Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Cognitive Impairment and Related Factors Among Middle-Aged and Elderly Patients with Type 2 Diabetes from a Bio-Psycho-Social Perspective
Authors Xu W ![]() , Hu X
, Hu X ![]() , Zhang X, Ling C, Wang C, Gao L
, Zhang X, Ling C, Wang C, Gao L ![]()
Received 14 August 2021
Accepted for publication 15 October 2021
Published 28 October 2021 Volume 2021:14 Pages 4361—4369
DOI https://doi.org/10.2147/DMSO.S333373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Weiran Xu,1,* Xiling Hu,2,* Xing Zhang,3 Cong Ling,4 Chaofan Wang,5 Lingling Gao1
1School of Nursing, Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Medicine, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 3Department of Endocrinology and Metabolism, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, People’s Republic of China; 4Department of Neurosurgery, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 5Department of Endocrinology and Metabolism, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lingling Gao Email [email protected]
Objective: This study investigated the biomedical, psychological, and social behavior risk factors for cognitive impairment in middle-aged and elderly patients with type 2 diabetes mellitus (T2DM).
Methods: This cross-sectional study included 240 patients with T2DM. A questionnaire was used to collect demographic and disease-related data on patients, and the Self-rating Depression Scale (SDS), Diabetes Self-care Scale (DSCS), and Social Support Rating Scale (SSRS) were used to assess patients’ depression status, self-management behavior, and social support, respectively. The Chinese version of the Montreal Cognitive Assessment (MoCA) was used to evaluate cognitive function, with a score < 26 set as the threshold for cognitive impairment.
Results: The prevalence of cognitive dysfunction in middle-aged and elderly patients with T2DM was 52.5%. Multivariate logistic regression analysis showed that older age, a history of hypoglycemia within 1 month, and depression were independent risk factors for cognitive impairment. Education for > 12 years, urban living, and a higher total score on the DSCS were independent protective factors against cognitive impairment.
Conclusion: T2DM patients with high risk of cognitive impairment can be identified early from the bio-psycho-social perspective. Patients with T2DM who are older, less educated, living in rural areas, have hypoglycemia history, and have poor self-management of diabetes are at increased risk of cognitive impairment. Closer monitoring of patients with hypoglycemia, early detection of depression, and improving patients’ self-management capacity can prevent cognitive impairment in middle-aged and elderly patients with T2DM.
Keywords: type 2 diabetes mellitus, cognitive impairment, depression, self-care, social support
Introduction
Type 2 diabetes mellitus (T2DM) is a common metabolic disease characterized by chronic hyperglycemia. It is estimated that about 9.3% (463 million) of the adult population worldwide suffers from diabetes, with T2DM accounting for 90% of cases.1 T2DM is often associated with organ damage and dysfunction including cardiovascular disease, blindness, nerve damage, and renal failure that can lead to disability or death.2
Recent studies have shown that T2DM increases the risk of cognitive impairment in middle-aged and elderly people.3,4 About 10–20% of patients with T2DM experience mild cognitive impairment (MCI).5,6 T2DM also accelerates the progression of MCI to dementia,7,8 which can diminish the quality of life and prognosis of patients. Cognitive impairment is one of the serious complications of T2DM, but it is often easy to be ignored. There are no standardized recommendations on the prevention and treatment of T2DM cognitive impairment. In addition, the impairment of cognitive function is difficult to reverse.9 Therefore, the early prevention of cognitive impairment is particularly important. Taking measures to delay the progress of cognitive impairment in MCI stage is the key measure to prevent its transformation to dementia.
The mechanism of type 2 diabetes affecting cognitive function is not yet clear. However, many studies have reported different risk factors, including long duration of diabetes, obesity,10 physical inactivity, age,11 depression,12 lack of social support,13,14 unstable blood glucose level,15,16 elevated level of inflammatory markers,17 and other diagnostic markers.18 Some studies have reported the protective effects of being married and living in the city19 on cognitive function in type 2 diabetic patients. And other studies have specifically explored the close relationship between cognitive function and self-management behavior.20,21
So far, the study on the influencing factors of cognitive function in T2DM patients is still limited, mainly focusing on biomedical factors, and many risk factors have also been evaluated separately. In this study, we investigated the status of cognitive function in middle-aged and elderly T2DM patients, and explored the effects of general information, self-management behavior, depression and social support on cognitive function in T2DM patients. To explore the risk factors of cognitive impairment in middle-aged and elderly T2DM patients from the biomedical, psychological, and social behavioral perspective. Furthermore, professional cognitive function assessment needs to be led by specialists and takes a long time. It is almost impossible to arrange professional evaluations for all T2DM patients. Therefore, we aim to provide clinicians and diabetes specialist nurses with a quick way to identify high-risk patients with cognitive impairment, so as to promote early assessment and intervention of cognitive impairment in T2DM patients and improve their health outcomes.
Materials and Methods
Study Design and Participants
This cross-sectional study included 240 patients with T2DM who were recruited at the Department of Endocrinology and Metabolism, the Third Affiliated Hospital of Sun Yat-sen University, from September 2019 to February 2020. All participants were eligible if they were aged 45 years or older, diagnosed with T2DM, and had diabetes for longer than 3 months. Participants were excluded if they were diagnosed with organic brain diseases; abused drugs; had mental or neurologic diseases or communication disorders; or had serious infections, cancer, or other serious diseases.
After the participants signed the informed consent form, we collected general information and performed the cognitive assessment. The participants also completed related questionnaires.
Main Variables
We collected patient data from the bio-psycho-social perspective. The biomedical dimension included sociodemographic and disease factors; the psychological dimension included depression; and the social behavior dimension included self-management behavior and social support.
Baseline data included the following.
- Sociodemographic factors: Age, sex, education level, place of residence, occupational status, smoking, drinking, and diabetes education.
- Disease factors: Body mass index; diabetes course; history of hypoglycemia; diabetes treatment; hypertension; diabetes complications (cardiovascular diseases, peripheral vascular disease, peripheral neuropathy, diabetic nephropathy, and diabetic retinopathy); blood glucose (glycated hemoglobin [HbA1c] and fasting blood glucose); blood lipids (total cholesterol, triglyceride, high-density lipoprotein, and low-density lipoprotein); liver function (aspartate aminotransferase and alanine aminotransferase [ALT]); and renal function (blood urea nitrogen, creatinine).
- Psychological factors: Self-Rating Depression Scale (SDS), which was compiled by Zung in 1965 and revised by Wang et al, consists of 20 items for a total of 80 points, with a score of 53 points set as the threshold for depression, A score of less than 53 means no depression.22,23 SDS has good reliability and validity and can accurately reflect the subjective depression of self-raters in the previous week.24
- Self-management factors: The Diabetes Self-care Scale (DSCS), which was compiled by Hurley and revised by Wang et al from Taiwan, has good internal consistency (Cronbach alpha = 0.87).25 The scale has 26 items, including 6 dimensions (diet management, blood glucose monitoring, foot care, exercise, medication according to doctor’s orders, and prevention and treatment of high and low blood sugar, with a higher score representing better self-management behavior).26
- Social support factors: Social Support Rating Scale (SSRS) was developed by Shuiyuan Xiao in 1986 and revised in 1990.27 The 10-item scale consists of 3 dimensions (subjective support, objective support, and support utilization, with a higher score representing better self-management behavior). The scale has presented great validity and reliability in Chinese population.28,29
Cognitive Assessment
Cognitive impairment was evaluated with the Chinese version of the Montreal Cognitive Assessment (MoCA), which has been validated in previous studies and takes into account the cultural and socioeconomic conditions of the Chinese population so that all question items can be easily understood and answered.30–32 The Chinese version of MoCA has good criterion-related validity (Pearson correlation coefficient MoCA vs MMSE = 0.933) and reliable internal consistency (Cronbach alpha = 0.818), consistent with the original version (Pearson correlation coefficient MoCA vs MMSE = 0.87 and Cronbach alpha = 0.83).32 The test has 12 question items, with the total score ranging from 0 to 30. Each item was assigned 1 point for a correct answer and 0 points for incorrect or unknown answers. If the participant had ≤12 years of education, 1 point was added to the overall MoCA score. An overall score <26 indicated cognitive impairment.
Statistical Analysis
We used SPSS v21.0 software (IBM, Armonk, NY, USA) for data analysis. Normally distributed continuous data are described as mean and standard deviation, with the independent t-test used for intergroup comparisons. Discrete data are described as frequency, composition ratio, or percentage, and the chi-squared and Mann–Whitney U-tests were used for intergroup comparisons. Variables with p < 0.1 in these tests were input into the multivariate logistic regression model to identify predictors of cognitive impairment. All findings from the regression modeling are reported as odds ratio with 95% confidence interval. All significant P values (P < 0.05) were 2-tailed.
Results
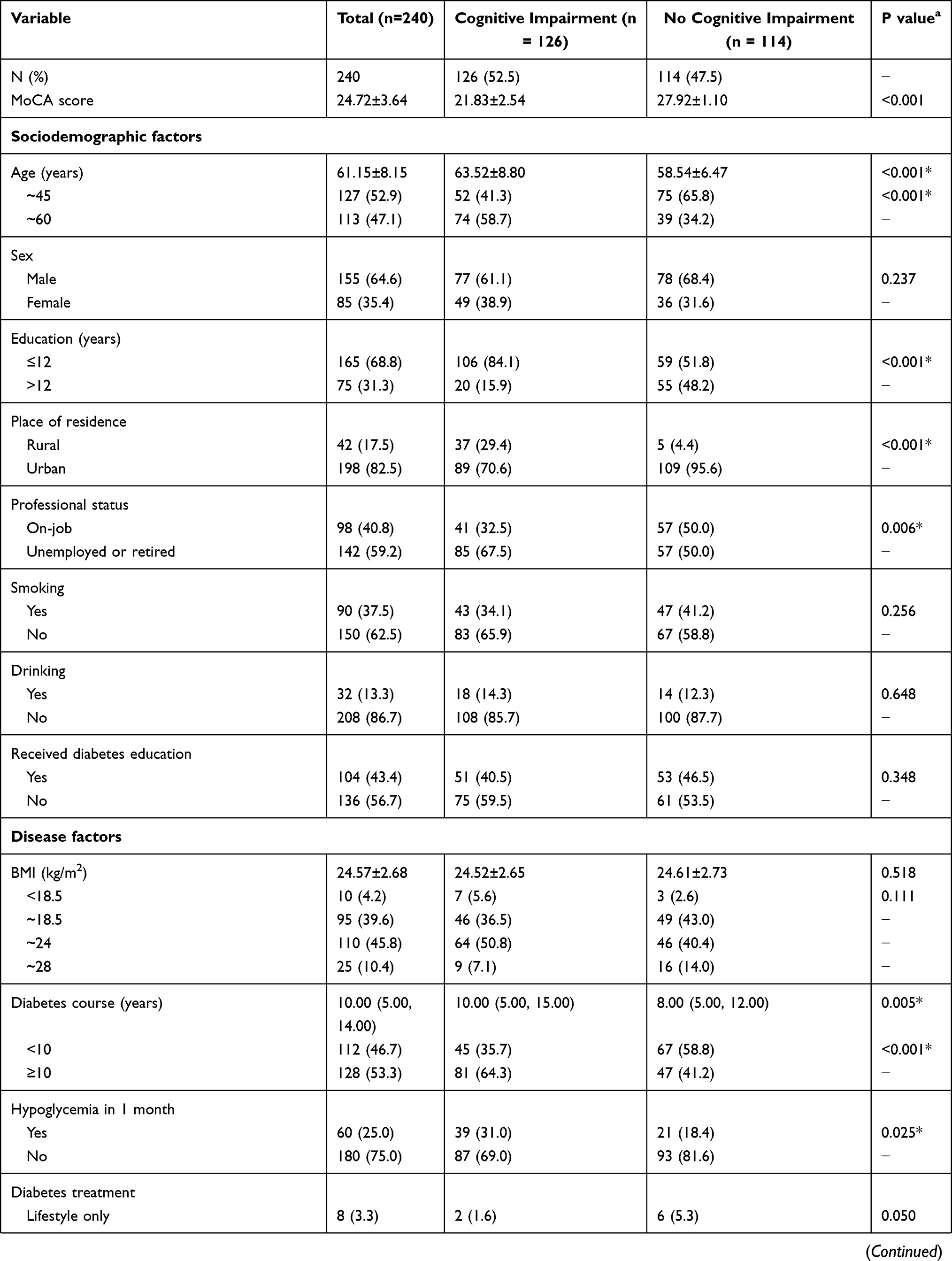
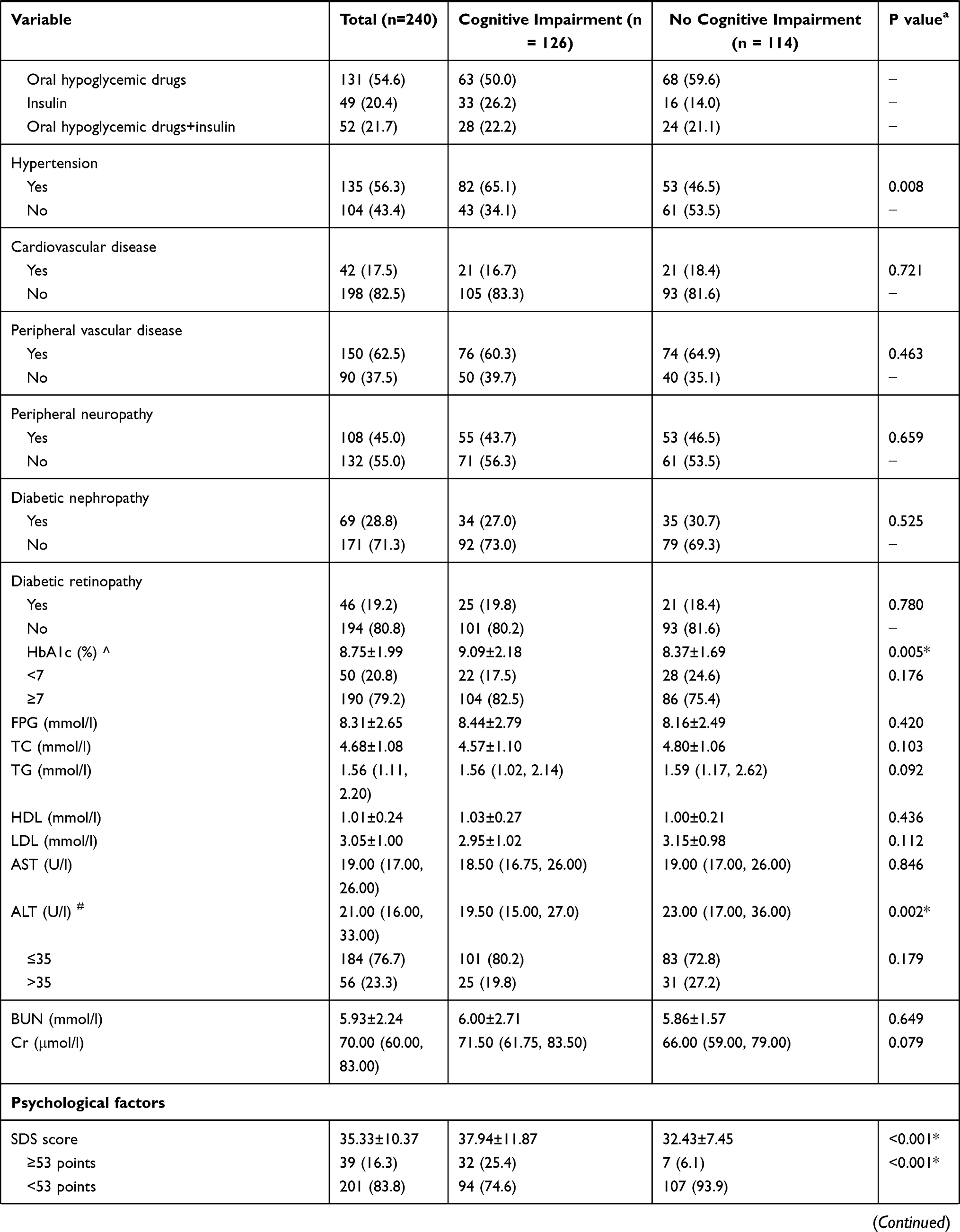
Baseline characteristics of the participants with and without cognitive impairment are shown in Table 1. The average age of the participants was 61.15 ± 8.15 years; 127 (52.9%) were middle-aged and 113 (47.1%) were elderly. The majority (64.6%) were male, and 82.5% lived in cities, and 53.3% had had diabetes for more than 10 years. A total of 60 participants had a history of hypoglycemia within 1 month and 79.2% had HbA1c ≥7%, with poor blood glucose control. The average MoCA score was 24.72 ± 3.64; 126 (52.5%) patients with a MoCA score <26 were classified as having cognitive impairment.
 |
 |
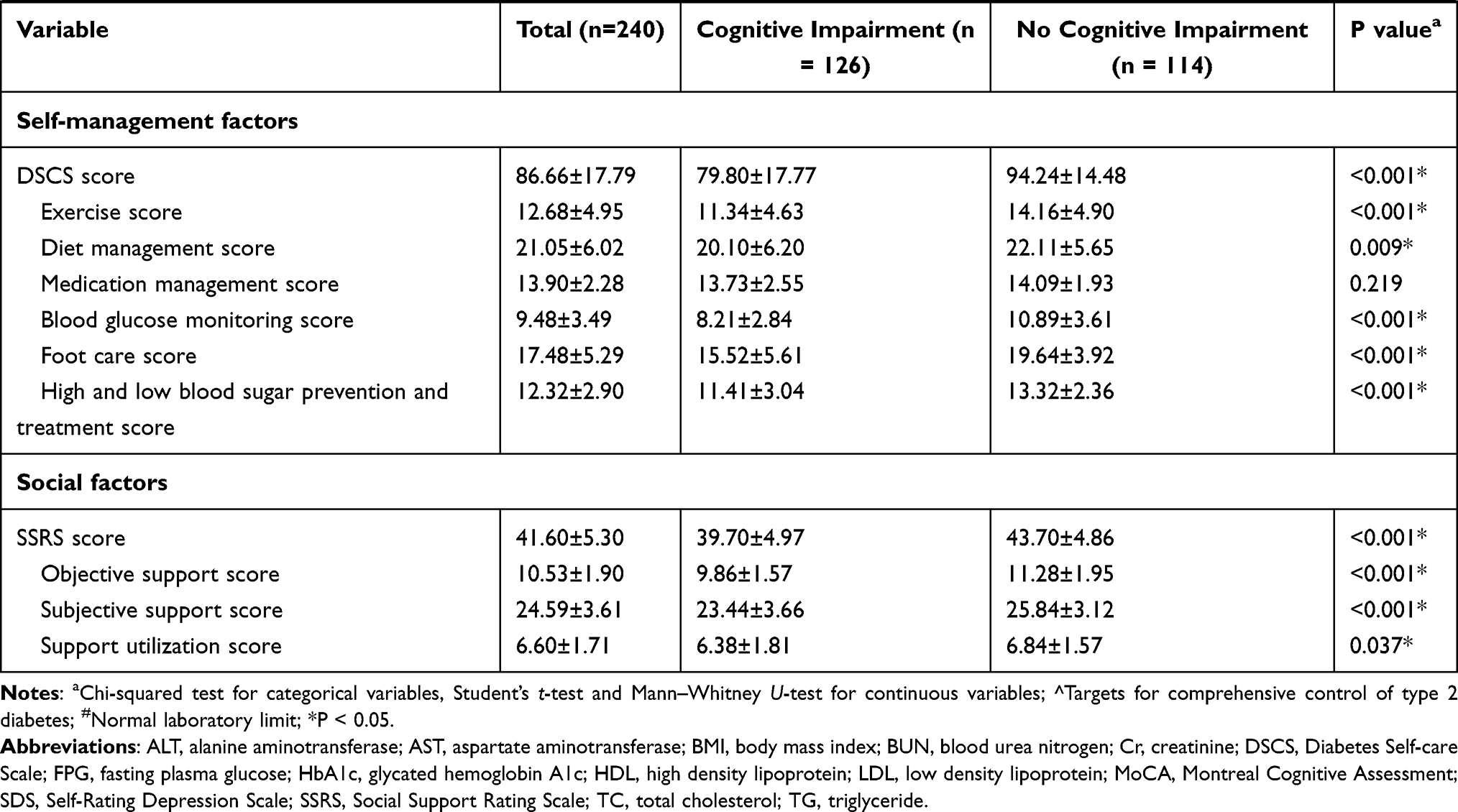 |
Table 1 Sociodemographic, Disease, Psychological, Self-Management, and Social Support Factors at Baseline Stratified by Cognitive Impairment |
In the biomedical dimension, participants with cognitive impairment were older, less educated, and more likely to live in rural areas and be unemployed than those with normal cognition. In terms of disease factors, participants with cognitive impairment had a longer course of diabetes, history of hypoglycemia within 1 month, high blood pressure, elevated HbA1c, and lower ALT. In the psychological dimension, 39 participants were determined to be depressed; participants with cognitive impairment had higher SDS scores. In the social behavior and self-management dimensions, participants with cognitive impairment had lower total scores on the DSCS and SSRS and lower scores on each dimension of these tests than those with normal cognition.
The results of the multivariate logistic regression analysis showed that older age, a history of hypoglycemia within 1 month, and depression were independent risk factors for cognitive impairment. Having > 12 years of education, urban living, and a higher total score on the DSCS were independent factors that protected against cognitive impairment. Professional status, diabetes course, combined hypertension, HbA1c, ALT, and SSRS score were not associated with cognitive impairment in the multivariate model (Table 2).
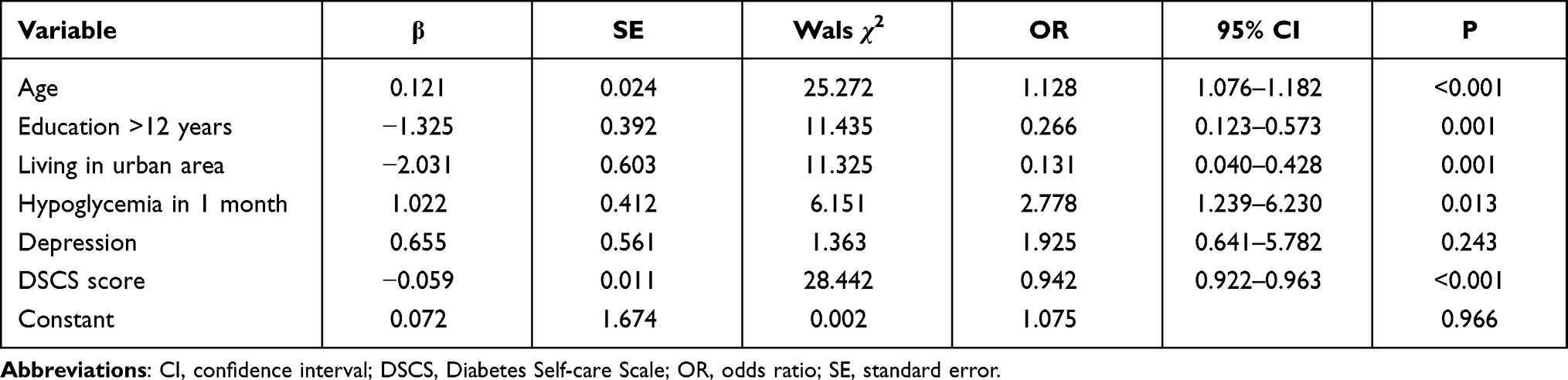 |
Table 2 Multivariate Logistic Regression Analysis of Cognitive Impairment in Patients with Type 2 Diabetes |
Discussion
In this study, we found that middle-aged and elderly patients with T2DM had high rates of cognitive dysfunction, which may be related to the use of only one instrument (MoCA) for evaluation. We also found older age, a history of hypoglycemia, and depression were independent risk factors for cognitive impairment whereas a higher education level, urban life, and better self-management were independent protective factors.
Our assumption was that biomedical and psychological factors and social behaviors all influence cognitive function. In the biomedical dimension, T2DM patients who were older, less educated, lived in rural areas, and had a history of hypoglycemia were at greater risk of cognitive impairment. This is in agreement with previous studies that have reported older age as a risk factor for cognitive impairment.33,34 Cognitive function declines with age; this is accelerated and is exacerbated in patients with diabetes compared to those without diabetes.35 Cognitive dysfunction in patients with T2DM was found to be 2.5 times more common in patients between 66 and 80 years of age than in those in the 40–60 age group.36 This may be attributable to the emergence of vascular changes and neurodegeneration in the brain with aging.37
Education level and place of residence have been shown to impact cognitive function.19,38 The results of a 21-year cohort study showed that people with a higher education level and who engaged in mental activities had a lower risk of cognitive impairment in old age,39 possibly because regular stimulation of neurons preserves their functioning over a long period of time. One study of 2017 elderly people reported a higher prevalence of cognitive impairment in rural residents.40 This may be because compared to life in an urban setting, rural living is more monotonous with less information and stimulation from the outside world.
The relationship between hypoglycemia and cognitive impairment in T2DM patients is controversial. Some studies have shown that hypoglycemia in patients with T2DM leads to impaired brain function and an increased rate of cognitive decline.41,42 However, others have reported no association between the risk of hypoglycemia and a decline in cognitive function or quality of life.34,43 The inclusion of the participants’ history of hypoglycemia into the regression model in our study underscored the importance of preventing this condition in the treatment of diabetes; safer treatments should be prescribed based on individual cases and health education concerning hypoglycemia is needed for patients. Meanwhile, clinicians should be aware of the increased risk of cognitive decline in patients with a history of hypoglycemia.
In the psychological dimension, depression was a risk factor for cognitive impairment in patients with T2DM. This is consistent with previous reports that individuals with comorbid T2DM and depression had a higher risk of cognitive impairment than those with either condition alone.44,45 Depression has been shown to promote the progression of MCI to dementia38 and can lead to poor blood glucose control and blood vessel and nerve damage, resulting in cognitive impairment. Thus, more attention should be paid to the mental health of patients with T2DM, and those exhibiting negative emotions or depressive tendencies should receive timely and appropriate treatment.
In the social behavior dimension, better self-management ability was a protective factor against cognitive impairment. This is in accordance with an earlier study in which cognitive impairment in patients with diabetes was found to be linked to poor medication management and glucose self-monitoring.21 The exercise and diet dimensions of self-management behavior are closely related to cognitive impairment.20 T2DM patients with good self-management also have more stable blood glucose, which may reduce the toxic effect of hyperglycemia on the central nervous system. Exercise directly excites the cerebral cortex, which could help to maintain nerve cells and synaptic function.
In the present study, the scores of each dimension of DSCs showed that “blood glucose monitoring” was at a low level; “Exercise”, “diet management”, “foot care”, “high and low blood sugar prevention and treatment” were at a medium level; “Medication management” was at a high level. It was suggested that the self blood glucose monitoring behavior of the participants in this study was not ideal. We should pay attention to the guidance and education of self blood glucose monitoring to help the patients master the correct knowledge and technology; Strengthen life guidance and formulate individualized exercise and diet programs; Emphasize the relationship between self-management and cognitive impairment. We also found that over half of the patients reported that they had not received comprehensive education on diabetes; in order to mitigate the risk of developing cognitive deficits, T2DM patients should be educated about diabetes and self-management behaviors.
In this study, we considered the comprehensive impact of factors of different dimensions on patients, and determined the risk factors for cognitive impairment in patients with T2DM, and emphasized the importance of long-term rational control of blood glucose, mood pleasure and good self-management. Our findings help clinicians or diabetes specialist nurses quickly identify T2DM patients with high risk of cognitive impairment and provide evidence for cognitive function screening in T2DM patients. High risk patients will benefit from more targeted lifestyle interventions, such as exercise, diet, hypoglycemia health education and stress reduction,46,47 which will help to prevent and delay the decline of cognitive function in T2DM patients. A limitation of our study was the cross-sectional design, which made it difficult to establish a causal relationship between specific risk factors and cognitive impairment; additionally, as there were no healthy middle-aged and elderly as a control group, we were unable to determine the precise relationship between diabetes and cognitive function. We will continue to follow up the participants in this study and at the same time expand the sample size in order to obtain more conclusive results.
Conclusions
We investigated the risk factors for cognitive impairment in 240 middle-aged and elderly patients with T2DM by assessing their cognitive function and influencing factors through questionnaires, along with depression status, self-management behavior, and social support. Patients with T2DM who are older, less educated, living in rural areas, have hypoglycemia history, and have poor self-management of diabetes are at increased risk of cognitive impairment; controlling hypoglycemia, detecting and treating depression as early as possible, and improving self-management capabilities are important for preventing cognitive decline in this group. Our study provides a basis for medical care personnel to early identify T2DM patients with high risk of cognitive impairment and carry out follow-up cognitive function screening, and provides theoretical support for the formulation of prevention and intervention measures for T2DM patients with cognitive impairment.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Medical Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University.
Consent
The patients provided written informed consent for participation in this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. Weiran Xu and Xiling Hu contributed equally to this work.
Funding
This study was funded by the Guangdong Basic and Applied Basic Research Foundation (2020A1515110195), and the Cultivation Project of National Natural Science Foundation of the Third Affiliated Hospital of Sun Yet-sen University (2021GZRPYQN06).
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF diabetes atlas, ninth edition 2019. Brussels, Belgium; 2019. Available from: https://www.diabetesatlas.org.
2. Harding JL, Pavkov ME, Magliano DJ, et al. Global trends in diabetes complications: a review of current evidence. Diabetologia. 2019;62(1):3–16. doi:10.1007/s00125-018-4711-2
3. Mccrimmon RJ, Ryan CM, Frier BM. Diabetes and cognitive dysfunction. Lancet. 2012;379(9833):2291–2299. doi:10.1016/S0140-6736(12)60360-2
4. Valenza S, Paciaroni L, Paolini S, et al. Mild cognitive impairment subtypes and type 2 diabetes in elderly subjects. J Clin Med. 2020;9(7):2055. doi:10.3390/jcm9072055
5. Gao Y, Xiao Y, Miao R, et al. The prevalence of mild cognitive impairment with type 2 diabetes mellitus among elderly people in China: a cross-sectional study. Arch Gerontol Geriatr. 2016;62:138–142. doi:10.1016/j.archger.2015.09.003
6. Langa KM, Levine DA. The diagnosis and management of mild cognitive impairment: a clinical review. JAMA. 2014;312(23):2551–2561. doi:10.1001/jama.2014.13806
7. Xu W, Caracciolo B, Wang HX, et al. Accelerated progression from mild cognitive impairment to dementia in people with diabetes. Diabetes. 2010;59(11):2928–2935. doi:10.2337/db10-0539
8. Cooper C, Sommerlad A, Lyketsos CG, et al. Modifiable predictors of dementia in mild cognitive impairment: a systematic review and meta-analysis. Am J Psychiatry. 2015;172(4):323–334. doi:10.1176/appi.ajp.2014.14070878
9. Boylen PA, Wilson RS, Aggarwal NT, et al. Mild cognitive impairment: risk of Alzheimer disease and rate of cognitive decline. Neurology. 2006;67(3):441–445. doi:10.1212/01.wnl.0000228244.10416.20
10. Hou Q, Guan Y, Yu W, et al. Associations between obesity and cognitive impairment in the Chinese elderly: an observational study. Clin Interv Aging. 2019;14:367–373. doi:10.2147/CIA.S192050
11. Dybjer E, Nilsson PM, Engstrom G, et al. Pre-diabetes and diabetes are independently associated with adverse cognitive test results: a cross-sectional, population-based study. BMC Endocr Disord. 2018;18(1):91. doi:10.1186/s12902-018-0318-3
12. Sullivan MD, Katon WJ, Lovato LC, et al. Association of depression with accelerated cognitive decline among patients with type 2 diabetes in the ACCORD-MIND trial. JAMA Psychiatry. 2013;70(10):1041–1047. doi:10.1001/jamapsychiatry.2013.1965
13. Uchmanowicz I, Jankowska-Polanska B, Mazur G, et al. Cognitive deficits and self-care behaviors in elderly adults with heart failure. Clin Interv Aging. 2017;12:1565–1572. doi:10.2147/CIA.S140309
14. Fu C, Li Z, Mao Z. Association between social activities and cognitive function among the elderly in China: a Cross-Sectional Study. Int J Environ Res Public Health. 2018;15(2):231. doi:10.3390/ijerph15020231
15. Xue M, Xu W, Ou Y-N, et al. Diabetes mellitus and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 144 prospective studies. Ageing Res Rev. 2019;55:e100944. doi:10.1016/j.arr.2019.100944
16. Mansur RB, Lee Y, Zhou AJ, et al. Determinants of cognitive function in individuals with type 2 diabetes mellitus: a meta-analysis. Ann Clin Psychiatry. 2018;30(1):38–50.
17. Marioni RE, Strachan MW, Reynolds RM, et al. Association between raised inflammatory markers and cognitive decline in elderly people with type 2 diabetes: the Edinburgh Type 2 Diabetes Study. Diabetes. 2010;59(3):710–713. doi:10.2337/db09-1163
18. Sun L, Diao X, Gang X, et al. Risk factors for cognitive impairment in patients with type 2 diabetes. J Diabetes Res. 2020;2020:e4591938. doi:10.1155/2020/4591938
19. Xiu S, Liao Q, Sun L, et al. Risk factors for cognitive impairment in older people with diabetes: a community-based study. Ther Adv Endocrinol Metab. 2019;10:e2042018819836640. doi:10.1177/2042018819836640
20. Feil DG, Zhu CW, Sultzer DL. The relationship between cognitive impairment and diabetes self- management in a population-based community sample of older adults with type 2 diabetes. J Behav Med. 2012;35(2):190–199. doi:10.1007/s10865-011-9344-6
21. Kim KJ, Fritschi C. Relationships between cognitive impairment and self-management in older adults with type 2 diabetes: an integrative review. Res Gerontol Nurs. 2021;14(2):104–112. doi:10.3928/19404921-20201117-01
22. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
23. Wang CF, Cai ZH, Xu Q. Analysis of self-rating depression scale - SDS in 1340 normal subjects. Chin J Nerv Ment Dis. 1986;5:267–268.
24. Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the zung scales. BMC Psychiatry. 2017;17(1):329. doi:10.1186/s12888-017-1489-6
25. Wang JX, Wang RX, Lin QJ. Self-care behaviors and related factors in outpatients newly diagnosed with non-insulin-dependent diabetes mellitus. J Nurs. 1998;45(2):60–74.
26. Hurley AC, Shea CA. Self-efficacy: strategy for enhancing diabetes self-care. Diabetes Educ. 1992;18(2):146–150. doi:10.1177/014572179201800208
27. Xiao SY. Theoretical basis and research application of ‘social support rating scale’. J Clin Psychiatry. 1994;4(2):98–100.
28. Yu Y, Yang JP, Shiu CS, et al. Psychometric testing of the Chinese version of the Medical Outcomes Study social support survey among people living with HIV/AIDS in China. Appl Nurs Res. 2015;28(4):328–333. doi:10.1016/j.apnr.2015.03.006
29. Liu JW, Li FY, Lian YL. Reliability and validity of social support rating scale. J Xinjiang Med Univ. 2008;1:4–6.
30. Hoops S, Nazem S, Siderowf AD, et al. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology. 2009;73(21):1738–1745. doi:10.1212/WNL.0b013e3181c34b47
31. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
32. Zhang LX, Liu XQ. A study on reliability and validity of MoCA scale of Chinese version. Chin Nurs Res. 2007;31:2906–2907.
33. Wong M, Tan CS, Venketasubramanian N, et al. Prevalence and risk factors for cognitive impairment and dementia in Indians: a Multiethnic Perspective from a Singaporean Study. J Alzheimers Dis. 2019;71(1):341–351. doi:10.3233/JAD-190610
34. Nathan DM. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37(1):9–16. doi:10.2337/dc13-2112
35. Petermann F, Troncoso-Pantoja C, Martínez MA, et al. Risk of cognitive impairment among older people with diabetes or family history of the disease. Rev Med Chil. 2018;146(8):872–881. doi:10.4067/s0034-98872018000800872
36. Kinoshita T, Shimoda M, Sanada J, et al. Association of GA/HbA1c ratio and cognitive impairment in subjects with type 2 diabetes mellitus. J Diabetes Complications. 2016;30(8):1452–1455. doi:10.1016/j.jdiacomp.2016.08.008
37. Biessels GJ, Strachan MW, Visseren FL, et al. Dementia and cognitive decline in type 2 diabetes and prediabetic stages: towards targeted interventions. Lancet Diabetes Endocrinol. 2014;2(3):246–255. doi:10.1016/S2213-8587(13)70088-3
38. Li W, Sun L, Li G, et al. Prevalence, influence factors and cognitive characteristics of mild cognitive impairment in type 2 diabetes mellitus. Front Aging Neurosci. 2019;11:180. doi:10.3389/fnagi.2019.00180
39. Anttila T, Helkala EL, Kivipelto M, et al. Midlife income, occupation, APOE status, and dementia: a population-based study. Neurology. 2002;59(6):887–893. doi:10.1212/wnl.59.6.887
40. Han R, Tang Z, Ma L. Related factors of cognitive impairment in community-dwelling older adults in Beijing Longitudinal Study of aging. Aging Clin Exp Res. 2019;31(1):95–100. doi:10.1007/s40520-018-0943-8
41. Whitmer RA, Karter AJ, Yaffe K, et al. Hypoglycemic episodes and risk of dementia in older patients with type 2 diabetes mellitus. JAMA. 2009;301(15):1565–1572. doi:10.1001/jama.2009.460
42. Languren G, Montiel T, Ramírez-Lugo L, et al. Recurrent moderate hypoglycemia exacerbates oxidative damage and neuronal death leading to cognitive dysfunction after the hypoglycemic coma. J Cereb Blood Flow Metab. 2019;39(5):808–821. doi:10.1177/0271678X17733640
43. Cukierman-Yaffe T, Bosch J, Jung H, et al. Hypoglycemia and incident cognitive dysfunction: a post hoc analysis from the ORIGIN trial. Diabetes Care. 2019;42(1):142–147. doi:10.2337/dc18-0690
44. Xiu S, Zheng Z, Liao Q, et al. Different risk factors for cognitive impairment among community- dwelling elderly, with impaired fasting glucose or diabetes. Diabetes Metab Syndr Obes. 2019;12:121–130. doi:10.2147/DMSO.S180781
45. Black S, Kraemer K, Shah A, et al. Diabetes, depression, and cognition: a recursive cycle of cognitive dysfunction and glycemic dysregulation. Curr Diab Rep. 2018;18(11):118. doi:10.1007/s11892-018-1079-0
46. Iessels GJ, Whitmer RA. Cognitive dysfunction in diabetes: how to implement emerging guidelines. Diabetologia. 2020;63(1):3–9. doi:10.1007/s00125-019-04977-9
47. Srikanth V, Sinclair AJ, Hill-Briggs F, et al. Type 2 diabetes and cognitive dysfunction-towards effective management of both comorbidities. Lancet Diabetes Endocrinol. 2020;8(6):535–545. doi:10.1016/S2213-8587(20)30118-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.