Back to Journals » Clinical Ophthalmology » Volume 20
Combined Burst Mode versus Torsional Mode Phacoemulsification for Patients with Hard Nuclear Cataracts: A Prospective Comparative Cohort Study
Authors Ainiwaer M ![]() , Hong Y, Xiao B, Sun Y, Zhang S, Ning L, Liu H, Zhu X
, Hong Y, Xiao B, Sun Y, Zhang S, Ning L, Liu H, Zhu X ![]() , Ji Y
, Ji Y ![]()
Received 19 December 2025
Accepted for publication 7 March 2026
Published 13 March 2026 Volume 2026:20 587531
DOI https://doi.org/10.2147/OPTH.S587531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Maierdanjiang Ainiwaer,1– 3,* Yingying Hong,1– 3,* Binghe Xiao,1– 3 Yang Sun,1– 3 Shaohua Zhang,1– 3 Li Ning,1– 3 Houyi Liu,1– 3 Xiangjia Zhu,1– 3 Yinghong Ji1– 3
1Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China; 2Key Laboratory of Myopia and Related Eye Diseases, NHC Key Laboratory of Myopia, Chinese Academy of Medical Sciences, Shanghai, 200031, People’s Republic of China; 3Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai, 200031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yinghong Ji, Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China, Email [email protected]
Purpose: To evaluate the hard nuclear cataract surgery outcomes by comparing the combined burst mode and continuous torsional mode conducted of Centurion Vision System.
Methods: Prospective comparative cohort study. Based on the Emery-Little classification, this study assigned cataract patients with nuclear density grade III to V into two groups: the combined mode group (Group A) and the torsional mode group (Group B). Endothelial cell density (ECD), central corneal thickness (CCT), and best-corrected distance visual acuity (BCVA) were evaluated at different time intervals, including 1 day, 1 week, 1 month, and 3 months.
Results: 207 patients: 100 in the group A and 107 in the group B. Patients in group A with severe nuclei experienced lower cumulative dissipated energy (p = 0.007) and shorter ultrasound time (p < 0.001). Both groups exhibited a decrease in ECD after surgery, but the decrease was comparatively lower among group A patients with severe nuclei (p < 0.05). There was a notable increase in the CCT in both groups at the 1-day and 1-week time points compared to the baseline values (p < 0.001). Changes in CCT were significantly greater in group B at 1-day (p < 0.001), 1-week (p = 0.002), and 1-month (p = 0.004) intervals among patients with severe nuclei.
Conclusion: Burst torsional combined with longitudinal ultrasound can be more effective for harder nuclei phacoemulsification than the continuous torsional ultrasound.
Trial Registration: This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Fudan University’s Eye & ENT Hospital. This study was registered as a clinical trial (number: NCT06991374).
Keywords: hard nuclear cataract, burst mode, torsional mode, phacoemulsification
Introduction
Phacoemulsification, a widely acknowledged surgical procedure for cataract extraction, has significantly enhanced the safety and efficacy of the operation.1–3 Nevertheless, during the surgical process of hard nucleus cataract removal, the utilization of higher-intensity ultrasound energy in phacoemulsification poses a potential risk of tissue damage and elevates the surgical risk for patients with hard nucleus cataracts, including those with corneal endothelial dysfunction postsurgery.4
With a primary emphasis on enhancing efficiency and safety, phacoemulsification equipment has undergone numerous technological advancements. These include the transition from conventional longitudinal ultrasound to the introduction of burst or pulse mode ultrasound, and presently, the adoption of torsional mode and combined burst mode. All these technological enhancements have been devised with the objective of diminishing the utilization of ultrasound energy and mitigating the extent of surgical harm inflicted upon the cornea. The burst mode has been acknowledged as a means to decrease the mean ultrasound time (UST) and cumulative dissipated energy (CDE).5 Compared to the conventional continuous mode, the burst mode is deemed more appropriate for the treatment of hard nuclear cataracts.3,6 Furthermore, the NeoSoniX ultrasound and torsional modes have been reported to exhibit greater efficacy in the management of hard nuclear cataracts than the traditional phacoemulsification mode.7–9 Currently, the use of the torsional ultrasound mode in phacoemulsification is extensive. The advent of the torsional mode has resulted in the neglect of the burst mode. Nevertheless, in the realms of clinical practice, the combination of torsional ultrasound with traditional ultrasound in burst mode may prove to be more effective than relying solely on the torsional mode, particularly when treating hard nuclear cataracts. However, direct comparative data on combined burst mode versus continuous torsional mode specifically for hard nuclear cataracts remain limited. This study aimed to address this gap.
Hence, a prospective comparative cohort study was conducted to assess the clinical efficacy, safety, and postoperative outcomes of torsional ultrasound combined with traditional ultrasound in burst mode and continuous torsional mode phacoemulsification for patients undergoing hard nuclear cataract surgery.
Materials and Methods
Patient Selection
Patients who underwent cataract surgery at the Eye, Ear, Nose, and Throat Hospital at Fudan University between August 2024 and August 2025 were enrolled in this prospective study. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Fudan University’s Eye & ENT Hospital. This study was registered as a clinical trial (number: NCT06991374). Informed consent was obtained from all patients.
The study recruited patients with age-related cataracts who were classified as nuclear hardness grade III–V only by Emery Little.10 Patients with white cataracts, a history of eye surgery, or eye diseases such as corneal pathology, uveitis, Fuchs’ dystrophy, or glaucoma were excluded. Additional inclusion criteria included a minimum dilated pupil diameter of 7 mm or above and a corneal endothelial cell count exceeding 1200/mm2. Patients were assigned to either the combined burst mode group (Group A) or the torsional mode group (Group B) based on the operating surgeon’s clinical preference. The surgeon (J.Y.H.) selected the phacoemulsification mode for each eligible patient according to routine practice, without any predefined randomization scheme. All consecutive patients meeting the inclusion criteria during the study period were enrolled. According to the nuclear grade, each group was divided into two subgroups: patients with grade III moderate nuclear cataract and patients with grade IV to V severe nuclear cataract.
Preoperative and postoperative measurements were taken by a single ophthalmologist. Comprehensive ophthalmic examination included the evaluation of corrected distance visual acuity (BCVA) and the assessment of corneal clarity through slit-lamp examination, which involved determining the presence of either a clear cornea or stromal edema/Descemet membrane folds.11 The central corneal thickness (CCT) and the anterior chamber depth (ACD) was measured using Scheimpflug imaging technology provided by Oculus Optikgerate GmbH. For baseline and postoperative imaging, all patients were examined with an EM-3000 autofocus specular microscope (Tomey Corp).
Surgical Procedure
In accordance with the standard protocol, all surgeries were performed by the same experienced surgeon (J.Y.H). Prior to the surgical procedure, all patients were administered topical levofloxacin (0.5%) at a frequency of four times daily over a duration of three days. One percent tropicamide eye drops were used to dilate the pupils before surgery.
Subsequently, all individuals scheduled for surgery were allocated to either the combined mode group (Burst Tor+ Burst US, Group A) or the torsional mode group (Linear Tor, Group B).
In both groups, 2.2-mm corneal incisions and 0.8-mm side-port incisions were made, and a viscoelastics of sodium hyaluronate 3.0% and chondroitin sulfate 4.0% (Viscoat, Alcon) was used in the surgery. Continuous curvilinear capsulorhexis ranging from 5.5 to 6.0 mm was performed using capsule forceps. Phacoemulsification was conducted on both groups utilizing Centurion Vision Systems (Centurion, Alcon) using divide and conquer technique. Group A patients underwent phacoemulsification in combined burst mode, while group B patients underwent phacoemulsification in continuous torsional mode. The anterior chamber was then injected with a cefuroxime solution of 1 mg/0.1 mL. The phacoemulsification parameters are presented in Table 1.
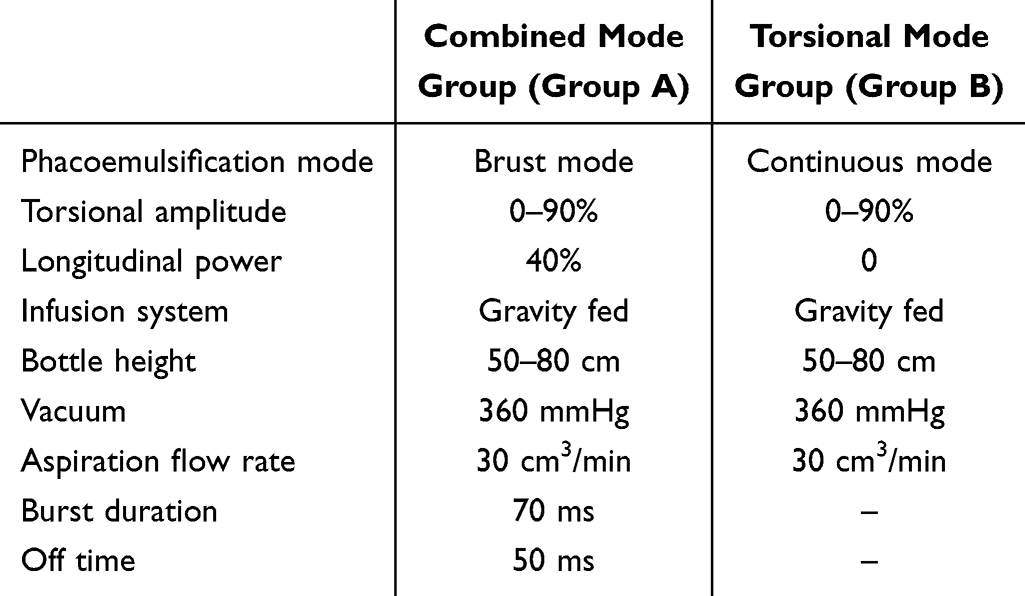 |
Table 1 Parameters for the Combined Mode Group (Burst Tor+ Burst US, Group A) and the Torsional Mode Group (Linear Tor, Group B) |
The postoperative regimen consisted of topical steroids (1% prednisolone acetate), topical nonsteroidal anti-inflammatory drugs (0.1% pranoprofen), and antibiotic eye drops (0.5% levofloxacin) for 4 weeks.
Measurements
During the surgical procedure, the following intraoperative parameters were documented: CDE, UST, and occlusion time. Preoperative ECD, CCT, corneal edema, and BCVA were obtained, as well as measurements at 1 day, 1 week, 1 month, and 3 months postsurgery. Both intraoperative and postoperative complications were recorded. All conditions were maintained for all eyes undergoing surgery by a technician who was not aware of the patient groupings.
Sample Size
The difference in CCT between group A and group B was assumed to be 15 μm on the first day after surgery. The power was estimated to be 80%, with a p value of 0.05. A sample size of 86 eyes in each group was needed. After allowing for 20% patient dropout, 207 patients were enrolled.
Statistical Analysis
We used SPSS 25 to conduct all the statistical analyses. All primary endpoints and subgroup analyses (by nuclear grade) were predefined in the study protocol. The normality of the data was assessed using the Kolmogorov‒Smirnov test, and the appropriate statistical methods were used. Using Mann‒Whitney U-tests and t tests, disparities in CDE and UST among the two groups were compared, as were postoperative changes in ECD and CCT. The categorical data are presented as percentages and numbers, and chi-square or continuity-corrected chi-square tests were used to analyze the results. A p value less than 0.05 indicated statistical significance.
Results
The study included a total of 207 eyes, 100 in Group A (combined mode group) and 107 in Group B (torsional mode group). Figure 1 illustrates the patient inclusion and follow-up process. The groups did not show any statistically significant differences in preoperative ECD, CCT, BCVA, anterior chamber depth or nuclear grading, as shown in Table 2.
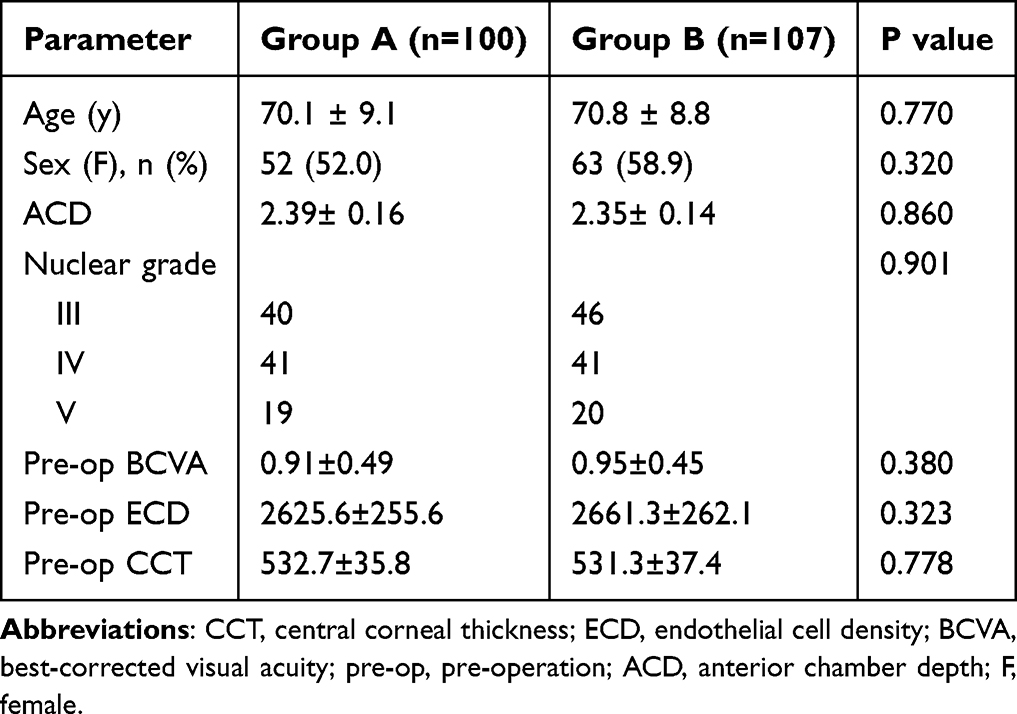 |
Table 2 Baseline Demographics in Both Groups |
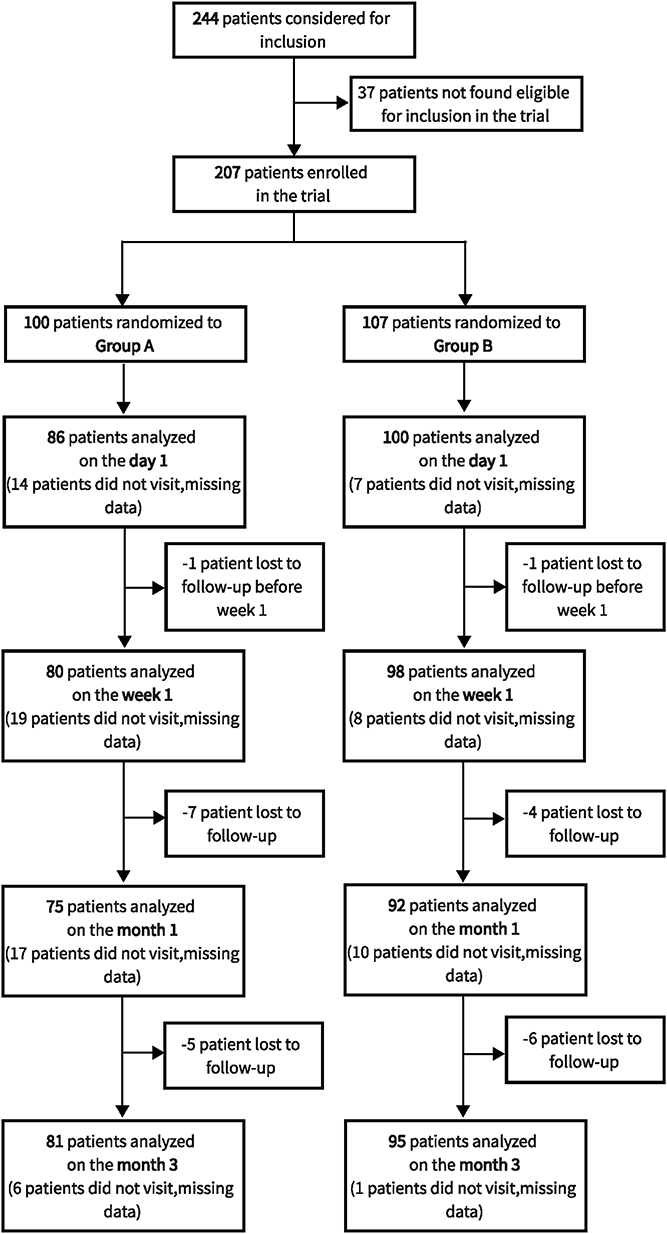 |
Figure 1 Flow diagram depicting patient inclusion and follow-up. Bold text indicates follow‑up time points and the number of patients analyzed at each time point. |
Cumulative Dissipated Energy and Ultrasound Time
The mean CDE values were 9.37 ± 4.90 and 10.90 ± 7.46 in group A and group B, respectively, with no statistically significant differences observed (p = 0.469). Among Grade III moderate nuclear cataracts, group A and B did not differ significantly in terms of CDE grade. However, group A demonstrated a lower CDE for severe nuclei (grade IV–V) than did Group B (group A:11.50±5.04; group B:15.05±7.47; p = 0.007). Additionally, group A had significantly shorter USTs than did group B in patients with moderate (group A:28.82±9.44; group B:34.77±10.64; p = 0.008) or severe (group A:36.84±15.61; group B:63.82±25.64; p < 0.001) nuclear cataracts. The observed trend indicates a consistent increase in UST and CDE measurements in eyes exhibiting higher grades of nuclear density (Table 3).
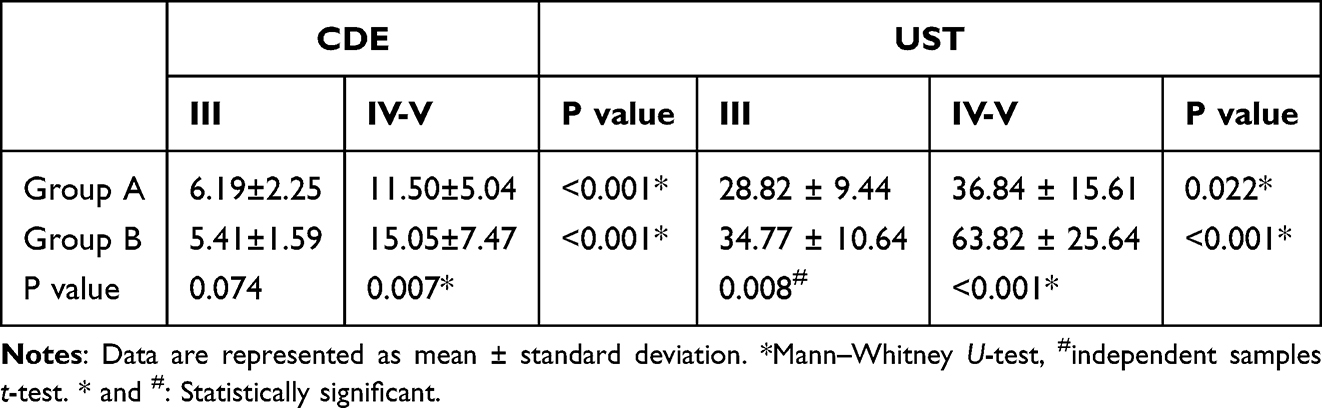 |
Table 3 Cumulative Dissipated Energy (CDE) and Mean Ultrasound Time (UST) in the 2 Groups During Surgery |
Postoperative ECD and CCT
The mean preoperative CCT values were 532.7 ± 35.8 μm and 531.3 ± 37.4 μm in Group A and Group B, respectively (p = 0.778). After surgery, there was a statistically significant increase in the CCT compared to the baseline at 1 day and 1 week in both groups (p < 0.001). Additionally, the changes in CCT between the preoperative data and postoperative follow-up time points were significantly greater in Group B than in Group A at 1 day (p < 0.001), 1 week (p = 0.002), and 1 month (p = 0.004) among patients with severe nuclei after surgery. There were no statistically significant differences observed in the changes in CCT at any time point between group A and group B, specifically in relation to moderate nuclear cataracts of Grade III, as indicated in Table 4 and Figure 2.
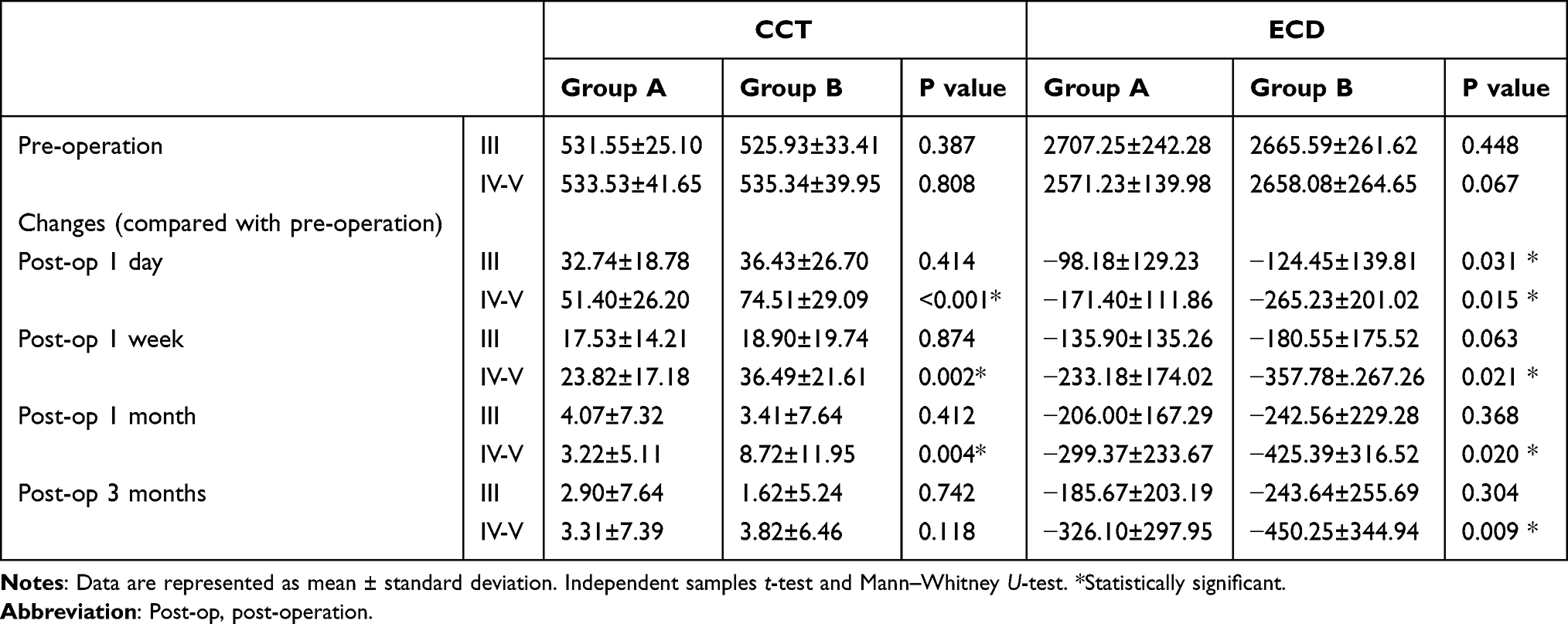 |
Table 4 Changes of Central Corneal Thickness (CCT, μm) and Endothelial Cell Density (ECD, Cells/mm2) in the Two Groups After Surgery |
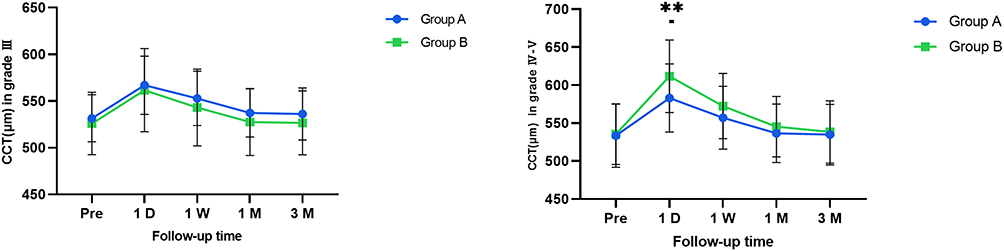 |
Figure 2 CCT changes in moderate nuclear cataract (grade III) and severe nuclear cataract (grade IV–V) patients. **P < 0.01. Abbreviation: CCT, central corneal thickness. |
Prior to the surgical procedure, the average ECD was 2625.6 ± 255.6 cells/mm2 in group A and 2661.3 ± 262.1 cells/mm2 in group B (p = 0.323). The objective of this study was to compare the changes in ECD between two groups at various time intervals. In patients with Grade III nuclear cataracts, Group B showed significantly greater ECD loss than Group A at 1 day postoperatively (p = 0.031), but no significant differences were observed at later time points. In patients with severe nuclear cataracts (Grade IV–V), Group B consistently showed greater ECD loss than Group A at all postoperative time points: 1 day (p = 0.015), 1 week (p = 0.021), 1 month (p = 0.020), and 3 months (p = 0.009). These findings were observed specifically among patients with Grade IV to V nuclear cataracts, as shown in Table 4.
Visual and Refractive Outcomes
The average BCVA before surgery was 0.91 ± 0.49 in group A and 0.95 ± 0.45 in group B, with no significant difference between the two groups (p = 0.380). Both groups showed significant improvements in BCVA after surgery (p < 0.001). Among patients with Grade III and Grade IV–V nuclear cataracts, there were no statistically significant differences in BCVA between the two groups postoperatively (p > 0.05) (Supplemental Table 1a and 1b).
Intraoperative and Postoperative Complications
Supplemental Table 2 presents the occurrence of occlusion within the infusion system during the phacoemulsification procedure, with 2 instances of more than 2 occlusions recorded. Notably, a significant disparity in occlusion frequency was observed between the two groups of patients with Grade IV-V nuclear cataracts (p = 0.020), with Group A exhibiting a lower incidence of occlusions than Group B.
Neither of the two study groups experienced posterior capsular rupture. Over the short-term follow-up period, no postoperative complications, such as fibrin formation, synechiae, macrophages on IOL optics, or endophthalmitis, were observed.
Supplemental Table 3 presents the corneal edema observed in the two groups 1 day and 1 week after the surgical procedure. Among patients with Grade III nuclear cataracts, no statistically significant difference was found between the two groups at either time point (p > 0.05). However, among patients with Grade IV-V nuclear cataracts, the proportion of corneal edema was greater in Group B than in Group A at 1 day post surgery. This difference between the two groups was found to be statistically significant (p = 0.033). Notably, at 1 month after the procedure, no instances of corneal edema were observed in either group.
Discussion
Phacoemulsification IOL implantation is presently the prevailing surgical technique for cataract treatment. Nevertheless, the utilization of ultrasound energy during phacoemulsification poses a substantial risk for surgical trauma, particularly in terms of corneal endothelial cell impairment or dysfunction.12 This impairment is particularly pronounced in patients with hard nuclear cataracts, as it leads to a more substantial decrease in endothelial cell density. Over the years, multiple advancements and enhancements have been made to phacoemulsification surgical equipment to minimize both ultrasound energy and duration.
In traditional phacoemulsification procedures, the cutting action primarily results from the longitudinal movement of the phacoemulsification tip. However, this longitudinal motion often leads to displacement of the nucleus, necessitating a pause to reposition the nucleus back toward the tip.13 The introduction of torsional ultrasound has enhanced the surgical procedure by minimizing the repulsive force exerted on the nucleus during the lateral movement of the tip. Additionally, the phacoemulsification tip maintains continuous contact with the nucleus, thereby enhancing safety in heat transfer, eliminating nuclear repulsion, and facilitating a larger area of phacoemulsification with nuclei.7,14 This advancement significantly improved the efficiency of phacoemulsification. In their prior study, Liu et al established that the utilization of the torsional mode in ultrasound procedures leads to a reduction in energy consumption and a decrease in the duration of ultrasound sessions when compared to the conventional ultrasound mode.7
In addition to the torsional technique, phacoemulsification devices have incorporated novel ultrasound modes to enhance the safeguarding of endothelial cells. Among these techniques, the burst mode stands out for mitigating the transfer of energy to the eye. This is achieved through intermittent activation, enabling the phaco tip to cool between energy pulses, thereby reducing the overall ultrasound time and power employed during the phacoemulsification procedure.15 In circumstances necessitating higher energy levels, such as the emulsification of dense nucleus cataracts, the overall energy consumption can be mitigated by discontinuing the utilization of ultrasound energy.16 The adoption of the burst mode has been demonstrated to substantially decrease energy consumption, resulting in advantageous outcomes such as diminished ocular harm.3,16
Currently, the utilization of continuous mode torsional ultrasound has increased in prevalence in cataract surgery. This study aimed to assess the outcomes of two distinct surgical approaches, namely, the combination of torsional and conventional ultrasound in burst mode versus torsional ultrasound in continuous mode, using the Centurion system in patients with hard nuclear cataracts.
The impact of cataract surgery on corneal endothelial cell damage was evaluated through the assessment of corneal edema, ECD, and CCT. Various factors, including mechanical damage from surgical instruments, contact of lens fragments with endothelial cells, ultrasonic damage caused by energy transfer near endothelial cells, and turbulence resulting from anterior chamber flushing fluid, can contribute to corneal damage following phacoemulsification. To minimize variations in surgical technique, all procedures were performed by the same experienced surgeon using identical techniques and settings as those employed in our study.
In this study, we conducted a comparison between intraoperative USTs and CDEs. Our findings indicate that in Grade IV–V hard nuclear cataract surgery, the use of the burst mode combined with the torsional approach leads to a reduction in the mean UST and CDE compared to those of the continuous torsional mode. Conversely, for Grade III hard nuclear cataract surgeries, there was no significant difference in the mean CDE between the two groups. However, the burst mode with the combined torsional mode still resulted in a decrease in the mean UST when compared to the continuous torsional mode. Hence, it was determined that employing the burst mode in conjunction with the combined torsional mode yields a reduction in overall ultrasound energy consumption when compared to the continuous torsional ultrasound mode during nuclear cataract surgeries with higher levels of cataract hardness. The use of lower energy levels and shorter ultrasound durations in this approach may contribute to the mitigation of corneal endothelial cell damage.17,18 This finding aligns with previous studies that have established a correlation between the application of ultrasound energy and the loss of endothelial cells.6,7
In patients diagnosed with Grade III moderate nuclear cataracts, a notable disparity in the changes in the ECD was observed on the first day after surgery. Specifically, the group treated with continuous torsional ultrasound exhibited a greater loss of corneal endothelial cells. However, no statistically significant differences were found between the two groups in terms of corneal edema, CCT, or changes in these parameters or in endothelial cells or changes in these parameters during subsequent follow-up periods. In the subgroup of Grade IV–V hard nuclear cataracts, the continuous torsional ultrasound group exhibited a greater increase in CCT and more endothelial cell loss in the postoperative period than did the combined group at up to 3 months of follow-up. Additionally, the occurrence of corneal edema was comparatively more pronounced on the first day following surgery. This suggests that the statistical difference in the ECD changes is manifested in the postoperative corneal edema.
At the 1-week follow-up after surgery, the corneal edema had nearly resolved, and there was no notable difference between the two cohorts. Both groups demonstrated a substantial improvement in BCVA from the preoperative baseline on day 1 and day 7; nevertheless, no statistically significant difference was detected between the groups. The BCVA remained stable without significant alterations at the 1- and 3-month postoperative assessments.
During the phacoemulsification procedure for Grade IV–V hard nuclear cataracts, our observations revealed a greater occurrence of infusion system occlusion in the continuous torsional mode group than in the combined burst mode group. We hypothesized that the utilization of the burst mode combined with torsional ultrasound could enhance the efficiency of managing relatively harder nucleated cataracts. This approach may reduce the duration of unnecessary infusion and expedite the procedure, thereby minimizing endothelial cell loss resulting from other contributing factors.
The superior performance of combined burst mode in hard nuclear cataracts may be explained by two synergistic mechanisms: First, reduced nuclear chatter and improved purchase. Torsional ultrasound alone can struggle to engage dense nuclear fragments, causing repulsion (“chatter”) away from the tip.13 The addition of intermittent longitudinal bursts in combined mode helps “grab” and hold fragments, improving followability and reducing the need for repetitive passes—a critical advantage in hard cataracts where fragments are more rigid. Second, superior thermal management. Hard cataracts require longer ultrasound times, increasing the risk of thermal injury.14 The burst component delivers longitudinal energy intermittently, allowing tip cooling between pulses. This intermittent energy delivery reduces heat accumulation, potentially minimizing thermal damage to corneal endothelial cells. In contrast, continuous torsional mode, while cooler than continuous longitudinal ultrasound, still produces sustained energy delivery during prolonged emulsification. These mechanisms are consistent with previous biomechanical studies13,14,17 and warrant further investigation.
Currently, several new technologies, such as femtosecond-assisted phacoemulsification, can help reduce the energy used in phacoemulsification; these methods have been shown in several studies to be more effective than phacoemulsification alone in reducing energy use and achieving a better surgical prognosis.19,20 Additionally, newer devices such as miLoop have exhibited enhanced effectiveness in managing challenging cases of nuclear cataract surgery.21,22 However, all of these require additional equipment to perform the surgery. Our study showed that it is possible to provide more cost-effective and better prognostic surgery for patients with hard cataracts by setting individual surgical parameters based on existing devices.
This study is subject to certain limitations. First, The duration of the follow-up period, which spanned 3 months, was relatively brief, preventing the evaluation of long-term outcomes and complications. However, previous studies have shown that endothelial cell loss at 1–3 months post-surgery is strongly correlated with loss at 1 year and beyond,23,24 suggesting that our findings are likely predictive of longer-term outcomes. Nevertheless, future studies with extended follow-up (eg, 1–2 years) are warranted to confirm the durability of the benefits observed with combined burst mode phacoemulsification. Second, as a non-randomized cohort study, it is subject to potential selection bias, as group assignment was based on surgeon preference rather than random allocation. Although the surgeon was masked to patient enrollment and preoperative data to minimize bias, unmeasured confounders may still exist. However, baseline characteristics were well-balanced between groups (Table 2), suggesting that any bias may be limited. Future randomized controlled trials are warranted to confirm our findings. Third, all surgeries were performed by a single experienced surgeon (J.Y.H). While this eliminates inter-surgeon variability and enhances internal validity, it may limit the generalizability of our findings to other surgeons or clinical settings with different levels of experience or surgical techniques.
Conclusion
In summary, we found that combined burst-torsional mode phacoemulsification resulted in lower cumulative dissipated energy, shorter ultrasound time, and less corneal endothelial cell damage compared to continuous torsional mode. These benefits were most pronounced in patients with severe nuclear cataracts (Grade IV–V), including reduced postoperative corneal edema and endothelial cell loss at 3 months. In contrast, for moderate nuclear cataracts (Grade III), the advantages of combined mode were less pronounced, with only transient differences in early postoperative endothelial cell loss. These findings support a tailored approach to phacoemulsification mode selection based on nuclear density, with combined burst-torsional mode offering particular advantages for challenging hard cataracts.
Data Sharing Statement
On reasonable request, the data supporting these findings can be obtained from the corresponding author.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Fudan University’s Eye & ENT Hospital.
Acknowledgments
We thank all the patients who participated in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Grant No.82070942 from National Natural Science Foundation of China and Shanghai Leading Talent Program of Eastern Talent Plan (BJWS2024015).
Disclosure
None of the authors has any financial or proprietary interest in any material or method mentioned in this work.
References
1. Kotb AMEM, Elawamry AI. Feasibility of the new torsional phacoemulsification software phacoemulsification (Ozil IP) in hard cataracts. Asia Pac J Ophthalmol. 2013;2(6):372–10. doi:10.1097/APO.0b013e31828a56f7
2. Shah PA, Yoo S. Innovations in phacoemulsification technology. Curr Opin Ophthalmol. 2007;18(1):23–26. doi:10.1097/ICU.0b013e328011f9d0
3. Kim EC, Byun YS, Kim MS. Microincision versus small-incision coaxial cataract surgery using different power modes for hard nuclear cataract. J Cataract Refract Surg. 2011;37(10):1799–1805. doi:10.1016/j.jcrs.2011.04.024
4. O’Brien PD, Fitzpatrick P, Kilmartin DJ, Beatty S. Risk factors for endothelial cell loss after phacoemulsification surgery by a junior resident. J Cataract Refract Surg. 2004;30(4):839–843. doi:10.1016/S0886-3350(03)00648-5
5. Zeng M, Liu X, Liu Y, et al. Torsional ultrasound modality for hard nucleus phacoemulsification cataract extraction. Br J Ophthalmol. 2008;92(8):1092–1096. doi:10.1136/bjo.2007.128504
6. Yang W-J, Wang X-H, Zhao F, Mei Z-M, Li S, Xiang Y. Torsional and burst mode phacoemulsification for patients with hard nuclear cataract: a randomized control study. Medicine. 2019;98e15870. doi:10.1097/MD.0000000000015870
7. Liu Y, Zeng M, Liu X, et al. Torsional mode versus conventional ultrasound mode phacoemulsification: randomized comparative clinical study. J Cataract Refract Surg. 2007;33(2):287–292. doi:10.1016/j.jcrs.2006.10.044
8. Kim D-H, Wee W-R, Lee J-H, Kim M-K. The comparison between torsional and conventional mode phacoemulsification in moderate and hard cataracts. Korean J Ophthalmol. 2010;24(6):336–340. doi:10.3341/kjo.2010.24.6.336
9. Vasavada AR, Raj SM, Lee YC. NeoSoniX ultrasound versus ultrasound alone for phacoemulsification: randomized clinical trial. J Cataract Refract Surg. 2004;30(11):2332–2335. doi:10.1016/j.jcrs.2004.02.077
10. Phacoemulsification and aspiration of cataracts: surgical techniques, complications, and results | semantic scholar. Available from: https://www.semanticscholar.org/paper/Phacoemulsification-and-aspiration-of-cataracts%3A-Emery-Little/7e0c05a9a75e4b44aa048aac3f90dfe6a9dbe986.
11. Xie L, Yao Z, Huang Y, Ying L. Corneal endothelial damage and its repair after phacoemulsification. Zhonghua Yan Ke Za Zhi. 2004;40(2):90–93.
12. Gupta PK, Berdahl JP, Chan CC, et al. The corneal endothelium: clinical review of endothelial cell health and function. J Cataract Refract Surg. 2021;47(9):1218–1226. doi:10.1097/j.jcrs.0000000000000650
13. Zacharias J, Ohl C-D. Fluid dynamics, cavitation, and tip-to-tissue interaction of longitudinal and torsional ultrasound modes during phacoemulsification. J Cataract Refract Surg. 2013;39(4):611–616. doi:10.1016/j.jcrs.2012.10.050
14. Han YK, Miller KM. Heat production: longitudinal versus torsional phacoemulsification. J Cataract Refract Surg. 2009;35(10):1799–1805. doi:10.1016/j.jcrs.2009.04.046
15. Bu JJ, Chung J, Afshari NA. Efficient use of ultrasound in cataract surgery. Curr Opin Ophthalmol. 2022;33(1):41–46. doi:10.1097/ICU.0000000000000821
16. Badoza D, Fernández Mendy J, Ganly M. Phacoemulsification using the burst mode. J Cataract Refract Surg. 2003;29(6):1101–1105. doi:10.1016/s0886-3350(03)00074-9
17. Reuschel A, Bogatsch H, Barth T, Wiedemann R. Comparison of endothelial changes and power settings between torsional and longitudinal phacoemulsification. J Cataract Refract Surg. 2010;36(11):1855–1861. doi:10.1016/j.jcrs.2010.06.060
18. Chen X, Ji Y, Lu Y. Comparison of clear corneal incision injuries between torsional and conventional phacoemulsification. Graefes Arch Clin Exp Ophthalmol. 2013;251(9):2147–2154. doi:10.1007/s00417-013-2423-3
19. Wang EF, Worsley A, Polkinghorne PJ. Comparative study of femtosecond laser-assisted cataract surgery and conventional phacoemulsification in vitrectomized eyes. Clin Exp Ophthalmol. 2018;46(6):624–629. doi:10.1111/ceo.13133
20. Liu Y-C, Setiawan M, Chin JY, et al. Randomized controlled trial comparing 1-year outcomes of low-energy femtosecond laser-assisted cataract surgery versus conventional phacoemulsification. Front Med. 2021;8:811093. doi:10.3389/fmed.2021.811093
21. Ianchulev T, Chang DF, Koo E, et al. Microinterventional endocapsular nucleus disassembly: novel technique and results of first-in-human randomised controlled study. Br J Ophthalmol. 2019;103(2):176–180. doi:10.1136/bjophthalmol-2017-311766
22. Wiley WF, Bafna S, Logothetis HD. Comparative study of phacoemulsification parameters with and without nitinol filament nuclear disassembly. J Cataract Refract Surg. 2021;47(8):1028–1031. doi:10.1097/j.jcrs.0000000000000575
23. Bourne RRA, Minassian DC, Dart JKG, Rosen P, Kaushal S, Wingate N. Effect of cataract surgery on the corneal endothelium: modern phacoemulsification compared with extracapsular cataract surgery. Ophthalmology. 2004;111(4):679–685. doi:10.1016/j.ophtha.2003.07.015
24. Walkow T, Anders N, Klebe S. Endothelial cell loss after phacoemulsification: relation to preoperative and intraoperative parameters. J Cataract Refract Surg. 2000;26(5):727–732. doi:10.1016/s0886-3350(99)00462-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.