Back to Journals » OncoTargets and Therapy » Volume 7
Colorectal cancer in Chinese patients: current and emerging treatment options
Received 29 May 2014
Accepted for publication 30 June 2014
Published 4 October 2014 Volume 2014:7 Pages 1817—1828
DOI https://doi.org/10.2147/OTT.S48409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Leung Li,1 Brigette BY Ma1,2
1Department of Clinical Oncology, Prince of Wales Hospital, 2State Key Laboratory of South China, Sir YK Pao Cancer Center, Hong Kong Cancer Institute, Sha Tin, Hong Kong
Abstract: Colorectal cancer is the second most common cancer in Hong Kong and its incidence is rising in economically developed Chinese cities, including Hong Kong and Shanghai. Several studies conducted in the People's Republic of China have characterized the unique molecular epidemiology of familial colorectal cancer syndromes and molecular biomarkers such as microsatellite instability and genetic mutations (eg, KRAS, NRAS, BRAF, PIK3CA, ERCC1) in Chinese populations. Interethnic differences in anticancer drug response and toxicity have been well described in many cancers, and this review examined the literature with regard to the tolerance of Chinese patients to commonly used chemotherapeutic regimens and targeted therapies for metastatic colorectal cancer. Studies on the pharmacogenomic differences in drug metabolizing and DNA repair enzymes between Chinese, North Asians, and Caucasian patients were also reviewed.
Keywords: Chinese, colorectal cancer, treatment
Epidemiology
According to the Global Cancer Statistics, the incidence of colorectal cancer (CRC) is rising in East Asia, probably as a result of multiple factors, including the adoption of a more Western style of high-fat and low-fiber diet and an increased prevalence of obesity and smoking.1 In the People’s Republic of China, although the age-standardized incidence of CRC was reported as 27/100,000 in men and 23/100,000 in women, which is significantly less than Western Europe and Australia, the incidence of CRC in the more economically developed cities such as Hong Kong and Shanghai has risen by 10% and 50%, respectively, between the 1980s and 2002.1 This is in contrast to the decreasing trend among Chinese emigrants living in the US between 1990–2008, where an annual percentage change of -1.9% in males and -0.7% in females has been reported.2 A rising trend has also been observed in many countries of the Asia–Pacific region.3 In Hong Kong, the mortality-to-incidence ratio for CRC was 41% in males and 37% in females from 2007–2011.4
However, a recent study has shown that the mortality of CRC in East Asian regions such as Japan, South Korea, Singapore, and Hong Kong has been declining in the last 40 years, especially in the younger age groups.4 Improvement in early diagnosis and in the management of CRC may be contributory factors.
In this review, the authors examined the literature regarding the epidemiology and molecular characteristics of CRC in the Chinese population, and addressed the question of whether Chinese patients may have different tolerance of chemotherapy and targeted therapy for the treatment of CRC compared with other ethnic groups. Such knowledge may be important to clinicians and researchers who are involved in the development of new drugs in Asia. Online search engines, including PubMed and Google, were searched using key terms, including “Chinese,” ‘colorectal cancer’, “China,” and “Hong Kong.” Articles published in English or Chinese from peer-reviewed journals were selected for this review.
Colorectal cancer screening in the Chinese
Various European trials have confirmed the efficacy of screening sigmoidoscopy for people aged 55–64 years in reducing the incidence of CRC,5–7 as well as in mortality and in an intention-to-treat analysis.5 Given the increasing incidence of CRC, there is rising support for population-based endoscopic screening in Hong Kong from the government and academic circles. A local review addressed some of the challenges of screening in Hong Kong because of the more frequent occurrence of nonpolypoid small CRC without preceding adenoma (de novo carcinoma) in Asia.8 These lesions tend to have deep invasion early and are more difficult to detect endoscopically and radiologically. Since 2008, investigators from the Chinese University of Hong Kong have initiated a Hong Kong-wide screening program. As of 2012, over 5,800 participants have undergone fecal occult blood tests and over 4,800 have had a colonoscopy. This program has identified precancerous polyps or bowel cancer in 1,512 people out of a total of 10,732 participants.9 Advanced CRC was identified in around 5.6% of all asymptomatic participants, and factors such as obesity, hypertension, and alcohol consumption were associated with higher incidence of advanced CRC at colonoscopy in this Chinese cohort. The Hong Kong government has recently announced a plan to initiate a pilot program of population-based CRC screening in 2014.10
Molecular genetics and pathology of colorectal cancer
Hereditary polyposis syndrome – prevalence in Chinese
The incidence of familial adenomatous polyposis in the People’s Republic of China is approximately 1.5/100,000 population and accounts for 0.94% of all CRCs in the People’s Republic of China. Malignant transformation usually occurs in the third or fourth decade.11 Familial adenomatous polyposis is caused by germline mutation in the APC gene and is inherited in an autosomal dominant manner. De novo germline mutations, sporadic somatic mutations in CRC, and various novel APC gene mutations have been well characterized in Chinese patients.11–16
Hereditary nonpolyposis colorectal cancer (HNPCC) and genetics
HNPCC (Lynch syndrome) results from germline mutations in one or more of the DNA mismatch repair (MMR) genes – MLH1, MSH2, MSH6, MLH3, and PMS1. These mutations pose a heightened risk of developing malignancy because the presence of a sporadic mutation in the remaining allele results in the inactivation of that gene product. The resultant defective DNA MMR protein commonly manifests as repetitive nucleotide sequences called microsatellites, which can be found in different regions of the DNA strands forming regions of microsatellite instability (MSI). MSI increases the vulnerability of DNA strands to breakage during DNA replication, which in turn increases the risk of gene mutations and rearrangements. Mutations in MLH1 and MSH2 account for the majority of HNPCCs.17 Affected subjects have an increased lifetime risk of developing colorectal, endometrial, and other cancers.
In the People’s Republic of China, HNPCC accounts for 2.2% of all CRCs if the Amsterdam criteria are applied.18 However, these criteria are not sensitive enough in reflecting the true prevalence of HNPCC in a country where national birth control policy has resulted in mostly small-sized families. Therefore, the National Hereditary CRC Network of the People’s Republic of China proposed Chinese HNPCC criteria that reduced the number of affected relatives required for establishing a diagnosis of HNPCC in order to better capture affected individuals and families.11 Furthermore, novel MMR gene mutations that were not found in international databases have been discovered from time to time in the People’s Republic of China and various Asian countries, suggesting a difference in genetic polymorphisms between Caucasian and Asians. This poses difficulty in establishing genetic diagnosis of HNPCC in the People’s Republic of China using Western data alone.19–26
MSI is a well-observed phenomenon in all CRCs and may arise from different mechanisms besides inherited mutations of the MMR genes. MSI can also result from sporadic germline mutations, somatic mutations, or epigenetic modifications of the MMR genes. Various Asian studies have investigated these diverse mechanisms of MSI in CRC in Asian patients.27–30 It is important to detect sporadic germline mutation in MMR genes because although affected subjects do not have significant family history, their offspring could inherit the condition in an autosomal dominant manner. The presence of MSI in CRC has been found to predict better survival following surgery in Asian and non-Asian populations.31–33 In a study conducted in Hong Kong,29 a high incidence of MSI-high tumors (>60%) were found in Chinese patients aged ≤31 years at diagnosis compared with 15% in patients aged ≥46 years. Germline mutations in MSH2, MLH1, or MSH6 could be found in >80% of those patients who were <31 years in this study.
RAS, BRAF, and PIK3CA genes
Activating mutations of KRAS, one of the isoforms of the RAS oncogenes, have been shown to predict a lack of response to EGFR antibodies in advanced CRC.34,35 Overall, around 30%–60% of CRCs harbor KRAS mutations, where 90% of all mutations are found in codons 12 and 13 of exon 2 and <5% are found in other locations such as codon 61, exon 3, and exon 4.36 On the contrary, the mutation G13D in exon 2 has been associated with better response to EGFR antibodies than other KRAS mutations, but the data are mixed.37,38 In addition to the exon 2 KRAS mutation, other mutations such as KRAS mutation exons 3–4 and NRAS mutation exons 2–4 have also emerged to be clinically relevant biomarkers of a lack of response to EGFR antibodies. For example, treating RAS-mutant tumor patients with panitumumab may even have a detrimental effect on survival as shown in the Panitumumab Randomized Trial in Combination With Chemotherapy for Metastatic CRC to Determine Efficacy (PRIME) study, where patients were randomized to first-line chemotherapy with or without panitumumab.39 Survival benefit was observed only in patients without RAS mutation.
To date, most Chinese studies have reported a similar prevalence of RAS mutations in CRC as Western studies, while the prevalence of rarer mutations such as non-exon 2 RAS mutations, BRAF, and PIK3CA mutations are less consistent. In the largest Chinese series to date, 966 CRC tumors were analyzed and the mutation rates of KRAS and BRAF were 38.8% and 4.4%, respectively. The most common KRAS mutations were found in codon 12 and 13 (G12D, G12V, and G13D), and the V600E type was the most common BRAF mutation.40 Despite some reports claiming a lower incidence of BRAF mutations in Chinese patients with CRC (<5%),41–43 the reported incidence rate is within the range of 4.7%–10% as reported in large Western series.44,45
Some new and uncommon non-exon 2 KRAS mutations that are found in codons 45, 69, and 80 have also been identified in Chinese patients with CRC, but their clinical significance has yet to be defined.46 BRAF mutation has been implicated as a prognostic marker in stage II/III and metastatic CRC in Western studies.45,47 Some Chinese studies from Mainland China and Taiwan have also reported similar findings.43 Table 1 summarizes the findings of various Chinese studies on RAS mutations.40–43,46,48–55
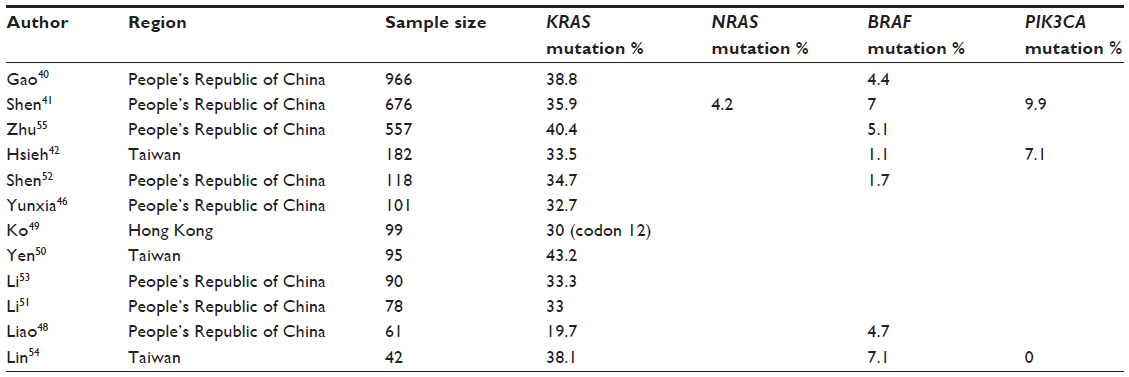 | Table 1 Chinese studies focusing on RAS, BRAF and PIK3CA mutations |
Tolerability to systemic therapy for colorectal cancer in Asians
Fluoropyrimidines and dihydropyrimidine dehydrogenase (DPD) polymorphisms
DPD is a key catabolic enzyme of 5-fluorouracil (5FU). It is encoded by the DPYD gene and its enzymatic activity is affected by genetic polymorphism. DPD deficiency is a syndrome with reduced DPD enzymatic activity that may cause excessive toxicity after treatment with fluoropyrimidine – typically severe diarrhea, mucositis, and pancytopenia.
The more common allelic variants that have been associated with the DPD deficiency syndrome are *2A, *9B, and *13.56 Differences in the allelic frequency and DPD activity between Asians and Caucasians have been previously reported.57–60 This may partially explain the observed differences between Asians and Caucasians in the tolerance of fluoropyrimidines.
Toxicities such as diarrhea, neutropenia, and hand–foot syndrome seem to be more common in Caucasians compared with Asians.61–63 There is a paucity of studies in Chinese populations. In one study of 142 patients with CRC, the prevalence of DPYD mutations was 2.8%. No correlation between the presence of DPYD mutations and toxicity to 5FU was found.64
Capecitabine-related toxicity in Chinese
In a US study of 1,189 patients with CRC who received adjuvant capecitabine or 5FU, Haller et al reported that East Asians are less likely to develop serious adverse events, including hand–foot syndrome, from fluoropyrimidines than other populations.61 The incidence of hand–foot syndrome of any grade or grade III in severity in Hong Kong Chinese receiving capecitabine in the palliative or adjuvant setting has been reported to be between 32%–49% and 1%–3%, respectively.65,66
S-1 (TS-1)
S-1 is an oral fluoropyrimidine, consisting of tegafur (ftorafur), gimeracil (5-chloro-2,4-dihydroxypyridine), and potassium oxonate at a molar ratio of 1:0.4:1. Tegafur is a prodrug of 5FU, gimeracil is an inhibitor of DPD, and potassium oxonate inhibits phosphorylation of intestinal 5FU and may contribute to treatment-related diarrhea.
The pharmacokinetics and pharmacodynamics of S-1 were compared in Asians and Caucasians by Chuah et al.62 Drug exposure for tegafur was significantly higher in Asians, while that for fluoro-b-alanine (a 5FU metabolite implicated in various toxicities) was significantly higher in Caucasians, but there was no difference in exposure to 5FU. Grade III/IV gastrointestinal toxicities occurred in 21% of Caucasians and 0% of Asians. This result is in line with the general trend of better tolerance of fluoropyrimidines amongst Asians compared with Caucasians. The majority of Phase II/III studies using S-1 are from Japan and Korea. Various dosing schedules of S-1 have been evaluated and the incidence of grade III/IV diarrhea in S-1 is generally around 10% when used as monotherapy, and around 17% when combined with irinotecan. Grade III/IV neutropenia is uncommon with single agent S-1, but the incidence has been reported to be 9%–53% when combined with irinotecan. Treatment-related mortality is low, with one report suggesting a 4% incidence rate in a study of 70–85 year olds.67
Irinotecan and pharmacogenomics
Genetic polymorphisms in the enzyme UGT1A1, such as the UGT1A1*28 allele, results in reduced UGT enzymatic activity causing excessive irinotecan toxicities – typically severe neutropenia, while severe diarrhea is less common in Chinese subjects.68
Patients who are homozygous for the UGT1A1*28 allele ([TA]7/7) are at increased risk of neutropenia; thus, the initial dose should be reduced. Heterozygous carriers of the *28 allele may have an increased risk of toxicity as well, but most patients tolerated normal starting doses. Genetic variation at the *28 allele is more commonly found in Caucasians compared with Asians. It has been estimated that homozygosity of the *28 allele can be found in around 10% of the North American population, while 40% of the population could be heterozygotes.69 A series reported the rate of *28 allelic frequency in the Chinese to be around 10.5%.70 In a multiethnic study that included 39 Chinese subjects, the incidence of homozygosity of UGT1A1 ([TA]7/7) was found to be 8% in Chinese, 5% in Asians, and 13% in Caucasians.71
The observed differences in toxicities and underlying genetic constitution between Asians and Caucasians have prompted multinational collaborative research into pharmacogenomic variations between the different populations. A study has identified many differences in the frequencies of several key functional polymorphisms of genes encoding enzymes such as UGT1A1, cytochrome P450s, N-acetyltransferase, glutathione S-transferase (GSTM1/GSTT1), and human leukocyte antigens between East Asians and Europeans. Interestingly, the frequencies of these genetic polymorphisms are quite similar amongst East Asians such as the Chinese, Japanese, and Koreans.72
Oxaliplatin
Infusional leucovorin/5FU/oxaliplatin (FOLFOX4) has been found to be well tolerated in Asians in a meta-analysis that compared the tolerability of FOLFOX4 in Asian and Western populations.73 Toxicity profiles were largely similar with the exception of grade III neurosensory toxicity and diarrhea, which appeared to be significantly lower in Asian than in Western populations. Severe anaphylactic reaction to oxaliplatin was reported to be 1.9% in a Taiwanese series of 412 Chinese patients, which is comparable to what has been generally reported for other non-Chinese populations.74
ERCC1 gene polymorphism has been extensively investigated as a potential predictive biomarker for oxaliplatin and platinum agents in a variety of cancers. Protein products of these genes are responsible for nucleotide excision repair of damaged DNA, especially those caused by platinum DNA adducts, and thus are implicated in overcoming the anticancer effect of platinum chemotherapy. Two Chinese studies have reported that the ERCC1 codon 118C → T polymorphism was associated with higher expression of ERCC1 protein and lower response rate and survival in Chinese patients who received FOLFOX4 for CRC.75,76 Another study reported that certain ERCC1 and XRCC genotypes may be associated with better survival.77 In a retrospective series of 180 Chinese patients with stage III CRC who received adjuvant FOLFOX4, ERCC1 overexpression was found to be an independent predictor of poorer disease-free survival and overall survival (OS).78
Antiangiogenesis agents – bevacizumab, aflibercept, and regorafenib
Results from the Phase III Avastin® in Combination With Chemotherapy in Chinese Patients with Metastatic CRC (ARTIST) and S-1/Oxaliplatin (SOX)/Bevacizumab versus FOLFOX/Bevacizumab in Treating Patients With Metastatic CRC (SOFT) trials have provided data regarding the tolerance of bevacizumab among Asians.79,80 The ARTIST trial evaluated the benefit of first-line bevacizumab plus irinotecan-based chemotherapy over chemotherapy alone in metastatic CRC, while the SOFT trial examined whether SOX/bevacizumab was noninferior to modified FOLFOX6/bevacizumab as first-line treatment of metastatic CRC. From these trials, the incidence of grade III/IV bevacizumab-related toxicities was comparable to Western Phase III studies. To date, there is no published data on the tolerability of Chinese patients to aflibercept and regorafenib. As shall be discussed in the subsequent section of this review, Phase III studies of these two agents are ongoing in the People’s Republic of China and Asian–Pacific regions.
EGFR antibodies – cetuximab and panitumumab
In Hong Kong and some major oncology centers in the People’s Republic of China, the KRAS mutation is now routinely determined in patients prior to starting EGFR antibody treatment for metastatic CRC. In the largest study involving Chinese (ie, Mainland, the People’s Republic of China, and Taiwan) and Asian–Pacific patients to date, the Asian Pacific Erbitux in Colorectal cancer (APEC) study was an open-labeled Phase II study of 289 patients with KRAS wild-type metastatic CRC who were treated with cetuximab and chemotherapy of the physician’s choice (FOLFOX or irinotecan/infused 5FU/leucovorin [FOLFIRI]).81 The incidence of cetuximab-related toxicities was comparable to that reported in Western Phase III studies.
Treatment options in adjuvant therapy
A population-based study in the US has shown that East Asian Americans with colon cancer had significantly better prognosis than White or African Americans, suggesting a racial disparity in the treatment outcome for CRC.82 However, there is a lack of population-based studies conducted in the People’s Republic of China. In a retrospective analysis of 100 Chinese patients in Hong Kong who received adjuvant capecitabine/oxaliplatin (XELOX) for stage III colon and upper rectal cancers, the 4-year disease-free survival was found to be 81% and 67% for colon and rectal cancers, respectively, while the 5-year OS for the whole group was 84%.66 In Hong Kong, most patients have ready access to Western style oncological care since public health care is heavily subsidized by the government. Chemotherapeutic agents such as capecitabine and oxaliplatin are categorized as “special drugs” by the public Hospital Authority and are thus offered free of charge for the treatment of stage III/IV CRC. Therefore, there is a preference for prescribing oral 5FU as a chemotherapeutic backbone over an infusional regimen such as FOLFOX (which requires central venous access and ambulatory infusion pump) amongst oncologists working in the public sector. In the US and Japan, other oral drugs of 5FU such as tegafur/uracil and S-1 have been evaluated in the Phase III adjuvant setting with positive results.83,84 However, these agents are not widely available for the treatment of CRC in Hong Kong at present.
Treatment options for metastatic disease
FOLFOX, XELOX, and FOLFIRI are commonly used chemotherapeutic regimens for unresectable metastatic CRC.85–89 Before targeted therapy became available, FOLFOX and FOLFIRI were found to yield similar results in terms of progression-free survival (PFS) and OS when used in the first-line setting.90 Therefore, exposure to all three cytotoxic agents (ie, 5FU, oxaliplatin, and irinotecan) – rather than the sequence – exerts more impact on survival.91 The use of oral 5FU as a backbone has also been confirmed in studies that showed that XELOX is noninferior to FOLFOX in both first-line92–94 and second-line95 settings.
Oral 5FU – S-1 and tegafur/uracil
To date, many studies have been published on the use of S-1 and tegafur/uracil in Korean and Japanese patients, but few in Chinese patients with metastatic CRC. The SOX regimen has been shown to be noninferior to CAPOX in a multicenter, open-label, randomized controlled Phase III trial in Korea,96 where 340 patients were randomized to SOX and XELOX. The median PFS was 8.5 months in the SOX group and 6.7 months in the XELOX group, a result which met the noninferiority criteria. Overall response rate was significantly higher in the SOX arm (47%) than in the XELOX arm (36%). Although hematological toxicity and hand–foot syndrome were lower in the SOX arm, grade III/IV neutropenia and thrombocytopenia were significantly higher. The addition of bevacizumab to the SOX regimen has been shown to be noninferior in terms of PFS to modified FOLFOX6/bevacizumab in the first-line treatment of metastatic CRC.80 S-1 combined with irinotecan was found to be noninferior to FOLFIRI in a Japanese randomized Phase II/III trial.97 The rate of grade III/IV neutropenia was significantly lower in the S-1/irinotecan arm (36%) compared with the FOLFIRI arm (52%), but diarrhea was significantly worse (21% versus 4.7%, respectively).
Oxaliplatin- and irinotecan-based regimens
Besides the ARTIST study,79 the majority of studies published to date in Chinese patients are single-arm Phase II studies. There is no definite evidence from the literature that Chinese patients respond differently to FOLFOX and FOLFIRI than other ethnic groups.73,98–101
In a relatively small survey of a few Asian centers conducted in 2010 on the patterns of use of chemotherapeutic regimens for metastatic CRC,102 FOLFOX was found to be the most popular first-line regimen in Taiwan, while FOLFOX and FOLFIRI were equally popular in Hong Kong. However, this pattern has changed in Hong Kong, where the costs of irinotecan, oxaliplatin, and capecitabine are now reimbursed by the government for the treatment of metastatic CRC in public hospitals. Therefore, capecitabine-based regimens such as XELOX and irinotecan/capecitabine (XELIRI) are often the preferred regimens in Hong Kong given its convenient administration in the outpatient setting.
Antiangiogenesis agents – bevacizumab, aflibercept, and regorafenib
Bevacizumab in combination with first-line chemotherapy (5FU/leucovorin, capecitabine, FOLFIRI, IFL, FOLFOX, XELOX) improved response rate and PFS when compared with chemotherapy alone.103–107 OS benefit was demonstrated when bevacizumab was added to IFL, FOLFIRI, or 5FU/leucovorin. In the People’s Republic of China, the multicenter, randomized, open-label Phase III ARTIST trial examined the benefit of first-line bevacizumab plus irinotecan-based chemotherapy over chemotherapy alone in 214 patients.79 The addition of bevacizumab significantly increased response rate from 17% to 35%, prolonged median PFS from 4.2 months to 8.3 months, and increased OS from 13.4 months to 18.7 months. In a report from Taiwan where bevacizumab is reimbursed by the government for the first-line treatment of metastatic CRC when combined with irinotecan-based chemotherapy, the efficacy and toxicity of bevacizumab-based chemotherapy seemed to be comparable with the Western studies.108
In another study, Claret et al investigated whether there is any ethnic difference in some new metrics for correlating tumor size response and OS in Western and Chinese patients who underwent bevacizumab treatment and chemotherapy for metastatic CRC.109 They found that the time to tumor growth was the best metric to predict OS in bevacizumab-treated patients irrespective of their ethnicity. This could be a relevant factor when designing and interpreting the results of clinical trials of bevacizumab in metastatic CRC. A randomized Phase III study of first-line bevacizumab in combination with FOLFIRI versus FOLFIRI alone in Chinese patients with metastatic CRC has completed enrollment and its result is pending (NCT00642577).110
The randomized Phase III Aflibercept Versus Placebo in Combination With Irinotecan and 5FU in the Treatment of Metastatic CRC After Failure of an Oxaliplatin-based Regimen (VELOUR) trial demonstrated the addition of aflibercept to second-line FOLFIRI increased response rate, PFS, and OS when compared to FOLFIRI alone.111,112 A multinational randomized double-blind, placebo-controlled Phase III study named Aflibercept Versus Placebo With FOLFIRI in Patients With Metastatic CRC Previously Treated With an Oxaliplatin Chemotherapy (AFLAME) – with a similar design to the pivotal VELOUR study – is currently ongoing in multiple centers from the People’s Republic of China, Hong Kong, Taiwan, and other East Asian countries.113 The primary endpoint is PFS and this trial has just completed accrual (NCT01661270).
The registration Phase III study named the Patients With Metastatic CRC Treated With Regorafenib or Placebo After Failure of Standard Therapy (CORRECT) trial114 has shown that the multitargeted VEGF receptor regorafenib can modestly improve PFS and OS when compared to best supportive care in patients who had exhausted all systemic options for metastatic CRC. A registration Phase III study named Asian Subjects With Metastatic CRC Treated With Regorafenib or Placebo After Failure of Standard Therapy (CONCUR) has just completed accrual in the People’s Republic of China, Hong Kong, and other Asian–Pacific centers. This study compared regorafenib with best supportive care in patients with metastatic CRC who had been previously treated with at least two lines of chemotherapy (NCT01584830).115 The primary endpoint is OS and the result will be available in 2014.
EGFR antibodies – cetuximab and panitumumab
In a survey of oncology centers from Asia, Europe, and Latin America conducted just around the time when the US Food and Drug Administration updated the labels of cetuximab and panitumumab on the mandatory testing of KRAS mutation in 2009, <50% of all sites surveyed in the People’s Republic of China and some Asian centers (Philippines, Singapore, Hong Kong, and Korea) would perform this analysis before starting EGFR antibodies.116 Of the Chinese sites that participated (the People’s Republic of China and Hong Kong) in another Asian-based survey, cetuximab was used mainly in the second- to third-line setting since panitumumab was not available at the time, while bevacizumab was used less commonly in the first-line setting compared to Western countries.102 These studies need to be interpreted with caution since only a few centers were invited and thus may not be representative of the standard of practice across the People’s Republic of China. Nowadays, in the public hospitals of Hong Kong, RAS (KRAS and NRAS) mutation testing is mandatory in every patient prior to starting EGFR antibodies for metastatic CRC.
In the APEC study as described above,81 the response rates of FOLFOX/cetuximab (n=188, 61.2%) and FOLFIRI/cetuximab (n=101, 54.5%) were comparable to that reported in other randomized studies conducted in the West, such as the Oxaliplatin and Cetuximab in First-line Treatment of Metastatic CRC (OPUS; FOLFOX/cetuximab response rate 57%) and Cetuximab Combined With Irinotecan in First-line Therapy for Metastatic CRC (CRYSTAL; FOLFIRI/cetuximab response rate 57.3%) studies.116–120 There was no difference in PFS or OS, although the study was not powered to detect a survival difference. The R0 resection rate for liver metastases was higher (11.7%) in the FOLFOX/cetuximab arm than in the FOLFIRI/cetuximab arm (6.9%). It is interesting to note that the Asian investigators of the APEC study preferred to use oxaliplatin as a partner with cetuximab in the first-line setting in this study. Furthermore, this study did not suggest that the combination of cetuximab and oxaliplatin was significantly inferior to a partnership with irinotecan, a controversial observation that has been supported by some Phase III studies.121,122 Several Phase III trials evaluating first- and second-line cetuximab in combination with chemotherapy in Chinese patients with metastatic CRC are now ongoing (NCT01228734 and NCT01550055).
Limited unresectable liver or lung metastases
Resection of isolated colorectal liver/lung metastases could produce long-term relapse-free survival in up to 25%–50% of patients.123 Therefore, resection is recommended for patients with resectable liver or limited lung metastasis. However, for those with unresectable metastases, conversion therapy using a regimen with high response rates (eg, bevacizumab or cetuximab/panitumumab in combination with chemotherapy) may render the disease resectable. The optimal choice of therapy depends on the tumor and patient characteristics, including RAS mutational status. In order to definitely address the question of whether the addition of EGFR antibodies to chemotherapy improves survival for patients with KRAS wild-type metastatic CRC, a randomized Phase III trial in 138 Chinese patients with KRAS wild-type CRC with synchronous unresectable liver metastasis who received treatment at a single institution in the People’s Republic of China has been published.124 Overall response rate significantly favored the cetuximab arm over the chemotherapy alone arm (57% versus 29%, respectively), and the complete resection rate also significantly increased (26% versus 7%, respectively). This study was the first to demonstrate that the addition of cetuximab prolonged the median OS (31 months versus 21 months for chemotherapy alone). As expected, patients in the cetuximab arm had a significantly higher rate of grade III/IV acneiform rash (13%), while the incidence of allergic reaction in the cetuximab arm was 2.9%. Among patients receiving cetuximab, the presence of acneiform rash was a predictive factor for higher overall response rate, but not survival. A Chinese guideline has been published on a comprehensive multidisciplinary approach to the evaluation and treatment for liver metastasis from CRC.125
Traditional Chinese medicine
Traditional Chinese herbal medicine is frequently utilized in the Chinese community and has been investigated in a randomized manner in various studies. Although a meta-analysis suggested that Chinese herbal medicine may have a positive effect on survival, tumor response, and performance status, the studies were in general of low quality, making it difficult to draw conclusions.126 This calls for high-quality randomized, double-blind, placebo-controlled trials to evaluate the benefit of Chinese herbal medicine in CRC patients.
Practice in the People’s Republic of China and Hong Kong
Common practice in Asian countries was discussed in the CRC Working Group report in the 30th Asia–Pacific Cancer Conference. FOLFOX was the most popular first-line regimen. Cetuximab was mainly used as a second- or third-line regimen with reference to KRAS status. Oxaliplatin-based adjuvant chemotherapy is commonly used for stage III disease, whereas the clinical practice for stage II disease varied.102 A guideline has been published on the management of colon cancer in the adjuvant and metastatic settings as well as a screening strategy for the Asia–Pacific region; it also summarizes the availability of national funding for chemotherapeutic and targeted agents for CRC in various Asian countries.3 There are few published guidelines within the People’s Republic of China, but some consensus statements have been published. These are not national guidelines but are from selected academic groups; therefore, they are not universally accepted. Anecdotally, the European Society for Medical Oncology and National Comprehensive Cancer Network guidelines are popularly used in some centers across Hong Kong.127
Conclusion
CRC is fast becoming the most common cancer in Hong Kong and its incidence is also rising in urbanized regions in the People’s Republic of China. This review has highlighted the differences between Chinese and other populations, such as Caucasians, in terms of the prevalence of genetic polymorphisms involved in hereditary cancer syndromes and the metabolism of fluoropyrimidines and irinotecan. The current literature suggests that Chinese patients have better tolerance to oral 5FU than Caucasians, but whether this extends to efficacy remains unclear. Disparities in access to medical health care and government subsidies for anticancer drugs may also influence the treatment outcome for Chinese patients with CRC. The multidisciplinary model of oncological care has been practiced in Hong Kong for decades and has been adopted in many major oncology centers in the People’s Republic of China.
Disclosure
Dr Ma has received research grant from Merck Serono, speakers honorarium from Roche, and consultancy for Bayer and Sanofi. Dr Li has no conflicts of interest to report.
References
Center MM, Jemal A, Ward E. International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomarkers Prev. 2009;18(6):1688–1694. | |
Gomez SL, Noone AM, Lichtensztajn DY, et al. Cancer incidence trends among Asian American populations in the United States,1990–2008. J Natl Cancer Inst. 2013;105(15):1096–1110. | |
Ku G, Tan IB, Yau T, et al. Management of colon cancer: resource-stratified guidelines from the Asian Oncology Summit 2012. Lancet Oncol. 2012;13(11):e470–e481. | |
Hong Kong Cancer Registry. Hong Kong: Hospital Authority; 2014. Available from: http://www3.ha.org.hk/cancereg/. Accessed August 26, 2014. | |
Atkin WS, Edwards R, Kralj-Hans I, et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicenter randomized controlled trial. Lancet. 2010;375(9726):1624–1633. | |
Segnan N, Armaroli P, Bonelli L, et al. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the Italian randomized controlled trial – SCORE. J Natl Cancer Inst. 2011; 103(17):1310–1322. | |
Hoff G, Grotmol T, Skovlund E, et al. Risk of colorectal cancer 7 years after flexible sigmoidoscopy screening: randomized controlled trial. BMJ. 2009;338:b1846. | |
Sung JJ, Lau JY, Goh KL, Leung WK. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol. 2005;6(11):871–876. | |
CUHK welcomes government’s proposal on bowel cancer screening [press release]. Sha Tin: Hong Kong: Chinese University of Hong Kong; 2014 [January 20]. Available from: http://www.cpr.cuhk.edu.hk/en/press_detail.php?id=1739. Accessed July 31, 2014. | |
Wong MC, Lam TY, Tsoi KK, et al. Predictors of advanced colorectal neoplasia for colorectal cancer screening. Am J Prev Med. 2014;46(5):433–439. | |
Shu Z, Yanqin H, Ying Y. Hereditary colorectal cancer in China. Hered Cancer Clin Pract. 2005;3(4):155–164. | |
Liu X, Shan X, Friedl W, et al. May the APC gene somatic mutations in tumor tissues influence the clinical features of Chinese sporadic colorectal cancers? Acta Oncol. 2007;46(6):757–762. | |
Fang Z, Xiong Y, Li J, et al. Detection of APC gene deletions in colorectal malignancies using quantitative PCR in a Chinese population. Pathol Oncol Res. 2011;17(3):657–661. | |
Huang X, Wang Y, Yu T, et al. Association study of APC polymorphisms with colorectal cancer in Han Chinese. Clin Biochem. 2012;45(18):1669–1672. | |
Liu XR, Shan XN, Friedl W, et al. [Detection of germline mutations in the APC gene with the protein truncation test]. Yi Chuan Xue Bao. 2005;32(9):903–908. Chinese. | |
Gan YB, Zheng S, Cai XH. [Detection of a gene mutation in familial adenomatous polyposis families by PCR-RFLP method]. Zhonghua Yi Xue Za Zhi. 1994;74(6):352–354. Chinese. | |
Palomaki GE, McClain MR, Melillo S, Hampel HL, Thibodeau SN. EGAPP supplementary evidence review: DNA testing strategies aimed at reducing morbidity and mortality from Lynch syndrome. Genet Med. 2009;11(1):42–65. | |
Zhang YZ, Sheng JQ, Li SR, Zhang H. Clinical phenotype and prevalence of hereditary nonpolyposis colorectal cancer syndrome in Chinese population. World J Gastroenterol. 2005;11(10):1481–1488. | |
Ho JW, Yuen ST, Chung LP, et al. Distinct clinical features associated with microsatellite instability in colorectal cancers of young patients. Int J Cancer. 2000;89(4):356–360. | |
Chan TL, Yuen ST, Ho JW, et al. A novel germline 1.8-kb deletion of hMLH1 mimicking alternative splicing: a founder mutation in the Chinese population. Oncogene. 2001;20(23):2976–2981. | |
Wang XL, Yuan Y, Zhang SZ, et al. Clinical and genetic characteristics of Chinese hereditary nonpolyposis colorectal cancer families. World J Gastroenterol. 2006;12(25):4074–4077. | |
Shen XS, Zhao B, Wang ZJ. Clinical features and hMSH2/hMLH1 germ-line mutations in Chinese patients with hereditary nonpolyposis colorectal cancer. Chin Med J (Engl). 2008;121(14):1265–1268. | |
Chan TL, Chan YW, Ho JW, et al. MSH2 c.1452-1455delAATG is a founder mutation and an important cause of hereditary nonpolyposis colorectal cancer in the southern Chinese population. Am J Hum Genet. 2004;74(5):1035–1042. | |
Cai Q, Sun MH, Lu HF, et al. Clinicopathological and molecular genetic analysis of four typical Chinese HNPCC families. World J Gastroenterol. 2001;7(6):805–810. | |
Luo DC, Cai Q, Sun MH, et al. Clinicopathological and molecular genetic analysis of HNPCC in China. World J Gastroenterol. 2005; 11(11):1673–1679. | |
Sheng JQ, Fu L, Sun ZQ, et al. Mismatch repair gene mutations in Chinese HNPCC patients. Cytogenet Genome Res. 2008;122(1):22–27. | |
Ko JM, Cheung MH, Kwan MW, et al. Genomic instability and alterations in Apc, Mcc, and Dcc in Hong Kong patients with colorectal carcinoma. Int J Cancer. 1999;84(4):404–409. | |
Jin HY, Liu X, Li VK, et al. Detection of mismatch repair gene germline mutation carrier among Chinese population with colorectal cancer. BMC Cancer. 2008;8:44. | |
Chan TL, Yuen ST, Chung LP, et al. Frequent microsatellite instability and mismatch repair gene mutations in young Chinese patients with colorectal cancer. J Natl Cancer Inst. 1999;91(14):1221–1226. | |
Yuen ST, Chan TL, Ho JW, et al. Germline, somatic, and epigenetic events underlying mismatch repair deficiency in colorectal and HNPCC-related cancers. Oncogene. 2002;21(49):7585–7592. | |
Watanabe T, Wu TT, Catalano PJ, et al. Molecular predictors of survival after adjuvant chemotherapy for colon cancer. N Engl J Med. 2001;344(16):1196–1206. | |
Kohonen-Corish MR, Daniel JJ, Chan C, et al. Low microsatellite instability is associated with poor prognosis in stage C colon cancer. J Clin Oncol. 2005;23(10):2318–2324. | |
Lanza G, Gafa R, Santini A, Maestri I, Guerzoni L, Cavazzini L. Immunohistochemical test for MLH1 and MSH2 expression predicts clinical outcome in stage II and III colorectal cancer patients. J Clin Oncol. 2006;24(15):2359–2367. | |
Jonker DJ, O’Callaghan CJ, Karapetis CS, et al. Cetuximab for the treatment of colorectal cancer. N Engl J Med. 2007;357(20):2040–2048. | |
Karapetis CS, Khambata-Ford S, Jonker DJ, et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N Engl J Med. 2008;359(17):1757–1765. | |
Janakiraman M, Vakiani E, Zeng Z, et al. Genomic and biological characterization of exon 4 KRAS mutations in human cancer. Cancer Res. 2010;70(14):5901–5911. | |
Gajate P, Sastre J, Bando I, et al. Influence of KRAS p.G13D mutation in patients with metastatic colorectal cancer treated with cetuximab. Clin Colorectal Cancer. 2012;11(4):291–296. | |
Tejpar S, Celik I, Schlichting M, Sartorius U, Bokemeyer C, Van Cutsem E. Association of KRAS G13D tumor mutations with outcome in patients with metastatic colorectal cancer treated with first-line chemotherapy with or without cetuximab. J Clin Oncol. 2012;30(29):3570–3577. | |
Douillard JY, Oliner KS, Siena S, et al. Panitumumab–FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med. 2013;369(11):1023–1034. | |
Gao J, Sun ZW, Li YY, Shen L. [Mutations of KRAS and BRAF in Chinese patients with colorectal carcinoma: analyses of 966 cases]. Zhonghua Bing Li Xue Za Zhi. 2012;41(9):579–583. Chinese. | |
Shen H, Yuan Y, Hu HG, et al. Clinical significance of K-ras and BRAF mutations in Chinese colorectal cancer patients. World J Gastroenterol. 2011;17(6):809–816. | |
Hsieh LL, Er TK, Chen CC, Hseih JS, Chang JG, Liu TC. Characteristics and prevalence of KRAS, BRAF, and PIK3CA mutations in colorectal cancer by high-resolution melting analysis in Taiwanese population. Clin Chim Acta. 2012;413(19–20):1605–1611. | |
Liou JM, Wu MS, Shun CT, et al. Mutations in BRAF correlate with poor survival of colorectal cancers in Chinese population. Int J Colorectal Dis. 2011;26(11):1387–1395. | |
De Roock W, Claes B, Bernasconi D, et al. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol. 2010;11(8):753–762. | |
Richman SD, Seymour MT, Chambers P, et al. KRAS and BRAF mutations in advanced colorectal cancer are associated with poor prognosis but do not preclude benefit from oxaliplatin or irinotecan: results from the MRC FOCUS trial. J Clin Oncol. 2009;27(35):5931–5937. | |
Yunxia Z, Jun C, Guanshan Z, Yachao L, Xueke Z, Jin L. Mutations in epidermal growth factor receptor and K-ras in Chinese patients with colorectal cancer. BMC Med Genet. 2010;11:34. | |
Roth AD, Tejpar S, Delorenzi M, et al. Prognostic role of KRAS and BRAF in stage II and III resected colon cancer: results of the translational study on the PETACC-3, EORTC 40993, SAKK 60-00 trial. J Clin Oncol. 2010;28(3):466–474. | |
Liao W, Liao Y, Zhou JX, et al. Gene mutations in epidermal growth factor receptor signaling network and their association with survival in Chinese patients with metastatic colorectal cancers. Anat Rec (Hoboken). 2010;293(9):1506–1511. | |
Ko JM, Cheung MH, Wong CM, et al. Ki-ras codon 12 point mutational activation in Hong Kong colorectal carcinoma patients. Cancer Lett. 1998;134(2):169–176. | |
Yen LC, Uen YH, Wu DC, et al. Activating KRAS mutations and overexpression of epidermal growth factor receptor as independent predictors in metastatic colorectal cancer patients treated with cetuximab. Ann Surg. 2010;251(2):254–260. | |
Li Z, Chen Y, Wang D, Wang G, He L, Suo J. Detection of KRAS mutations and their associations with clinicopathological features and survival in Chinese colorectal cancer patients. J Int Med Res. 2012;40(4):1589–1598. | |
Shen Y, Wang J, Han X, et al. Effectors of epidermal growth factor receptor pathway: the genetic profiling of KRAS, BRAF, PIK3CA, NRAS mutations in colorectal cancer characteristics and personalized medicine. PLoS One. 2013;8(12):e81628. | |
Li FH, Shen L, Li ZH, et al. Impact of KRAS mutation and PTEN expression on cetuximab-treated colorectal cancer. World J Gastroenterol. 2010;16(46):5881–5888. | |
Lin JK, Lin AJ, Lin CC, et al. The status of EGFR-associated genes could predict the outcome and tumor response of chemo-refractory metastatic colorectal patients using cetuximab and chemotherapy. J Surg Oncol. 2011;104(6):661–666. | |
Zhu XL, Cai X, Zhang L, et al. [KRAS and BRAF gene mutations in correlation with clinicopathologic features of colorectal carcinoma in Chinese]. Zhonghua Bing Li Xue Za Zhi. 2012;41(9):584–589. Chinese. | |
Morel A, Boisdron-Celle M, Fey L, et al. Clinical relevance of different dihydropyrimidine dehydrogenase gene single nucleotide polymorphisms on 5-fluorouracil tolerance. Mol Cancer Ther. 2006;5(11):2895–2904. | |
Mattison LK, Fourie J, Desmond RA, Modak A, Saif MW, Diasio RB. Increased prevalence of dihydropyrimidine dehydrogenase deficiency in African-Americans compared with Caucasians. Clin Cancer Res. 2006;12(18):5491–5495. | |
Shin JG, Cheong HS, Kim JY, et al. Screening of dihydropyrimidine dehydrogenase genetic variants by direct sequencing in different ethnic groups. J Korean Med Sci. 2013;28(8):1129–1133. | |
Sohn DR, Cho MS, Chung PJ. Dihydropyrimidine dehydrogenase activity in a Korean population. Ther Drug Monit. 1999;21(2):152–154. | |
Maekawa K, Saeki M, Saito Y, et al. Genetic variations and haplotype structures of the DPYD gene encoding dihydropyrimidine dehydrogenase in Japanese and their ethnic differences. J Hum Genet. 2007;52(10):804–819. | |
Haller DG, Cassidy J, Clarke SJ, et al. Potential regional differences for the tolerability profiles of fluoropyrimidines. J Clin Oncol. 2008;26(13):2118–2123. | |
Chuah B, Goh BC, Lee SC, et al. Comparison of the pharmacokinetics and pharmacodynamics of S-1 between Caucasian and East Asian patients. Cancer Sci. 2011;102(2):478–483. | |
Shirao K, Hoff PM, Ohtsu A, et al. Comparison of the efficacy, toxicity, and pharmacokinetics of a uracil/tegafur (UFT) plus oral leucovorin (LV) regimen between Japanese and American patients with advanced colorectal cancer: joint United States and Japan study of UFT/LV. J Clin Oncol. 2004;22(17):3466–3474. | |
He YF, Wei W, Zhang X, et al. Analysis of the DPYD gene implicated in 5-fluorouracil catabolism in Chinese cancer patients. J Clin Pharm Ther. 2008;33(3):307–314. | |
Ma BB, Chan SL, Ho WM, et al. Intermittent versus continuous erlotinib with concomitant modified “XELOX” (q3W) in first-line treatment of metastatic colorectal cancer: correlation with serum amphiregulin and transforming growth factor alpha. Cancer. 2013;119(23):4145–4153. | |
Chiu J, Tang V, Leung R, et al. Efficacy and tolerability of adjuvant oral capecitabine plus intravenous oxaliplatin (XELOX) in Asian patients with colorectal cancer: 4-year analysis. Asian Pac J Cancer Prev. 2013;14(11):6585–6590. | |
Shin SJ, Jeong JH, Park YS, et al. Phase II trial of S-1 monotherapy in elderly or frail patients with metastatic colorectal cancer. Invest New Drugs. 2011;29(5):1073–1080. | |
Gao J, Zhou J, Li Y, Lu M, Jia R, Shen L. UGT1A1 6/28 polymorphisms could predict irinotecan-induced severe neutropenia not diarrhea in Chinese colorectal cancer patients. Med Oncol. 2013;30(3):604. | |
Innocenti F, Undevia SD, Iyer L, et al. Genetic variants in the UDP- glucuronosyltransferase 1A1 gene predict the risk of severe neutropenia of irinotecan. J Clin Oncol. 2004;22(8):1382–1388. | |
Zhang X, Ao G, Wang Y, et al. Genetic variants and haplotypes of the UGT1A9, 1A7, and 1A1 genes in Chinese Han. Genet Mol Biol. 2012;35(2):428–434. | |
Liu JY, Qu K, Sferruzza AD, Bender RA. Distribution of the UGT1A1*28 polymorphism in Caucasian and Asian populations in the US: a genomic analysis of 138 healthy individuals. Anticancer Drugs. 2007;18(6):693–696. | |
Kurose K, Sugiyama E, Saito Y. Population differences in major functional polymorphisms of pharmacokinetics/pharmacodynamics-related genes in Eastern Asians and Europeans: implications in the clinical trials for novel drug development. Drug Metab Pharmacokinet. 2012;27(1):9–54. | |
Sugihara K, Ohtsu A, Shimada Y, et al. Safety analysis of FOLFOX4 treatment in colorectal cancer patients: a comparison between two Asian studies and four Western studies. Clin Colorectal Cancer. 2012;11(2):127–137. | |
Wang JH, King TM, Chang MC, Hsu CW. Oxaliplatin-induced severe anaphylactic reactions in metastatic colorectal cancer: case series analysis. World J Gastroenterol. 2012;18(38):5427–5433. | |
Chang PM, Tzeng CH, Chen PM, et al. ERCC1 codon 118 C → T polymorphism associated with ERCC1 expression and outcome of FOLFOX-4 treatment in Asian patients with metastatic colorectal carcinoma. Cancer Sci. 2009;100(2):278–283. | |
Chai H, Pan J, Zhang X, et al. ERCC1 C118T associates with response to FOLFOX4 chemotherapy in colorectal cancer patients in Han Chinese. Int J Clin Exp Med. 2012;5(2):186–194. | |
Huang MY, Huang ML, Chen MJ, et al. Multiple genetic polymorphisms in the prediction of clinical outcome of metastatic colorectal cancer patients treated with first-line FOLFOX-4 chemotherapy. Pharmacogenet Genomics. 2011;21(1):18–25. | |
Huang MY, Tsai HL, Lin CH, et al. Predictive value of ERCC1, ERCC2, and XRCC1 overexpression for stage III colorectal cancer patients receiving FOLFOX-4 adjuvant chemotherapy. J Surg Oncol. 2013;108(7):457–464. | |
Guan ZZ, Xu JM, Luo RC, et al. Efficacy and safety of bevacizumab plus chemotherapy in Chinese patients with metastatic colorectal cancer: a randomized Phase III ARTIST trial. Chin J Cancer. 2011;30(10):682–689. | |
Yamada Y, Takahari D, Matsumoto H, et al. Leucovorin, fluorouracil, and oxaliplatin plus bevacizumab versus S-1 and oxaliplatin plus bevacizumab in patients with metastatic colorectal cancer (SOFT): an open-label, non-inferiority, randomized Phase III trial. Lancet Oncol. 2013;14(13):1278–1286. | |
Cheng AL, Cornelio G, Shen L, et al. First-line cetuximab with FOLFOX or FOLFIRI every 2 weeks in KRAS wild-type metastatic colorectal cancer: Phase II APEC study. Ann Oncol. 2013;24(Suppl 4):iv34–iv35. | |
Hashiguchi Y, Hase K, Ueno H, et al. Impact of race/ethnicity on prognosis in patients who underwent surgery for colon cancer: analysis for white, African, and East Asian Americans. Ann Surg Oncol. 2012;19(5):1517–1528. | |
Lembersky BC, Wieand HS, Petrelli NJ, et al. Oral uracil and tegafur plus leucovorin compared with intravenous fluorouracil and leucovorin in stage II and III carcinoma of the colon: results from National Surgical Adjuvant Breast and Bowel Project Protocol C-06. J Clin Oncol. 2006;24(13):2059–2064. | |
Nakamoto Y, Ishiguro M, Yoshida M, et al. Noninferiority of S-1 to UFT/LV as adjuvant chemotherapy for stage III colon cancer: a randomized Phase III trial (ACTS-CC) [abstract]. J Clin Oncol. 2013; 31 Suppl:abstract 3518. | |
de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol. 2000;18(16):2938–2947. | |
Giacchetti S, Perpoint B, Zidani R, et al. Phase III multicenter randomized trial of oxaliplatin added to chronomodulated fluorouracil–leucovorin as first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2000;18(1):136–147. | |
Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: a multicenter randomized trial. Lancet. 2000;355(9209):1041–1047. | |
Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. N Engl J Med. 2000;343(13):905–914. | |
Kohne CH, Van Cutsem E, Wils J, et al. Phase III study of weekly high-dose infusional fluorouracil plus folinic acid with or without irinotecan in patients with metastatic colorectal cancer: European Organization for Research and Treatment of Cancer Gastrointestinal Group Study 40986. J Clin Oncol. 2005;23(22):4856–4865. | |
Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004;22(2):229–237. | |
Grothey A, Sargent D. Overall survival of patients with advanced colorectal cancer correlates with availability of fluorouracil, irinotecan, and oxaliplatin regardless of whether doublet or single-agent therapy is used first line. J Clin Oncol. 2005;23(36):9441–9442. | |
Cassidy J, Clarke S, Diaz-Rubio E, et al. Randomized Phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first-line therapy for metastatic colorectal cancer. J Clin Oncol. 2008;26(12):2006–2012. | |
Porschen R, Arkenau HT, Kubicka S, et al. Phase III study of capecitabine plus oxaliplatin compared with fluorouracil and leucovorin plus oxaliplatin in metastatic colorectal cancer: a final report of the AIO Colorectal Study Group. J Clin Oncol. 2007;25(27):4217–4223. | |
Diaz-Rubio E, Tabernero J, Gomez-Espana A, et al. Phase III study of capecitabine plus oxaliplatin compared with continuous-infusion fluorouracil plus oxaliplatin as first-line therapy in metastatic colorectal cancer: final report of the Spanish Cooperative Group for the Treatment of Digestive Tumors Trial. J Clin Oncol. 2007;25(27):4224–4230. | |
Rothenberg ML, Navarro M, Butts C, et al. Phase III trial of capecitabine + oxaliplatin (XELOX) vs 5-fluorouracil (5-FU), leucovorin (LV), and oxaliplatin (FOLFOX4) as second-line treatment for patients with metastatic colorectal cancer (MCRC) [abstract]. J Clin Oncol. 2007;25(Suppl 18):abstract 4031. | |
Hong YS, Park YS, Lim HY, et al. S-1 plus oxaliplatin versus capecitabine plus oxaliplatin for first-line treatment of patients with metastatic colorectal cancer: a randomized, non-inferiority Phase III trial. Lancet Oncol. 2012;13(11):1125–1132. | |
Muro K, Boku N, Shimada Y, et al. Irinotecan plus S-1 (IRIS) versus fluorouracil and folinic acid plus irinotecan (FOLFIRI) as second-line chemotherapy for metastatic colorectal cancer: a randomized Phase II/III non-inferiority study (FIRIS study). Lancet Oncol. 2010;11(9):853–860. | |
Bao HY, Fang WJ, Zhang XC, et al. Phase II study of FOLFIRI regimen in patients with advanced colorectal cancer refractory to fluoropyrimidine and oxaliplatin. Cancer Chemother Pharmacol. 2011;67(1):147–152. | |
Zhang W, Zhao ZY, Wu Q, et al. [Multicenter Phase II study of modified FOLFIRI regimen in the advanced colorectal cancer patient refractory to fluoropyrimidine and oxaliplatin]. Zhonghua Zhong Liu Za Zhi. 2006;28(10):788–790. Chinese. | |
Li J, Xu JM, Zhang XD, et al. [Irinotecan plus fuorouracil/leucovorin (FOLFIRI) as a second line chemotherapy for refractory or metastatic colorectal cancer]. Zhonghua Zhong Liu Za Zhi. 2008;30(3):225–227. Chinese. | |
Guo Y, Shi M, Shen X, Yang C, Yang L, Zhang J. Capecitabine plus irinotecan versus 5-FU/leucovorin plus irinotecan in the treatment of colorectal cancer: a meta-analysis. Clin Colorectal Cancer. 2014;13(2):110–118. | |
Hyodo I, Suzuki H, Takahashi K, et al. Present status and perspectives of colorectal cancer in Asia: Colorectal Cancer Working Group report in 30th Asia–Pacific Cancer Conference. Jpn J Clin Oncol. 2010;40(Suppl 1):i38–i43. | |
Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342. | |
Fuchs CS, Marshall J, Mitchell E, et al. Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. J Clin Oncol. 2007;25(30):4779–4786. | |
Kabbinavar FF, Hambleton J, Mass RD, Hurwitz HI, Bergsland E, Sarkar S. Combined analysis of efficacy: the addition of bevacizumab to fluorouracil/leucovorin improves survival for patients with metastatic colorectal cancer. J Clin Oncol. 2005;23(16):3706–3712. | |
Kabbinavar FF, Schulz J, McCleod M, et al. Addition of bevacizumab to bolus fluorouracil and leucovorin in first-line metastatic colorectal cancer: results of a randomized Phase II trial. J Clin Oncol. 2005;23(16):3697–3705. | |
Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized Phase III study. J Clin Oncol. 2008;26(12):2013–2019. | |
Lee KD, Chen HH, Wang HM, et al. An open-label safety study of first-line bevacizumab in combination with standard chemotherapy in Chinese patients with metastatic colorectal cancer treated in an expanded access program in Taiwan. Oncology. 2013;84(5):299–304. | |
Claret L, Gupta M, Han K, et al. Evaluation of tumor-size response metrics to predict overall survival in Western and Chinese patients with first-line metastatic colorectal cancer. J Clin Oncol. 2013;31(17):2110–2114. | |
Hoffman-La Roche. An observational study of Avastin (bevacizumab) in combination with 5-FU-based as first-line treatment in Chinese patients with metastatic colorectal cancer. Available from: http://clinicaltrials.gov/show/NCT01319877. NLM identifier: NCT01319877. Accessed July 31, 2014. | |
Van Cutsem E, Tabernero J, Lakomy R, et al. Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a Phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J Clin Oncol. 2012;30(28):3499–3506. | |
Tabernero J, Van Cutsem E, Lakomy R, et al. Aflibercept versus placebo in combination with fluorouracil, leucovorin, and irinotecan in the treatment of previously treated metastatic colorectal cancer: prespecified subgroup analyses from the VELOUR trial. Eur J Cancer. 2014;50(2):320–331. | |
Sanofi. A study of aflibercept versus placebo with FOLFIRI in patients with metastatic colorectal cancer previously treated with an oxaliplatin chemotherapy (AFLAME). Available from: http://clinicaltrials.gov/show/NCT01661270. NLM identifier: NCT01661270. Accessed July 31, 2014. | |
Grothey A, Van Cutsem E, Sobrero A, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 381(9863):303–312. | |
Bayer. Asian subjects with metastatic colorectal cancer treated with regorafenib or placebo after failure of standard therapy (CONCUR). Available from: http://clinicaltrials.gov/show/NCT01584830. NLM identifier: NCT01584830. Accessed July 31, 2014. | |
Ciardiello F, Tejpar S, Normanno N, et al. Uptake of KRAS mutation testing in patients with metastatic colorectal cancer in Europe, Latin America, and Asia. Target Oncol. 2011;6(3):133–145. | |
Bokemeyer C, Bondarenko I, Hartmann JT, et al. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: the OPUS study. Ann Oncol. 2011;22(7):1535–1546. | |
Bokemeyer C, Bondarenko I, Makhson A, et al. Fluorouracil, leucovorin, and oxaliplatin with and without cetuximab in the first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2009;27(5):663–671. | |
Van Cutsem E, Kohne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360(14):1408–1417. | |
Van Cutsem E, Kohne CH, Lang I, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol. 2011;29(15):2011–2019. | |
Tveit KM, Guren T, Glimelius B, et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: the NORDIC-VII study. J Clin Oncol. 2012;30(15):1755–1762. | |
Maughan TS, Adams RA, Smith CG, et al. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomized Phase III MRC COIN trial. Lancet. 2011;377(9783):2103–2114. | |
Adam R, De Gramont A, Figueras J, et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist. 2012;17(10):1225–1239. | |
Ye LC, Liu TS, Ren L, et al. Randomized controlled trial of cetuximab plus chemotherapy for patients with KRAS wild-type unresectable colorectal liver-limited metastases. J Clin Oncol. 2013;31(16):1931–1938. | |
Xu J, Qin X, Wang J, et al. Chinese guidelines for the diagnosis and comprehensive treatment of hepatic metastasis of colorectal cancer. J Cancer Res Clin Oncol. 2011;137(9):1379–1396. | |
Zhong LL, Chen HY, Cho WC, Meng XM, Tong Y. The efficacy of Chinese herbal medicine as an adjunctive therapy for colorectal cancer: a systematic review and meta-analysis. Complement Ther Med. 2012;20(4):240–252. | |
Van Cutsem E, Nordlinger B, Cervantes A. Advanced colorectal cancer: ESMO clinical practice guidelines for treatment. Ann Oncol. 2010;21(Suppl 5):v93–v97. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.