Back to Journals » Journal of Pain Research » Volume 13
Combination of Gluteal Trigger Points Dry Needling and Percutaneous Endoscopic Lumbar Discectomy for Complex Low Back-Related Leg Pain
Authors Li S ![]() , Yi D, Luo Q
, Yi D, Luo Q ![]() , Jia D
, Jia D
Received 31 August 2020
Accepted for publication 23 October 2020
Published 24 November 2020 Volume 2020:13 Pages 3125—3129
DOI https://doi.org/10.2147/JPR.S279592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michael Schatman
Shuiqing Li, Duan Yi, Qipeng Luo, Donglin Jia
Department of Pain Medicine, Peking University Third Hospital, Beijing 100191, People’s Republic of China
Correspondence: Duan Yi
Department of Pain Medicine, Peking University Third Hospital, No. 49 North Garden Road, Haidian District, Beijing 100191, People’s Republic of China
Email [email protected]
Purpose: Causes of low back-related leg pain (LBLP) can be complex and diverse. A detailed medical history, physical examination, laboratory tests, and imaging are necessary to accurately distinguish the pathomechanisms of LBLP and determine the most appropriate treatment.
Case: In this study, we report the first documented case in which the combination of dry needling (DN) and percutaneous endoscopic lumbar discectomy (PELD) was used for a patient with active myofascial trigger points (MTrPs) in the gluteus minimus muscle as well as L3-4 lumbar disc herniation (LDH). This 63-year-old woman complained of LBLP for 3 months. After careful examination and analysis, we determined this pain originated from two active MTrPs in the gluteal region and not LDH in L3-4. We first performed MTrPs DN, and the patient’s LBLP was relieved completely. We then performed PELD at the L3-4 level for residual numbness on the medial and anterior aspect of the left lower limb. Finally, the patient received a satisfactory result.
Conclusion: The gluteal MTrPs test may be used as a routine examination for patients with LBLP, especially when clinical findings are discordant with imaging results.
Keywords: percutaneous endoscopic lumbar discectomy, dry needling, low back-related leg pain, myofascial trigger points
Introduction
Chronic low back-related leg pain (LBLP) is one of the most commonly encountered clinical problems in pain clinics. It is a complex and diverse disorder, which brings a great challenge to differential diagnosis and pain management, and the premise of pain treatments is to have good recognition of pathomechanism of pain and its common etiologies include lumbar disc herniation (LDH), lumbosacral spondylosis, lumbar spinal stenosis, spondylolisthesis, piriformis syndrome, pelvic tumors, pregnancy, and myofascial trigger points (MTrPs) and so on.1,2 MTrPs were first described by Travell in 1942. They are now recognized as a common cause of pain in patients presenting with musculoskeletal pain.3 Epidemiologic data suggest that the lifetime prevalence of MTrPs may be as high as 85% in the general population.4 According to Travell and Simons,3,5 MTrPs are defined as one or more hyperirritable nodules in the taut band of skeletal muscles that are painful upon compression and can evoke referred pain and related autonomic responses. Several studies have reported the frequent presence of active MTrPs in patients with low back pain with or without radicular pain.2,6,7 Travell and Simons first suggested that active MTrPs in the posterior gluteal minimus muscle could imitate LBLP, with pain referred to the lateral thigh and the posterior region below the knee. This is similar to the symptoms of S1 radiculopathy, named “pseudoradicular syndrome” of myofascial origin.5
As such, the clinical diagnosis and management of LBLP is difficult. Herein, we report the case of a patient who experienced LBLP due to LDH at the L3-4 level with coexistence of gluteal minimus MTrPs.
Case Presentation
A 63-year-old woman presented to the pain clinic of our hospital in October 2017 with a 3-month history of chronic sciatic-type left leg pain. We first performed MTrPs dry needling (DN) followed by percutaneous endoscopic lumbar discectomy (PELD) at the L3-4 level. We followed up the case at postoperative 15 days, 3 months, and 6 months. The patient’s symptoms were relieved at the last follow-up.
Symptoms
The patient’s symptoms started in July 2017 with no significant inducement. She reported moderate pain in the left gluteal muscle, posterolateral thigh, and posterior calf, numbness in the medial calf, and discomfort in the lower back. These symptoms were exacerbated by prolonged sitting and long-distance walking and were initially alleviated by bed rest in the first month. She was evaluated by a local general practitioner who diagnosed her with lumbar disc herniation and prescribed non-steroidal anti-inflammatory drugs; her pain improved slightly. However, in the following 2 months, her pain progressively worsened. She could not stand or walk on her own and reported experiencing intractable pain, even in bed when she was admitted to our pain management ward in October 2017. On a visual analog scale (VAS), the pain score of the left buttock and leg was 8 on average. Oral analgesics (such as tramadol) and physical therapy were not beneficial.
Relevant Physical Examination
The superficial sensation of the anteromedial aspect of the left lower leg, the myodynamia of the left tibialis anterior, and the reflex of the left patellar tendon decreased when compared with the right side. Mild tenderness and percussion pain of the L3-4 interspinous space were found, and the left femoral nerve stretch test was positive.
It is worth noting that the patient complained of two exact pain points in buttocks without a press and two intense tender points were palpated in the left superior gluteal area with significant pain points (probably gluteus minimus), not on the piriformis muscle region (Figure 1), and the pain referred to the posterolateral aspect of the thigh and the peroneal region of the lower leg (the region in which the patient complained of pain) when these two trigger points were pressed. Moreover, palpation of a taut band and tender nodules in the taut band were found. Based on Travell and Simons’ theory and diagnostic criteria,3,5 we suspected the patient’s pain originated from an active trigger point in the gluteus minimus muscle instead of lumbar disc herniation. Dr. Yi performed the examinations.
 |
Figure 1 Two marked intense tender points on the left superior gluteal area. |
Other tests, including the Patrick test, straight leg raise test, and piriformis tension test, were all negative. There was no palpable trigger point on piriformis muscle region and other muscles in buttocks.
Imaging Manifestation
Lumbar X-ray showed mild scoliosis of the lumbar vertebra, mild collapse of the L3-4 intervertebral space, and mild forward slip of the L3 centrum (Figure 2).
 |
Figure 2 Frontal and lateral view of X-ray showed mild scoliosis of lumbar vertebra, mild collapse of L3-4 intervertebral space, and mild forward slip of L3 centrum. |
Lumbar MRI showed L3-4 intervertebral disc extrusion with dural sac compression and left L4 nerve root compression, as well as mild intervertebral disc bulging without dural sac and nerve compression at the L4-5 and L5-S1 levels (Figure 3).
 |
Figure 3 Sagittal and axial view of MRI scan showed L3-4 intervertebral disc extrusion with dural sac and left L4 nerve root compression. |
Ultrasound of the hip was used to exclude the possibility of piriformis syndrome.
Treatment Strategy and Results
The LBLP area of which the patient complained differed from the distribution where the L4 nerve root usually innervated. It was similar to the region of the S1 nerve root, which meant we could not immediately perform an L3-4 discectomy. Instead, we found intense tenderness in the superior lateral quadrant of the left buttock and referred pain in the left leg.
We performed DN (Figure 4). First, the two trigger points within the gluteus muscle that provoked the referred pain were marked. Then, we inserted a 0.25×75-mm needle at these two spots using a rapid needle entry and exit technique, and a local surface muscle response was observed. After 2 min of manipulation, the response disappeared, and the needle was pulled out. The patient reported soreness in the buttock, but the pain in her right leg was immediately and completely relieved. She could walk and sit normally and did not feel pain in the next 2 days. However, she still complained of numbness on the medial and anterior aspect of the left lower leg that was especially aggravated with long-distance walking. We believed that the remnant numbness came from L3-4 lumbar disc herniation, and we successfully performed percutaneous endoscopic lumbar disc discectomy (PELD) 2 days after DN treatment. She was discharged from the hospital 1 day after the surgery.
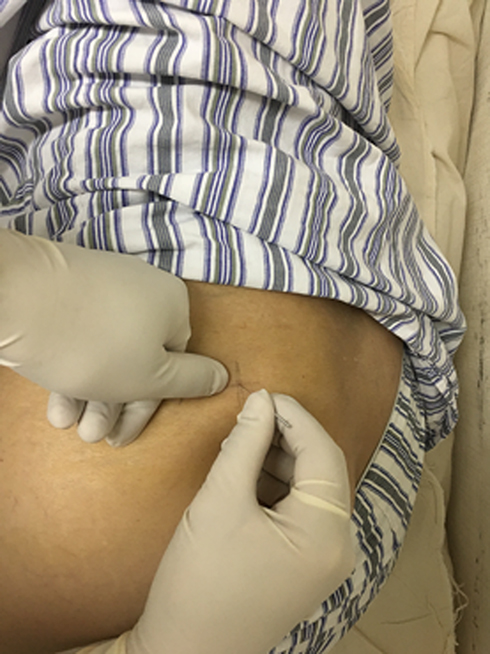 |
Figure 4 Dry needling for these two marked gluteal trigger points. |
We followed up the case at postoperative 15 days, 3 months and 6 months. The numbness gradually relieved after the surgery and six months after the operation, the patient reported that the numbness had disappeared and the VAS was 1. She said mild pain occasionally occurred in the left leg after prolonged sitting or walking, but it did not affect her quality of life.
Discussion
This is an interesting case and similar cases of combined therapy have rarely been reported before. The patient suffered from LBLP, in detail, we found the patient had L3-4 LDH, while pain originated from gluteal minimus MTrPs. We first performed MTrPs DN to solve firstly complained pain from gluteal minimus MTrPs, followed by L3-4 PELD to further deal with the numbness on the medial and anterior aspect of the left lower leg, and the patient received satisfactory results.
The reason why we first performed the DN treatment was that the patient mainly and firstly complained of pain in posterolateral aspect of the thigh and the peroneal region of the lower leg when admission to hospital, which was the referred regions of L5-S1 nerve root and not consistent with the lesion in MRI imaging – L3-4 LDH, and the patient complained of 2 identified pain points in buttocks and the pain in the posterolateral aspect of the thigh and the peroneal region of the lower leg could be triggered, thus we firstly performed diagnostic and therapeutic DN treatment to solve the pain. After the treatment of DN, the patient complained of numbness, which became the main problem to the patient. Therefore, we further performed the PELD 2 days after DN to solve the numbness on the medial and anterior aspect of the left lower leg.
LDH is the most common pathological condition resulting in LBLP.1 Almost 20% of adults in China with low back and leg pain are diagnosed with LDH.8 LDH occurs mainly at the L4-5 and L5-S1 levels; upper LDH (L3-4 and above) is rare.9 Although the overall diagnostic accuracies of neurological testing procedures in detecting lumbar radicular pain is poor10 and a novel adjunctive tool to detect lumbar radicular pain was recently reported,11 in this patient, the numbness on the left medial calf and abnormal findings on physical examination (decline of superficial sensation in the left medial calf, tibialis anterior myodynamia and patellar tendon reflex, and a positive result of the femoral nerve traction test) could all be attributed to compression of the spinal L4 nerve root by L3-4 protruded disc materials when combined with the imaging in lumbar MRI. However, it should be noted that the patient’s pain distribution was not in an area commonly innervated by the L4 nerve root but instead by the L5 or S1 nerve root, there was no significant herniation at the L4-5 or L5-S1 levels, and the full spinal X-ray excluded the presence of transitional vertebra. Therefore, the mechanical compression of LDH could not explain the LBLP in this patient;1 other related reasons should be taken into consideration.
In the present case, we found two active MTrPs in the superior lateral quadrant of the gluteal area that were in a similar palpation region according to Travell and Simons criteria. It is difficult to clearly distinguish the exact muscle containing the MTrPs simply by palpation, the MTrPs should be gluteal minimus muscle according to Travell and Simons criteria. Future studies should utilize ultrasound or other tools to accurately determine the position of MTrPs.
DN is frequently used for MTrPs; DN targeted to MTrPs can disrupt the dysfunctional neuromuscular activity in the muscles, decrease muscle tone, and normalize the neurochemical pathways of muscles.3,5 Several studies have demonstrated that DN of MTrPs could provide immediate or short-term benefit for CLBP, but its long-term effects remain unclear, and further high-quality, long-term trials are needed.12–14 In this case, we performed gluteal MTrPs DN only once, and the patient’s pain was relieved in a 6-month follow-up. Skorupska et al15 reported a similar case: For a young man with a 3-year history of LBLP, laser decompression for L5-S1 lumbar disc minor herniation did not work. Active MTrPs were found in the gluteus minimus muscle. The patient received five sessions of DN, once each week, and the pain was resolved by the end. The number of DN sessions differed in these two cases, but the pain-relief effects were similar. The optimal frequency of DN is yet to be determined.
After DN therapy, the patient’s referred pain disappeared, while numbness of the lower leg and other abnormal physical examination results due to L3-4 LDH remained. As such, we proceeded to the next stage and performed PELD, a minimally invasive procedure for the treatment of LDH that has been widely used recently. Many clinical studies have confirmed that PELD for soft LDH has similar long-term results to conventional open discectomy and has obvious advantages such as smaller incision and shorter operation time, hospital stay, and recovery time.16,17 Therefore, we chose PLED as an ideal treatment plan.
Conclusions
Causes of LBLP can be complex and diverse, involving LDH, MTrPs, and more. A detailed medical history, physical examination, laboratory tests, and imaging are necessary to accurately diagnose the condition and provide proper treatment. A gluteal MTrPs test should be used as a routine examination, and gluteal MTrPs DN might be a reasonable treatment for patients with radicular LBP, especially when clinical findings are discordant with imaging results. We report the first documented case of the combined application of MTrPs DN and PELD for a patient with active trigger points in the gluteus minimus muscle as well as L3-4 LDH. We look forward to more applications of similar combined interventional treatments for complex LBLP.
Ethical Statement
Institutional approval was not required to publish the case details, but the patient provided written informed consent for publication of her case details.
Acknowledgment
The authors would like to thank the patient for her generosity in allowing her case to be presented for publication.
Funding
There was no external funding for the preparation of this manuscript.
Disclosure
The authors have no conflicts of interest to report.
References
1. Ropper A, Zafonte R. Sciatica. N Engl J Med. 2015;372(13):1240–1248. doi:10.1056/NEJMra1410151
2. Adelmanesh F, Jalali A, Jazayeri Shooshtari SM, Raissi GR, Ketabchi SM, Shir Y. Is there an association between lumbosacral radiculopathy and painful gluteal trigger points? A cross-sectional study. Am J Phys Med Rehabil. 2015;94(10):784–791. doi:10.1097/PHM.0000000000000261
3. Simons DG, Travell JG. Myofascial Pain and Dysfunction: The Trigger Point Manual, Vol 1: Upper Half of Body.
4. Fleckenstein J, Zaps D, Rüger LJ, et al. Discrepancy between prevalence and perceived effectiveness of treatment methods in myofascial pain syndrome: results of a cross-sectional, nationwide survey. BMC Musculoskelet Disord. 2010;11:32. doi:10.1186/1471-2474-11-32
5. Travell JG. Myofascial Pain and Dysfunction, the Trigger Point Manual, Vol. 2. The Lower Extremities. Williams & Wilkins, Lippincott; 1992.
6. Lluch E, Nijs J, De Kooning M, et al. Prevalence, incidence, localization, and pathophysiology of myofascial trigger points in patients with spinal pain: a systematic literature review. J Manipulative Physiol Ther. 2015;38(3):587–600. doi:10.1016/j.jmpt.2015.08.004
7. Iglesias-González JJ, Muñoz-García MT, Rodrigues-de-Souza DP, Alburquerque-Sendín F, Fernández-de-las-Peñas C. Myofascial trigger points, pain, disability, and sleep quality in patients with chronic nonspecific low back pain. Pain Med. 2013;14(12):1964–1970. doi:10.1111/pme.12224
8. Chen R, Xiong J, Chi Z, Zhang B. Heat-sensitive moxibustion for lumbar disc herniation: a meta-analysis of randomized controlled trials. J Tradit Chin Med. 2012;32(3):322–328. doi:10.1016/s0254-6272(13)60032-1
9. Albert TJ, Balderston RA, Heller JG, et al. Upper lumbar disc herniations. J Spinal Disord. 1993;6(4):351–359. doi:10.1097/00002517-199306040-00009
10. Al Nezari NH, Schneiders AG, Hendrick PA. Neurological examination of the peripheral nervous system to diagnose lumbar spinal disc herniation with suspected radiculopathy: a systematic review and meta-analysis. Spine J. 2013;13(6):657–674. doi:10.1016/j.spinee.2013.02.007
11. Samolsky Dekel BG, Sorella MC, Vasarri A, Melotti RM. Reliability of the buttock applied strain test to diagnose radicular pain in patients with low back pain. Pain Pract. 2020. doi:10.1111/papr.12890
12. Tüzün EH, Gıldır S, Angin E, Tecer BH, Dana KÖ, Malkoç M. Effectiveness of dry needling versus a classical physiotherapy program in patients with chronic low-back pain: a single-blind, randomized, controlled trial. J Phys Ther Sci. 2017;29(9):1502–1509. doi:10.1589/jpts.29.1502
13. Liu L, Huang QM, Liu QG, et al. Evidence for dry needling in the management of myofascial trigger points associated with low back pain: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2018;99(1):144–152. doi:10.1016/j.apmr.2017.06.008
14. Koppenhaver SL, Walker MJ, Smith RW, et al. Baseline examination factors associated with clinical improvement after dry needling in individuals with low back pain. J Orthop Sports Phys Ther. 2015;45(8):604–612. doi:10.2519/jospt.2015.5801
15. Skorupska E, Rychlik M, Pawelec W, Bednarek A, Samborski W. Trigger point-related sympathetic nerve activity in chronic sciatic leg pain: a case study. Acupunct Med. 2014;32(5):418–422. doi:10.1136/acupmed-2013-010504
16. Ahn Y, Lee SG, Son S, Keum HJ. Transforaminal endoscopic lumbar discectomy versus open lumbar microdiscectomy: a comparative cohort study with a 5-year follow-up. Pain Physician. 2019;22(3):295–304.
17. Li X, Han Y, Di Z, et al. Percutaneous endoscopic lumbar discectomy for lumbar disc herniation. J Clin Neurosci. 2016;33:19–27. doi:10.1016/j.jocn.2016.01.043
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.