Back to Journals » Integrated Pharmacy Research and Practice » Volume 10
Collaborative Medication Reviews to Identify Inappropriate Prescribing in Pre-Admission Medications at Emergency Department Short-Term Ward
Authors Celikkayalar E, Puustinen J, Palmgren J, Airaksinen M
Received 22 September 2020
Accepted for publication 19 February 2021
Published 22 April 2021 Volume 2021:10 Pages 23—32
DOI https://doi.org/10.2147/IPRP.S280523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Jonathan Ling
Ercan Celikkayalar,1,2 Juha Puustinen,1,3,4 Joni Palmgren,2 Marja Airaksinen1
1Clinical Pharmacy Group, Division of Pharmacology and Pharmacotherapy, Faculty of Pharmacy, University of Helsinki, Helsinki, Finland; 2Hospital Pharmacy Department, Satasairaala Central Hospital, Pori, Finland; 3Social Security Center of Pori, Pori, Finland; 4Unit of Neurology, Satasairaala Central Hospital, Pori, Finland
Correspondence: Ercan Celikkayalar Email [email protected]
Purpose: Collaborative medication reviews (CMR) have been shown to reduce inappropriate prescribing (IP) in various settings. This study aimed at describing a CMR practice in an emergency department (ED) short-term ward in Finland to investigate IP in pre-admission medications.
Patients and Methods: Pre-admission medications were collaboratively reviewed for all the adult ED admissions within a 5-month study period in 2016. Types of IP were inductively categorized, and descriptive statistics were used to show the incidence and type of IP events.
Results: The pre-admission medications of 855 adult ED patients were reviewed by the pharmacist, with 113 IP events identified in 83 (9.7%) of the patients. The majority (81%, n=67) of these patients were older adults (≥ 65 years). Of these 94 IP events identified in 67 older patients, 58 (62%) were confirmed by the ED physicians. The following 3 main categories were inductively developed for the types of identified and confirmed IP events: 1) Misprescribing (prescription of medications that significantly increase the risk of adverse drug events); 2) Overprescribing (prescription of medications for which no clear clinical indications exist); and 3) Underprescribing (omission of potentially beneficial medications that are clinically indicated for treatment or prevention of a disease). Misprescribing was the most common type of IP identified (79% of the identified and 72% confirmed IP events). Benzodiazepines (29%) and antidepressants (28%) were involved in 33 out of 58 (57%) confirmed IP events. Medications with strong anticholinergic effects were involved in 19% of the confirmed IP events.
Conclusion: The CMR practice was able to identify IP in pre-admission medications of about one-tenth of ED patients. Older patients using benzodiazepines and drugs with strong anticholinergic effects should be paid special attention to ED admissions.
Keywords: medication reviews, collaborative medication reviews, inappropriate prescribing, potentially inappropriate medications, emergency department, clinical pharmacist
Introduction
A concerning number of preventable adverse drug events (pADE) lead to emergency department (ED) admissions or other hospital admissions.1–3 A systematic review reported that one in five prescriptions among the older adults in primary care was potentially inappropriate.4 Inappropriate prescribing (IP) results from errors in clinical decision making, leading to prescribing errors (PEs).5 PEs include failures both in the prescribing decision and the prescription writing process. Dean5 defined PE as
A clinically meaningful prescribing error occurs when, as a result of a prescribing decision or prescription writing process, there is an unintentional significant (1) reduction in the probability of treatment being timely and effective or (2) increase in the risk of harm when compared with generally accepted practice.
Using this definition, an earlier study in patients admitted to nine hospitals in the UK found one or more errors in 43.8% of the evaluated prescriptions. Nearly half (47.5%) of these PEs were related to inappropriateness of prescriptions, such as medication omissions, including omissions on admission or discharge, a drug not prescribed but indicated, and dosing errors, ie, underdose, overdose, dose/rate mismatch.6
Collaborative medication reviews (CMR) with pharmacist participation have been suggested to reduce IP. This has been found by a systematic review conducted first in 2014 (including ten studies) and updated in 2018 by adding two studies to the previous review.7 However, the clinical impact of these reductions in IP was not clear. Another earlier systematic review (ten studies) from 2016 found no evidence on CMR to reduce mortality or hospital readmissions but showed evidence that medication review may reduce ED contacts.8 A randomized clinical multicenter study (2018) from Denmark enrolled 1467 patients (median age, 72 years) during 20 months with a six-month follow-up and found that clinical pharmacist-led medication review intervention may likely reduce the number of ED visits and hospital readmissions.9
Because ED is the care unit where acutely ill patients are first admitted to being examined, it is also the place where drug-induced symptoms and events can be identified. Therefore, CMR in EDs has excellent potential for being a point of care to identify IP in pre-admission medications, mostly taken at home.10 For example, the geriatric ED guideline by The American College of Emergency Physicians (ACEP) suggests that CMRs should be initiated early in the ED.11 However, only a few recent studies explored CMRs in the ED units12–15 One of the recent studies investigated the effect of CMR among high-risk ED patients on the number of days patients spent in the hospital.12 The patients in the CMR group spent fewer days in the hospital within 30 days of the ED visit than patients in the control group who received only medication reconciliation.
Another previous study found that significant polypharmacy and potentially inappropriate medications (PIM) were lower in the post-intervention group with CMR than the pre-intervention group without CMR.13 The number of medications was also reduced significantly in the post-intervention period in patients with significant polypharmacy.13 A third study evaluated the effect of an ED-based pharmacist-led medication review intervention in high-risk patients admitted to an ED on long-term outpatient health services utilization.14 However, the pharmacist’s intervention did not show long-term changes to outpatient health services utilization. The researchers discussed that the lack of impact might have been related to not adequately communicating pharmacist recommendations to community-based providers. Therefore, the recommendations may not have affected health care delivery.14
In a previous study from Finland (2019), ED admissions in two university hospitals were investigated, and CMR, including medication reconciliation, was conducted on 150 patients.15 In the study, discrepancies in medication lists were observed in almost all study subjects (149/150). The CMRs also found a high number of medication-related problems in the study subjects. As a result, the study suggested that the current medication reconciliation and review process on the admission of older ED patients in Finland needs improvement.
To our knowledge, no previous studies have investigated the IP in pre-admission medications in ED settings using a CMR model. Therefore, the current study aimed to explore the incidence and types of IP events in pre-admission medications identified in an ED short term ward using CMRs led by a clinical pharmacist.
Patients and Methods
Evolution of CMR Practices in Finland
In Finland, CMR practices are relatively new. The development of the first CMR procedures was initiated in 2005 as part of a long-term continuing education providing accredited comprehensive CMR competence for practicing pharmacists.16 Therefore, the development of CMR practices in Finland began from comprehensive reviews, which have been thereafter extended to less comprehensive procedures such as medication list reviews (ie, prescription reviews) and various CMR procedures.16,17 After 2005, CMRs have become more common in Finnish hospitals, although the progress has been relatively slow.15,16 An inventory conducted by the Finnish Medicine Agency in 2015 identified 43 CMR procedures, of which almost half (n=22) were designed for older adults in primary care, being mostly established between 2013 and 2015.16 Fifteen of the practices were reported from government or municipality funded hospitals; health care settings were not specified.16
Study Design and Setting
This study was conducted at an ED ward, an acute, short-term care unit with 16 beds in a secondary care hospital in Finland. Patients from the emergency room are admitted to the ED ward for further medical observation up to one or two days, for specialist consultations, or before transfer to other wards in primary or secondary care, or for discharge. In this study, the ED ward was part of an ED providing primary and specialized secondary health care with 24,000 annual patient visits. The unit is located at a 350-bed secondary care hospital, serving a district with 224,000 inhabitants on Finland’s Western coast.
This was a prospective cross-sectional study. Before the actual study, a 3-month pilot was conducted to establish and standardize the CMR procedure in ED. A paper form for CMR documentation and communication was developed during the pilot phase, piloted, and introduced to the ED physicians and nurses. The form was divided into two sections: 1) documentation of findings from ED pharmacist’s review of medication for IP identification and recommendations for possible changes in the medication, and below, 2) documentation of ED physicians’ final assessments and clinical decisions, eg, confirming IPs identified by the pharmacist.
In the first phase of the study, all the adult patient admissions (≥18 years) to the ED short term ward within the study period of 5 months were reviewed (Figure 1). Patients’ readmissions to the ED within the study period were not counted in this study. After admission to the ED short-term ward for further medical observation, the physician assessed the patient’s conditions. The pre-admission medications were documented, and medication history was taken by a nurse in collaboration with the ED pharmacist. Pre-admission medications were reviewed by the ED pharmacist for each adult ED short term ward patient within 24 hours of ED presentation from Monday to Friday, for five months from April to August 2016. The specially trained ED pharmacist assessed the appropriateness of prescribing for each of the reviewed patients. After the rounds, when needed, the pharmacist and the physicians discussed the clinical relevance of the pharmacist’s recommendations to solve IP events.
 |
Figure 1 Study flow. Abbreviations: CMR, collaborative medication reviews; IP, inappropriate prescribing. |
Assessing the Inappropriateness of Pre-Admission Medications
Only prescribed pre-admission medications that the patient had been using before admission to ED were reviewed. The following definition for IP was adopted: “prescribing medications that have more potential risk than the potential benefit or prescribing that does not agree with accepted medical standards.”18 This definition was used when the ED pharmacist judged whether the patient’s medication was inappropriate. The following IP events were observed: 1) Significant drug-drug interactions (DDIs); 2) Incorrect doses considering patient’s age or condition; 3) Incorrect frequency or duration of the treatment; 4) Medication with no indication; 5) Therapeutic duplication (prescribing and dispensing of two or more drugs from the same therapeutic category such that the combined daily dose puts the patient at increased risk of adverse drug reactions without additional therapeutic benefits);19 and 6) Untreated indication.
The ED pharmacist used electronic evidence-based medication risk management databases for identifying IP events (Table 1). These databases were widely used in the Finnish social and health services system at the time of the study through the National Health Portal (Table 1). Confirmed changes to medications were documented to medication records by the ED physicians. Any change in the medication based on CMR, including adding or discontinuing a drug, alternative dose, alternative route, time, or duration of use, was counted as an implemented change on medication charts.
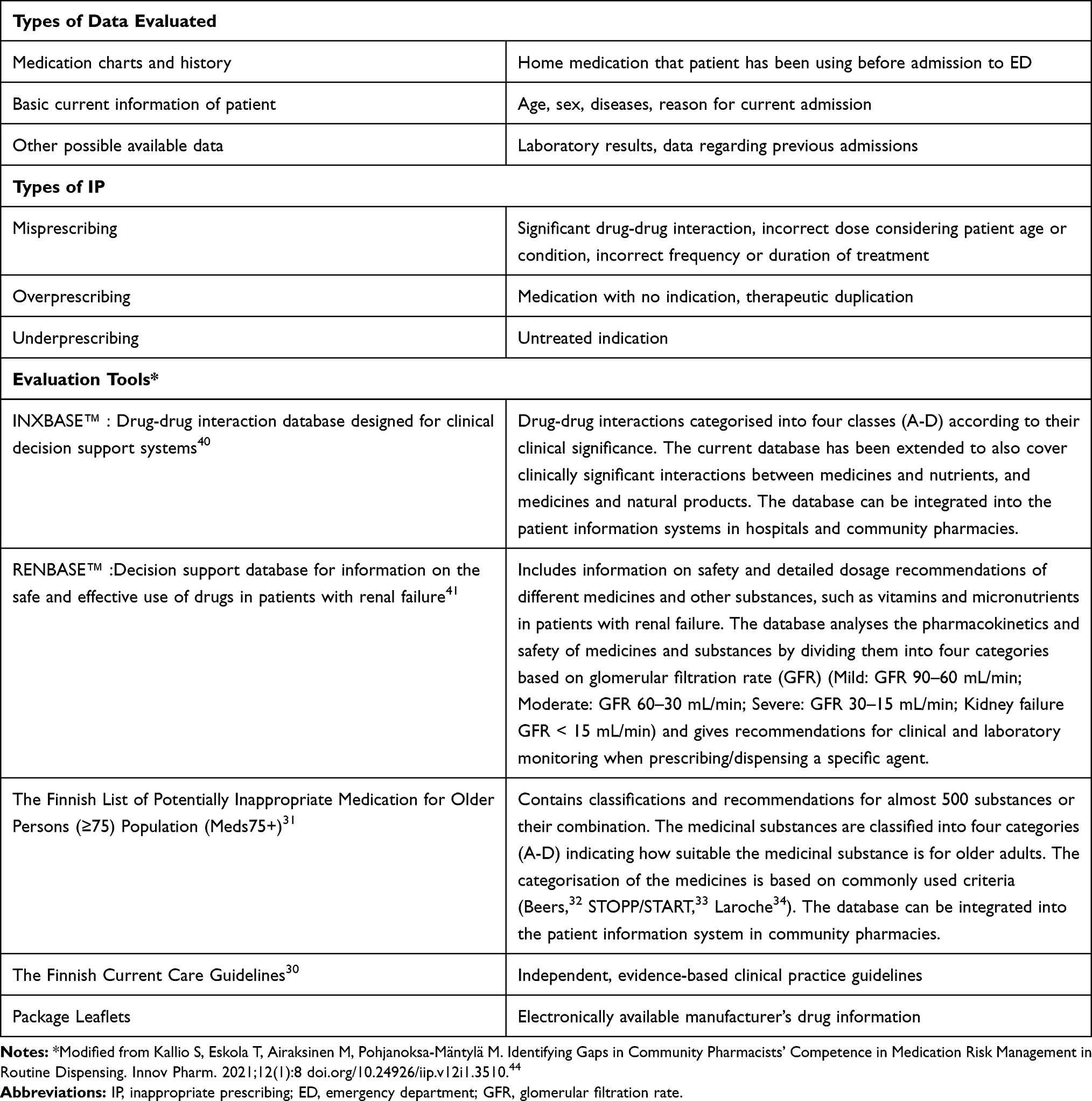 |
Table 1 Assessment of IP in Pre-Admission Medications of ED Patients: Types of Patient Data Used, Types of IP Assessed and Evaluation Tools Applied by the ED Pharmacist in Medication Reviews |
Statistical Analysis
For the descriptive analysis of the data, identified and confirmed IP events were inductively categorized.20 The first phase of the descriptive analysis included all the adult ED admissions with the CMR. The further descriptive analysis of IP events was targeted to older patients (≥65 years) because the majority of patients with at least one IP event were found to belong to this age segment (Figure 1). Quantitative variables are presented as means, standard deviations (SD), medians, and ranges (minimum and maximum). The Student’s t-test was used to compare differences. A p-value less than 0.05 was considered statistically significant. The statistical analyses were performed using SPSS 26.0.
Ethics Approval
This study was conducted with the approval of the Institutional Review Board of Satasairaala Central Hospital and under the permission of the chief administrative physician. The study was carried out in accordance with the National Research Ethics Guidelines and Regulations,21 which are in line with the Declaration of Helsinki.22 Written informed consent was obtained from participating patients. The Regional Ethics Committee, Turku Clinical Research Centre (Turku CRC) was also consulted. According to the Turku CRC’s statement, additional approval from the Regional Ethics Committee was not required for this descriptive study. Turku CRC offers support and services for investigator-initiated clinical studies.23 Its services are available to investigators at the University of Turku and in the Hospital District of Southwest Finland, including Satasairaala Central Hospital. At the time of this study, according to the National Research Ethics Guidelines and Regulations,21 Regional Research Ethics’ committee’s approval was not required for clinical practice studies based on current care guidelines.
Results
Altogether, pre-admission medications of 855 adult patients (64% women, 36% men) presented in the ED short-term ward were reviewed by the ED pharmacist during the 5-month study period. The pharmacist identified 83 (9.7%) of these patients with at least one IP event (mean 1.4 IP events per patient). The majority (81%, n=67) of the patients with IP events were older adults (≥65 years old). Therefore, further analysis on IP focused on this patient segment (Figure 1).
The pharmacist identified a total of 94 IP events in 67 older adults (mean 1.4 IP events per patient). Of the 94 identified IP events, 58 (62%) were confirmed by the ED physicians, concerning 49 out of 67 patients (73%), leading to implemented changes in their medication records. The number of regularly used pre-admission medications in the older adults with identified IP events (n=67) ranged from 2 to 18 (median 7) (Table 2). The corresponding range for the older adults with confirmed IP cases (n=49) was 6 to 18 (median 9). Of these, 36 out of 49 (73%) were female, and 13 (27%) were male (Table 2). The mean age (p=0.03) and the mean number of pre-admission medication in regular use (p=0.01) were higher in confirmed IP events than identified IP events (Table 2).
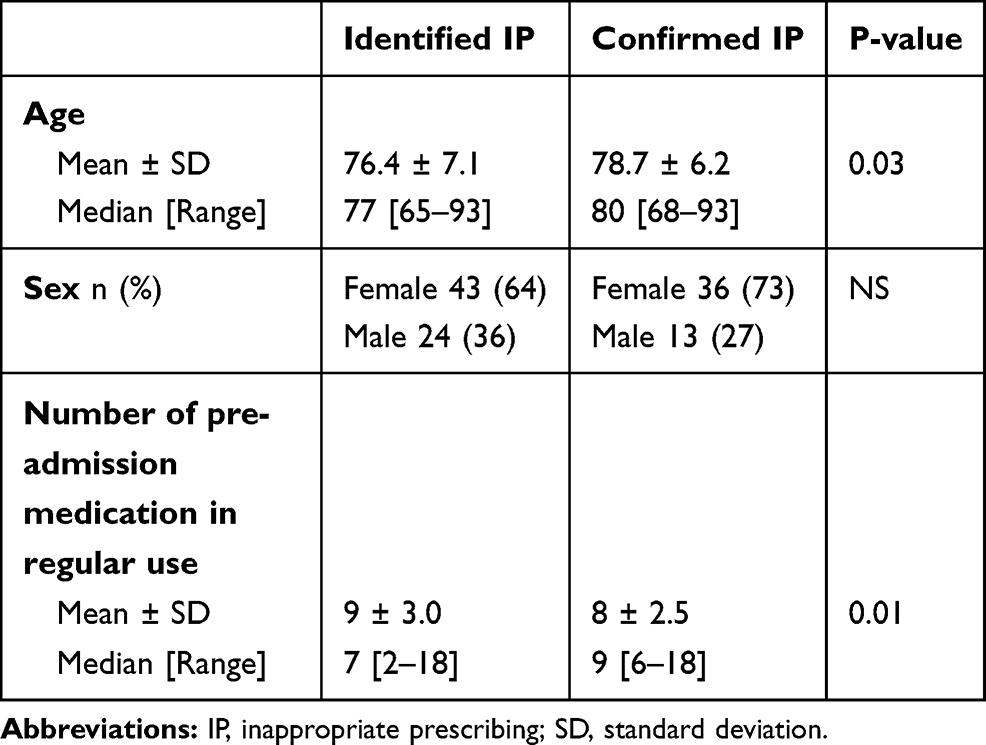 |
Table 2 Demographics for Patients ≥65 Years Old with Identified (N= 67) and Confirmed IP (N= 49) |
Types of IP Events
The inductive categorization yielded the following three main types of IP events:20 1) Misprescribing (prescribing medications that significantly increase the risk of adverse drug events); 2) Overprescribing (prescribing medications for which no clear clinical indications exist); and 3) Underprescribing (omission of potentially beneficial medications that are clinically indicated for treatment or prevention of a disease) (Table 3). Misprescribing was the most common type of IP identified (79% of the identified and 72% of the confirmed IP events), followed by overprescribing (15% vs 21%) and underprescribing (6% vs 7%) (Table 3). The majority of the misprescribing events were clinically significant DDIs (40% vs 35%) and incorrect doses considering the patient’s age or conditions (28% vs 24%). Of the incorrect doses, those considering renal impairment (RI) were the most common ones (11% vs 12%) (Table 3).
 |
Table 3 Types of IP in the Identified and Confirmed IP Events |
The Implementation Rate of Changes According to the Type of IP and the Therapeutic Group of the Medicine
Identified IP events among the older adults led to a change in medications in 62% (implementation rate) of the cases (Figure 1). Implementation rate varied from 53% (significant drug-drug interactions) to 100% (therapeutic duplications). The highest (86%) implementation rate was in overprescribing category, followed by underprescribing (67%). The lowest (57%) implementation rate was in misprescribing category (Table 3).
Benzodiazepines (chlordiazepoxide, diazepam, oxazepam, and temazepam) and antidepressants (amitriptyline, citalopram, doxepin, and fluoxetine) were involved together in 33 out of 58 (57%) IP events where changes were implemented (Table 4). Three drugs with strong anticholinergic effects (amitriptyline, doxepin, and oxybutynin) were involved in 19% of all cases where changes were implemented (Table 4).
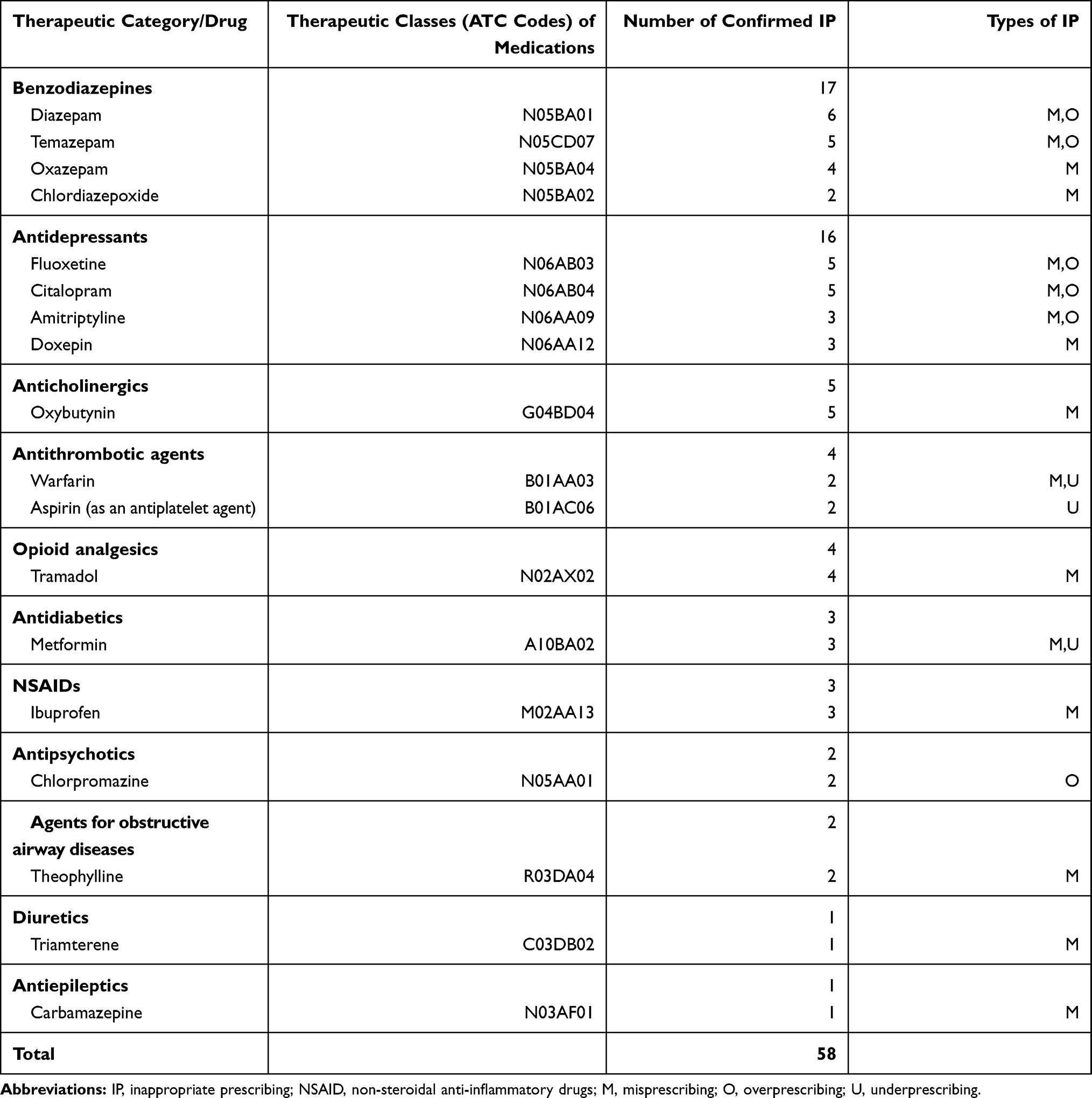 |
Table 4 Pre-Admission Medications Involved in Confirmed IP Events |
Discussion
The CMR practice was able to identify IP in pre-admission medications of about one-tenth of ED patients. The following observations were made of the incidence and type of IP events: 1) IP in pre-admission medication was most common in older adults; 2) majority of the IP events were related to misprescribing because of clinically significant DDIs, incorrect doses, frequency, or duration of treatments; 3) benzodiazepines and antidepressants were the medicines most commonly involved in IP events, followed by other medicines widely used in older adults, but considered as high-alert medicines or potentially inappropriate medicines (PIMs) to be used with caution in this age segment of adults, eg, anticholinergics.
Our study found that a high majority (81%) of the patients admitted to the ED short-term ward who had at least one IP event in their pre-admission medications were patients aged 65 years or older. This indicates that in the circumstances of scarce resources, CMR in the ED units could be focused on this patient segment. IP events identified in this research are in line with the risks identified in the previous studies.24 In our study, such commonly used PIMs as benzodiazepines and antidepressants appeared in more than half of the IP events confirmed by the ED physicians. Benzodiazepines alone (diazepam, temazepam, oxazepam, chlordiazepoxide) were related to almost one-third (30%) of the confirmed IP events with implemented changes. Even though a previous national register-based study observed a declining trend in benzodiazepine use in Finland from 2006 to 2014, the long‐term use remained high, particularly in older adults.25 Another earlier national register study based on reimbursement data found that more than one-third of the total PIM use was associated with benzodiazepines in older adults in Finland in 2007.26 In that study, temazepam was the most commonly reimbursed PIM. Previous studies have suggested actions to reduce IP concerning benzodiazepine use in older adults. These actions include training physicians and other healthcare providers in geriatric pharmacotherapy and psychotropic deprescribing,25,26 providing computerized decision-making support and alerting systems for physicians,26 involving pharmacists in medication reviews,26,27 as well as enhancing patient involvement and improving their awareness of potential risks related to benzodiazepines they are taking.25–27 For long-term benzodiazepine users, benzodiazepine withdrawal interventions have been suggested.25–29
Our present study indicates that well-coordinated CMR practice in the ED setting could effectively identify IP in benzodiazepine use and use of other PIMs in older adults. We also found that drugs with strong anticholinergic effects (amitriptyline, doxepin, or oxybutynin) were commonly used by older study participants identified with IP events. These medicines were involved in one-fifth of the implemented IP events. These highly anticholinergic, sedating drugs cause, eg, orthostatic hypotension and may lead to falls.30,31 Therefore, they are recommended to be avoided according to the national IP evaluation criteria used in this study (Table 1). The same recommendation is given in the latest Beers criteria, which is internationally among the most commonly used explicit criteria for identifying PIMs in older adults.32 Although we did not directly use the widely recognized Beers32 or STOPP/START33 criteria in our study, their information contents were incorporated in the electronic medication risk management tools used in our study (Table 1). These tools are regularly updated according to most recent scientific evidence, also covering such PIM criteria as the Beers,32 STOPP/START criteria,33 and Laroche list.34
A majority (79%) of the IP events in pre-admission medications of older ED ward patients were related to misprescribing, particularly contributing to clinically significant DDIs (40% of the misprescribing cases). The high rate of DDIs can be partly explained by polypharmacy, which is common in older patients, and older patients are considered a high-risk population for DDIs.35 Studies have shown that physicians are aware only of a minority of actual clinically significant DDIs.36 Although most of the identified IP events in our study were clinically significant DDIs, the implementation rate of changes was the lowest (53%) compared to other IP subcategories. This means that clinically significant DDIs were common, but physicians did confirm the identified DDIs only in about half of the cases. This may relate to the notion that patients did not present symptoms that could have been regarded as DDI-induced in many identified IP events. Therefore, physicians did not want to make any changes to the medication without signs of DDI-induced harmful effects. However, in these DDI cases with the uncertainty of effects, physicians, after negotiating with the ED-pharmacist, added a note to the patient record of the identified but not confirmed DDI for a possible later notice.
According to our study, one in ten of the IP events in the older patients admitted to the ED ward were dosage adjustment requirements due to renal impairment (RI). Incorrect dosing considering RI was presented in nearly half of the identified and implemented misprescribing events. RI-related inappropriate medication has been identified as a significant problem also in other studies in acute care; it has been reported that a concerning amount of prescriptions requiring dosage adjustments according to renal function remain unadjusted.37–39 A previous study found that nearly 40% of the patients had impaired renal function at hospital discharge,37 and approximately 25% of the prescribed drugs for these patients required dosage adjustment. However, only 60% of the prescriptions were adjusted according to the recommendations. Another study suggested a collaboration with clinical pharmacists to improve compliance with the clinical decision support system recommendations.39
Our study used electronically available up-to-date guidelines30,31,40,41 that are integrated into the patient administration system (Table 1). Finland has a long history of national evidence-based clinical guidelines30 that are widely and routinely use throughout the social and health services system; therefore, they were reliable tools to identify IP among patients in our study. These Guidelines are widely available in electronic format via the national health portal Terveysportti,42 which make their use feasible at the point of care. It includes up-to-date care and treatment recommendations, pharmaceutical information, and numerous medication risk management applications designed to help everyday activities. The Guidelines are based on the best available scientific and clinical evidence, and they are continuously updated.43 The “clinical eye” of professionals is needed to interpret information from the databases to make therapeutic decisions and communicate them to patients and the care team involved.
CMR proved to be a feasible method for enhancing prospective medication risk management of patients admitted to ED short term ward. However, this study has some limitations to consider when interpreting results. The study was relatively small in scale, included only one ED. It is also difficult to compare studies reporting the impact of medication review interventions because of the large variety, eg, in the interventions, patient care settings with differing levels of communication culture in organizations, and a variety of criteria and methods used to assess inappropriateness in medications.24 Our study also did not include a follow-up phase after the discharge of the patients with the confirmed IP and to see the impact of the implemented changes on their health and quality of life. Our study focused on reviewing pre-admission medications of ED patients (prescribed medications). Thus, we did not summarize any therapies prescribed during medication changes, including non-pharmacological treatments. Neither did we focus on possible alternative therapy recommendations by the ED pharmacist. This would be an interesting potential topic for further research to gain a more holistic understanding of patient care decisions at ED wards.
Conclusion
The CMR practice was able to identify IP in pre-admission medications of about one-tenth of ED patients. The majority of the IP events were related to misprescribing because of clinically significant DDIs, incorrect doses, frequency, or duration of treatments. Older patients using benzodiazepines and drugs with strong anticholinergic effects should be paid special attention to ED admissions.
Acknowledgments
We thank our Emergency Department pharmacist Mr. Jussi Lohikoski, BSc(Pharm), at the Satakunta Hospital District for his dedicated efforts. We would also like to extend our thanks to the Emergency Department staff, nurses, and doctors at the Satasairaala Central Hospital for contributing to this research and for their most appreciated collaboration.
Disclosure
This work was financially supported by the Research Fund of Satakunta Hospital District, Finland. The funders had no role in study design, data collection, analysis, decision to publish, or manuscript preparation. The funding was used by the corresponding author Ercan Celikkayalar for analysis and interpretation of data and for drafting and revising this manuscript. Juha Puustinen reports personal fees from Boehringer-Ingelheim, lecture fees from Novartis, lecture fees from Orion, lecture fees from Sanofi-Aventis, and advisory board fees from Sanofi-Aventis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Panesar SS, deSilva D, Carson-Stevens A, et al. How safe is primary care? A systematic review. BMJ Qual Saf. 2016;25(7):544–553. doi:10.1136/bmjqs-2015-004178
2. Hohl CM, Nosyk B, Kuramoto L, et al. Outcomes of emergency department patients presenting with adverse drug events. Ann Emerg Med. 2011;58(3):270–279.e274. doi:10.1016/j.annemergmed.2011.01.003
3. Woo SA, Cragg A, Wickham ME, et al. Preventable adverse drug events: descriptive epidemiology. Br J Clin Pharmacol. 2020;86(2):291–302. doi:10.1111/bcp.14139
4. Opondo D, Eslami S, Visscher S, et al. Inappropriateness of medication prescriptions to elderly patients in the primary care setting: a systematic review. PLoS One. 2012;7(8):e43617. doi:10.1371/journal.pone.0043617
5. Dean B, Barber N, Schachter M. What is a prescribing error? Qual Health Care. 2000;9(4):232–237. doi:10.1136/qhc.9.4.232
6. Seden K, Kirkham JJ, Kennedy T, et al. Cross-sectional study of prescribing errors in patients admitted to nine hospitals across North West England. BMJ Open. 2013;3(1):e002036. doi:10.1136/bmjopen-2012-002036
7. Rankin A, Cadogan CA, Patterson SM, et al. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst Rev. 2018;9(9):CD008165. doi:10.1002/14651858.CD008165.pub4
8. Christensen M, Lundh A. Medication review in hospitalised patients to reduce morbidity and mortality. Cochrane Database Syst Rev. 2016;2(2):CD008986. doi:10.1002/14651858.CD008986.pub3
9. Ravn-Nielsen LV, Duckert ML, Lund ML, et al. Effect of an in-hospital multifaceted clinical pharmacist intervention on the risk of readmission: a randomized clinical trial. JAMA Intern Med. 2018;178(3):375–382. doi:10.1001/jamainternmed.2017.8274
10. Dresden SM, Allen K, Lyden AE. Common medication management approaches for older adults in the emergency department. Clin Geriatr Med. 2018;34:415–433.
11. American College of Emergency Physicians. Geriatric Emergency Department Guideline. Available from: https://www.acep.org/globalassets/uploads/uploaded-files/acep/clinical-and-practice-management/resources/geriatrics/geri_ed_guidelines_final.pdf.
12. Hohl CM, Partovi N, Ghement I, et al. Impact of early in-hospital medication review by clinical pharmacists on health services utilization. PLoS One. 2017;12(2):e0170495. doi:10.1371/journal.pone.0170495
13. Liu Y, Chu L, Su H, et al. Impact of computer-based and pharmacist-assisted medication review initiated in the emergency department. J Am Geriatr Soc. 2019;67(11):2298–2304. doi:10.1111/jgs.16078
14. Kitchen S, McGrail K, Wickham M, et al. Emergency department-based medication review on outpatient health services utilization: interrupted time series. BMC Health Serv Res. 2020;20:254. doi:10.1186/s12913-020-05108-6
15. Schepel L, Lehtonen L, Airaksinen M, Ojala R, Ahonen J, Lapatto-Reiniluoto O. Medication reconciliation and review for older emergency patients requires improvement in Finland. Int J Risk Saf Med. 2019;30(1):19–31. doi:10.3233/JRS-180030
16. Kiiski A, Airaksinen M, Mäntylä A, et al. An inventory of collaborative medication reviews for older adults - evolution of practices. BMC Geriatr. 2019;19:321. doi:10.1186/s12877-019-1317-6
17. Leikola SN, Tuomainen L, Ovaskainen H, et al. Continuing education course to attain collaborative comprehensive medication review competencies. Am J Pharm Educ. 2009;73(6):108. doi:10.5688/aj7306108
18. Hanlon J, Schmader K, Ruby C, Weinberger M. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001;49:200–209. doi:10.1046/j.1532-5415.2001.49042.x
19. Fulda TR, Lyles A, Pugh MC, Christensen DB. Current status of prospective drug utilization review. J Manag Care Pharm. 2004;10(5):433–441. doi:10.18553/jmcp.2004.10.5.433
20. O’Connor MN, Gallagher P, O’Mahony D. Inappropriate prescribing: criteria, detection and prevention. Drugs Aging. 2012;29(6):437–452. doi:10.2165/11632610-000000000-00000
21. Finnish Advisory Board on Research Integrity. Responsible conduct in research and procedures for handling allegations of misconduct in Finland. Available from: https://www.tenk.fi/en/tenk-guidelines.
22. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
23. Turku Clinical Research Center. 2021. Available from: http://www.turkucrc.fi/luvat_ja_ohjeet/eettisen_toimikunnan_lausunto/laaketieteellisen_tutkimuksen_eettinen_ennakkoarviointi. Accessed February 7, 2021. Finnish.
24. Thomas RE, Thomas BC. A systematic review of studies of the STOPP/START 2015 and American Geriatric Society Beers 2015 criteria in patients ≥ 65 years. Curr Aging Sci. 2019;12(2):121–154. doi:10.2174/1874609812666190516093742
25. Kurko T, Saastamoinen L, Tuulio-Henriksson A, et al. Trends in the long-term use of benzodiazepine anxiolytics and hypnotics: a national register study for 2006 to 2014. Pharmacoepidemiol Drug Saf. 2018;27(6):674–682. doi:10.1002/pds.4551
26. Leikola S, Dimitrow M, Lyles A, Pitkälä K, Airaksinen M. Potentially inappropriate medication use among Finnish non- institutionalized people aged ≥65 years: a register-based, cross- sectional, national study. Drugs Aging. 2011;28(3):227–236. doi:10.2165/11586890-000000000-0000027
27. Celikkayalar E, Airaksinen M, Kivelä SL, Nieminen J, Kleme J, Puustinen J. Are older people aware of potential risks related to benzodiazepines they are taking and has anything changed in risk awareness over ten years? Patient Prefer Adherence. 2021;15:141–147. doi:10.2147/PPA.S280503
28. Salonoja M, Salminen M, Aarnio P, Vahlberg T, Kivelä SL. One-time counselling decreases the use of benzodiazepines and related drugs among community-dwelling older persons. Age Ageing. 2010;39(3):313–319. doi:10.1093/ageing/afp255
29. Lahteenmaki R, Puustinen J, Vahlberg T, et al. Melatonin for sedative withdrawal in older patients with primary insomnia: a randomized double-blind placebo-controlled trial. Br J Clin Pharmacol. 2014;77(6):975–985. doi:10.1111/bcp.12294
30. The National Current Care Guidelines. Available from: https://www.kaypahoito.fi/suositukset.
31. Finnish Medicines Agency (FIMEA). Meds75+ database of medication for older persons. Available from: https://www.fimea.fi/web/en/databases_and_registeries/medicines_information/database_of_medication_for_older_persons.
32. Fick DM, Semla TP, Steinman M, et al.; 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 updated AGS Beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
33. Ryan C, O’Mahony D, Byrne S. Application of STOPP and START criteria: interrater reliability among pharmacists. Ann Pharmacother. 2009;43:1239–1244. doi:10.1345/aph.1M157
34. Laroche ML, Charmes JP, Merle L. Potentially inappropriate medications in the elderly: a French consensus panel list. Eur J Clin Pharmacol. 2007;63(8):725–731. doi:10.1007/s00228-007-0324-2
35. Sánchez-Fidalgo S, Guzmán-Ramos MI, Galván-Banqueri M, et al. Prevalence of drug interactions in elderly patients with multimorbidity in primary care. Int J Clin Pharm. 2017;39:343–353. doi:10.1007/s11096-017-0439-1
36. Toivo TM, Mikkola JA, Laine K, Airaksinen M. Identifying high risk medications causing potential drug-drug interactions in outpatients: a prescription database study based on an online surveillance system. Res Social Adm Pharm. 2016;12:559–568. doi:10.1016/j.sapharm.2015.09.004
37. van Dijk EA, Drabbe NR, Kruijtbosch M, De Smet PA. Drug dosage adjustments according to renal function at hospital discharge. Ann Pharmacother. 2006;40(7–8):1254–1260. doi:10.1345/aph.1G742
38. Aronof GR, Aronof JR. Drug prescribing in kidney disease: can’t we do better? Am J Kidney Dis. 2014;63(3):382–383. doi:10.1053/j.ajkd.2013.11.011
39. Desmedt S, Spinewine A, Jadoul M, Henrard S, Wouters D, Dalleur O. Impact of a clinical decision support system for drug dosage in patients with renal failure. Int J Clin Pharm. 2018;40(5):1225–1233. doi:10.1007/s11096-018-0612-1
40. INXBASE interaction database. Available from: https://www.terveysportti.fi/terveysportti/interaktio.inxbase.koti#.
41. RENBASE (drug dosing in renal failure). Available from: https://www.terveysportti.fi/apps/renbase/en.
42. The Finnish Medical Society Duodecim. Terveysportti. The Finnish health portal. Available from: https://www.terveysportti.fi/terveysportti/koti.
43. The Finnish Medical Society Duodecim. Evidence-based medicine guidelines. Available from: https://www.duodecim.fi/english/products/ebmg/.
44. Kallio S, Eskola T, Airaksinen M, Pohjanoksa-Mäntylä M. Identifying Gaps in Community Pharmacists’ Competence in Medication Risk Management in Routine Dispensing. Innov Pharm. 2021;12(1):8. doi:10.24926/iip.v12i1.3510.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.