Back to Journals » Infection and Drug Resistance » Volume 19
Combination of Ceftazidime-Avibactam and Aztreonam Effectively Treated Post-Cardiac Surgery Pneumonia Caused by Hypervirulent KPC- and NDM-Producing Klebsiella pneumoniae: A Case Report
Authors Wei Q, Cong R, Shen C, Chen C, Cao Z, Ren C, Liu T
Received 16 December 2025
Accepted for publication 11 March 2026
Published 23 March 2026 Volume 2026:19 589388
DOI https://doi.org/10.2147/IDR.S589388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Qimei Wei,1,* Rong Cong,1,* Chang Shen,2 Chen Chen,1 Zheng Cao,1 Chanjun Ren,3 Tingting Liu2
1Department of Clinical Laboratory, Wuhan Asia Heart Hospital, Wuhan, 430022, People’s Republic of China; 2Department of Cardiac Critical Care Medicine, Wuhan Asia Heart Hospital, Wuhan, 430022, People’s Republic of China; 3Department of Laboratory Medicine, Wuhan Kingmed Center for Clinical Laboratory, Wuhan, 430022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tingting Liu, Department of Cardiac Critical Care Medicine, Wuhan Asia Heart Hospital, No. 753 Jinghan Avenue, Jianghan District, Wuhan, 430022, People’s Republic of China, Tel +86 18627794672, Email [email protected]
Background: Hypervirulent carbapenem‑resistant Klebsiella pneumoniae (hv-CRKP) co‑producing Klebsiella pneumoniae carbapenemase‑2 (KPC‑2) and New Delhi metallo‑β‑lactamase‑1 (NDM‑1) represents a serious clinical threat due to limited treatment options and high mortality. This study aimed to describe the clinical course, microbiological characteristics, and therapeutic outcome of a severe postoperative pneumonia caused by such a strain, and to evaluate the effectiveness of combination antimicrobial therapy.
Case Presentation: A 59‑year‑old woman developed severe pneumonia and acute respiratory distress syndrome following cardiac surgery. Bronchoalveolar lavage fluid culture yielded carbapenem‑resistant K. pneumoniae. Antimicrobial susceptibility testing showed resistance to meropenem (minimum inhibitory concentration [MIC] ≥ 16 μg/mL), ceftazidime‑avibactam (CZA) (MIC ≥ 16/4 μg/mL), and aztreonam (ATM) (MIC ≥ 64 μg/mL). Molecular analysis identified blaKPC and blaNDM carbapenemase genes and hypervirulence‑associated genes including rmpA and iucA. In vitro synergy testing demonstrated a marked reduction in MIC (≤ 1 μg/mL) when CZA was combined with ATM. Based on these findings, combination therapy was initiated, resulting in rapid clinical improvement, a decline in procalcitonin levels from 4.83 ng/mL to 0.5 ng/mL, radiographic resolution of pulmonary infiltrates, and sustained microbiological clearance.
Conclusion: This case demonstrates that CZA combined with ATM may be an effective therapeutic option for severe infections caused by hypervirulent KPC‑2‑ and NDM‑1‑producing K. pneumoniae. Early molecular identification and synergy‑guided antimicrobial therapy are essential for optimizing outcomes in critically ill patients.
Keywords: Carbapenem-resistant Klebsiella pneumoniae, hypervirulent Klebsiella pneumoniae, KPC, NDM, ceftazidime-avibactam, aztreonam
Introduction
Carbapenem‑resistant Klebsiella pneumoniae (CRKP) represents a critical and escalating global public health threat, particularly in hospital and intensive care unit settings. Of special concern are strains co‑producing blaKPC and blaNDM carbapenemases (KN-CRKP), which exhibit extensive resistance to nearly all β‑lactam antibiotics and are associated with markedly increased mortality.1 Recent epidemiological studies indicate that the prevalence of KN-CRKP among CRKP isolates has risen steadily worldwide over the past decade, reflecting ongoing plasmid‑mediated dissemination and selective antibiotic pressure.2 In China, this problem is compounded by the rapid emergence of hypervirulent CRKP (hv‑CRKP), most commonly associated with the ST11‑KL64 lineage, which combines multidrug resistance with enhanced invasiveness and poor clinical outcomes.3,4
The convergence of carbapenem resistance and hypervirulence represents a particularly alarming evolution of K. pneumoniae. Hypervirulent strains harbor virulence determinants such as rmpA and aerobactin‑associated genes, which promote hypermucoviscosity, immune evasion, and metastatic infection.3 When these virulence traits coexist with KPC and NDM carbapenemases, treatment options become extremely limited and mortality rates are substantially higher than those observed with classic CRKP infections.5 Although this dual‑risk pathogen is increasingly recognized, clinical data supporting effective therapeutic strategies remain scarce. This is especially true for critically ill postoperative patients.
Ceftazidime‑avibactam (CZA) has become an important option for treating infections caused by KPC‑producing Enterobacterales, but it lacks activity against metallo‑β‑lactamases such as NDM.6 In contrast, aztreonam (ATM) is intrinsically stable to NDM but is often hydrolyzed by co‑produced serine β‑lactamases, limiting its use as monotherapy.7 The combination of CZA and ATM provides a mechanistically rational approach to overcoming this resistance profile, and current Infectious Diseases Society of America (IDSA) guidelines recommend this regimen for infections caused by metallo‑β‑lactamase–producing organisms.8 However, real‑world clinical evidence supporting this strategy in hypervirulent KPC–NDM‑co‑producing K. pneumoniae, particularly in severe pneumonia and acute respiratory distress syndrome after cardiac surgery, is limited.
In this context, we report a case of post‑cardiac surgery pneumonia caused by hypervirulent KPC‑2‑ and NDM‑1‑producing K. pneumoniae that was successfully treated with microbiologically guided CZA plus ATM combination therapy. This case highlights the clinical importance of early pathogen characterization, in vitro synergy testing, and individualized antimicrobial selection, and it contributes practical evidence to inform the management of similarly challenging infections in high‑risk surgical patients.
Case Presentation
A 59-year-old woman was admitted to our hospital with a six-month history of intermittent chest tightness and shortness of breath. She also had a recent episode of syncope accompanied by fecal incontinence. Six months earlier, she had experienced unexplained chest tightness and dyspnea, without chest pain or dizziness. An external transthoracic echocardiogram revealed a dilated ascending aorta, left heart enlargement, and moderate-to-severe mitral regurgitation. Coronary angiography demonstrated 80% stenosis in the proximal-to-mid left anterior descending artery. The patient was initially hospitalized locally on February 11, 2025, and received medical management, including circulatory support, diuretics, antiplatelet agents, and lipid-lowering therapy, with subsequent improvement in symptoms.
One month prior to the current admission, the patient experienced a syncopal episode accompanied by urinary and fecal incontinence, which led to another hospitalization. She was subsequently referred to our institution for further evaluation and management. Her past medical history was notable for hypertension and prior stroke. On admission, vital signs were stable and there were no remarkable findings on physical examination. Preliminary diagnoses included coronary artery disease, unstable angina, valvular heart disease, and mitral regurgitation. After multidisciplinary evaluation, surgical intervention was indicated.
The patient underwent successful coronary artery bypass grafting (CABG ×3), mitral valve bioprosthesis replacement, and tricuspid valve annuloplasty under general anesthesia, hypothermia, and cardiopulmonary bypass. Postoperatively, she was transferred to the intensive care unit (ICU) for continued sedation, mechanical ventilation, hemodynamic monitoring, and cardiac support. Prophylactic cefazolin was administered intraoperatively.
On postoperative day (POD) 1, the patient’s body temperature began to rise above 38°C. Laboratory tests revealed leukocytosis (WBC 16.5 × 109/L) and elevated procalcitonin (PCT 0.54 ng/mL). Chest X-ray demonstrated significant pulmonary infiltrates, and concomitant arterial blood gas analysis confirmed the presence of hypoxemia. Bronchoscopy revealed congested airway mucosa and thick secretions obstructing both main bronchi; bronchoalveolar lavage (BAL) was performed and samples were sent for microbiological analysis. Empirical antibiotic therapy was escalated to piperacillin-tazobactam (4.5 g every 8 hours) for suspected hospital-acquired pneumonia.
On POD 2, the patient’s body temperature continued to rise, reaching 38.6°C. Inflammatory markers further increased (WBC 21.5 × 109/L, PCT 4.83 ng/mL), and arterial blood gas analysis showed a PaO2/FiO2 ratio of 158 mmHg, consistent with acute respiratory distress syndrome (ARDS). Antibiotic therapy was changed to meropenem (1 g every 8 hours).
On POD 3, BAL cultures from samples obtained on POD 1 identified CRKP. Initial susceptibility testing indicated resistance to all tested antibiotics except aminoglycosides and polymyxins (Table 1). Prior to BAL specimen collection, the only in‑hospital antimicrobial exposure was intraoperative prophylactic cefazolin. Information regarding antibiotic use before transfer to our institution was unavailable, as neither the patient nor her family could provide specific details. Preliminary carbapenemase phenotyping suggested concurrent production of KPC and NDM (Figure 1). Metagenomic next-generation sequencing of BAL fluid (performed using a targeted capture-based mNGS workflow on an Illumina MiniSeq platform, with human read removal and alignment to curated microbial reference databases downloaded from NCBI) confirmed the presence of K. pneumoniae with resistance genes blaKPC-2 and blaNDM-1, as well as hypervirulence genes (iutA, iucA [A/B/C/D], ompA, rmpA, rmpA2). Additional susceptibility testing for CZA, ATM, and their combination was performed. Both broth microdilution (Figure 2A) and disk diffusion (Kirby-Bauer, Figure 2B) methods demonstrated resistance to each agent alone but marked synergy for the combination, with a fractional inhibitory concentration (FIC) index of 0.006 and MICs of (0.5/4)/1 (CZA /ATM).
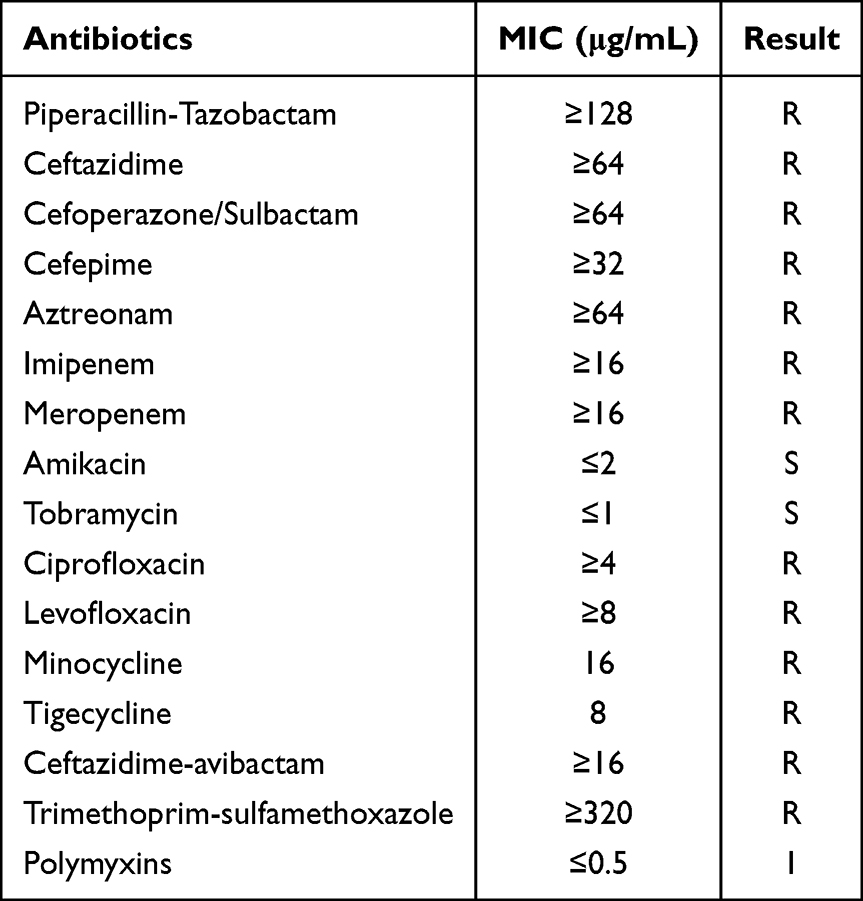 |
Table 1 Results of Drug Resistance Phenotypes of Klebsiella Pneumoniae by MIC Drug Susceptibility Testing |
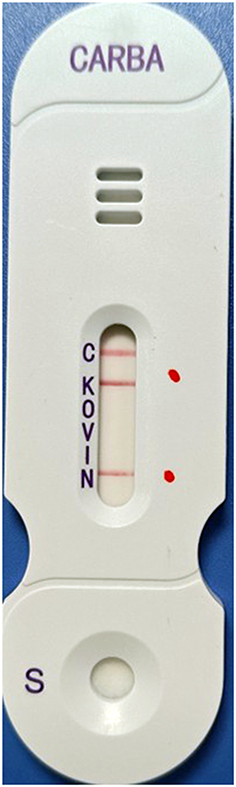 |
Figure 1 Phenotypic assay indicating concurrent production of KPC (K) and NDM (N) carbapenemases. The red dots are placed adjacent to the “K” and “N” bands to highlight the positive detection of KPC and NDM, respectively. |
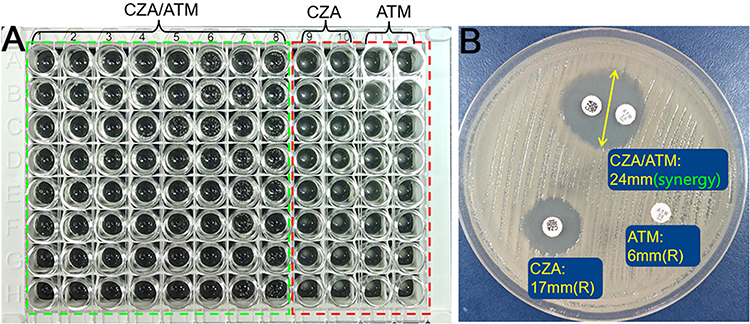 |
Figure 2 In vitro antimicrobial susceptibility testing. (A) Broth microdilution results showing resistance to ceftazidime-avibactam (CZA) and aztreonam (ATM) as single agents, with marked synergy observed when used in combination. The area marked by the green dashed line represents the testing wells for the CZA/ATM combination, whereas the area marked by the red dashed line represents the testing wells for CZA and ATM as single agents. (B) Disk diffusion (Kirby-Bauer) results confirming resistance to each agent alone and demonstrating synergistic inhibition when CZA and ATM are combined. The yellow double-sided arrow indicates the maximum diameter of the synergistic zone of inhibition between the CZA and ATM disks. |
Based on these findings, targeted therapy with CZA (2.5 g every 8 hours) combined with ATM (2 g every 8 hours) was initiated on POD 4. The clinical course, laboratory parameters, imaging findings, and therapeutic interventions from POD 1 to POD 8 are summarized in Table 2. During the five days of combination therapy, the patient’s body temperature returned to normal. Inflammatory markers have also improved, with WBC decreasing to 14.1 × 109/L and PCT to 0.5 ng/mL. Follow-up chest X-ray showed a marked contrast to previous imaging, with the original patchy shadows having been absorbed and dissipated, and the lung fields becoming clear (Figure 3). Subsequent sputum cultures were negative for K. pneumoniae. With continued clinical improvement, the patient was transferred from the ICU to the general ward on POD 8. Combination antibiotic therapy was continued for a total of two weeks, during which repeat sputum cultures remained negative. Following approximately four additional weeks of cardiac rehabilitation and arrhythmia management on the general ward, the patient was discharged in stable condition on POD 43.
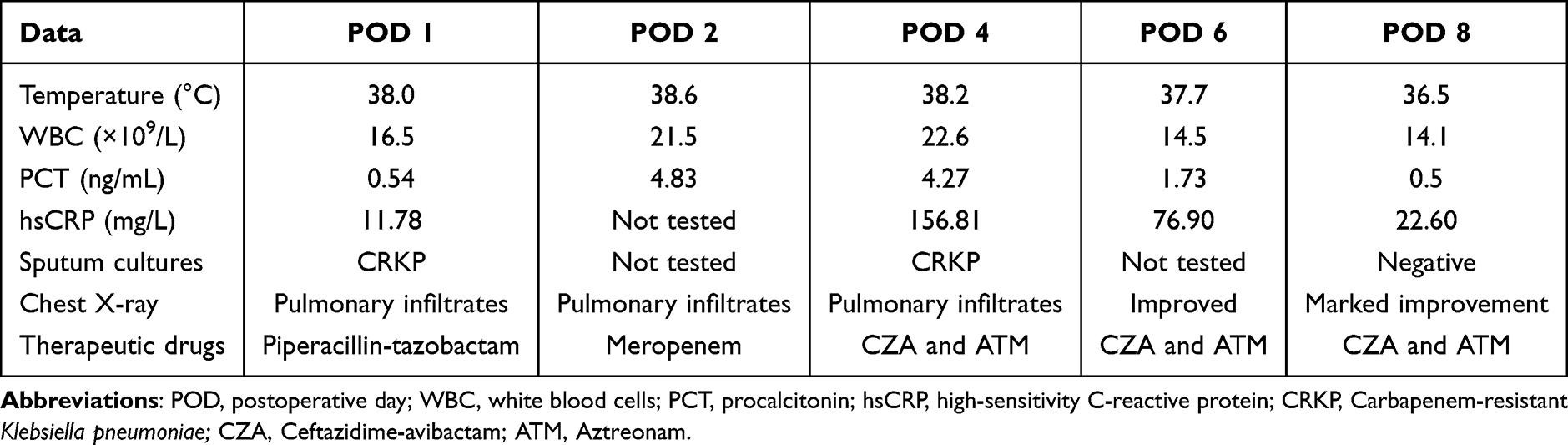 |
Table 2 Clinical Parameters, Microbiological Findings, Imaging, and Therapeutic Interventions from Postoperative Day 1 to 8 |
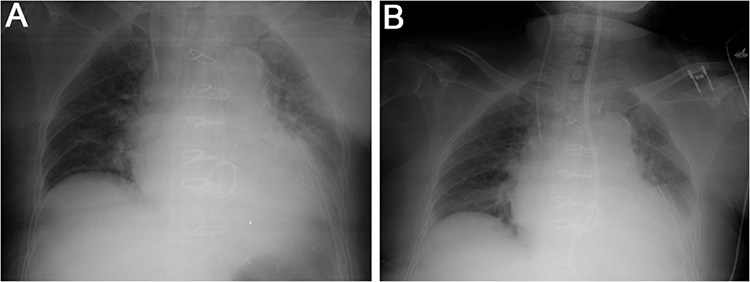 |
Figure 3 Radiological evolution during treatment. (A) Chest X-ray showing significant pulmonary infiltrates; (B) Follow-up chest X-ray demonstrating resolution of infiltrates and clear lung fields. |
Discussion
The present report illustrates the effective management of a severe case of pneumonia and ARDS triggered by a hv-CRKP strain harboring both KPC-2 and NDM-1 carbapenemases. The rapid progression to ARDS highlights the highly invasive and life-threatening nature of hv-CRKP infections, which are frequently associated with sepsis and metastatic complications.9 Early microbiological identification and tailored combination therapy were pivotal in achieving a favorable outcome, emphasizing the importance of prompt diagnosis and individualized treatment approaches for such dual-risk pathogens.
The exceptionally high level of antimicrobial resistance observed in this case can be explained by the convergence of multiple resistance‑promoting factors. Foremost, the simultaneous production of KPC‑2 and NDM‑1 carbapenemases confers resistance to nearly all β‑lactam antibiotics, including carbapenems, and severely limits therapeutic options. In addition, hv‑CRKP strains, particularly those belonging to epidemic clones, are prone to acquiring resistance determinants via plasmids and transposons. This genetic plasticity facilitates the emergence of multidrug‑resistant and extensively drug‑resistant phenotypes.1,5 Although the patient’s individual antibiotic exposure before admission could not be fully reconstructed, the regional prevalence of carbapenemase‑producing K. pneumoniae and the circulation of high‑risk clones likely contributed to the emergence and maintenance of this highly resistant strain. Importantly, this case exemplifies the increasingly recognized convergence of hypervirulence and multidrug resistance, which amplifies both pathogenicity and treatment failure risk.
The aggressive clinical phenotype observed can be attributed to the pathogen’s distinct microbiological features. The presence of hypervirulence genes, such as iucA and rmpA, mirrors profiles reported in the literature for hv-CRKP strains responsible for invasive infections, including liver abscesses and bacteremia.10 Infections caused by hv‑CRKP co‑producing KPC and NDM are associated with a poor prognosis. One study reported a 30‑day mortality rate of 56% among patients with bacteremia caused by these strains.11 Similarly, a Chinese case series of eight patients with KPC‑2‑ and NDM‑1‑co‑producing hv‑CRKP reported a mortality rate of 75%, with pulmonary infections predominating among fatal cases.10
The ST11-KL64 clone has emerged as the predominant hv-CRKP type in China and is frequently linked to KPC-NDM co-production.12 Genomic analyses indicate that ST11-KL64 (Clone Group 1) accounts for 55% of global KN-CRKP isolates and is characterized by a hypermucoviscous phenotype and a propensity for metastatic spread.12 Although whole-genome sequencing was not performed, the co-production of KPC-2 and NDM-1 and the presence of a definitive hypervirulence gene profile strongly suggest our isolate belongs to the prevalent ST11-KL64 clone. This warrants heightened clinical vigilance.
Our case exemplifies the effective use of CZA plus ATM for treating pneumonia and ARDS caused by KPC-2- and NDM-1-co-producing hv-CRKP. This therapeutic approach has been increasingly reported in other severe infections caused by metallo-β-lactamase–producing Enterobacterales, particularly bloodstream and lower respiratory tract infections, where CZA/ATM was associated with improved survival compared with polymyxin- or tigecycline-based regimens.13,14 Current IDSA guidelines recommend the CZA/ATM combination or cefiderocol for infections with MBL-producing Enterobacterales,8 while advising against polymyxins due to nephrotoxicity, uncertain efficacy, and lack of Clinical and Laboratory Standards Institute (CLSI) susceptibility breakpoints. The synergistic mechanism involves avibactam protecting ceftazidime and ATM from hydrolysis by serine β-lactamases (such as KPC), while ATM retains stability against MBLs (such as NDM).15,16 In our patient, in vitro synergy testing yielded an extremely low FIC index of 0.006, providing a strong rationale for combination therapy. Compared with alternative strategies, including cefiderocol monotherapy, polymyxin‑based combinations, or tigecycline‑containing regimens, CZA/ATM offered a favorable balance of microbiological efficacy, pulmonary penetration, and safety. These characteristics were particularly important in the setting of ARDS. The patient’s rapid clinical improvement, evidenced by declining inflammatory markers, radiographic resolution, and negative cultures within five days, supports the regimen’s efficacy and aligns with retrospective studies reporting lower mortality for CZA/ATM in NDM-producing bacteremia.14,17
Although a fixed-dose aztreonam–avibactam combination was recently approved in China (June 2025). However, issues of accessibility and cost remain practical barriers. In the absence of direct comparative studies, treatment decisions should be guided by susceptibility profiles, infection site, and local resource availability. Where the fixed‑dose combination is unavailable, CZA/ATM remains a practical and effective therapeutic option for infections caused by KPC‑ and NDM‑co‑producing hv‑CRKP. This approach is particularly well supported when in vitro synergy is demonstrated. Beyond conventional antibiotics, experimental studies have explored natural antibacterial agents, such as medium‑ and long‑chain fatty acids, which have demonstrated in vitro activity against NDM‑1‑producing and carbapenem‑resistant K. pneumoniae. Notably, Kwiatkowski et al and Mohamed et al reported membrane‑disruptive effects and growth inhibition of CRKP strains.18,19 However, these approaches remain preclinical or adjunctive in nature, and robust clinical evidence supporting their use in severe infections such as pneumonia or ARDS is currently lacking. Consequently, while promising, natural antibacterial agents cannot yet replace evidence‑based combination antibiotic therapy in critically ill patients.
Regarding the infection source, this case represents the first isolation of a KPC-NDM-co-producing hv-CRKP at our institution. Given the patient’s recent hospitalizations elsewhere and the early post-operative isolation from bronchoalveolar lavage fluid, exogenous acquisition is likely, rather than nosocomial transmission within our hospital. Although pre-operative nasal screening was negative, this case highlights the potential utility of broader screening (eg., rectal swabs) for intestinal colonization in high-risk patients.
This study has several notable limitations. Primarily, the absence of whole-genome sequencing prevented the confirmation of the strain’s clonal lineage and relatedness, highlighting the need for future investigations to incorporate molecular epidemiology for precise tracking. Clinically, our understanding of the patient’s prior exposure to antimicrobial agents is restricted, as a complete long-term antibiotic history (eg., over the past decade) could not be obtained due to her limited recall. Ultimately, while the CZA and ATM combination was effective in this instance, its long-term safety and the potential for resistance emergence warrant further evaluation in larger prospective cohorts.
Conclusion
In summary, we achieved favorable clinical outcomes in a patient with post-cardiac surgery pneumonia caused by hv-CRKP co-producing KPC-2 and NDM-1 through rapid pathogen identification and targeted combination therapy. Rapid pathogen identification using combined conventional and metagenomic methods, along with synergy-guided CZA plus ATM therapy, were key to clinical recovery. Where new fixed-dose regimens are unavailable, this combination remains a practical alternative. Clinicians should maintain vigilance for hv-CRKP in high-risk patients, emphasizing the importance of rapid diagnosis and personalized therapy.
Compliance with Ethics Guidelines
All identifying information has been removed or anonymized throughout the manuscript. The patient has provided written informed consent for publication of the case details and images. All patient data was handled in accordance with applicable data protection regulations, ensuring that any information collected was stored securely and accessed only by authorized personnel. This study was approved by the Medical Ethics Committee of the Wuhan Asia Heart Hospital (approval no. 2025-B042), and this institutional approval covers the publication of the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Qimei Wei and Rong Cong contributed equally to this work and should be considered as co-first authors. The authors declare that they have no conflicts of interest for this work.
References
1. Gao H, Liu Y, Wang R, Wang Q, Jin L, Wang H. The transferability and evolution of NDM-1 and KPC-2 co-producing Klebsiella pneumoniae from clinical settings. EBioMedicine. 2020;51:102599. doi:10.1016/j.ebiom.2019.102599
2. Guo H, Wu Y, Li L, Wang J, Xu J, He F. Global emergence of carbapenem-resistant Klebsiella pneumoniae co-carrying multiple carbapenemases. Comput Struct Biotechnol J. 2023;21:3557–8. doi:10.1016/j.csbj.2023.07.013
3. Huang J, Yi M, Yuan Y, et al. Emergence of a fatal ST11-KL64 tigecycline-resistant hypervirulent Klebsiella pneumoniae clone cocarrying blaNDM and blaKPC in plasmids. Microbiol Spectr. 2022;10(6):e0253922. doi:10.1128/spectrum.02539-22
4. Zhao J, Liu C, Liu Y, et al. Genomic characteristics of clinically important ST11 Klebsiella pneumoniae strains worldwide. J Glob Antimicrob Resist. 2020;22:519–526. doi:10.1016/j.jgar.2020.03.023
5. Wang Q, Ye MY, Hong C, Li ZP, Lin L. The mechanisms of resistance, epidemiological characteristics, and molecular evolution of carbapenem-resistant hypervirulent Klebsiella pneumoniae. Lab Med. 2025;56(4):323–335. doi:10.1093/labmed/lmae110
6. Rossolini GM, Stone GG. Assessment of the in vitro activity of ceftazidime/avibactam against a global collection of multidrug-resistant Klebsiella spp. from the INFORM surveillance programme (2015–2017). Int J Antimicrob Agents. 2020;56(3):106111. doi:10.1016/j.ijantimicag.2020.106111
7. Le Terrier C, Nordmann P, Poirel L. In vitro activity of aztreonam in combination with newly developed β-lactamase inhibitors against MDR Enterobacterales and Pseudomonas aeruginosa producing metallo-β-lactamases. J Antimicrob Chemother. 2022;78(1):101–107. doi:10.1093/jac/dkac360
8. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious Diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant Gram-negative infections. Clin Infect Dis. 2024. doi:10.1093/cid/ciae403
9. Pu D, Zhao J, Chang K, Zhuo X, Cao B. “Superbugs” with hypervirulence and carbapenem resistance in Klebsiella pneumoniae: the rise of such emerging nosocomial pathogens in China. Sci Bull. 2023;68(21):2658–2670. doi:10.1016/j.scib.2023.09.040
10. Huang Y, Li J, Wang Q, Tang K, Cai X, Li C. Detection of carbapenem-resistant hypervirulent Klebsiella pneumoniae ST11-K64 co-producing NDM-1 and KPC-2 in a tertiary hospital in Wuhan. J Hosp Infect. 2023;131:70–80. doi:10.1016/j.jhin.2022.09.014
11. Li J, Wu W, Wu M, et al. Clinical and molecular characteristics of patients with bloodstream infections caused by KPC and NDM co-producing carbapenem-resistant Klebsiella pneumoniae. Infect Drug Resist. 2024;17:1685–1697. doi:10.2147/idr.S455146
12. Zhang F, Liu X, Li Z, et al. Tracking international and regional dissemination of the KPC/NDM co-producing Klebsiella pneumoniae. Nat Commun. 2025;16(1):5574. doi:10.1038/s41467-025-60765-7
13. Gupta N, Boodman C, Prayag P, Manesh A, Kumar TP. Ceftazidime-avibactam and aztreonam combination for Carbapenem-resistant Enterobacterales bloodstream infections with presumed Metallo-β-lactamase production: a systematic review and meta-analysis. Expert Rev Anti Infect Ther. 2024;22(4):203–209. doi:10.1080/14787210.2024.2307912
14. Huespe IA, Huaier Arriazu EF, Sanchez M, et al. Mortality of metallo-β-lactamase-producing Enterobacterales bacteremias with combined ceftazidime-avibactam plus aztreonam vs. other active antibiotics: a multicenter target trial emulation. Lancet Reg Health Am. 2025;49:101175. doi:10.1016/j.lana.2025.101175
15. Karaiskos I, Galani I, Daikos GL, Giamarellou H. Breaking Through Resistance: a Comparative Review of New Beta-Lactamase Inhibitors (Avibactam, Vaborbactam, Relebactam) Against Multidrug-Resistant Superbugs. Antibiotics. 2025;14(5). doi:10.3390/antibiotics14050528
16. Assefa GM, Roberts JA, Aslan AT, Mohammed SA, Sime FB. A systematic review and individual bacterial species level meta-analysis of in vitro studies on the efficacy of ceftazidime/avibactam combined with other antimicrobials against carbapenem-resistant Gram-negative bacteria. J Antimicrob Chemother. 2025;80(2):334–346. doi:10.1093/jac/dkae451
17. Guzek A, Rybicki Z, Tomaszewski D, Mackiewicz K, Piechota W, Chciałowski A. Outcomes of 23 patients diagnosed with New Delhi metallo-beta-lactamase (NDM)-producing Klebsiella pneumoniae infection treated with ceftazidime/avibactam and aztreonam at a single center in Poland. Eur J Clin Microbiol Infect Dis. 2024;43(8):1579–1587. doi:10.1007/s10096-024-04859-y
18. Kwiatkowski P, Sienkiewicz M, Pruss A, et al. Antibacterial and anti-biofilm activities of essential oil compounds against New Delhi metallo-β-lactamase-1-producing uropathogenic Klebsiella pneumoniae strains. Antibiotics. 2022;11(2):147. doi:10.3390/antibiotics11020147
19. Mohamed H, Marusich E, Afanasev Y, Leonov S. Bacterial outer membrane permeability increase underlies the bactericidal effect of fatty acids from Hermetia illucens (black soldier fly) larvae fat against hypermucoviscous isolates of Klebsiella pneumoniae. Front Microbiol. 2022;13:844811. doi:10.3389/fmicb.2022.844811
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Phenotypic and Genetic Analysis of KPC-49, a KPC-2 Variant Conferring Resistance to Ceftazidime–Avibactam and Maintaining Resistance to Imipenem and Meropenem
Yu M, Wei Q, Song W, Yuan J
Infection and Drug Resistance 2023, 16:2477-2485
Published Date: 27 April 2023