Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Combination Therapy Against Mood and Anxiety Disorders: Association Between Efficacy and White Blood Cell Count
Authors Qiao MX, Yu H, Fu Z, Wei W, Li XJ, Deng W ![]() , Guo WJ, Li T
, Guo WJ, Li T
Received 21 January 2025
Accepted for publication 23 July 2025
Published 13 August 2025 Volume 2025:21 Pages 1655—1668
DOI https://doi.org/10.2147/NDT.S516881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Meng-Xuan Qiao,1,2 Hua Yu,1,3– 5 Zheng Fu,1,2 Wei Wei,1,3– 5 Xiao-Jing Li,1,3– 5 Wei Deng,1,3– 5 Wan-Jun Guo,1,3– 5 Tao Li1– 5
1Affiliated Mental Health Center and Hangzhou Seventh People’s Hospital and School of Brain Science and Brain Medicine, Zhejiang University School of Medicine, Hangzhou, 310058, People’s Republic of China; 2School of Mental Health, Wenzhou Medical University, Wenzhou, 325035, People’s Republic of China; 3Zhejiang Key Laboratory of Clinical and Basic Research on Mental Disorders, Hangzhou, People’s Republic of China; 4Zhejiang Engineering Research Center for Intelligent Diagnosis and Treatment of Mental Disorders, Hangzhou, People’s Republic of China; 5Liangzhu Laboratory, MOE Frontier Science Center for Brain Science and Brain-Machine Integration, State Key Laboratory of Brain-Machine Intelligence, Zhejiang University, Hangzhou, 311121, People’s Republic of China
Correspondence: Tao Li, Affiliated Mental Health Center and Hangzhou Seventh People’s Hospital and School of Brain Science and Brain Medicine, Zhejiang University School of Medicine, Hangzhou, 310058, People’s Republic of China, Email [email protected] Hua Yu, Affiliated Mental Health Center and Hangzhou Seventh People’s Hospital and School of Brain Science and Brain Medicine, Zhejiang University School of Medicine, Hangzhou, 310058, People’s Republic of China, Email [email protected]
Background: Numerous studies suggest that hyperactivation of the immuno-inflammatory system, as reflected in cytokine levels, is associated with more severe symptoms in mood and anxiety disorders and weaker response to treatment. Here we examined whether the efficacy of a combination of bright light therapy, repetitive transcranial magnetic stimulation and medication is associated with another immuno-inflammatory index, white blood cell count, before and/or after treatment, in a retrospective observational study.
Methods: We retrospectively analyzed 467 inpatients with major depressive, bipolar, or generalized anxiety disorder who were treated with combination therapy for at least one week at Hangzhou Seventh People’s Hospital between April 2022 and April 2024. Potential associations between remission incidences within four weeks after treatment and white blood cell count both before treatment and post-treatment were explored. We used mixed-effects linear modeling to examine the association between treatment characteristics and changes in white blood cell count and depressive symptoms.
Results: Bipolar and major depressive disorders were associated with significantly higher white blood cell counts at baseline than generalized anxiety disorder as well as with significantly lower remission incidences. Bright light therapy’s effects depended on baseline inflammation, more sessions led to greater reductions in the Hamilton Depression Rating Scale score with low baseline white blood cell count, and greater decreases in white blood cell count with high baseline count. In contrast, repetitive transcranial magnetic stimulation sessions showed no association with white blood cell count.
Conclusion: These results highlight the need to account for an individual’s immuno-inflammatory state when personalizing treatment for mental health disorders.
Keywords: depressive symptoms, white blood cell count, bright light therapy, inflammation
Introduction
Mood disorders are major public health challenges around the world, with prevalence as high as 12.9% for major depressive disorder, 3.7% for generalized anxiety disorder, and 2% for bipolar disorder.1,2 These disorders contribute to chronic disability and reduce quality of life.3–5 Both major depressive and bipolar disorders involve depressive symptoms such as persistently low mood, chronic fatigue, irritability, difficulty in concentrating, and sleep disturbance.6 Such symptoms also occur in many individuals with generalized anxiety disorder.7,8
Mood and anxiety disorders appear to involve disturbances in the immuno-inflammatory system,9–11 typically detected as elevated levels of cytokines such as interleukin-6 and C-reactive protein.12–14 Greater elevation of these cytokines has been associated with more severe fatigue, sleep disturbance as well as loss of appetite and energy in individuals with different mood and anxiety disorders.15–18 It has also been associated with worse response to pharmacological and other types of treatment.19,20 This extensive literature argues for assessing the extent of dysregulation of the immuno-inflammatory system in individuals with mood or anxiety disorders in order to personalize treatment, and for researching the contribution of the immuno-inflammatory system to these disorders in large populations.
Such large-scale clinical screening and research would be much easier if it relied on analyses of immuno-inflammatory indices that are routinely performed on admission, rather than on specific cytokine assays. White blood cell count, which takes into account the numbers of lymphocytes, monocytes, neutrophils, eosinophils and basophils, provides a routine, cost-effective index of inflammation.21 Higher or lower white blood cell count are directly proportional to severity of depressive symptoms in both the general population and individuals with mood disorders.22,23 Elevated white blood cell count suggests a heightened inflammatory response, while lower count may indicate impaired immune cell production.24 Among postmenopausal women in the general population, higher white blood cell count has been associated with greater risk of having depressive symptoms and of using anti-depressants.25 Still unclear is whether baseline white blood cell count, analogously to baseline cytokine levels, correlates with the ability of combination treatment to mitigate the severity of depressive symptoms and/or the inflammatory state of individuals with mood and anxiety disorders.
We explored these questions by retrospectively examining data for patients at our hospital who were diagnosed with major depressive, bipolar or generalized anxiety disorder and who were treated with combination therapy involving drugs—in turn a combination of selective serotonin reuptake inhibitors with mood stabilizers or low-dose antipsychotics26—as well as the non-invasive neurostimulation techniques of bright light therapy and repetitive transcranial magnetic stimulation.27–29 All these approaches have been shown to mitigate neuroinflammation,30,31 but whether this can be detected through normalization of the white blood cell count is unclear. Therefore, this study aimed to investigate whether baseline white blood cell count is associated with remission incidences following combination treatment, and whether treatment-related changes in white blood cell count may differ across inflammatory states.
Methods
Participants
We retrospectively examined a consecutive series of inpatients diagnosed with major depressive, bipolar or generalized anxiety disorder at Hangzhou Seventh People’s Hospital between April 2022 and April 2024. This study was approved by the Ethics Committee of Hangzhou Seventh People’s Hospital and was conducted in accordance with the Declaration of Helsinki (2013).
Individuals were considered eligible for inclusion if (1) they were diagnosed with major depressive disorder (first-episode or recurrent), bipolar disorder (depressive or mixed episodes) or generalized anxiety disorder according to the 10th revision of the International Classification of Diseases; (2) they received a combination of medication, bright light therapy and repetitive transcranial magnetic stimulation for at least one week; and (3) their white blood cell counts before treatment and after treatment were available.
Individuals were excluded from the study if (1) they had acute illness or severe chronic disorder that might affect white blood cell count, such as infection, autoimmune disease, heart failure, or cancer; (2) they were younger than 15 years or older than 65 years; or (3) their white blood cell count before treatment deviated more than three standard deviations from the mean.
Assessments
Clinicodemographic data on all participants and the therapies they received were retrieved from our hospital’s electronic medical records. We also collected information on the treatments administered, including types and doses of medications as well as numbers of sessions of bright light therapy and repetitive transcranial magnetic stimulation. Scores on the Hamilton Depression Rating Scale before treatment and after treatment within four weeks during hospital were determined through interviews conducted by psychiatrists. The percent change in score was calculated as follows:
Percent change = [(score at baseline - score after treatment) / score at baseline] × 100.
White blood cells count was determined within our hospital’s clinical laboratory, and the percent change between baseline and after treatment was calculated as above.
Treatment Protocol
In terms of medication management, we follow clinical guidelines and prioritize the use of mood stabilizers and antipsychotics for bipolar depressive episodes, supplemented with antidepressants when necessary. For major depressive disorder or generalized anxiety disorder, selective serotonin reuptake inhibitors are the first-line treatment. Patients presenting with anxiety symptoms may receive additional anxiolytic agents. For all patients, benzodiazepines may be prescribed during hospitalization as clinically appropriate, based on their clinical status and symptom severity. To quantify medication exposure, we calculated the total defined daily dose (DDD) for each major drug category, including antipsychotics, antidepressants, mood stabilizers, anxiolytics, and benzodiazepines. In efforts to accelerate symptom relief, some hospitalized patients received combined drug therapy with repetitive transcranial magnetic stimulation and bright light therapy. As described previously, all patients included in our study received both pharmacotherapy and non-invasive neurostimulation therapy. Bright light therapy was administered to all patients using a commercially available white light box that delivered 7000 lux of illumination for 30 minutes each morning. For repetitive transcranial magnetic stimulation, stimulation protocols differed by diagnosis. Patients with major depressive disorder or bipolar depression underwent high-frequency (10 Hz) excitatory stimulation targeting the left dorsolateral prefrontal cortex, delivered at 40% of the motor threshold (with the threshold set at 55) in 4-second trains with 15-second inter-train intervals, totaling 2400 pulses over 19 minutes per session. In contrast, patients with generalized anxiety disorder received low-frequency (1 Hz) inhibitory stimulation over the right dorsolateral prefrontal cortex, administered at 120% of the motor threshold in 20-second trains without inter-train intervals, totaling 1200 pulses over 20 minutes per session.
Statistical Analysis
Data were analyzed statistically using R 4.3.1 (www.r-project.org), and the normality of data distributions was assessed using the Kolmogorov–Smirnov test. Differences between groups with different types of mental disorder were assessed for significance using a chi-squared test in the case of sex, or using a two-samples t test in the case of age, white blood cell counts, Hamilton Depression Rating Scale scores, and other treatment-related variables. Participants were categorized into quartiles based on white blood cell count at baseline, and potential associations between quartile and sex were explored using the Cochrane-Armitage trend test. Within each quartile, trends in age, use of a specific medication or score on the Hamilton Depression Rating Scale were explored using the chi-squared test.
Percent changes in white blood cell count were compared across quartiles within each type of mental disorder using repeated-measures ANOVA. Remission incidences were compared between the same quartiles for different types of mental disorder using the chi-squared test. These analyses included post hoc correction based on the false discovery rate.
Potential associations of treatment-related factors on percent changes in white blood cell count and scores on the Hamilton Depression Rating Scale were explored using a mixed-effects linear model that controlled for age and sex, while treating the type of mental disorder as a random effect.
Results
Of the 707 inpatients screened for enrollment, we excluded 124 who were diagnosed with schizophrenia, sleep disorders, or obsessive-compulsive disorder; 73 who fell outside the eligible age range; and 43 whose white blood cell count at baseline was more than three standard deviations from the mean (Figure 1). The remaining 467 patients were included in the final analysis, comprising 225 individuals with major depressive disorder, 132 with generalized anxiety disorder, and 110 with bipolar disorder. Scores on the Hamilton Depression Rating Scale before and after treatment were available for 131 individuals with major depressive disorder, 77 with generalized anxiety disorder, and 57 with bipolar disorder.
 |
Figure 1 Flow chart of study selection process. |
Across the three types of mental disorder, the individuals did not differ significantly in sex, numbers of sessions of bright light therapy or repetitive transcranial magnetic stimulation, or use of anxiolytic medications (Table 1). Frequencies of use of mood stabilizers and antipsychotic medications were significantly higher among those with bipolar disorder than in the other two groups. Frequency of use of antidepressants was significantly higher among those with major depressive disorder, while frequency of use of benzodiazepines was significantly higher among those with generalized anxiety disorder.
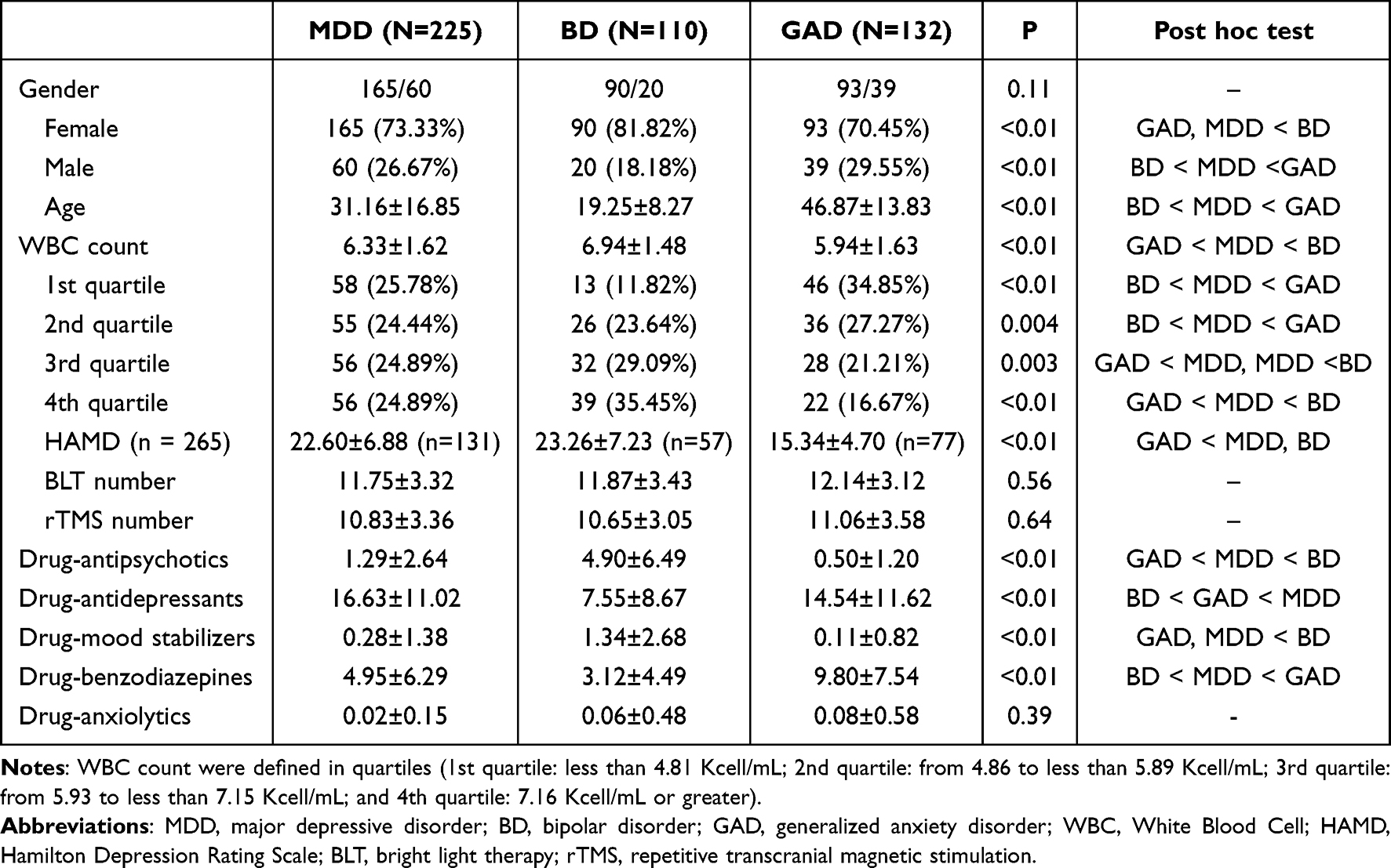 |
Table 1 Demographic and Clinical Characteristics Among Different Diseases Status |
White blood cell counts at baseline were highest among individuals with bipolar disorder and lowest among those with generalized anxiety disorder. When all participants were categorized into quartiles based on baseline count, those with bipolar disorder were more likely to be in the highest quartile, while those with generalized anxiety disorder were more likely to be in the lowest.
Across all participants in the study, regardless of type of mental disorder, white blood cell count at baseline correlated inversely with age and use of benzodiazepine during treatment, whereas it correlated positively with use of antipsychotics and anxiolytic medications (Table 2). It did not correlate significantly with use of anti-depressants or mood stabilizers. Age, use of benzodiazepine and anxiolytics and baseline scores on the Hamilton Depression Rating Scale varied significantly with quartile.
 |
Table 2 Relationship Between White Blood Cell Count and Sociodemographic, Antidepressant Use During Treatment, and Depressive Symptoms |
Association Between Treatment and WBC Change
Upon analyzing the combined data from all three patient groups, we observed distinct patterns based on initial white blood cell count. Specifically, patients with the lowest baseline white blood cell count (first quartile) experienced an increase in white blood cell count following treatment, while those with the highest initial white blood cell count (fourth quartile) experienced a decrease. This trend was consistent across the different diagnostic groups (Figure 2 and Supplemental Table 1). In the major depressive disorder group, white blood cell count increased after treatment in the first and second quartiles but decreased in the third and fourth quartiles. Similarly, in the bipolar disorder group, white blood cell count increased in the first and second quartile, but decreased in the fourth quartile, whereas in the generalized anxiety disorder group, white blood cell count decreased in the second and fourth quartiles.
 |
Figure 2 Retrospective Changes in white blood cell count after treatment across different quartiles and disease groups. Abbreviations: WBC, White Blood Cell; MDD, major depressive disorder; BD, bipolar disorder; GAD, generalized anxiety disorder. Notes: White blood cell count was defined in quartiles (1st quartile: less than 4.81 Kcell/mL; 2nd quartile: from 4.86 to less than 5.89 Kcell/mL; 3rd quartile: from 5.93 to less than 7.15 Kcell/mL; and 4th quartile: 7.16 Kcell/mL or greater); p=significant at *<0.05, **<0.01, ***<0.001. |
Associations Between White Blood Cell Count at Baseline and Remission Incidence After Treatment
When participants were compared in terms of type of mental disorder, remission incidence was significantly higher among those with generalized anxiety disorder than among those with major depressive or bipolar disorder (Figure 3 and Supplemental Table 2). When participants were compared in terms of quartile of white blood cell count at baseline, remission incidence among those in the second quartile was higher for generalized anxiety disorder than for major depressive disorder, and remission incidence in the highest quartile was higher for generalized anxiety disorder than for bipolar disorder and major depressive disorder.
 |
Figure 3 Association between Baseline WBC Count and Remission Incidence in Different Diseases. Abbreviations: WBC, White Blood Cell; MDD, major depressive disorder; BD, bipolar disorder; GAD, generalized anxiety disorder. Notes: White blood cell count was defined in quartiles (1st quartile: less than 4.81 Kcell/mL; 2nd quartile: from 4.86 to less than 5.89 Kcell/mL; 3rd quartile: from 5.93 to less than 7.15 Kcell/mL; and 4th quartile: 7.16 Kcell/mL or greater); P=significant at *<0.05, **<0.01, ***<0.001. |
Associations of Treatment Factors with Percent Change in White Blood Cell Count
Across all participants, mixed-effects linear modeling linked the use of anxiolytics to a decrease in white blood cell count (β = 0.07, 95% CI 0.02 to 0.12) and use of mood stabilizers to an increase in white blood cell count (β = −0.02, 95% CI −0.03 to 0.00) (Table 3). In contrast, variations in the other treatment modalities—whether anti-depressants, anti-psychotics or numbers of sessions of bright light therapy or transcranial magnetic stimulation—were not associated with significant changes in white blood cell count.
 |
Table 3 Mixed-Effects Linear Models Assessing the Association of Treatment Factors with White Blood Cell Count |
When participants were stratified by quartile of white blood cell count at baseline, use of anti-psychotics by those in the third quartile was associated with a decrease in white blood cell count (β = 0.01, 95% CI 0.00 to 0.02), as was use of benzodiazepines (β = 0.01, 95% CI 0.00 to 0.01). Among those in the highest quartile, in contrast, anti-depressants were minimally associated with change in white blood cell count (β = 0.00, 95% CI −0.01 to 0.00); mood stabilizers, for their part, were linked to a decrease in white blood cell count (β = −0.02, 95% CI −0.04 to 0.00) in this quartile, suggesting an immunosuppressive effect. Conversely, the number of bright light sessions was positively associated with changes in white blood cell counts (β = 0.03, 95% CI 0.01 to 0.05), implying immunostimulation. The number of sessions of repetitive transcranial magnetic stimulation, in contrast, was not significantly associated with changes in white blood cell count.
Associations of Treatment Factors with Percent Change in Scores on the Hamilton Depression Rating Scale
Across all participants, mixed-effects linear modeling linked the use of anti-psychotics to a slight increase (β = −0.01, 95% CI −0.01 to 0.00), and the use of anxiolytics to a larger increase (β = −0.05, 95% CI −0.09 to 0.00), in severity of depressive symptoms based on the change in score on the Hamilton Depression Rating Scale (Table 4). Thus, these two classes of drug may worsen depressive symptoms. Conversely, a larger number sessions of bright light therapy was associated with greater mitigation of depressive symptoms (β = 0.02, 95% CI 0.01 to 0.02). However, use of other psychiatric medications and the number of sessions of transcranial magnetic stimulation were not significantly associated with changes in symptom severity.
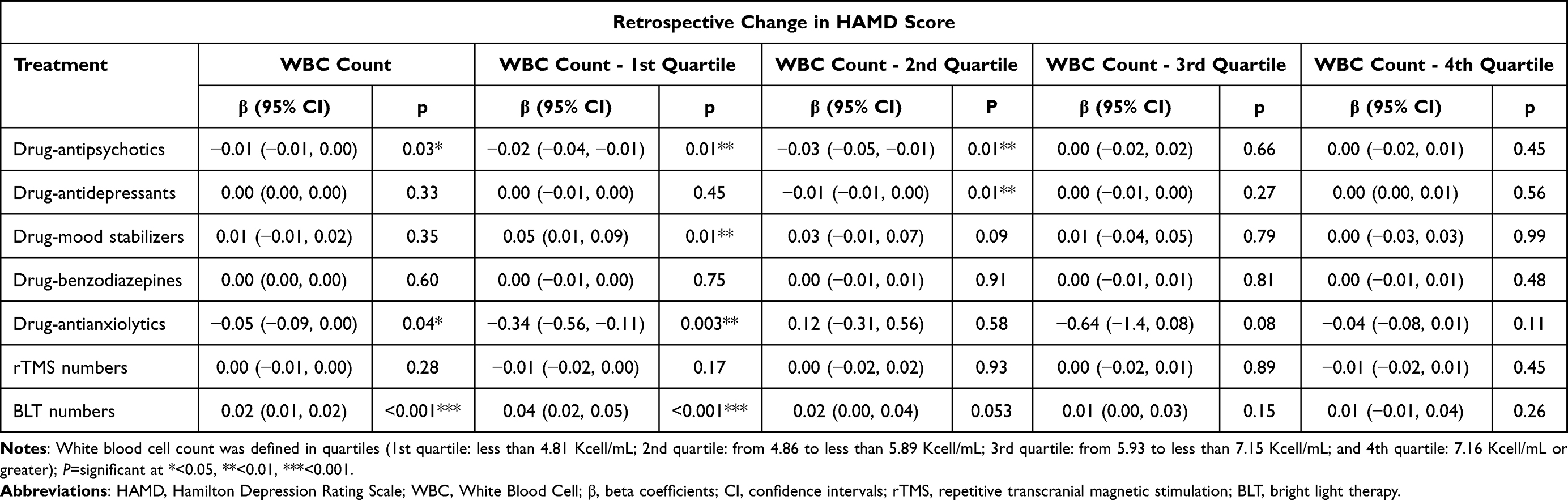 |
Table 4 Mixed-Effects Linear Models Assessing the Association of Treatment Factors with HAMD Scores |
When participants were stratified by quartile of white blood cell count at baseline, use of anti-psychotics by those in the lowest quartile was associated with slight worsening of depressive symptoms (β = −0.02, 95% CI −0.04 to −0.01), while use of anxiolytics was associated with more pronounced worsening (β = −0.34, 95% CI −0.56 to −0.11). Conversely, use of mood stabilizers (β = 0.05, 95% CI 0.01 to 0.09) and larger number of sessions of bright light therapy (β = 0.04, 95% CI 0.02 to 0.05) were associated with improvement of symptoms.
Use of anti-psychotics by those in the second quartile was associated with slight worsening of depressive symptoms (β = −0.03, 95% CI −0.05 to −0.01), while use of anti-depressants was associated with marginal worsening (β = −0.01, 95% CI −0.01 to 0.00).
Discussion
In this study, the ability of different combination treatments to induce remission or mitigate the severity of depressive symptoms in individuals with major depressive, bipolar or generalized anxiety disorder was found to depend on their white blood cell count at baseline. Our data highlight the need to take into account an individual’s immuno-inflammatory state in order to personalize treatment, and they suggest that white blood cell count may be a useful routine index for this purpose.
Regardless of their type of mental disorder, individuals in our study with a lower level of inflammation at baseline tended to experience an increase in white blood cell count after combination treatment, implying recovery or activation of immune responses. Conversely, individuals with a higher level of inflammation at baseline generally experienced a decrease in white blood cell count, which could indicate dampening of inflammatory and immune responses. Whatever the underlying processes, the combination treatment in our study generally tended towards normalizing white blood cell counts, reflecting the importance of maintaining a balanced immune system for optimal psychiatric outcomes.32,33
Our study raises the possibility of white blood cell count at baseline as a predictor of the efficacy of combination treatment. Compared to the higher inflammatory states observed in patients with bipolar disorder and major depressive disorders, those with generalized anxiety who had low baseline white blood cell counts exhibited higher remission incidences. Among our study participants in the highest quartile of white blood cell count at baseline, remission incidence after treatment was significantly higher for generalized anxiety and major depressive disorders than for bipolar disorder, which may be due to those individuals with bipolar disorder showed the highest white blood cell counts at baseline. These findings are consistent with previous work linking higher levels of inflammatory markers to weaker response to anti-depressants in individuals with major depressive disorder perhaps because neuroinflammation reduces the availability of serotonin.19,20,34 Future research should explore the usefulness of baseline white blood cell count for personalizing treatment of mood and anxiety disorders.
Our study analyzed inpatients who were treated according to routine practice in our specialized mental health unit, which aims to apply the latest advances in therapies combining pharmacological and other modalities in order to optimize prognosis. While this approach makes our analysis immediately relevant to the “real world” of the clinic, it also means that we cannot separately examine the effects of the drug and non-drug components on remission incidence or severity of depression symptoms in our sample. Future work should clarify whether and how combination treatments involving drugs, bright light therapy and repetitive transcranial magnetic stimulation improve prognosis by dampening inflammation, as has been suggested for anxiolytics, benzodiazepines, anti-psychotics and anti-depressants,35,36 as well as for bright light therapy and repetitive transcranial magnetic stimulation.37,38 Such work should be suitably designed to detect potentially complex mechanisms.
In our analysis, the use of anxiolytic medications was associated with a reduction in white blood cell count (β = 0.07, 95% CI 0.12 to 0.02). Although the effect size was relatively small, the confidence interval was narrow and excluded zero, suggesting a statistically significant and stable association. This finding may reflect the potential anti-inflammatory effects of anxiolytic agents, possibly mediated through the activation of dopamine D3 receptors and serotonin 1A receptors, both of which have been implicated in modulating immune responses and neuroinflammatory signaling.39 The mood stabilizer lithium, for example, has been shown to increase inflammatory signaling in one study40 but to dampen it in other studies,41,42 reflecting its complex and potentially bidirectional effects on immune function. In our analysis, the use of mood stabilizers was associated with a slight increase in white blood cell count (β = −0.02, 95% CI −0.03 to 0.00). Although the effect size was modest, the confidence interval approached statistical significance, suggesting a possible immunosuppressive effect. It may be that the different components of combination therapy exert therapeutic effects by simultaneously promoting pro- and anti-inflammatory processes. A greater number of sessions of bright light therapy in our sample was associated with greater reduction in white blood cell count (β = 0.03, 95% CI 0.05 to 0.01), consistent with the idea that the therapy dampens inflammation.43,44 Although the effect size was modest, the confidence interval was narrow and excluded zero, indicating a statistically significant and robust association. This lends further support to the hypothesis that bright light therapy may exert its therapeutic effects, at least in part, by dampening peripheral inflammation. In contrast, no significant association was observed between the number of transcranial magnetic stimulation sessions and white blood cell count. Transcranial stimulation may exert anti-depressant effects not by altering peripheral inflammation, of which white blood cell count serves as a marker, but by altering neural activity45 and neuroinflammation, of which interleukin-6 and tumor necrosis factor-α serve as markers.46 Future studies should explore this possibility.
Future work should also examine carefully whether bright light therapy and repetitive transcranial magnetic stimulation can synergize with drugs to dampen inflammation46–48 and thereby mitigate depressive symptoms by targeting, simultaneously, the neurobiological pathways involved in mood regulation as well as the inflammatory processes associated with mood and anxiety disorders.30 Exploring therapeutic mechanisms in preclinical models should be performed with caution, given that treatments that mitigate inflammation and behavioral deficits in animal models of depression do not always perform similarly in patients.49
In fact, the present study already suggests one context in which white blood cell count at baseline may be useful for optimizing treatment. The number of sessions of bright light therapy was positively associated with improvement of depressive symptoms after combination treatment among individuals in the lowest quartile of white blood cell count at baseline, but not among individuals in the highest quartile, even though it was positively associated with the percent decrease in white blood cells in those quartiles. These results suggest that individuals with elevated inflammation may require initial treatments that reduce systemic inflammation before bright light therapy can be effective as an anti-depressant.50–52
Our findings should be interpreted in caution in light of the fact that we were unable to minimize confounding by smoking status, body mass index, illness duration or age at illness onset, the data for which were missing for many participants. Smoking, body mass index and illness duration are known to influence immune function and inflammation.53 In addition, we did not include a control group of individuals without mood or anxiety disorders whose white blood cell counts could provide a reference for determining whether the counts in our patients were truly associated with their mental condition. Another limitation relates to the assessment of anxiety symptoms. As Hamilton Depression Rating Scale was retained as the primary outcome measure in the main analysis to ensure consistency across diagnostic groups. This approach may have reduced the sensitivity to anxiety-specific changes. Finally, although the diagnosis variable was modeled as a random intercept in the mixed-effects linear model to account for group-level heterogeneity, disease-specific analyses were not performed due to limited sample sizes. Future studies with larger and more balanced samples may allow for stratified analyses by diagnostic category to further validate these findings.
Despite these limitations, our study underscores the critical role of inflammation in mental health disorders and the need to take into account the baseline level of inflammation in order to personalize treatment and optimize outcomes. The initial level of inflammation may influence the efficacy of combination treatment, especially regimes involving anxiolytics, mood stabilizers, and bright light therapy. It may be necessary, for example, to reduce systemic inflammation before initiating bright light therapy. Our results suggest that a “one-size-fits-all” approach may not be the most effective for treating mood and anxiety disorders. Future work should verify and extend our findings using larger, more heterogeneous samples, different combination therapies and longitudinal assessments that include additional inflammatory markers such as C-reactive protein, interleukin-6 and tumor necrosis factor-α.
Ethics Approval and Consent to Participate
This study protocol was approved by the Ethics Committee of Hangzhou Seventh People’s Hospital and was conducted in accordance with the Declaration of Helsinki (2013). As this was a retrospective study using anonymized clinical data, informed consent was not required.
Acknowledgments
The authors are grateful for valuable contributions from their coworkers at the Affiliated Mental Health Centre, Hangzhou Seventh People’s Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China Key Projects (82230046 to T.L.), National Natural Science Foundation of China (82101598 to H.Y.), Hangzhou Special Project for Biomedical and Health Industry (2022WJC122 to H.Y.) and 2021 Project for Hangzhou Medical Disciplines of Excellence (to T.L.).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ruscio AM, Hallion LS, Lim CCW, et al. Cross-sectional comparison of the epidemiology of DSM-5 generalized anxiety disorder across the globe. JAMA Psychiatry. 2017;74(5):465–475. doi:10.1001/jamapsychiatry.2017.0056
2. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/s0140-6736(20)30925-9
3. Havinga PJ, Maciejewski DF, Hartman CA, Hillegers MHJ, Schoevers RA, Penninx B. Prevention programmes for children of parents with a mood/anxiety disorder: systematic review of existing programmes and meta-analysis of their efficacy. Br J Clin Psychol. 2021;60(2):212–251. doi:10.1111/bjc.12277
4. Kayhan F, Cıcek E, Uguz F, Karababa IF, Kucur R. Mood and anxiety disorders among inpatients of a university hospital in Turkey. Gen Hosp Psychiatry. 2013;35(4):417–422. doi:10.1016/j.genhosppsych.2013.03.004
5. Yoon S, Kim YK. Possible oxytocin-related biomarkers in anxiety and mood disorders. Prog Neuropsychopharmacol Biol Psychiatr. 2022;116:110531. doi:10.1016/j.pnpbp.2022.110531
6. Marr NS, Zainal NH, Newman MG. Focus on and venting of negative emotion mediates the 18-year bi-directional relations between major depressive disorder and generalized anxiety disorder diagnoses. J Affect Disord. 2022;303:10–17. doi:10.1016/j.jad.2022.01.079
7. Wang X, Lin J, Liu Q, et al. Major depressive disorder comorbid with general anxiety disorder: associations among neuroticism, adult stress, and the inflammatory index. J Psychiatr Res. 2022;148:307–314. doi:10.1016/j.jpsychires.2022.02.013
8. Grande I, Berk M, Birmaher B, Vieta E. Bipolar disorder. Lancet. 2016;387(10027):1561–1572. doi:10.1016/s0140-6736(15)00241-x
9. Michopoulos V, Powers A, Gillespie CF, Ressler KJ, Jovanovic T. Inflammation in Fear- and Anxiety-Based Disorders: PTSD, GAD, and Beyond. Neuropsychopharmacology. 2017;42(1):254–270. doi:10.1038/npp.2016.146
10. Bai YM, Su TP, Tsai SJ, et al. Comparison of inflammatory cytokine levels among type I/type II and manic/hypomanic/euthymic/depressive states of bipolar disorder. J Affect Disord. 2014;166:187–192. doi:10.1016/j.jad.2014.05.009
11. Dooley LN, Kuhlman KR, Robles TF, Eisenberger NI, Craske MG, Bower JE. The role of inflammation in core features of depression: insights from paradigms using exogenously-induced inflammation. Neurosci Biobehav Rev. 2018;94:219–237. doi:10.1016/j.neubiorev.2018.09.006
12. Lynall ME, Turner L, Bhatti J, et al. Peripheral Blood Cell-Stratified Subgroups of Inflamed Depression. Biol Psychiatry. 2020;88(2):185–196. doi:10.1016/j.biopsych.2019.11.017
13. Kelly KM, Smith JA, Mezuk B. Depression and interleukin-6 signaling: a Mendelian Randomization study. Brain Behav Immun. 2021;95:106–114. doi:10.1016/j.bbi.2021.02.019
14. Valkanova V, Ebmeier KP, Allan CL. IL-6 and depression: a systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2013;150(3):736–744. doi:10.1016/j.jad.2013.06.004
15. Frank P, Jokela M, Batty GD, Cadar D, Steptoe A, Kivimäki M. Association between systemic inflammation and individual symptoms of depression: a pooled analysis of 15 population-based cohort studies. Am J Psychiatry. 2021;178(12):1107–1118. doi:10.1176/appi.ajp.2021.20121776
16. Lotrich FE, Butters MA, Aizenstein H, Marron MM, Reynolds CF, Gildengers AG. The relationship between interleukin-1 receptor antagonist and cognitive function in older adults with bipolar disorder. Int J Geriatr Psychiatry. 2014;29(6):635–644. doi:10.1002/gps.4048
17. Kuring JK, Mathias JL, Ward L, Tachas G. Inflammatory markers in persons with clinically-significant depression, anxiety or PTSD: a systematic review and meta-analysis. J Psychiatr Res. 2023;168:279–292. doi:10.1016/j.jpsychires.2023.10.009
18. Sealock JM, Lee YH, Moscati A, et al. Use of the PsycheMERGE network to investigate the association between depression polygenic scores and white blood cell count. JAMA Psychiatry. 2021;78(12):1365–1374. doi:10.1001/jamapsychiatry.2021.2959
19. Kruse JL, Olmstead R, Hellemann G, et al. Inflammation and depression treatment response to electroconvulsive therapy: sex-specific role of interleukin-8. Brain Behav Immun. 2020;89:59–66. doi:10.1016/j.bbi.2020.05.069
20. Lanquillon S, Krieg JC, Bening-Abu-Shach U, Vedder H. Cytokine production and treatment response in major depressive disorder. Neuropsychopharmacology. 2000;22(4):370–379. doi:10.1016/s0893-133x(99)00134-7
21. Zhang Y, Tao S, Coid J, et al. The role of total white blood cell count in antipsychotic treatment for patients with schizophrenia. Curr Neuropharmacol. 2024;22(1):159–167. doi:10.2174/1570159x21666230104090046
22. Shafiee M, Tayefi M, Hassanian SM, et al. Depression and anxiety symptoms are associated with white blood cell count and red cell distribution width: a sex-stratified analysis in a population-based study. Psychoneuroendocrinology. 2017;84:101–108. doi:10.1016/j.psyneuen.2017.06.021
23. Köhler-Forsberg O, Sylvia L, Deckersbach T, et al. Clinically relevant and simple immune system measure is related to symptom burden in bipolar disorder. Acta Neuropsychiatr. 2018;30(5):297–305. doi:10.1017/neu.2017.34
24. Köhler O, Sylvia LG, Bowden CL, et al. White blood cell count correlates with mood symptom severity and specific mood symptoms in bipolar disorder. Aust N Z J Psychiatry. 2017;51(4):355–365. doi:10.1177/0004867416644508
25. Beydoun HA, Beydoun MA, Wassertheil-Smoller S, et al. Depressive symptoms and antidepressant use in relation to white blood cell count among postmenopausal women from the women’s health initiative. Transl Psychiatry. 2024;14(1):157. doi:10.1038/s41398-024-02872-5
26. Kennedy SH, Lam RW, McIntyre RS, et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. pharmacological treatments. Can J Psychiatry. 2016;61(9):540–560. doi:10.1177/0706743716659417
27. Al-Karawi D, Jubair L. Bright light therapy for nonseasonal depression: meta-analysis of clinical trials. J Affect Disord. 2016;198:64–71. doi:10.1016/j.jad.2016.03.016
28. Pjrek E, Friedrich ME, Cambioli L, et al. The efficacy of light therapy in the treatment of seasonal affective disorder: a meta-analysis of randomized controlled trials. Psychother Psychosom. 2020;89(1):17–24. doi:10.1159/000502891
29. Wang S, Zhang Z, Yao L, Ding N, Jiang L, Wu Y. Bright light therapy in the treatment of patients with bipolar disorder: a systematic review and meta-analysis. PLoS One. 2020;15(5):e0232798. doi:10.1371/journal.pone.0232798
30. Guo B, Zhang M, Hao W, Wang Y, Zhang T, Liu C. Neuroinflammation mechanisms of neuromodulation therapies for anxiety and depression. Transl Psychiatry. 2023;13(1):5. doi:10.1038/s41398-022-02297-y
31. Zuo C, Cao H, Feng F, et al. Repetitive transcranial magnetic stimulation exerts anti-inflammatory effects via modulating glial activation in mice with chronic unpredictable mild stress-induced depression. Int Immunopharmacol. 2022;109:108788. doi:10.1016/j.intimp.2022.108788
32. Gasmi A, Shanaida M, Oleshchuk O, et al. Natural Ingredients to Improve Immunity. Pharmaceuticals. 2023;16(4):528. doi:10.3390/ph16040528
33. Subramaniapillai M, Carmona NE, Rong C, McIntyre RS. Inflammation: opportunities for treatment stratification among individuals diagnosed with mood disorders. Dialogues Clin Neurosci. 2017;19(1):27–36. doi:10.31887/DCNS.2017.19.1/rmcintyre
34. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732–741. doi:10.1016/j.biopsych.2008.11.029
35. Schmidt FM, Kirkby KC, Lichtblau N. Inflammation and immune regulation as potential drug targets in antidepressant treatment. Curr Neuropharmacol. 2016;14(7):674–687. doi:10.2174/1570159x14666160115130414
36. Kohler O, Krogh J, Mors O, Benros ME. Inflammation in depression and the potential for anti-inflammatory treatment. Curr Neuropharmacol. 2016;14(7):732–742. doi:10.2174/1570159x14666151208113700
37. Valiuliene G, Valiulis V, Zentelyte A, Dapsys K, Germanavicius A, Navakauskiene R. Anti-neuroinflammatory microRNA-146a-5p as a potential biomarker for neuronavigation-guided rTMS therapy success in medication resistant depression disorder. Biomed Pharmacother. 2023;166:115313. doi:10.1016/j.biopha.2023.115313
38. Roberts JE. Light and immunomodulation. Ann N Y Acad Sci. 2000;917(1):435–445. doi:10.1111/j.1749-6632.2000.tb05408.x
39. Thomas Broome S, Fisher T, Faiz A, et al. Assessing the anti-inflammatory activity of the anxiolytic drug buspirone using CRISPR-Cas9 gene editing in LPS-stimulated BV-2 microglial cells. Cells. 2021;10(6):1312. doi:10.3390/cells10061312
40. Petersein C, Sack U, Mergl R, et al. Impact of lithium alone and in combination with antidepressants on cytokine production in vitro. J Neural Transm. 2015;122(1):109–122. doi:10.1007/s00702-014-1328-6
41. Sakrajda K, Szczepankiewicz A. Inflammation-related changes in mood disorders and the immunomodulatory role of lithium. Int J Mol Sci. 2021;22(4):1532. doi:10.3390/ijms22041532
42. Chiu CT, Wang Z, Hunsberger JG, Chuang DM. Therapeutic potential of mood stabilizers lithium and valproic acid: beyond bipolar disorder. Pharmacol Rev. 2013;65(1):105–142. doi:10.1124/pr.111.005512
43. Song C, Luchtman D, Kang Z, et al. Enhanced inflammatory and T-helper-1 type responses but suppressed lymphocyte proliferation in patients with seasonal affective disorder and treated by light therapy. J Affect Disord. 2015;185:90–96. doi:10.1016/j.jad.2015.06.003
44. Benedetti F, Dallaspezia S, Melloni EMT, et al. Effective antidepressant chronotherapeutics (sleep deprivation and light therapy) normalize the IL-1β: IL-1ra ratio in bipolar depression. Front Physiol. 2021;12:740686. doi:10.3389/fphys.2021.740686
45. Eichler A, Kleidonas D, Turi Z, et al. Microglial cytokines mediate plasticity induced by 10 Hz repetitive magnetic stimulation. J Neurosci. 2023;43(17):3042–3060. doi:10.1523/jneurosci.2226-22.2023
46. Bai YW, Yang QH, Chen PJ, Wang XQ. Repetitive transcranial magnetic stimulation regulates neuroinflammation in neuropathic pain. Front Immunol. 2023;14:1172293. doi:10.3389/fimmu.2023.1172293
47. Feldman SR, Goffe B, Rice G, et al. The challenge of managing psoriasis: unmet medical needs and stakeholder perspectives. Am Health Drug Benefits. 2016;9(9):504–513.
48. Elliott JE, McBride AA, Balba NM, et al. Feasibility and preliminary efficacy for morning bright light therapy to improve sleep and plasma biomarkers in US Veterans with TBI. A prospective, open-label, single-arm trial. PLoS One. 2022;17(4):e0262955. doi:10.1371/journal.pone.0262955
49. Pedraz-Petrozzi B, Insan S, Spangemacher M, et al. Association between rTMS-induced changes in inflammatory markers and improvement in psychiatric diseases: a systematic review. Ann Gen Psychiatry. 2024;23(1):31. doi:10.1186/s12991-024-00514-0
50. Costello A, Linning-Duffy K, Vandenbrook C, Lonstein JS, Yan L. Effects of bright light therapy on neuroinflammatory and neuroplasticity markers in a diurnal rodent model of seasonal affective disorder. Ann Med. 2023;55(2):2249015. doi:10.1080/07853890.2023.2249015
51. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
52. Demirkol ME, Namlı Z, Tamam L. Efficacy of light therapy on non-seasonal depression and inflammatory markers. Eur J Psych. 2019;33(3):104–111. doi:10.1016/j.ejpsy.2019.03.002
53. Koh DH. The relationship between heated cigarette smoking and blood white blood cell count: a population-based cross-sectional study. Public Health. 2023;222:154–159. doi:10.1016/j.puhe.2023.07.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.