Back to Journals » Clinical Ophthalmology » Volume 20
Cohort Validation of the Endophthalmitis Vitrectomy Study for Generalized Etiologies
Authors Carpenter E, Zhou Y ![]() , Wilson MK, Gilberstadt N, Bowman L, Hu JK
, Wilson MK, Gilberstadt N, Bowman L, Hu JK
Received 25 May 2025
Accepted for publication 19 December 2025
Published 20 January 2026 Volume 2026:20 542667
DOI https://doi.org/10.2147/OPTH.S542667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Emma Carpenter,1 Yujia Zhou,2 Mary Kate Wilson,2 Noah Gilberstadt,1 Lee Bowman,1 Jonathan K Hu2
1University of Florida College of Medicine, Gainesville, FL, USA; 2Department of Ophthalmology, University of Florida, Gainesville, FL, USA
Correspondence: Emma Carpenter, Email [email protected]
Purpose: To evaluate longitudinal visual acuity (VA) outcomes in patients with endophthalmitis of any etiology at a university-affiliated hospital, using a modified Endophthalmitis Vitrectomy Study (EVS) framework comparing immediate pars plana vitrectomy (PPV), tap and injection (TAP), and TAP followed by PPV.
Patients and Methods: The study included 125 patients diagnosed with endophthalmitis between 2011 and 2023. Patients were categorized into three treatment groups: TAP, PPV, and TAP followed by PPV. Data included demographics, etiology, causative organisms, adjunctive treatments, and VA at presentation, postoperative month 3 (POM3), and final follow-up. Statistical tests included t-tests, ANOVA, Kaplan–Meier analysis, and Mann–Whitney U-tests (p < 0.05).
Results: Mean patient age was 61 years; 67.2% were male, and 45.6% were transferred from another facility. Endogenous endophthalmitis was the most common etiology (32.8%), and bacterial organisms accounted for 41.6% of cases. Mean LogMAR VA at presentation was 1.984; 76.8% had VA ≤ 20/800. Fungal cases had better initial VA than bacterial (p < 0.001), though final VA was similar. Poorer initial VA was associated with primary PPV (p < 0.001). Final VA did not differ significantly among treatment groups, though patients with light perception (LP) or worse trended toward better outcomes with PPV. Systemic antimicrobials and dexamethasone injections were not associated with improved outcomes.
Conclusion: Initial VA strongly influenced treatment. While overall outcomes were similar across groups, patients with LP or worse may benefit from primary PPV. EVS principles may apply broadly across endophthalmitis etiologies.
Keywords: endophthalmitis, pars-plana vitrectomy, complete and early vitrectomy for endophthalmitis, endophthalmitis vitrectomy study, intravitreal injection
Introduction
Endophthalmitis is a bacterial or fungal infection within the eye and may lead to profound vision loss, loss of the eye, or even death in certain cases.1,2 Endogenous cases are inoculated by bloodstream infections, while exogenous endophthalmitis cases are infected through openings in the eye formed by surgery, trauma, or corneal ulcer.1 Patients are rarely asymptomatic, usually presenting with pain, photophobia, chemosis, and decreased vision as poor as light perception (LP) in 26% of cases.3 Given the threat to vision, early diagnosis and prompt treatment are necessary.4,5
In 1995, the Endophthalmitis Vitrectomy Study (EVS), a randomized controlled trial of 420 eyes with postoperative endophthalmitis after cataract or lens replacement surgery, demonstrated unequivocal benefit of pars plana vitrectomy (PPV) in patients with initial LP vision, as opposed to vitreous tap and injection of antibiotics (TAP). There were no vision differences between treatments for eyes with hand motion (HM) vision or better, and there was no additional benefit of systemic antibiotics.3,5 The EVS, however, used 20-gauge vitrectomy systems, did not analyze the use of intraocular steroid, and only performed core vitrectomy in cases where the posterior hyaloid was attached.
In the 30 years following the EVS, vitrectomy advances, new pathogens, and changing etiologies have transformed the practice landscape.6 A modified scheme where TAP is followed by planned PPV irrespective of clinical course has become an increasingly popular treatment protocol, whereas the EVS only retreated with PPV for clinical worsening 36 to 60 hours after TAP.3 Complete and early vitrectomy for endophthalmitis (CEVE) has also been shown to be effective; however, despite the increasing number of paradigms, real-world practice patterns still show significant variation.7–9 For example, in recent IRIS registry data, primary PPV is performed in only 34% of LP cases.10 Additionally, the variety of endophthalmitis in tertiary care centers is broad –– ranging from corneal ulcers, infected glaucoma surgeries, post-intravitreal injections, trauma, and endogenous –– and may behave differently from post-cataract surgery endophthalmitis.
While subsequent studies and practice patterns have generalized some EVS findings for other etiologies and initial visual acuities, insufficient data exists to generalize findings for the spectra of endophthalmitis cases encountered in an academic setting.11–13
Existing reviews and analyses depend primarily on single-center retrospective reports to determine whether TAP is a reasonable alternative to PPV for initial management of endophthalmitis, but can lack analysis of long-term outcomes.14–18 Therefore, this study compares vision outcomes after TAP and immediate PPV for endophthalmitis treatment estimated over the post-treatment period using survival analysis and including all etiologies at an academic hospital. Outcomes in the TAP group are compared between patients who responded well and those who underwent subsequent PPV (TAP to PPV) within 7 days.
Materials and Methods
Study Design
This single-center retrospective study was conducted at the University of Florida and approved by the University of Florida Institutional Review Board (IRB). The IRB waived the requirement for individual patient consent, as the study involved retrospective review of de-identified medical records and posed minimal risk to patient confidentiality. The research was conducted in compliance with the Health Insurance Portability and Accountability Act (HIPAA) and adhered to the tenets of the Declaration of Helsinki. Patients treated for endophthalmitis of any etiology between 2011 and 2023, as identified by ICD codes, were included. Patients without initial visual acuity measurements, without a known vision baseline, or with follow-up of fewer than 90 days were excluded, except for patients whose infection resolved within 90 days resulting in no light perception (NLP) vision or return to baseline vision (20/20). Baseline demographic information, presentation delay, time to PPV, etiology, number of follow-ups, causative organism, treatments (eg, PPV, TAP, systemic antimicrobials, and dexamethasone injections), and complications of endophthalmitis were recorded. Unknown etiologies were designated as “other.” Treatment groups included (1) TAP, (2) PPV, and (3) TAP followed by PPV within 7 days, including both scheduled PPV and rescue PPV performed for worsening clinical status as determined by the responsible surgeon. Visual acuity time points include initial, post-operative month 3 (POM3), and time of last vision measurement (final) determined by recovery to 20/20 vision, enucleation, evisceration, phthisis, or a maximum of 3 years.
Surgical and Biopsy Methods
Microincision vitrectomy surgery (MIVS) was performed by vitreoretinal surgeons at the University of Florida. All surgeries were performed on the same vitrectomy system (Alcon Constellation), and 23-, 25-, or 27-gauge surgeries were utilized depending on the surgeon’s preference. In all patients with an attached posterior hyaloid, induction of posterior vitreous detachment was attempted. However, if the hyaloid was extremely adherent or the view was inadequate for proper visualization, further manipulation was not attempted. In all cases, a core vitrectomy was performed, followed by as thorough a peripheral shave as possible. The decision for tamponade was left up to the primary surgeon. Keratoplasty, lens removal, foreign body removal, and anterior chamber washout were performed as indicated in cases with anterior segment infection. Subconjunctival dexamethasone and gentamycin were used routinely after cases, as were topical prednisolone and topical antibiotics, including moxifloxacin, tobramycin, or neomycin-polymyxin B. Vitreous samples were plated on blood, chocolate, and Sabouraud dextrose agar. Gram and Giemsa stains were used on glass slides for microscopic examination. Initial empiric therapy consisted of intravitreal vancomycin (1 mg/0.1 mL) and ceftazidime (2.25 mg/0.1 mL) in both the TAP and PPV groups. Topical, intravitreal, and systemic fungal treatment was administered to patients with suspected fungal etiology, and primarily consisted of voriconazole, amphotericin, and fluconazole. In endogenous infections with known organisms, therapy was tailored according to culture results.
Statistical Analysis
Statistical analysis was conducted using JASP software (v0.18.3).19 VA was converted from Snellen to logarithm of the minimum angle of resolution (LogMAR) for analysis.20 VA of CF, HM, LP, and NLP were assigned LogMAR values of 1.9, 2.3, 2.7, and 3.0, respectively.21 Paired samples t-tests and Mann–Whitney U-tests were performed to investigate the association between prognostic factors and VA. Analysis of variance (ANOVA) was used for between-group comparisons of VA and Tukey’s HSD post hoc testing was performed. Kaplan–Meier survival analysis was performed to assess the probability of vision improvement. For all analyses, p < 0.05 was considered statistically significant.
Results
Cohort Characteristics
A total of 125 patients were included in this study, including 84 males and 41 females with an average age of 61 years (range = 24–94, SD = 17.28). The median presentation delay was 5 days (range = 0–62, skew = 2.406), with 57 patients (45.6%) transferred from another facility or external clinic. The mean LogMAR VA recorded at presentation was 1.984 (SD = 0.773), corresponding to a Snellen VA of approximately count fingers (CF) at two feet. Ninety-six patients (76.8%) presented with a Snellen VA of 20/800 or worse. Twenty-four patients (19.2%) presented with LP vision and 5 patients (4%) presented with NLP vision. Forty-nine patients received TAP (40.8%), 30 patients received PPV (25%), and 41 patients received TAP followed by PPV (34.2%). Silicone tamponade was used in 38 (50%) cases, air or gas in 18 (23.7%) cases, and no tamponade in 20 (26.3%) cases.
Etiology and Causative Organisms
The majority of endophthalmitis cases were exogenous (61.6%), while the remainder were endogenous (32.8%) or “other” (5.6%). More detailed etiologies are displayed in Figure 1a and b, which show that most organisms were bacterial (52 patients; 41.6%), followed by fungal (12 patients; 9.6%), or polymicrobial (6 patients; 4.8%). No organism formed a majority (Figure 1c), but the most common causative organism belonged to the genus Staphylococcus (20 patients; 16%). Among the 125 patients, 53 (42.4%) had positive eye cultures identifying a causative organism, 47 (37.6%) had negative eye cultures with no additional cultures available, and 16 (12.8%) had negative eye cultures but the endogenous pathogen was presumed from systemic cultures. In 9 cases (7.2%), both systemic and intraocular cultures showed no growth, yet endogenous endophthalmitis was suspected due to the patients’ response to intravitreal or systemic antimicrobials.
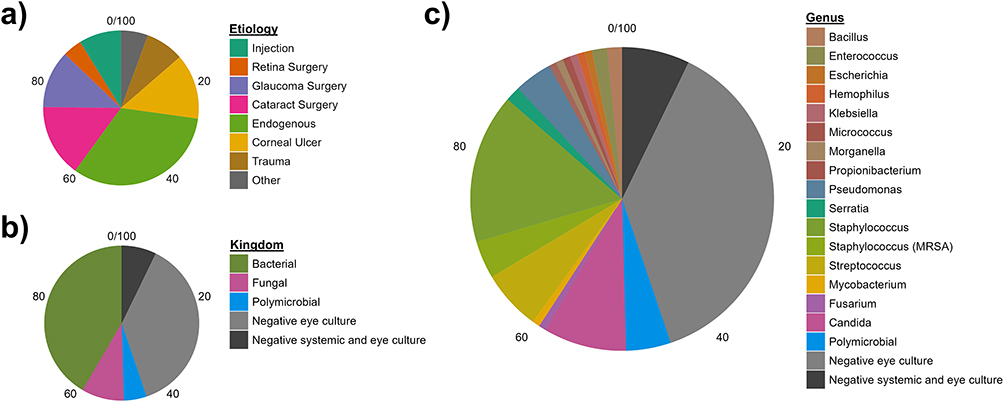 |
Figure 1 Pie charts of (a) the suspected etiology of endophthalmitis and the intraocular culture pathogen (b) kingdom and (c) genus. Cases with no positive culture but with a known etiology and treatment response to antibiotics alone, with or without PPV, were also considered endophthalmitis. |
One-way ANOVA of initial VA by etiology revealed that there were no significant differences in initial vision (Figure 2a), but the endogenous endophthalmitis group had better final visual outcomes compared to the glaucoma surgery group (p = 0.036) (Figure 2b), and there was no other statistically significant difference in final VA among other etiologies. Fungal endophthalmitis presented with superior vision compared to bacterial (p < 0.001) and polymicrobial (p = 0.009) cases (Figure 3a), but there were no significant differences in final VA among the pathogen kingdoms (Figure 3b).
 |
Figure 2 Box plots of (a) initial visual acuity and (b) final visual acuity measured in LogMAR separated by presumed etiology. |
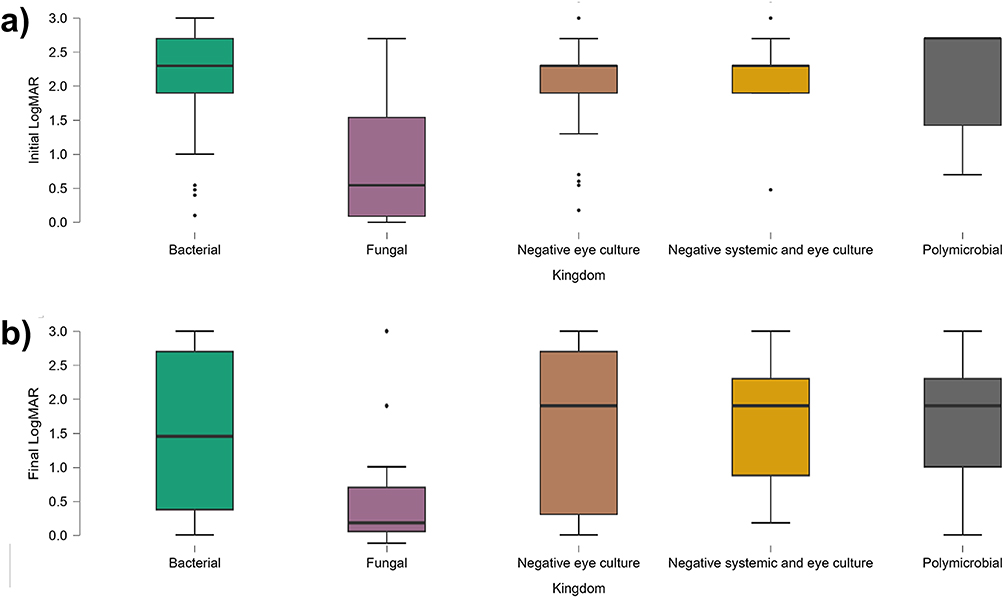 |
Figure 3 Box plots of (a) initial visual acuity and (b) final visual acuity measured in LogMAR separated by kingdom of causative organism. |
Vision Outcomes
In this cohort (Figure 4), 49 patients received TAP (40.8%), 30 patients received PPV (25%), and 41 patients received TAP followed by PPV (34.2%). Initial VA was worse for PPV than TAP (p < 0.001), generally following EVS principles, but no association was found at POM3 or final VA by two-way repeated-measures ANOVA (Figure 5). The TAP to PPV group was not significantly different from either group. Initial vision was correlated with final vision (r = 0.474, p < 0.001); therefore, a paired-sample analysis was used. There was no association between presentation delay or diagnosis-to-PPV interval and final vision (p > 0.05). Longer presentation delay correlated with a longer diagnosis-to-PPV interval (r = 0.26, p < 0.001). The distribution, skewed by a few patients presenting after more than 10 days, indicates that chronic endophthalmitis cases tended to receive PPV with less urgency.
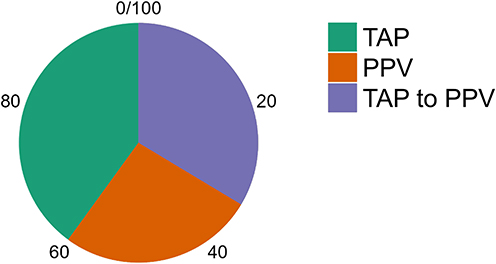 |
Figure 4 Pie chart representing the split between treatment groups: tap and injection (TAP), pars plana vitrectomy (PPV), and TAP followed by PPV (“TAP to PPV”). |
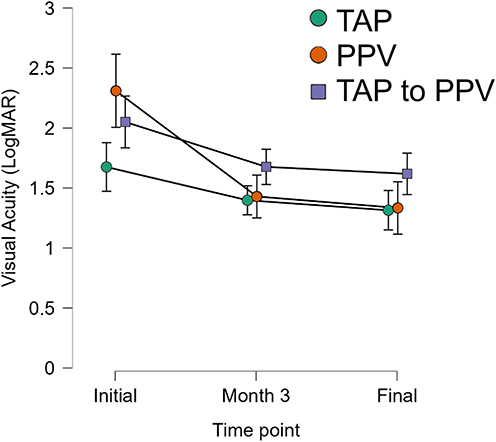 |
Figure 5 Line plots represent visual acuity measured in LogMAR over time, each line representing a treatment group including tap and injection (TAP), pars plana vitrectomy (PPV), and TAP followed by PPV (“TAP to PPV”). 95% confidence intervals are used for error bars. |
The efficacy of the treatment groups was further compared by dividing patients into two subgroups based on initial VA: those with LP vision or worse at presentation and those with vision better than LP at presentation. LP status was associated with significantly different VA trends (p < 0.001) and the effect of treatment group on visual outcomes depended on LP status (p = 0.045). While subgroup size (nTAP = 7, nPPV = 10, nTAP to PPV = 11) was insufficient for statistical analysis, there may be a general trend for greater vision gains with primary PPV among LP and NLP eyes, as seen in Figure 6.
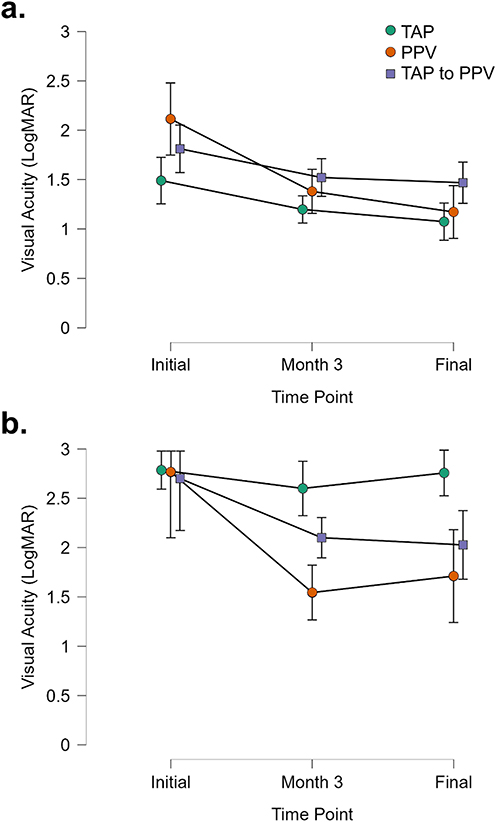 |
Figure 6 Line plots represent visual acuity measured in LogMAR over time, each line representing a treatment group including tap and injection (TAP), pars plana vitrectomy (PPV), and TAP followed by PPV (“TAP to PPV”). Separate graphs are displaced for each initial visual acuity group: (a) initial visual acuity greater than light perception and (b) initial visual acuity of light perception or worse. 95% confidence intervals are used for error bars. |
Survival analysis assessing the probability of vision improvement (VA > 20/200) was performed (Figure 7). No significant difference in visual outcomes was observed across treatment groups (p = 0.541), but patients in the TAP to PPV group appeared to have delayed vision recovery. Nevertheless, no group had significantly different vision recovery after 1 year.
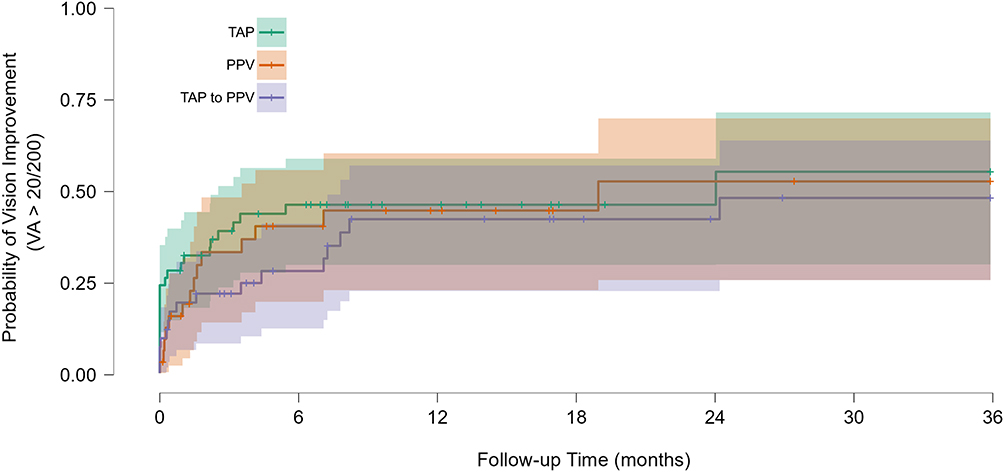 |
Figure 7 Kaplan-Meier survival curves show probability of vision improvement (visual acuity > 20/200) for three treatment groups: injection only (green), PPV only (orange), and injection followed by PPV (“TAP to PPV”, purple). Shaded regions represent 95% confidence intervals. |
Adjunct Medical Therapy
Intraocular dexamethasone was given more often (p < 0.001) to patients who underwent PPV first (47.9%) compared to patients who underwent initial TAP (27.4%) or had TAP followed by PPV (21.6%). Systemic treatment was given to 68% of patients similarly across groups. However, several systemic agents were often used either by the referring physician or the hospitalist team in endogenous endophthalmitis. Up to 27 different systemic antimicrobials were reportedly administered, with the most common systemic antimicrobials being ciprofloxacin (34 patients; 27.2%) and fluconazole (20 patients; 16%). A one-way ANOVA revealed no significant differences in the VA of patients receiving intravitreal antibiotics and systemic antimicrobials at any time point (Figure 8). There was also no difference in vision trend by tamponade type by one-way ANOVA. Moreover, a one-way ANOVA revealed no significant association between VA and dexamethasone injection at any time point (Figure 9), nor were there significant interactions with treatment group.
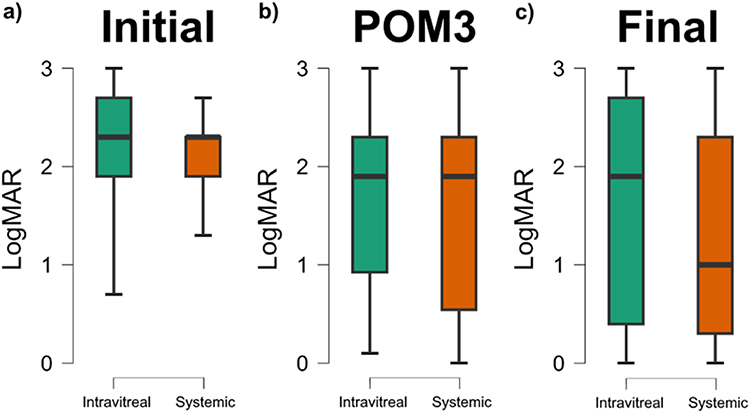 |
Figure 8 Box plot of visual acuities measured in LogMAR at (a) initial, (b) post-operative month 3, and (c) final evaluation separated by treatment of intravitreal (cyan) or systemic and intravitreal antimicrobials (orange). |
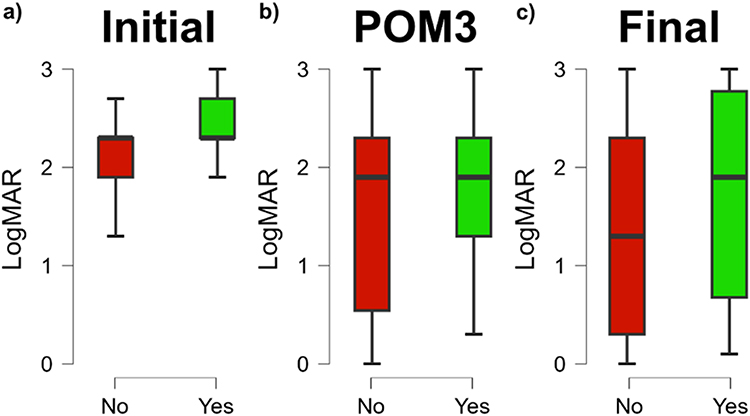 |
Figure 9 Box plot of visual acuities measured in LogMAR at (a) initial, (b) post-operative month 3, and (c) final evaluation separated into patients who received dexamethasone injection (green) and patients who did not (red). |
Discussion
The EVS has greatly influenced the management of endophthalmitis since its publication in 1995, establishing PPV as an effective option that is equal or superior to injection alone for endophthalmitis.3,5 However, the findings of the EVS may not be generalizable for all etiologies of endophthalmitis.11 Moreover, almost 30 years after the publication of EVS, some consider the EVS protocol outdated due to advances in the understanding of endophthalmitis and treatment modalities.6–8 As such, this study assesses longitudinal VA outcomes of endophthalmitis of any etiology at a university-affiliated hospital, along with analyses of adjunct steroid and systemic antibiotic use.
Characteristics of a Combined Hospital, Emergency Department, and Clinic Cohort
The cohort was predominantly male (67.2%) with an average age of 61 years; this contrasts with the EVS, which was 43% males with an average age of 75 years.3 The younger average age observed may reflect the various etiologies of endophthalmitis included in this study, rather than only post-cataract or secondary intraocular lens implantation. Moreover, the higher male preponderance may reflect the inclusion of etiologies with a known sex predilection, such as posttraumatic endophthalmitis.15,22 A slightly smaller percentage of patients (76.8%) in this study presented with an initial Snellen VA of 20/800 or worse compared to the EVS (86%). Similarly, a slightly smaller percentage of patients (19.2%) in this study presented with LP vision compared to the EVS (26%). The relatively similar initial VA of patients allowed for a cohort comparable to that seen in the EVS.
Treatment Effects on Vision
Patients with worse initial VA were more likely to receive immediate PPV (Figure 5), which reflects practice patterns at the University of Florida following standards established by the EVS. Practice interpretations captured in this cohort are loose and do not strictly follow the EVS guidelines for LP vision. As previously mentioned, data from the IRIS registry suggest that overall implementation of the EVS differs even more, with only a minority (34%) of LP vision patients receiving immediate vitrectomy.10 Although it was not statistically significant, this subgroup analysis did show a trend toward improved final visual acuity with primary PPV among LP and NLP eyes (Figure 6b), suggesting that the EVS and subsequent studies are correct to recommend earlier vitrectomy for cases with low initial vision (HM, LP, or NLP) due to potential for greater vision gains.11,12 Nevertheless, there was no significant difference in overall POM3 or final VA between treatment groups, consistent with the EVS finding that endophthalmitis generally has similar visual outcomes regardless of treatment sequence (eg, TAP, PPV, and TAP to PPV). This lack of significant difference between treatments is reassuring, particularly in situations where surgery may be of higher risk, as it suggests that TAP may be a reasonable option for cases such as eyes with no vision potential, systemic contraindications to surgery, or other causes for LP vision such as severe corneal opacity.
After initial TAP, subsequent PPV may be considered depending on the clinical course. In the EVS, 11% of TAP patients underwent PPV as rescue therapy within 60 hours of TAP and were included in the intention-to-treat analysis. Our analysis suggests that even when PPV is performed after TAP, vision outcomes are not substantially different from those who underwent initial PPV (Figure 6). While our findings align with the EVS overall, the EVS provided minimal data on outcomes for the subset of TAP-treated patients who subsequently underwent PPV. Our analysis addresses this gap by presenting survival curves for patients who underwent TAP followed by PPV, showing similar likelihoods of achieving > 20/200 vision, with a modest delay in visual recovery noted (Figure 7). In cases that respond well to TAP, PPV may still be done for vision rehabilitation and clearing the visual axis after endophthalmitis resolves. The adoption of MIVS and improved visualization systems make staged PPV a much more attractive option today compared to 1995.23,24 Delaying PPV in a staged protocol may allow operating under less inflammatory conditions, and avoiding PPV in the treatment of early endophthalmitis with relatively preserved visual acuity may help mitigate the risks of complications such as cataract formation, retinal detachment, and the potential for glaucoma.25,26
Treatment with systemic antimicrobials did not improve visual outcomes in patients with endophthalmitis in this study, consistent with the findings of the EVS in 1995. This finding can now be applied to various etiologies of endophthalmitis and antimicrobials, rather than only amikacin and ceftazidime used in the EVS. Third-generation fluoroquinolones are now widely available as well and have allowed outpatient treatment for many patients which would have required admission for inpatient antibiotics in 1995.1,6 The low cost and risks of outpatient antibiotics compared to the potential of worsening vision loss from endophthalmitis may help explain why, despite EVS findings, many surgeons continue to give systemic antibiotic treatments for these cases. Consistent with the EVS findings, dexamethasone injections did not affect vision outcomes in the treatment of endophthalmitis (Figure 9). Nevertheless, steroids are sometimes used in clinical practice because they have been proven safe in cases of endophthalmitis as long as definitive treatment with TAP or PPV is performed.7,27,28 Some surgeons recommend dexamethasone whenever silicone oil is used, either because it allows the silicone oil to be better tolerated or because silicone oil is used in more severe cases of endophthalmitis.7
Study Limitations and Future Directions
This study is limited by its retrospective nature, lack of a control group, and modest sample size. Nevertheless, high-quality experimental studies of all causes of endophthalmitis have not yet replaced or confirmed the findings and recommendations of the EVS, so retrospective studies are still needed for meta-analyses as vitrectomy and antibiotic technologies evolve.13–16 Additionally, the subgroup analysis conducted in this study lacked the statistical power needed to definitively corroborate the EVS finding that patients with LP vision or worse benefit from primary PPV. Thus, a large, multi-center study with a greater sample size of each etiology is preferable to further compare the efficacies of PPV and TAP.
Conclusion
In this study, there was overall no difference in endophthalmitis visual outcomes after PPV compared to TAP when analyzed in aggregate, although subgroup analysis of patients with presenting LP vision appears to suggest a benefit with primary PPV. Additionally, this study reports no benefit from dexamethasone injections or systemic antimicrobials in the treatment of endophthalmitis. Thus, the present study provides support that several EVS findings –– namely, PPV and TAP have similar vision outcomes in most cases, no benefit from systemic antibiotics or adjunct steroids, and good efficacy of PPV following initial TAP –– may be generalizable to other causes of endophthalmitis. Longitudinal outcomes also show that PPV after TAP results in similar outcomes. As such, dexamethasone injections and systemic antimicrobials may be omitted when appropriate, and it is reasonable to perform tap and injection followed by close monitoring when vision is initially HM or better.
Abbreviations
VA, Visual Acuity; EVS, Endophthalmitis Vitrectomy Study; TAP, Tap and Injection; PPV, Pars Plana Vitrectomy; POM3, Postoperative Month 3; LP, Light Perception; NLP, No Light Perception; HM, Hand Motion; CF, Count Fingers; LogMAR, Logarithm of the Minimum Angle of Resolution; ANOVA, Analysis of Variance; IRB, Institutional Review Board; HIPAA, Health Insurance Portability and Accountability Act; CEVE, Complete and Early Vitrectomy; HSD, Honestly Significant Difference (Tukey’s HSD test); ICD, International Classification of Diseases; MIVS, Microincision Vitrectomy Surgery.
Acknowledgments
The abstract was presented at the Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting, May 5, 2025, Salt Lake City, UT.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Durand ML. Bacterial and fungal endophthalmitis. Clin Microbiol Rev. 2017;30(3):597–11. doi:10.1128/CMR.00113-16
2. Desilets J, Lee CS, Fang W, Hinkle DM. Mortality risk associated with endophthalmitis in West Virginia. Int Ophthalmol. 2021;41(8):2887–2895. doi:10.1007/s10792-021-01849-3
3. Endophthalmitis Vitrectomy Study Group. Results of the endophthalmitis vitrectomy study: a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113(12):1479–1496. doi:10.1001/archopht.1995.01100120009001
4. Kernt M, Kampik A. Endophthalmitis: pathogenesis, clinical presentation, management, and perspectives. Clin Ophthalmol. 2010;4:121–135. doi:10.2147/opth.s6461
5. Forster RK. The endophthalmitis vitrectomy study. Arch Ophthalmol. 1995;113(12):1555–1557. doi:10.1001/archopht.1995.01100120085015
6. Panahi P, Mirzakouchaki-Borujeni N, Pourdakan O, Arevalo JF. Early vitrectomy for endophthalmitis: are EVS guidelines still valid? Ophthalmic Res. 2023;66(1):1318–1326. doi:10.1159/000534650
7. Kuhn F, Gini G. Complete and Early Vitrectomy for Endophthalmitis (CEVE) as today’s alternative to the endophthalmitis vitrectomy study. In: Kirchhof B, Wong D, editors. Vitreo-Retinal Surgery. Springer Berlin Heidelberg; 2007:53–68. doi:10.1007/978-3-540-33670-9_5
8. Shao EH, Yates WB, Ho IV, Chang AA, Simunovic MP. Endophthalmitis: changes in presentation, management and the role of early vitrectomy. Ophthalmol Ther. 2021;10(4):877–890. doi:10.1007/s40123-021-00406-6
9. Barry P, Cordovés L, Gardner S. ESCRS guidelines for prevention and treatment of endophthalmitis following cataract surgery: data, dilemmas and conclusions. Eur Soc Cataract Refract Surg. 2013:1–44.
10. Tomaiuolo M, Deaner J, VanderBeek BL, et al. Are treatment patterns for endophthalmitis after cataract surgery following the EVS trial recommendations?: an IRIS® Registry (Intelligent Research in Sight) analysis. Invest Ophthalmol Vis Sci. 2024;65(7):2424.
11. Flynn HW, Scott IU. Legacy of the endophthalmitis vitrectomy study. Arch Ophthalmol. 2008;126(4):559–561. doi:10.1001/archopht.126.4.559
12. Sen AC, Mehta SM, Sule A, et al. Immediate vitrectomy vs tap and inject in eyes with acute postcataract endophthalmitis and visual acuity ≥HM: a randomized clinical trial. Retina. 2023;43(6):940. doi:10.1097/IAE.0000000000003759
13. Zhang WF, Zhao XY, Meng LH, Chen H, Chen YX. Endophthalmitis at a tertiary referral center: characteristics and treatment outcomes over three decades. Front Cell Dev Biol. 2022;10:952375. doi:10.3389/fcell.2022.952375
14. Jackson TL, Paraskevopoulos T, Georgalas I. Systematic review of 342 cases of endogenous bacterial endophthalmitis. Surv Ophthalmol. 2014;59(6):627–635. doi:10.1016/j.survophthal.2014.06.002
15. Chen G, Tzekov R, Li W, Jiang F, Mao S, Tong Y. Incidence of endophthalmitis after vitrectomy: a systematic review and meta-analysis. Retina. 2019;39(5):844. doi:10.1097/IAE.0000000000002055
16. Fileta JB, Scott IU, Flynn HW. Meta-analysis of infectious endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents. Ophthalmic Surg Lasers Imaging Retina. 2014;45(2):143–149. doi:10.3928/23258160-20140306-08
17. Far PM, Yeung SC, Farimani PL, et al. Tap and inject versus pars plana vitrectomy for postprocedural endophthalmitis: a Meta-analysis. Retina. 2021;41(10):2009. doi:10.1097/IAE.0000000000003203
18. Cioana M, Naidu S, Far PM, Yeung SC, You Y, Yan P. Postintravitreal injection and postcataract extraction endophthalmitis visual outcomes by organism: a systematic review and meta-analysis. Retina. 2024;44(9):1608–1618. doi:10.1097/IAE.0000000000004143
19. Love J, Selker R, Marsman M, et al. JASP: graphical statistical software for common statistical designs. J Stat Softw. 2019;88(2):1–17. doi:10.18637/jss.v088.i02
20. Bach M, Schulze-Bonsel K, Feltgen N, Burau H, Hansen L. Author response: numerical imputation for low vision states. (eLetter). 2007.
21. Bach M. Visual acuity cheat sheet. Available from: https://michaelbach.de/sci/acuity.html.
22. Pieramici DJ, Sternberg P, Aaberg TM, et al; The Ocular Trauma Classification Group. A system for classifying mechanical injuries of the eye (globe). Am J Ophthalmol. 1997;123(6):820–831. doi:10.1016/s0002-9394(14)71132-8
23. Ribeiro L, Oliveira J, Kuroiwa D, et al. Advances in vitreoretinal surgery. J Clin Med. 2022;11(21):6428. doi:10.3390/jcm11216428
24. Blom K, Jørstad ØK, Faber RT, et al. Primary vitrectomy or intravitreal antibiotics followed by early vitrectomy for acute endophthalmitis: a prospective observational study. Acta Ophthalmol. 2023;101(1):100–108. doi:10.1111/aos.15207
25. Miele A, Govetto A, Fumagalli C, et al. Ocular hypertension and glaucoma following vitrectomy: a systematic review. Retina. 2018;38(5):883–890. doi:10.1097/IAE.0000000000001651
26. Jin W, Xu Y, Wang W, Xing Y, Yang A. Efficacy and safety of 23-gauge pars plana vitrectomy/silicone oil tamponade combination for treatment of pediatric post-traumatic endophthalmitis. Curr Eye Res. 2017;42(8):1143–1148. doi:10.1080/02713683.2017.1297460
27. Soliman MK, Gini G, Kuhn F, et al. International practice patterns for the management of acute postsurgical and postintravitreal injection endophthalmitis: european vitreo-retinal society endophthalmitis study report 1. Ophthalmol Retina. 2019;3(6):461–467. doi:10.1016/j.oret.2019.03.009
28. Hall EF, Scott GR, Musch DC, Zacks DN. Adjunctive intravitreal dexamethasone in the treatment of acute endophthalmitis following cataract surgery. Clin Ophthalmol. 2008;2(1):139–145. doi:10.2147/opth.s2128
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Changes in Aqueous Humor Cytokine Profile Following Intravitreal Brolucizumab Injection
Ruamviboonsuk V, Kongwattananon W, Chuaypen N
Clinical Ophthalmology 2025, 19:427-437
Published Date: 11 February 2025
Epidemiology, Microbiology, Management and Outcomes of Endophthalmitis: An 18 Year Retrospective Observational Study at a Tertiary Referral Center in Australia
Maher C, Guo B, Sim B, Loewenthal MR, Gillies D, Hall AB
Clinical Ophthalmology 2026, 20:583832
Published Date: 6 February 2026