficial for patients with irregular or distorted corneas. Additionally, the Pentacam can measure astigmatism at various meridians on the cornea and compute the axis of astigmatism, aiding in the determination of the most suitable surgical approach for astigmatism correction.
The variability of wound healing also plays a significant role in the predictability of astigmatism reduction outcomes.29–31 The population exhibits variation in corneal biomechanical properties, as indicated by measurements of corneal hysteresis and corneal resistance factor. Ziemer Ophthalmic Systems use low-energy pulses, a high repetition rate, and overlapping laser spots for complete and smoother sections to produce effective tissue separation without the need for secondary mechanical tearing. High-energy pulses with low repetition rate, on the other hand, rely on the mechanical tearing of the tissue between the lasers, potentially damaging the adjacent tissue.32 The laser–tissue interaction produced by the laser energy used to make the incisions could affect the surrounding tissue, which can contribute to the wound healing process and, in turn, affect the astigmatism outcome. The full refractive effect of laser arcuate keratotomies may not be exhibited until the incisions are opened due to the variability in the integrity of femtosecond laser incisions.15
Another limitation of this study pertains to the utilization of disparate methodologies for assessing astigmatism, both preoperatively and postoperatively. Preoperatively, corneal astigmatism was quantified employing the IOL Master 700, which facilitated the measurement of both anterior and posterior corneal astigmatism in preparation for surgical correction. Conversely, postoperative assessment relied on automated keratometry. A previous study demonstrated minimal discrepancies (≤0.12 D) among measurements obtained via automated, manual, and simulated keratometry.33 However, the determination of total corneal power using the IOL Master yielded higher astigmatism measurements than those derived from automated or simulated keratometry, primarily because the latter methods do not account for posterior corneal considerations. Relying on a solitary keratometric index to compensate for the posterior corneal factors may not furnish an accurate reflection of the actual corneal astigmatism.34 Consequently, the disparity between preoperative and postoperative astigmatism measurements introduces limitations into the accuracy of the analysis regarding the astigmatism changes induced by FLAK in this study.
Based on a multivariate analysis of parameters affecting the decrease in astigmatism, in the ATR group, age influenced the decrease in postoperative astigmatism. As previous studies have stated, the effect of relaxing incisions of the cornea increases with age. The influence of age is probably due to the modification of the biomechanical properties of the corneal tissue, which are correlated with changes associated with the aging process.35 In the WTR group, arc length and torque significantly correlate with the decrease in astigmatism. Based on our data, although the correction results (<0.5D) of WTR astigmatism were more favorable (44.38%), 49% of the remaining subjects still had residual astigmatism >0.5D. Subjects with remaining astigmatism (>0.5D) showed a higher level of overcorrection. The arc length was adjusted according to astigmatism and age based on the NAPA nomogram, and further analysis was needed to adjust the nomogram for Indonesian populations. Intraoperative misalignment, as mentioned earlier, was highly likely the cause of the torque axis.
Conclusion
WTR consisted of the youngest study participants compared to the ATR and OBL groups. Eye laterality influenced the placement of incisions in overlapping cases, and efforts were made to prevent corneal perforation. The ATR and OBL groups had a higher proportion of subjects with left eyes, while the WTR group had more subjects with right eyes.
Overall, there was a reduction of astigmatism in all groups, with the highest reduction observed in the WTR group, followed by the ATR and OBL groups. In the ATR group with high astigmatism (>2.00 D), FLAK is not a suitable method for astigmatism reduction. Significant decreases in astigmatism were observed in both the right and left eyes of the WTR and ATR groups, while the decrease was not significant in the OBL group.
In the WTR group with astigmatism in the right eye, there was a higher rate of intended correction with no meridian shift. Overcorrection was higher in the right eye compared to the left eye. In the ATR group, the intended astigmatism meridian was more common in the right eye, and overcorrection was higher in the right eye as well. Unpredictable outcomes shifting to oblique astigmatism were more common in the left eye. In the oblique astigmatism group, correction in the intended meridian was only observed in the right eye, while both eyes showed unpredictable postoperative shifts with astigmatism shifting towards ATR and WTR. Our findings indicate that higher astigmatism is more commonly observed in the dominant eye, typically the right eye. Overcorrection and unpredictable shifts in astigmatism were prevalent in all groups in both the right and left eyes.
FLACS combined with the astigmatic keratotomy method may be considered as a method to reduce moderate astigmatism (1.00D to <3.00D). Astigmatism reduction was significantly reduced in 3 months follow-up in with-the-rule and against-the-rule astigmatism. No significant complications were found in this study. Further studies are needed to improve the accuracy and predictability of this method.
Abbreviations
FLACS, femtosecond laser-assisted cataract surgery; ATR, against-the-rule; WTR, with-the-rule; OBL, oblique; D, dioptre; AK, astigmatic keratotomy; WHO, World Health Organization; OCCI, opposite clear corneal incisions; LRI, limbal relaxing incisions; IOL, intraocular lens; CCW, counter clockwise; CW, clockwise; NA, Not applicable.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Global Health. 2017;5(12):e1221–34. doi:10.1016/S2214-109X(17)30393-5
2. Vision impairment and blindness. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment.
3. Chen W, Zuo C, Chen C, et al. Prevalence of corneal astigmatism before cataract surgery in Chinese patients. J Cataract Refract Surg. 2013;39(2):188–192. doi:10.1016/j.jcrs.2012.08.060
4. Nichamin LD. Nomogram for limbal relaxing incisions. J Cataract Refract Surg. 2006;32(9):1408. doi:10.1016/j.jcrs.2006.03.046
5. Chan TCY, Ng AL, Cheng GP, Wang Z, Woo VC, Jhanji V. Corneal astigmatism and aberrations after combined femtosecond-assisted phacoemulsification and arcuate keratotomy: two-year results. Am J Ophthalmol. 2016;170:83–90. doi:10.1016/j.ajo.2016.07.022
6. Roberts HW, Wagh VK, Sullivan DL, Archer TJ, O’Brart DPS. Refractive outcomes after limbal relaxing incisions or femtosecond laser arcuate keratotomy to manage corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg. 2018;44(8):955–963. doi:10.1016/j.jcrs.2018.05.027
7. Visco DM, Bedi R, Packer M. Femtosecond laser-assisted arcuate keratotomy at the time of cataract surgery for the management of preexisting astigmatism. J Cataract Refract Surg. 2019;45(12):1762–1769. doi:10.1016/j.jcrs.2019.08.002
8. Nichamin LD. Astigmatism Control. Ophthalmol Clin. 2006;19(4):485–493.
9. Núñez MX, Henriquez MA, Escaf LJ, et al. Consensus on the management of astigmatism in cataract surgery. Clin Ophthalmol. 2019;13:311–324. doi:10.2147/OPTH.S178277
10. Fouda S, Kamiya K, Aizawa D, Shimizu K. Limbal relaxing incision during cataract extraction versus photoastigmatic keratectomy after cataract extraction in controlling pre-existing corneal astigmatism. Graefes Arch Clin Exp Ophthalmol. 2010;248(7):1029–1035. doi:10.1007/s00417-009-1272-6
11. Nagy Z, Takacs A, Filkorn T, Sarayba M. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery. J Refract Surg. 2009;25(12):1053–1060. doi:10.3928/1081597X-20091117-04
12. Alió JL, Abdou AA, Puente AA, Zato MA, Nagy Z. Femtosecond laser cataract surgery: updates on technologies and outcomes. J Refract Surg. 2014;30(6):420–427. doi:10.3928/1081597X-20140516-01
13. Mester U, Vaterrodt T, Goes F, et al. Impact of personality characteristics on patient satisfaction after multifocal intraocular lens implantation: results from the happy patient study. J Ref Surg. 2014;30(10):674–678. doi:10.3928/1081597X-20140903-05
14. Asano K, Nomura H, Iwano M, et al. Relationship between astigmatism and aging in middle-aged and elderly japanese. Jpn J Ophthalmol. 2005;49(2):127–133. doi:10.1007/s10384-004-0152-1
15. Collier Wakefield O, Annoh R, Nanavaty MA. Relationship between age, corneal astigmatism, and ocular dimensions with reference to astigmatism in eyes undergoing routine cataract surgery. Eye. 2016;30(4):562–569. doi:10.1038/eye.2015.274
16. Namba H, Sugano A, Murakami T, et al. Age-related changes in astigmatism and potential causes. Cornea. 2020;39:S34. doi:10.1097/ICO.0000000000002507
17. Doganay F, Dadaci Z, Topcu-Yilmaz P, Doganay Aydin H. The association between ocular dominance and physiological palpebral fissure asymmetry. Laterality. 2017;22(4):412–418. doi:10.1080/1357650X.2016.1209212
18. Saunders H. Changes in the axis of astigmatism: a longitudinal study. Ophthal Physiolog Optic. 1988;8(1):37–42. doi:10.1111/j.1475-1313.1988.tb01080.x
19. Jiang L, Zhang K, He W, Zhu X, Zhou P, Lu Y. Perceived pain during cataract surgery with topical anesthesia: a comparison between first-eye and second-eye surgery. J Ophthalmol. 2015;2015:1–6. doi:10.1155/2015/383456
20. Han SU, Ryu S, Jung H, et al. Analysis of keratometric measurements in accordance with axial length in an aged population. Sci Rep. 2022;12(1):4087. doi:10.1038/s41598-022-08194-0
21. Villegas EA, Alcón E, Artal P. Minimum amount of astigmatism that should be corrected. J Cataract Refract Surg. 2014;40(1):13–19. doi:10.1016/j.jcrs.2013.09.010
22. Bradley MJ, Coombs J, Olson RJ. Analysis of an approach to astigmatism correction during cataract surgery. Ophthalmologica. 2006;220(5):311–316. doi:10.1159/000094621
23. Hummel CD, Diakonis VF, Desai NR, Arana A, Weinstock RJ. Cyclorotation during femtosecond laser–assisted cataract surgery measured using iris registration. J Cataract Refract Surg. 2017;43(7):952–955. doi:10.1016/j.jcrs.2017.04.034
24. Lin HY, Chuang YJ, Lin PJ, Ho YJ. Novel method for preventing cyclorotation in Ziemer Femto LDV Z8 femtosecond laser-assisted cataract surgery with Verion image-guided system. Clin Ophthalmol. 2019;13:415–419. doi:10.2147/OPTH.S177219
25. Chan TCY, Wan KH, Tang FY, Wang YM, Yu M, Cheung C. Repeatability and agreement of a swept-source optical coherence tomography–based biometer IOLMaster 700 versus a scheimpflug imaging–based biometer AL-scan in cataract patients. Eye Contact Lens. 2020;46(1):35. doi:10.1097/ICL.0000000000000603
26. Gill ES, Le C, Joseph J, Munir WM. Comparison of Preoperative Parameter Measurements Using an Optical Biometer, Automated Keratometer, and a Placido-Based Topographer Module. Eye Contact Lens. 2020;46(1):46. doi:10.1097/ICL.0000000000000605
27. Park DY, Lim DH, Hwang S, Hyun J, Chung TY. Comparison of astigmatism prediction error taken with the pentacam measurements, Baylor nomogram, and Barrett formula for toric intraocular lens implantation. BMC Ophthalmol. 2017;17(1):1–9. doi:10.1186/s12886-017-0550-z
28. Lim CW, Somani S, Chiu HH, Maini R, Tam ES. Astigmatic outcomes of single, non-paired intrastromal limbal relaxing incisions during femtosecond laser-assisted cataract surgery based on a custom nomogram. Clin Ophthalmol. 2020;1059–1070. doi:10.2147/OPTH.S238016
29. Azar DT, Chang JH, Han KY. Wound healing after keratorefractive surgery: review of biological and optical considerations. Cornea. 2012;31(0 1):S9–19. doi:10.1097/ICO.0b013e31826ab0a7
30. Jester JV, Villaseñor RA, Schanzlin DJ, Cavanagh HD. Variations in corneal wound healing after radial keratotomy: possible insights into mechanisms of clinical complications and refractive effects. Cornea. 1992;11(3):191–199. doi:10.1097/00003226-199205000-00002
31. Spadea L, Giammaria D, Trabucco P. Corneal wound healing after laser vision correction. Br J Ophthalmol. 2016;100(1):28–33. doi:10.1136/bjophthalmol-2015-306770
32. Latz C, Asshauer T, Rathjen C, Mirshahi A. Femtosecond-laser assisted surgery of the eye: overview and impact of the low-energy concept. Micromachines. 2021;12(2):122. doi:10.3390/mi12020122
33. Visser N, Berendschot TT, Verbakel F, de Brabander J, Nuijts RM. Comparability and repeatability of corneal astigmatism measurements using different measurement technologies. J Cataract Refract Surg. 2012;38(10):1764–1770. doi:10.1016/j.jcrs.2012.05.036
34. Srivannaboon S, Chirapapaisan C, Chonpimai P, Comparison of corneal astigmatism and axis location in cataract patients measured by total corneal power, automated keratometry, and simulated keratometry. J Cataract Refract Surg. 2012;38(12):2088–2093. doi:10.1016/j.jcrs.2012.07.024
35. Cristóbal JA, Del Buey MA, Ascaso FJ, Lanchares E, Calvo B, Doblaré M. Effect of limbal relaxing incisions during phacoemulsification surgery based on nomogram review and numerical simulation. Cornea. 2009;28(9):1042–1049. doi:10.1097/ICO.0b013e3181a27387
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.