Back to Journals » Psychology Research and Behavior Management » Volume 16
Cognitive Functions, Depressive and Anxiety Symptoms After One Year of CPAP Treatment in Obstructive Sleep Apnea
Authors Vanek J ![]() , Prasko J
, Prasko J ![]() , Genzor S
, Genzor S ![]() , Belohradova K, Visnovsky J
, Belohradova K, Visnovsky J ![]() , Mizera J
, Mizera J ![]() , Bocek J
, Bocek J ![]() , Sova M
, Sova M ![]() , Ociskova M
, Ociskova M ![]()
Received 21 March 2023
Accepted for publication 22 May 2023
Published 21 June 2023 Volume 2023:16 Pages 2253—2266
DOI https://doi.org/10.2147/PRBM.S411465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Jakub Vanek,1 Jan Prasko,1– 4 Samuel Genzor,5 Kamila Belohradova,1 Jozef Visnovsky,1 Jan Mizera,5 Jonas Bocek,1 Milan Sova,5,6 Marie Ociskova1,4
1Department of Psychiatry, Faculty of Medicine and Dentistry of Palacky University, Olomouc, the Czech Republic; 2Institute for Postgraduate Education in Health Care, Prague, The Czech Republic; 3Department of Psychology Sciences, Faculty of Social Science and Health Care of Constantine the Philosopher University, Nitra, the Slovak Republic; 4Jessenia Inc. - Rehabilitation Hospital, Akeso Holding, Beroun, the Czech Republic; 5Department of Respiratory Medicine, Faculty of Medicine and Dentistry of Palacky University, Olomouc, the Czech Republic; 6Department of Respiratory Medicine, University Hospital and Faculty of Medicine of Masaryk University, Brno, the Czech Republic
Correspondence: Jan Prasko, Department of Psychiatry, University Hospital Olomouc and Faculty of Medicine and Dentistry, Palacky University Olomouc, I. P. Pavlova 6, Olomouc, 77520, the Czech Republic, Tel +420 603 414 930, Email [email protected]
Objective: The study worked with depressive symptoms, anxiety score and cognitive functions in obstructive sleep apnea (OSA) patients treated with CPAP.
Methods: Eighty-one subjects with OSA and without psychiatric comorbidity were treated with CPAP for one year and completed the following scales and cognitive tests: Trail Making Test, Verbal Fluency Test, d2 Test, Beck Depression Inventory-II and Beck Anxiety Inventory. MINI ruled out psychiatric disorder. At the two months check-up, subjects were re-evaluated for depressive and anxiety symptoms, and after one year of CPAP treatment, subjects repeated cognitive tests and scales. Data about therapy adherence and effectiveness were obtained from the patient’s CPAP machines.
Results: The study was completed by 59 CPAP adherent patients and eight non-adherent patients. CPAP therapy effectiveness was verified in all patients by decreasing the apnea-hypopnoea index below 5 and/or 10% of baseline values. The adherent patients significantly improved depressive and anxiety symptoms. There was also an improvement in overall performance in the attention test; however, performance in many individual items did not change. The adherent patients also improved verbal fluency and in the Part B of the Trail making test. The non-adherent group significantly increased the number of mistakes made in the d2 test; other results were non-significant.
Conclusion: According to our results, OSA patients’ mood, anxiety and certain cognitive domains improved during the one-year therapy with CPAP.
Trial Registration Number: NCT03866161.
Keywords: obstructive sleep apnoea, depression, cognitive functions, CPAP treatment, treatment efficacy, Trail Making Test, Verbal Fluency Test
Introduction
Obstructive sleep apnea (OSA) is the most frequent syndrome in the spectrum of sleep-disordered breathing. It is characterized by the presence of repeated airflow limitations throughout sleep. The closing of airways and the decrease in saturation are associated with the stress reaction of the sleeping organism via the sympathetic nervous system.1 OSA results in significant changes in sleep architecture subjective and objective sleep parameters. Subjective sleep quality is poor in OSA patients.1 Objectively, OSA disrupts sleep continuity and reduces total sleep time and sleep effectivity. Direct consequences are disrupted sleep architecture and continuity and increase of N1 sleep. Another consequence is the presence of repeated arousals related to the respiratory effort.1
According to epidemiological studies, the average pooled prevalence of OSA is usually referred in 34% of males and 17% of females in adult population.2,3 Symptomatic OSA is present in 6% of males and 4% of females.3 The literature established the link between OSA and cardiovascular diseases (OSA is the most common basis for treatment-resistant hypertension) and glucose and lipid metabolism disorders.4,5
Mood Disorders in OSA
Besides other medical and psychosocial conditions, OSA is often connected with depressive symptoms.6,7 The current knowledge about the psychological aspects of OSA is ambiguous. Several investigators have stated that individuals with OSA do not usually show a clinically significant degree of depressive symptoms or that they are no more depressed than controls or other patients with chronic illnesses.8–13 On the other hand, many investigations have recognized a significant association between OSA and clinical depression or pronounced depressive symptoms either as a direct outcome of the sleep deprivation or secondarily as a consequence of social impacts of the syndrome (or both).3,14–23
Some studies have also aimed to measure the properties of the relationship between depression, excessive daytime sleepiness (EDS), and OSA and proposed that depression is more likely be more related to EDS rather than to OSA.4,10 Conversely, OSA can initiate depressive disorder based on sleep fragmentation, insomnia, and cognitive alterations brought by recurrent hypoxemia, while sleep disruption and weight increase caused by depression could, in turn, aggravate OSA, closing the vicious circle.11,24 Furthermore, the signs of OSA can mimic the signs of depression, eg, fatigue, sleep disruption, reduced volition and decision capacity, cognitive disturbances, and a lower quality of life.25,26
Cognitive Dysfunctions in OSA
A number of studies have examined the cognitive functions of subjects with OSA, and a meta-analysis assessed neurocognitive functions in OSA patients as well.11,27,28 Published investigations have recognized attention, episodic memory, working memory, and executive functioning are the most impacted cognitive functions in patients, while most verbal functions remained preserved and mixed outcomes were found for psychomotor speed.29–45
Several investigations have confirmed that OSA patients show deficiencies in all three domains of attention – sustainability, selectivity, and division.38,42,46 A meta-review confirmed these observations.27,47 Given the degree and magnitude of impairment, it has been proposed that issues with vigilance and attention may perhaps impact other intellectual functions.35,42,46
Executive functions are proposed as one of the main cognitive areas influenced by OSA. A contemporary meta-analysis suggests that executive functioning is decreased in OSA in all five subdomains: inhibition, shifting, updating/monitoring information, producing original knowledge and reasoning, and problem-solving.27,47 Working memory is another significant cognitive function consisting of the capability to remember, operate, revise, and work with information for the length of a job. Studies showed that the OSA subjects have worse results in working memory tasks than controls.48–50 Certain executive features of verbal performance, such as processing speed, plasticity, and synthetic skills are also reduced in subjects with OSA, in spite of intact verbal skills.29,33,47,48
In subjects with OSA, a decrease in manual dexterity was described and fine motor coordination is established to be more vulnerable to prolonged hypoxemia rather than to sleep disturbances.29,34,48,50,51 A literature evaluation demonstrated that half of the available investigations described that the patients with OSA had a decreased information managing speed compared to control subjects.45,52 This impaired information managing affects performances in cognitive tests and visual attention. Unsurprisingly, the OSA patients are worse than healthy controls in timed tasks that consist of a visuomotor synchronization.53
Episodic memory, the capability to memorize verbal or visual data in a spatiotemporal context, was widely studied among OSA patients.54,55 A meta-review presented that OSA subjects had various samples of insufficiencies in verbal and visual episodic memory. Each memory component was impaired for verbal material, namely instant and late recall, understanding and identification.56 Nevertheless, in visuospatial memory tests, the OSA patients presented weakening only in instant and late recalls and had normal scores for learning and identification.56,57 It was proposed that this disturbance is not completely described by reduced attention or the OSA seriousness.26,58
Therapy of OSA
Continuous positive airway pressure (CPAP) resolves all OSA signs by maintaining the upper airways open utilizing the air pressure, which causes a decline of hypoxemia and restores sleep architecture and is considered a standard treatment for moderate and severe surgically untreatable OSA.59,60
Influence of Treatment by CPAP on Depressive Symptoms
The review by Giles et al claimed that the outcomes of the OSA therapy on depressive signs are partial and vary amongst studies due to high heterogeneity of the samples and methodology.61 Povitz et al, in a meta-analysis of nineteen identified papers, concluded that CPAP therapy resulted in a decline in symptoms of depression compared to controls with major heterogeneity between trials.62 The results were and still are conflicting, and studies supporting both variants can be found.19,59,61,63 Several studies showed that the presence of depressive symptomatology was not affected by treatment with CPAP, and it was necessary to intervene with targeted antidepressant therapy. Another group of studies demonstrated that depressive symptoms partially improved or completely disappeared after CPAP treatment.11,62–64 Even in the studies mentioned above, it is problematic that they often do not distinguish between subjectively perceived depressive symptoms and a clinical diagnosis of a depressive disorder.11
Influence of Treatment by CPAP on Cognitive Functions
The CPAP therapy improves subjective daytime functioning and performance in cognitive tasks.33,48,51,65–67 Also, the CPAP treatment returns to normal electroencephalographic results (EEG) assessed during the awake time in the OSA subjects, which is connected with diminished daytime sleepiness.59,68,69 Nevertheless, CPAP must be used for minimum of 4 hours each night for a subjective impact on sleepiness and at least 6 hours each night to influence objectively measured sleepiness.70,71 Divergent from other cognitive areas, psychomotor speed and fine coordination are not enhanced with CPAP therapy, which proposes that OSA can cause enduring damage to cortical and subcortical parts responsible for motor skills.45,59,69
As for the treatability of the cognitive decline, a meta-analysis of cognitive functioning in subjects with the CPAP therapy described that eleven of the seventeen papers demonstrated a significant enhancement in vigilance and attention with CPAP.27,53 However, despite the significantly improved concentration, CPAP is frequently incapable of completely normalizing attention. These outcomes suggest that sleep fragmentation and hypoxemia partially cause attention deficits in OSA, but that OSA also might cause enduring impairment in areas of the brain used in attention.33,34,47,67 Although all mechanisms of the verbal episodic memory evaluation are impaired in OSA a 3-months CPAP therapy resulted in the normalization of performances for instant and late recall and both verbal and visuospatial learning.33,56,67
A meta-analysis demonstrated that the CPAP therapy significantly enhances executive functions.27,53 After a short CPAP treatment, studies showed improved mental flexibility and verbal fluency in OSA. Longer treatments produce mixed results in cognitive tests.33 Moreover, it was described that OSA patients are not systematically equal to the healthy adults after a three-month of CPAP or even after prolonged treatment.67 In summary, presented literature proposes that only a particular part of executive functioning recovers after a CPAP therapy and OSA patients probably never reach the level of healthy controls.33,51,67 The circumstance that further cognitive domains, such as attention and vigilance, are essential to perform most executive functioning and that OSA can result in lasting damage to the prefrontal cortex can clarify partially of the inconsistency in works examining the effects of therapy on this cognitive function.38
Aims of the Study
The objective is to test the influence of 1-year CPAP therapy on depressive and anxiety symptoms and cognitive functions in subjects with OSA. We hypothesized that treatment with the CPAP would decrease depressive and anxiety symptoms and improve cognitive functioning.
Hypotheses
- Compliant patients with OSA show decreasing depressive and anxiety symptoms assessed by the BDI-II and BAI inventories.
- Compliant patients with OSA demonstrate cognitive improvement performance:
- Trail Making Tests A and B, measured in seconds.
- Verbal Fluency test, measured in the number of words.
- d2 test, measured in overall performance (increase) and percentage error rate (decrease).
- Non-adherent patients with OSA do not improve in cognitive tests and depressive and anxiety symptoms.
Method
Participants
The inclusion and exclusion conditions for the study are described in Table 1. Participants with a diagnosed obstructive sleep apnoea referred for CPAP treatment (AHI >15) were enrolled from the patients of our Sleep Laboratory. Consecutive patients were admitted Sleep laboratory for CPAP titration before administering the treatment for home use and, at that point, were asked to participate in the study.
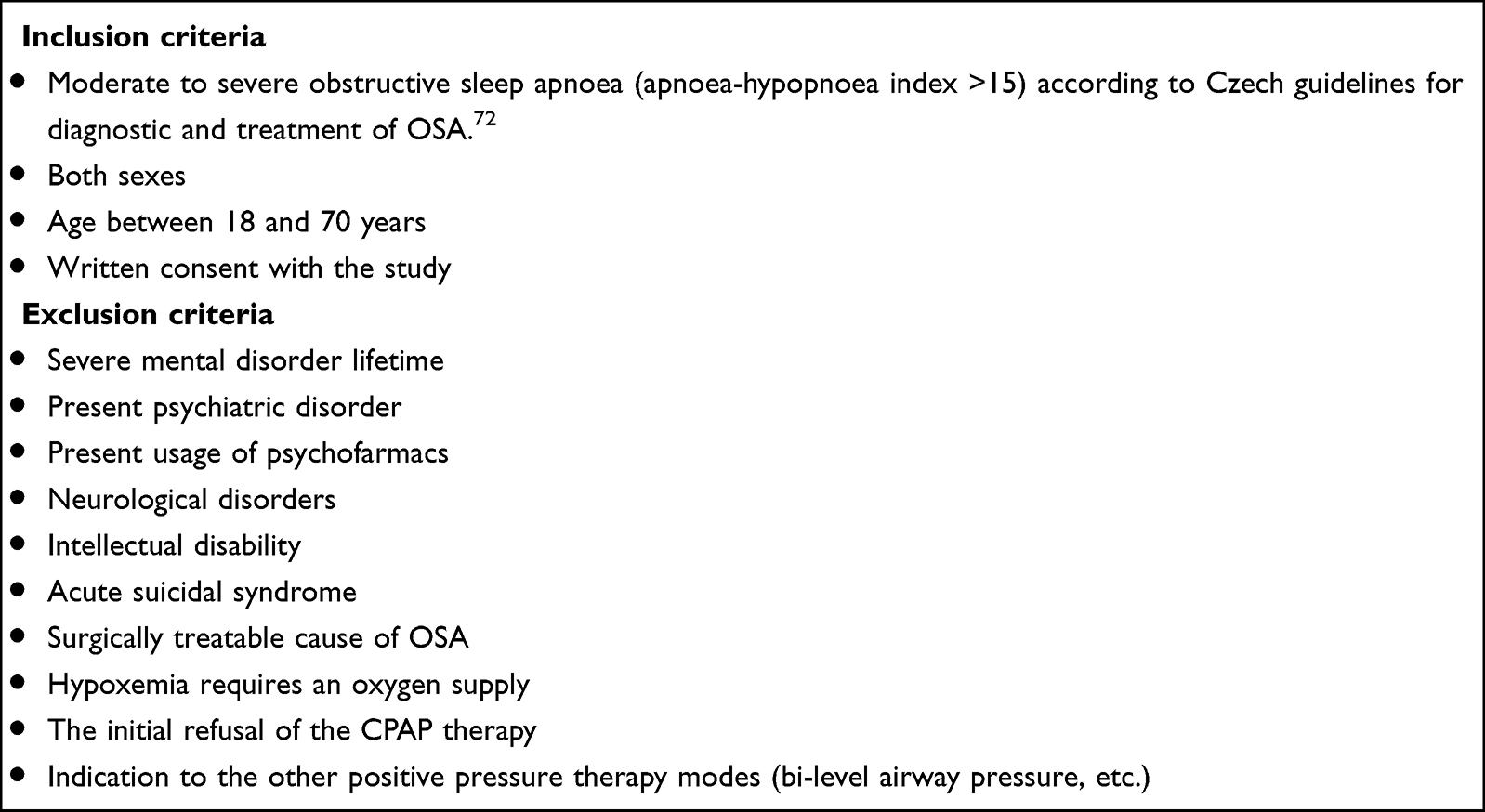 |
Table 1 Inclusion and Exclusion Criteria |
Measurements
The patients approved to take part in the study signed informed consent and underwent several cognitive tests and scales. The sleep study was performed with respiratory sleep polygraphy (Alice 6LDe, Phillips Respironics, United States). The following parameters were measured and analyzed: apnoea/hypopnoea index (AHI), number of desaturations per hour (ODI), average saturation and time spent under 90% saturation. The CPAP titration was performed by auto CPAP machine (Dreamstation Auto CPAP, Phillips Respironics, United States) for three nights according to Czech guidelines and the effectiveness of the CPAP therapy was confirmed.72 Daytime sleepiness was measured via Epworth Sleepiness Scale. All patients were also measured in weight and height; body mass index was determined, and a history of comorbid disorders was taken. Additionally, all patients were examined by a pneumologist, including awake pulse oxymetry, pulmonary function tests (spirometry + body-plethysmography) and a chest x-ray was performed to exclude another respiratory disease.
The following scales and tests were administered:
- BDI-II (Beck Depression Inventory, Second Edition) – The questionnaire contains 21 items describing depressive signs – subjects indicate symptoms and their severity throughout the last week. Internal reliability of the inventory is greater in the psychiatric population (α = 0.86) than in the general population (α = 0.81).73 The Czech translation was published by Preiss and Vacir.74 Ociskova et al did psychometric standardization for the Czech population.75
- The BAI (Beck Anxiety Inventory) scale includes 21 parts with a four-point Likert scale that the patient utilized to evaluate the gravity of anxiety symptoms last week.76 Kamaradova et al validated BAI in Czech population. The scale demonstrated excellent internal reliability (Cronbach’s alpha = 0.92).76
- d2 test of attention is a reliable and valid test for visual scanning precision, speed, and performance quality in distinguishing similar visual stimuli.77 The paper-pencil test requests participants to strike through any letter “d” with two marks around. It measures selective attention and mental concentration.78 According to a recent study, our study’s primary outcomes were a total clean score (error corrected speed score) and a percentage of mistakes, viewed as the most reliable outcomes.79
- TMT (Trail Making Test) is a neuropsychological test involving visual searching and working memory. TMT consists of Part A and Part B. Patient has to draw a line throughout 24 consecutive numbers (Part A) or alternating numbers and letters (Part B). Both parts test sustained attention, working memory and visuospatial coordination. Part A is also helpful in assessing psychomotor speed, whereas Part B considers higher executive functioning, flexibility, and the ability to switch between tasks. The test is easy to administer and is standardized with international norms. Our primary outcome was timed performance measured in seconds.80 Czech norms were conducted and standardized by Bezdicek et al.81
- VFT (Verbal Fluency Test) is a validated neuropsychological task measuring verbal cognitive functions. It can measure two subdomains – semantic and letter fluency. The patient is given one minute to name as many words as possible in a given semantic group or start with a particular letter. It has been used to assess cognitive impairment in neurodegenerative disorders in clinical settings and verbal ability and lexical retrieval in non-clinical settings.82,83 In a standardized Czech version of the test, patients were given letters N, K and P each for 1 minute. Our primary measured outcome was the number of unique words.84
- ESS (Epworth Sleepiness Scale) evaluates daytime somnolence in 8 routine circumstances in the last week. EDS is present in a score of ten or higher.85
- MINI (Mini International Neuropsychiatric Interview) is a standard diagnostic interview covering diagnostic criteria for common psychiatric disorders according to DSM-IV and ICD-10.86 The psychometric properties of the interview are acceptable.87
Procedure and Method of the Treatment
All participants underwent a standardized diagnostic procedure for OSA in the Sleep Laboratory of the Pulmonary Medicine Department at University Hospital Olomouc. The battery of tests and scales was conducted when the patients were admitted for inpatient CPAP titration in the sleep laboratory. All patients underwent the MINI interview to exclude severe psychiatric disorders.
The follow-up examination was coordinated with regular outpatient care for OSA patients with CPAP in the Czech Republic. Patients were assessed self-administered questionnaires at the check-up after two months, and the time of CPAP usage and residual AHI data were obtained. At the check-up after one year of CPAP treatment, a battery of tests and scales was conducted again, and data regarding the total time of CPAP usage and a residual AHI was obtained. The evaluation was performed in a peaceful setting with each patient separately, with a maximum exclusion of distractions. The same procedure was conducted with each patient to ensure the same conditions for both tests. The American Academy of Sleep Medicine (AASM) defined necessary adherence to the CPAP treatment as more than four hours of CPAP treatment per night.1,88
Statistics
Statistics were calculated by statistical software SPSS 24.0, Prism (GraphPad PRISM version 5.0; http://www.graphpad.com/prism/prism.htm), and G*Power (Faul et al 2007). The applied statistical procedures were descriptive statistics for mean scores and the character of data distribution. Differences between results calculated at the start and the end of the treatment were determined by parametric or nonparametric pair t-tests. Results were deemed to be significant when p-values were smaller than 0.05. The standardized effect size was calculated for the obtained results.
Ethics Statement
The study followed the latest Helsinki Declaration and the Guideline for Good Clinical Practice (EMEA 2002). The Palacky University and University Hospital’s ethical committee in Olomouc authorized the study design and written consent (approval nr. 12/19). Written informed consent was acquired from all subjects after the procedures had been fully described, and participants were not financially rewarded for their participation.
Results
Sample Description
Eighty-one consecutive OSA patients (56 men, 25 women) enrolled in the study. The average age was 54.9 ± 9.9 years, and the average BMI indicated severe obesity. The average AHI at the start of the treatment showed severe OSA in the sample. Fifty-nine patients completed the study and were adherent to the CPAP therapy. Eight patients completed the study design but were not adherent to the CPAP therapy, and their data, although limited in generalizability, were used as a quazi control group. The not adherent patients did not receive any additional therapy. Fourteen patients dropped out of the study throughout the year, and most dropouts were due to the restrictions and lockdowns given by the COVID-19 pandemic. The basic clinical data of the included patients are in Table 2.
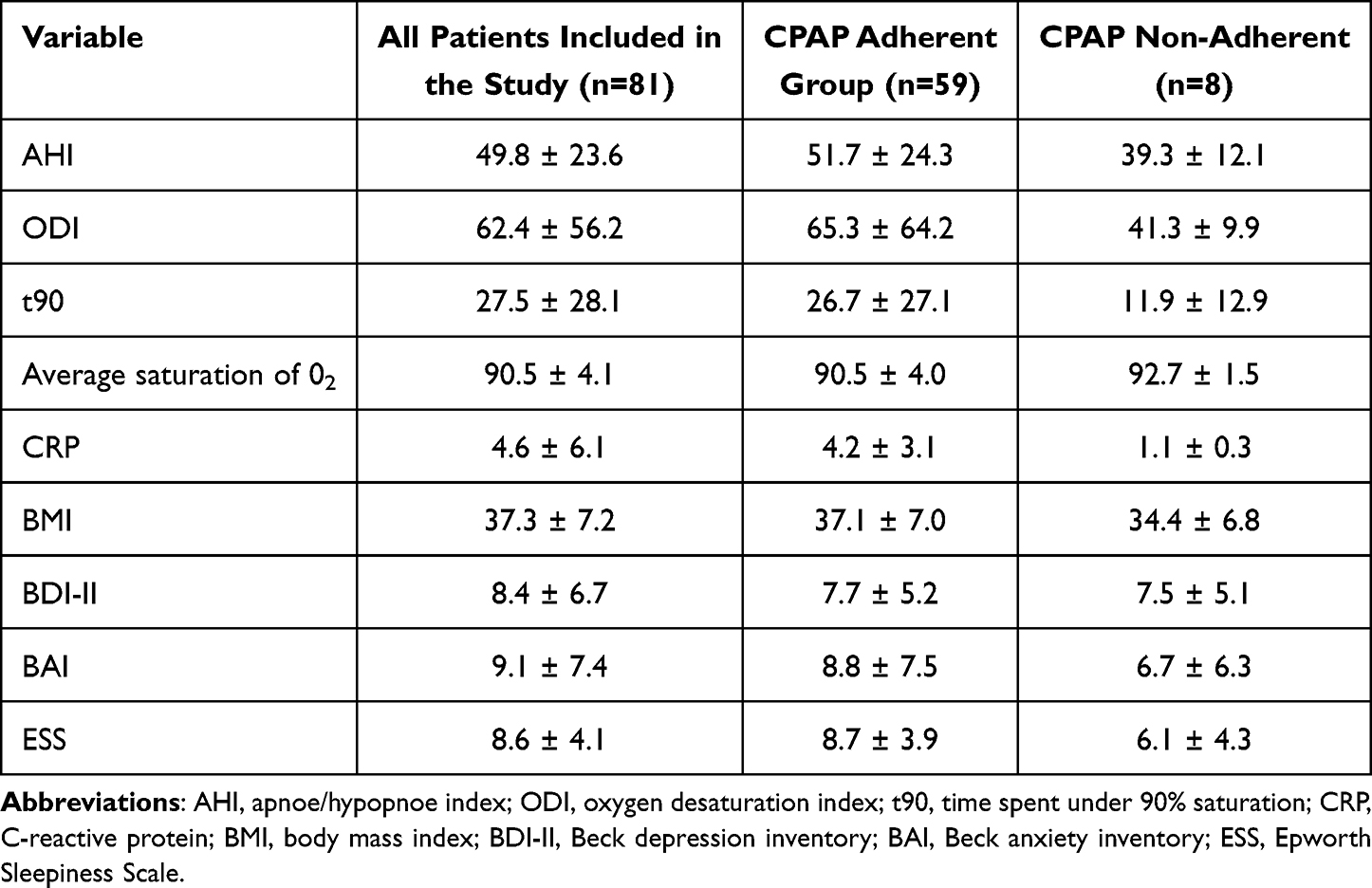 |
Table 2 Initial Measures of Patients at the Beginning of the CPAP Treatment |
We observed a statistically significant reduction in OSA parameters in the adherent group. ESS significantly decreased (p < 0.001) at two months and statistically significantly decreased (p < 0.001) at 1-year follow-up compared to the beginning. AHI very significantly decreased at two months (p < 0.0001) and at one year (p < 0.001). This indicates that the adherent group was successfully treated, and residual AHI parameters were sufficiently low. In the non-adherent group, the patients did not use/tolerate the CPAP treatment, therefore, did not reach the required usage of 4 hours/night. However, the non-adherent group had lower severity OSA parameters, including EDS measured via ESS. ESS in the non-adherent group changed non-significantly. Parameters regarding OSA are summarized in Table 3.
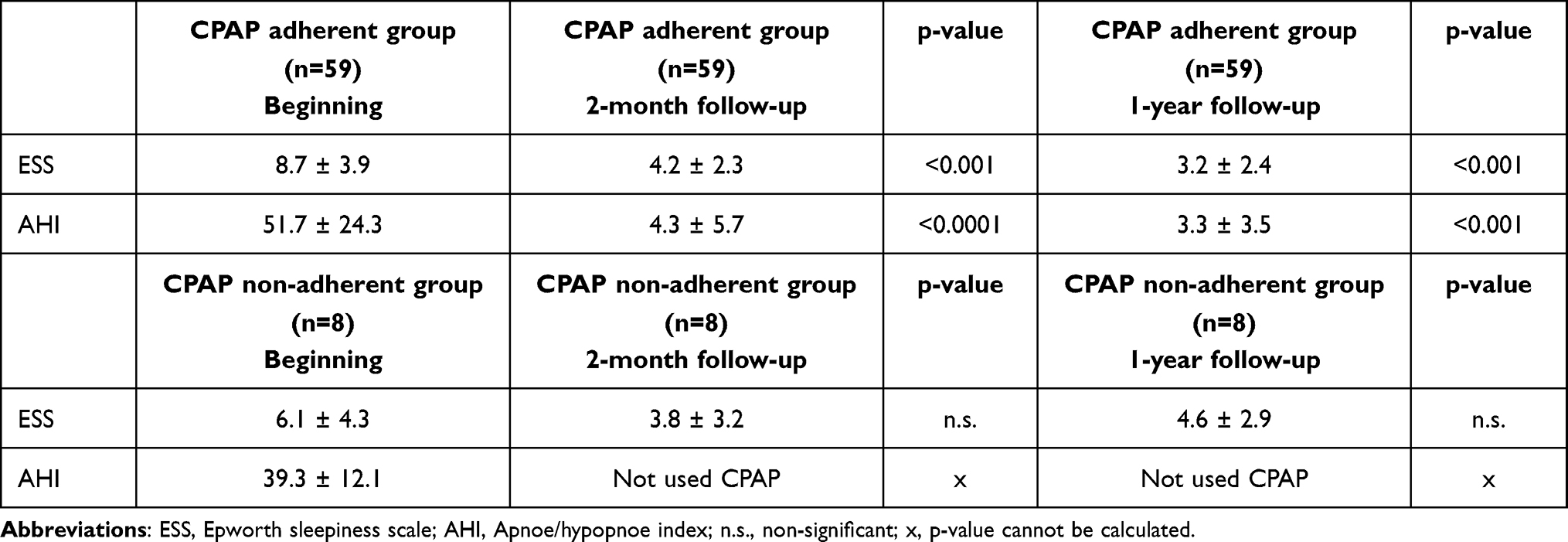 |
Table 3 Summary of OSA Treatment Results in Adherent and Non-Adherent Group |
Depressive and Anxiety Symptoms
Depressive symptoms were evaluated via BDI-II, and anxiety symptoms were evaluated via BAI. In the adherent group average, we observed a statistically significant decrease after two months of CPAP treatment (p < 0.001, medium effect size). After one year, BDI-II was statistically significant decrease compared to the beginning (p < 0.001, medium effect size), but not statistically significant when comparing two months and 1-year check-ups. In the non-adherent group, we observed borderline non-statistically significant change at two months (p = 0.053, medium effect size), and statistically significant decrease at 1-year (p < 0.01, large effect size).
In the adherent group in anxiety symptoms measured by BAI, we observed a statistically significant decrease after two months of CPAP treatment (p < 0.001, medium effect size). After one year, there was statistically significant decrease compared with the beginning of the treatment (p < 0.001, medium effect size), but it was not further decreased from the two months check-up. In the non-adherent group, we observed a non-statistically significant change at two months and at one year.
When analyzing answers in the scales, depressive and anxiety symptoms were generally decreased in all symptom domains, such as depressive cognitions and emotions, not only in those that OSA shares with depression and anxiety (eg, sleep disturbances and energy levels). Results are summarised in Table 4.
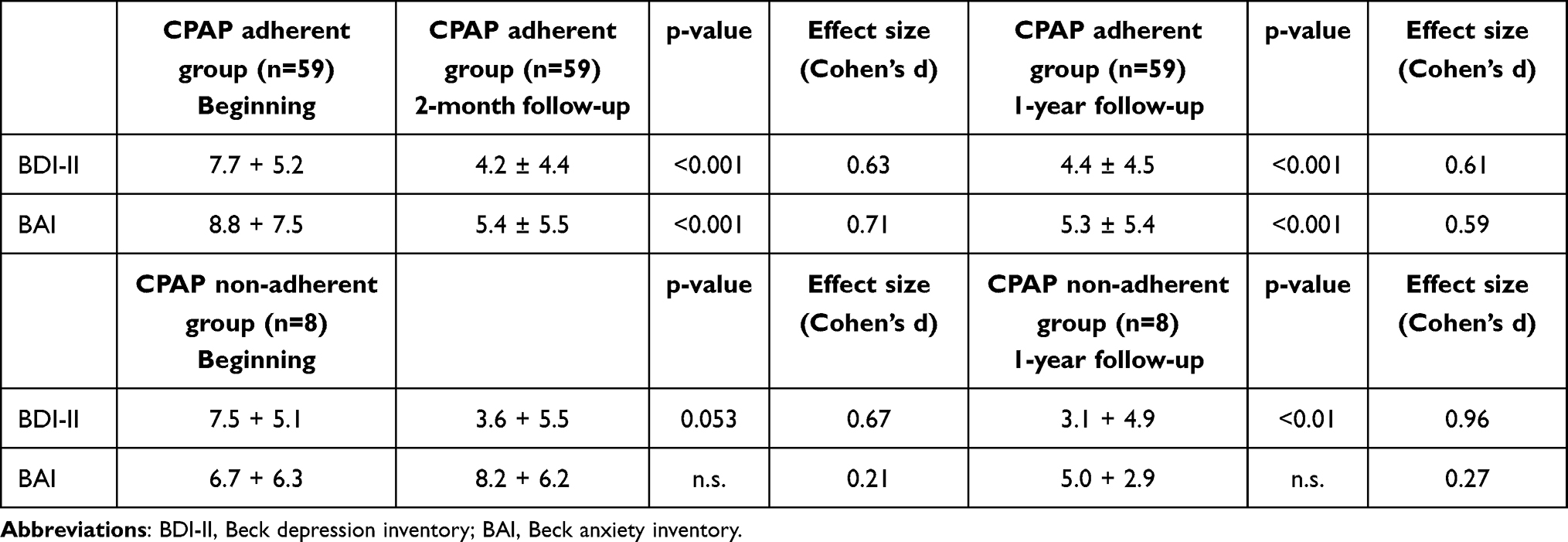 |
Table 4 Comparison of Results in BDI-II and BAI in the Adherent Group |
Trail Making Test
In TMT-Part A in an adherent group, the average time pre-treatment and after one year of the treatment presented almost no change with negligible effect size. Conversely, the performance in TMT-Part B significantly improved (p < 0.01, small effect size).
In the non-adherent group, the average pre-treatment performance in TMT-Part A saw non-significant deterioration (n.s., large effect size), and for TMT-Part B non-adherent group presented non-significant improvement (n.s., small effect size).
Verbal Fluency Test
In the adherent group verbal fluency, the average number of words statistically significantly increased (p < 0.01, small effect size). In the non-adherent group, we observed a negligible increase in the average number of words post-treatment (n.s., small effect size).
d2 Test of Attention
In the d2 test of attention, the total clean score in the adherent group statistically significantly increased (p < 0.001, medium effect size). The non-adherent group showed a non-significant increase (n.s., small effect size).
In the percentage of errors, an adherent group presented a non-significant decrease (n.s., small effect size). The non-adherent group made significantly more mistakes after one year (p < 0.01, large effect size).
All the cognitive tests and comparisons between groups are presented in Table 5.
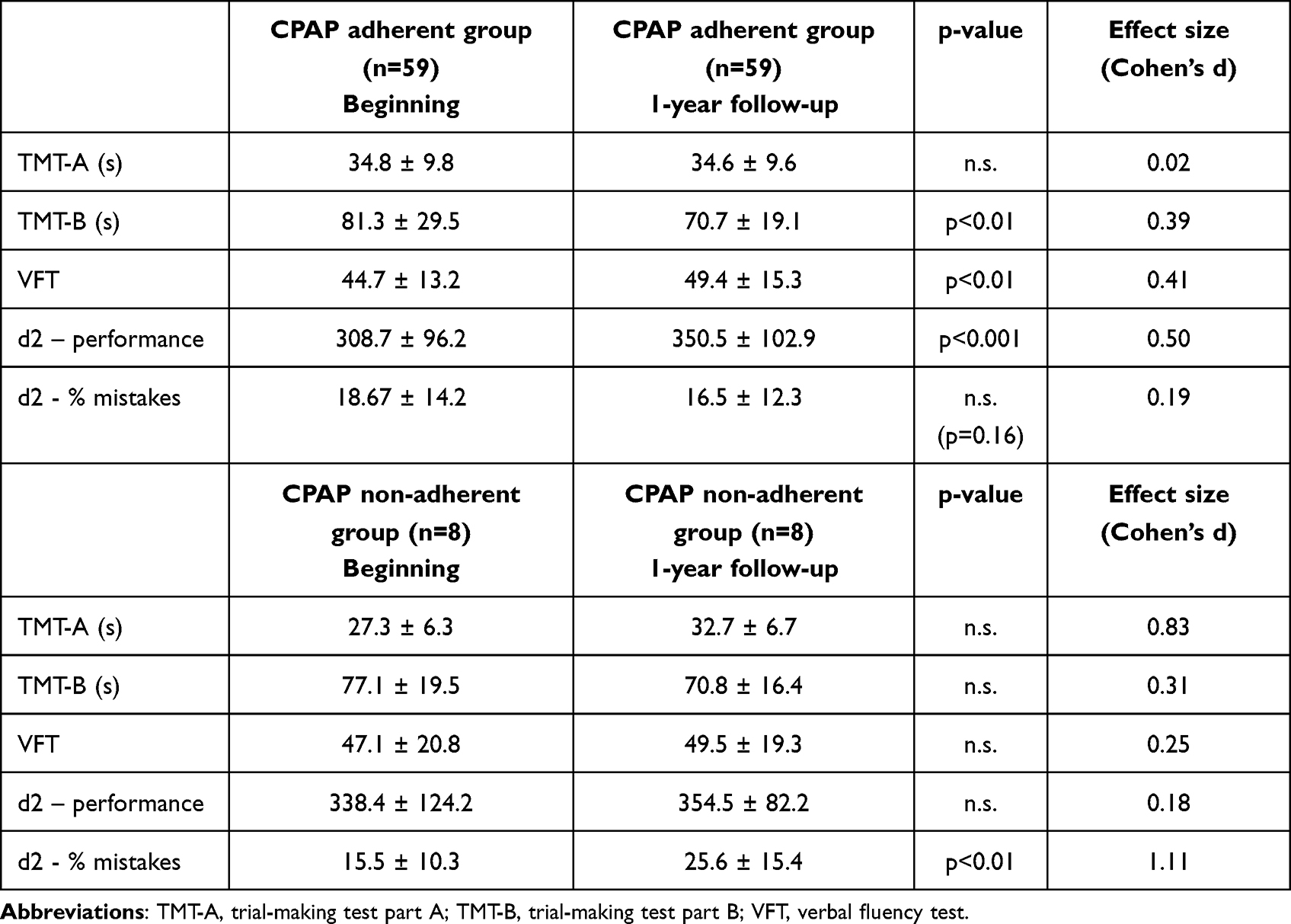 |
Table 5 Comparison of Results in Cognitive Tests in the Adherent Group |
Discussion
The presented study was the first longitudinal investigation on this topic in the Czech population. Most of the hypotheses were confirmed. The 1-year CPAP treatment significantly affected the cognitive functions, but not all investigated parameters were improved. Firstly, on average, the non-adherent group had lower results in OSA severity parameters. Another difference was lower BMI and lower daytime sleepiness measured by ESS. All this potentially results in fewer symptoms and impairment in daily life activities, resulting in lower motivation for treatment. This is in accordance with our previous finding in a longitudinal observation study about adherence to CPAP, proposing that there is a difference in motivation and adherence according to severity of OSA.88
The mean score of depressive symptoms assessed by BDI-II was relatively low and did not reach the threshold for mild or clinically relevant depression.89 It corresponds with no patient being diagnosed with depression via MINI interview. However, although the rates of depression were low, the patients with OSA treated with CPAP still decreased their scores and showed an improvement across the symptoms. Part of the change is likely attributable to the fact that some BDI-II items overlap with the signs of sleep apnoea (fatigue, hypoenergia, disturbances of concentration, and change in sleep). Still, the participants improved even in the more specific symptoms, such as depressive cognitions and mood symptoms. The reversibility of the depressive symptoms in OSA is a topic of many studies.61,62 Daniel et al presented a study of 50 patients and found that the proportion of patients with OSA and comorbid depression was significantly higher than in the general population.64
Two months of CPAP therapy significantly improved depressive symptoms reported in the BDI-II. It is in accordance with the Iacono Isidoro et al study, which shows that a short-term use of CPAP significantly decreased depressive symptoms.90 There is a lack of studies for longitudinal observation, and our study provides three points in time where the depressive symptoms were assessed. Our results show that the depressive symptoms decrease after the initiation of the CPAP therapy to a lower level. Then they stay relatively stable after one year of the treatment. This corresponds with our earlier work, Hobzova et al, in which treated patients showed statistically significant improvement in depressive symptoms after 1 month of CPAP.91
In the anxiety symptoms, we observed the same trend in the adherent group –a decrease after two months which remained stable in the one-year follow-up. Even though the patients had subclinical anxiety, they still felt relieved from their symptoms. In our study, BAI scores were relatively low compared to Rezaeitalab et al; with higher severity of OSA, higher anxiety scores were reported.92 In the non-adherent group, we observed non-significant increase in anxiety symptoms.
We observed different results for two tested parts in the Trail Making Test. In the adherent group, Part A did not show improvement after one year of treatment, and the average test time remained unchanged. In contrast, the performance in Part B significantly improved. One hypothesis explaining this difference is that different cognitive domains are tested in respective parts. Apart from visuospatial coordination and sustained attention, Part A assesses psychomotor speed, whereas Part B assesses higher cognitive functioning, such as shifting between tasks and flexibility. Another theory works with the fact that Part A is compared to Part B easier task and therefore is less influenced by the OSA. This could be supported by the fact that the results in our study are within the norms for the appropriate age group reported by Tombaugh.93 Literature here shows mixed results in studies. Meurice et al presented improvement in both parts of TMT.94 Montplaisir et al published negative results in TMT-B.95 Our results follow a meta-analysis by Kylstra et al that included 533 OSA patients and 497 controls and found no improvement in TMT-A and a small significant effect in TMT-B.96 Ferini-Strambi et al showed that after fifteen days of CPAP, there was an improvement in both TMT-A and TMT-B; however, there was no further progress after four months of CPAP.33 In a novel study from 2021, Parker et al showed that the TMT-A score was connected to the stages of sleep more pronounced in OSA patients. Worse results in TMT-A were associated with more N1-stage sleep, whereas better results were connected with more N3-stage sleep in older adults.97 Gelir et al described that subjects with OSA did not differ from healthy controls in TMT-A performance, in contrast with TMT-B performance, in which healthy controls showed better results than OSA patients.98 This result is in agreement with the research by Saunamäki et al, in which patients with OSA also reported worse results in TMT-B.99
Interestingly, in the meta-analysis, Kylstra et al found no impact of CPAP on verbal fluency.96 This contrasts with our results, which showed a small but statistically significant effect of CPAP therapy on the number of words recalled by patients. On the other hand, in an older study by Montplaisir et al, verbal fluency measured by Wechsler Adult Intelligence Scale was improved in subjects treated with CPAP.95 In a research from 2011, Bawden et al presented that patients with OSA did not diverge from healthy controls in verbal fluency tests.100 On the other hand, Salorio et al found significantly worse performance in verbal fluency in subjects with OSA compared to healthy controls.32
In the d2 attention test, the adherent group significantly improved in performance (speed score) but the percentage of errors showed a non-significant positive change. Kotterba et al observed that most subjects with OSA had pathological d2 test results.101 Per our results, Lau et al showed a slight improvement in attention after CPAP treatment.67 However, this contrasts with our previous work, Hobzova et al, in which patients with OSA showed improvement in both categories after one month of CPAP treatment.91 More recent work by D’Rozario et al showed improvement in sustained attention after six months of CPAP treatment.37 Another factor in play is the connection between excessive daytime sleepiness (measured by ESS in our study) and attention. Angeleli et al discovered that ESS scores correlated with results in attention intensive tasks but curiosly not in the tasks requiring divided attention. The authors propose that sleepiness plays multifaceted role in cognitive performance of OSA patients.102 Notably, however small the non-adherent quazi control group is, there is a statistically significant worsening in the percentage of mistakes.
According to the literature, it could be hypothesized that the CPAP treatment significantly affects the domains mainly impaired by OSA. This would explain the differences in TMT-A and TMT-B in our study. On the other hand, only one part of the d2 attention test improved, and attention is one of the most impaired cognitive functions in OSA. As the reduction of mistakes percentage was nearing a statistical trend, with more respondents, this could prove significant. In our study, patients also improved in verbal fluency, which is not consistently true in most intervention studies, as confirmed by a meta-analysis from 2013.27 Our subjects also showed a substantial reduction in subclinical depressive and anxiety symptoms, and the effect was sustained even after one year of treatment.
One variable that is to be taken into consideration is the COVID-19 pandemic that emerged during the course of the study. Growing body of literature suggests that neuropsychiatric consequences of COVID-19 include anxiety and depressive symptoms. According to a review from 2021, up to 40% of patients reported depressive and anxiety symptoms after recovery from the infection.103 The precise impact of the pandemic on our sample of patients is unclear and outside the scope of the study, but it is a variable that needs to be taken into account as a number of patient contracted COVID-19 and one patient died after the completion of the study as a direct consequence of COVID-19 infection.
Strengths and Limitations of the Study
This is the first longitudinal study in the Czech Republic’s clinical population. To our knowledge, most research studied either the short-term effect of CPAP treatment or a maximum follow-up period of 6 months. It is a novelty to prove that the impact of CPAP treatment is long-term, at least for one year of treatment. It is also of note that in studies with short-term effects of CPAP, test-retest repeatability is often an issue, as the patients could improve based on the previous knowledge of the test. Our study minimises this, as one year is sufficient to prevent this effect of exposure based on previous testing. Our study also implemented objective MINI interviews to exclude patients with comorbid psychiatric disorders, working solely with individuals suffering from subclinical depressive and anxiety symptoms. One of the study’s major strengths of the reported efficiency of the CPAP therapy in all included patients.
The study has several shortcomings. The main limitation is the absence of a proper control group. Because of adherence monitoring, we could differentiate non-adherent patients and create a quasi-control group, however rather small to be conclusive (n = 8). This is reflected in many studies in the field as it is unethical to leave patients with moderate and severe OSA without treatment for prolonged periods, given the severe morbidity and mortality that pose untreated OSA. In our previous work from 2017, we had a control group of the same severity on the waiting list for one month of CPAP. However, more extended periods without treatment are ethically inexcusable, posing limitations on obtaining severity and age-matched OSA control group. Another limitation is the fact the polysomnography study was not used for confirmation of the effectiveness of the CPAP treatment and could influence the outcomes. As respiratory polygraphy was used in the diagnostic procedure, the effectiveness of CPAP was assessed via residual AHI parameters indirectly. Regarding the generalizability another limitation is our sample is not stratified by age or social background. These could impact performance in cognitive tasks.
Furthermore, the number of participants was relatively small. Studies with larger samples need to confirm the results. Our numbers were partly limited by the amount of CPAP available yearly for our department and the COVID-19 pandemic and lockdowns hindered recruitment to the study. Another limitation might pose the application of the self-report scales for measuring depression and anxiety and lack of scale for sleep quality. These scales rely on the introspections of the participants and their motivation to be honest in their reports.
Conclusion
The study explored whether patients with OSA improved depressive and anxiety symptoms and cognitive functions after prolonged treatment with CPAP. After one year of therapy, several monitored cognitive parameters showed a statistically significant improvement: overall performance in the attention d2 test, executive functions in Trail Making Test – Part B and verbal fluency in the Verbal Fluency Test. We also found improvement and relief in subclinical depressive and anxiety symptoms, and the study did not find improvement in psychomotor speed in Trail Making Test – Part A.
CPAP treatment remains the primary intervention in moderate and severe OSA patients. Its effect on impaired cognitive functions seems consistent in specific domains and is present even after long-term treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2019;15(2):335–343. doi:10.5664/jcsm.7640
2. Young T, Palta M, Dempsey J, Peppard PE, Nieto FJ, Hla KM. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ. 2009;108(5):246–249.
3. Senaratna CV, English DR, Currier D, et al. Sleep apnoea in Australian men: disease burden, co-morbidities, and correlates from the Australian longitudinal study on male health. BMC Public Health. 2016;16(Suppl 3):1029. doi:10.1186/s12889-016-3703-8
4. bixler EO, Vgontzas AN, Lin HM, Calhoun SL, Vela-Bueno A, Kales A. Excessive daytime sleepiness in a general population sample: the role of sleep apnea, age, obesity, diabetes, and depression. J Clin Endocrinol Metab. 2005;90(8):4510–4515. doi:10.1210/jc.2005-0035
5. Bonsignore MR, Baiamonte P, Mazzuca E, Castrogiovanni A, Marrone O. Obstructive sleep apnea and comorbidities: a dangerous liaison. Multidiscip Respir Med. 2019;14:8. doi:10.1186/s40248-019-0172-9
6. Fleetham J, Ayas N, Bradley D, et al. Canadian Thoracic Society 2011 guideline update: diagnosis and treatment of sleep disordered breathing. Can Respir J. 2011;18(1):25–47. doi:10.1155/2011/506189
7. Liu H, Peng W, Zhou L, et al. Depression with obstructive sleep apnea lead to high cardiovascular disease morbidity/all-cause mortality: findings from the SHHS cohort [published online ahead of print, 2023 Feb 2]. J Sleep Res. 2023:e13828. doi:10.1111/jsr.13828
8. Gall R, Isaac L, Kryger M. Quality of life in mild obstructive sleep apnea. Sleep. 1993;16(8 Suppl):S59–S61. doi:10.1093/sleep/16.suppl_8.s59
9. Flemons WW, Whitelaw WA, Brant R, Remmers JE. Likelihood ratios for a sleep apnea clinical prediction rule. Am J Respir Crit Care Med. 1994;150(5 Pt 1):1279–1285. doi:10.1164/ajrccm.150.5.7952553
10. Hobzova M, Prasko J, Vanek J, et al. Depression and obstructive sleep apnea. Neuro Endocrinol Lett. 2017;38(5):343–352.
11. Vanek J, Prasko J, Genzor S, et al. Obstructive sleep apnea, depression and cognitive impairment. Sleep Med. 2020;72:50–58. doi:10.1016/j.sleep.2020.03.017
12. Klonoff H, Fleetham J, Taylor DR, Clark C. Treatment outcome of obstructive sleep apnea. Physiological and neuropsychological concomitants. J Nerv Ment Dis. 1987;175(4):208–212. doi:10.1097/00005053-198704000-00003
13. DeJean D, Giacomini M, Vanstone M, Brundisini F. Patient experiences of depression and anxiety with chronic disease: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser. 2013;13(16):1–33.
14. Reynolds CF, Kupfer DJ, McEachran AB, Taska LS, Sewitch DE, Coble PA. Depressive psychopathology in male sleep apneics. J Clin Psychiatry. 1984;45(7):287–290.
15. Millman RP, Fogel BS, McNamara ME, Carlisle CC. Depression as a manifestation of obstructive sleep apnea: reversal with nasal continuous positive airway pressure. J Clin Psychiatry. 1989;50(9):348–351.
16. Cheshire K, Engleman H, Deary I, Shapiro C, Douglas NJ. Factors impairing daytime performance in patients with sleep apnea/hypopnea syndrome. Arch Intern Med. 1992;152(3):538–541. doi:10.1001/archinte.1992.00400150068012
17. Peppard PE, Szklo-Coxe M, Hla KM, Young T. Longitudinal association of sleep-related breathing disorder and depression. Arch Intern Med. 2006;166(16):1709–1715. doi:10.1001/archinte.166.16.1709
18. Ramos Platón MJ, Espinar Sierra J. Changes in psychopathological symptoms in sleep apnea patients after treatment with nasal continuous positive airway pressure. Int J Neurosci. 1992;62(3–4):173–195. doi:10.3109/00207459108999770
19. Borak J, Cieślicki J, Szelenberger W, Wilczak-Szadkowska H, Koziej M, Zieliński J. Psychopathological characteristics of the consequences of obstructive sleep apnea prior to and three months after CPAP. Psychiatr Pol. 1994;28(3 Suppl):33–44.
20. Edinger JD, Carwile S, Miller P, Hope V, Mayti C. Psychological status, syndromatic measures, and compliance with nasal CPAP therapy for sleep apnea. Percept Mot Skills. 1994;78(3 Pt 2):1116–1118. doi:10.2466/pms.1994.78.3c.1116
21. Engleman HM, Martin SE, Deary IJ, Douglas NJ. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet. 1994;343(8897):572–575. doi:10.1016/s0140-6736(94)91522-9
22. Flemons WW, Tsai W. Quality of life consequences of sleep-disordered breathing. J Allergy Clin Immunol. 1997;99(2):S750–S756. doi:10.1016/s0091-6749(97)70123-4
23. Gabryelska A, Turkiewicz S, Ditmer M, Sochal M. Neurotrophins in the neuropathophysiology, course, and complications of obstructive sleep apnea-a narrative review. Int J Mol Sci. 2023;24(3):1808. doi:10.3390/ijms24031808
24. Harris M, Glozier N, Ratnavadivel R, Grunstein RR. Obstructive sleep apnea and depression. Sleep Med Rev. 2009;13(6):437–444. doi:10.1016/j.smrv.2009.04.001
25. Szaulińska K, Pływaczewski R, Sikorska O, et al. Obstructive sleep apnea in severe mental disorders. Psychiatr Pol. 2015;49(5):883–895. doi:10.12740/PP/32566
26. Rosenzweig I, Glasser M, Polsek D, Leschziner GD, Williams SC, Morrell MJ. Sleep apnoea and the brain: a complex relationship. Lancet Respir Med. 2015;3(5):404–414. doi:10.1016/S2213-2600(15)00090-9
27. Bucks RS, Olaithe M, Eastwood P. Neurocognitive function in obstructive sleep apnoea: a meta-review. Respirology. 2013;18(1):61–70. doi:10.1111/j.1440-1843.2012.02255.x
28. Gilley RR. The role of sleep in cognitive function: the value of a good night’s rest. Clin EEG Neurosci. 2023;54(1):12–20. doi:10.1177/15500594221090067
29. Bédard MA, Montplaisir J, Richer F, Malo J. Nocturnal hypoxemia as a determinant of vigilance impairment in sleep apnea syndrome. Chest. 1991;100(2):367–370. doi:10.1378/chest.100.2.367
30. Décary A, Rouleau I, Montplaisir J. Cognitive deficits associated with sleep apnea syndrome: a proposed neuropsychological test battery. Sleep. 2000;23(3):369–381. doi:10.1093/sleep/23.3.1d
31. Rouleau I, Décary A, Chicoine AJ, Montplaisir J. Procedural skill learning in obstructive sleep apnea syndrome. Sleep. 2002;25(4):401–411. doi:10.1093/sleep/25.4.398
32. Salorio CF, White DA, Piccirillo J, Duntley SP, Uhles ML. Learning, memory, and executive control in individuals with obstructive sleep apnea syndrome. J Clin Exp Neuropsychol. 2002;24(1):93–100. doi:10.1076/jcen.24.1.93.973
33. Ferini-Strambi L, Baietto C, Di Gioia MR, et al. Cognitive dysfunction in patients with obstructive sleep apnea (OSA): partial reversibility after continuous positive airway pressure (CPAP). Brain Res Bull. 2003;61(1):87–92. doi:10.1016/s0361-9230(03)00068-6
34. Aloia MS, Arnedt JT, Davis JD, Riggs RL, Byrd D. Neuropsychological sequelae of obstructive sleep apnea-hypopnea syndrome: a critical review. J Int Neuropsychol Soc. 2004;10(5):772–785. doi:10.1017/S1355617704105134
35. Verstraeten E, Cluydts R, Pevernagie D, Hoffmann G. Executive function in sleep apnea: controlling for attentional capacity in assessing executive attention. Sleep. 2004;27(4):685–693.
36. Mathieu A, Mazza S, Décary A, et al. Effects of obstructive sleep apnea on cognitive function: a comparison between younger and older OSAS patients. Sleep Med. 2008;9(2):112–120. doi:10.1016/j.sleep.2007.03.014
37. D’Rozario AL, Hoyos CM, Wong KKH, et al. Improvements in cognitive function and quantitative sleep electroencephalogram in obstructive sleep apnea after six months of continuous positive airway pressure treatment. Sleep. 2022;45(6):zsac013. doi:10.1093/sleep/zsac013
38. Beebe DW, Gozal D. Obstructive sleep apnea and the prefrontal cortex: towards a comprehensive model linking nocturnal upper airway obstruction to daytime cognitive and behavioral deficits. J Sleep Res. 2002;11(1):1–16. doi:10.1046/j.1365-2869.2002.00289.x
39. Lezak M, Howieson D, Loring D. Neuropsychological Assessment.
40. Sforza E, Haba-Rubio J, De Bilbao F, Rochat T, Ibanez V. Performance vigilance task and sleepiness in patients with sleep-disordered breathing. Eur Respir J. 2004;24(2):279–285. doi:10.1183/09031936.04.00091903
41. Alvarez JA, Emory E. Executive function and the frontal lobes: a meta-analytic review. Neuropsychol Rev. 2006;16(1):17–42. doi:10.1007/s11065-006-9002-x
42. Mazza S, Pépin JL, Naëgelé B, Plante J, Deschaux C, Lévy P. Most obstructive sleep apnoea patients exhibit vigilance and attention deficits on an extended battery of tests. Eur Respir J. 2005;25(1):75–80. doi:10.1183/09031936.04.00011204
43. Olaithe M, Bucks RS. Executive dysfunction in OSA before and after treatment: a meta-analysis. Sleep. 2013;36(9):1297–1305. doi:10.5665/sleep.2950
44. Tulek B, Atalay NB, Kanat F, Suerdem M. Attentional control is partially impaired in obstructive sleep apnea syndrome. J Sleep Res. 2013;22(4):422–429. doi:10.1111/jsr.12038
45. Kilpinen R, Saunamäki T, Jehkonen M. Information processing speed in obstructive sleep apnea syndrome: a review. Acta Neurol Scand. 2014;129(4):209–218. doi:10.1111/ane.12211
46. Simões EN, Padilla CS, Bezerra MS, Schmidt SL. Analysis of attention subdomains in obstructive sleep apnea patients. Front Psychiatry. 2018;9:435. doi:10.3389/fpsyt.2018.00435
47. Kong J, Zhou L, Li X, Ren Q. Sleep disorders affect cognitive function in adults: an overview of systematic reviews and meta-analyses. Sleep Biol Rhythms. 2023;21:1–10.
48. Naegele B, Pepin JL, Levy P, Bonnet C, Pellat J, Feuerstein C. Cognitive executive dysfunction in patients with obstructive sleep apnea syndrome (OSAS) after CPAP treatment. Sleep. 1998;21(4):392–397. doi:10.1093/sleep/21.4.392
49. Redline S, Tishler PV, Hans MG, Tosteson TD, Strohl KP, Spry K. Racial differences in sleep-disordered breathing in African-Americans and Caucasians [published correction appears in Am J Respir Crit Care Med 1997 May;155(5):1820]. Am J Respir Crit Care Med. 1997;155(1):186–192. doi:10.1164/ajrccm.155.1.9001310
50. Vaessen TJ, Overeem S, Sitskoorn MM. Cognitive complaints in obstructive sleep apnea. Sleep Med Rev. 2015;19:51–58. doi:10.1016/j.smrv.2014.03.008
51. Bédard MA, Montplaisir J, Malo J, Richer F, Rouleau I. Persistent neuropsychological deficits and vigilance impairment in sleep apnea syndrome after treatment with continuous positive airways pressure (CPAP). J Clin Exp Neuropsychol. 1993;15(2):330–341. doi:10.1080/01688639308402567
52. Devita M, Zangrossi A, Marvisi M, Merlo P, Rusconi ML, Mondini S. Global cognitive profile and different components of reaction times in obstructive sleep apnea syndrome: effects of continuous positive airway pressure over time. Int J Psychophysiol. 2018;123:121–126. doi:10.1016/j.ijpsycho.2017.10.003
53. Aloia MS, Ilniczky N, Di Dio P, Perlis ML, Greenblatt DW, Giles DE. Neuropsychological changes and treatment compliance in older adults with sleep apnea. J Psychosom Res. 2003;54(1):71–76. doi:10.1016/s0022-3999(02)00548-2
54. Tulving E, editor. Episodic and Semantic Memory in Organization of Memory. New York: Academic Press; 1972.
55. Greene NR, Naveh-Benjamin M. Adult age-related changes in the specificity of episodic memory representations: a review and theoretical framework [published online ahead of print, 2023 Feb 2]. Psychol Aging. 2023;38(2):67–86. doi:10.1037/pag0000724
56. Wallace A, Bucks RS. Memory and obstructive sleep apnea: a meta-analysis. Sleep. 2013;36(2):203–220. doi:10.5665/sleep.2374
57. Kloepfer C, Riemann D, Nofzinger EA, et al. Memory before and after sleep in patients with moderate obstructive sleep apnea. J Clin Sleep Med. 2009;5(6):540–548. doi:10.5664/jcsm.27655
58. Twigg GL, Papaioannou I, Jackson M, et al. Obstructive sleep apnea syndrome is associated with deficits in verbal but not visual memory. Am J Respir Crit Care Med. 2010;182(1):98–103. doi:10.1164/rccm.200901-0065OC
59. Loredo JS, Ancoli-Israel S, Dimsdale JE. Effect of continuous positive airway pressure vs placebo continuous positive airway pressure on sleep quality in obstructive sleep apnea. Chest. 1999;116(6):1545–1549. doi:10.1378/chest.116.6.1545
60. Calik MW. Treatments for obstructive sleep apnea. J Clin Outcomes Manag. 2016;23(4):181–192.
61. Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;(1):CD001106. doi:10.1002/14651858.CD001106.pub2
62. Povitz M, Bolo CE, Heitman SJ, Tsai WH, Wang J, James MT. Effect of treatment of obstructive sleep apnea on depressive symptoms: systematic review and meta-analysis. PLoS Med. 2014;11(11):e1001762. doi:10.1371/journal.pmed.1001762
63. Muñoz A, Mayoralas LR, Barbé F, Pericás J, Agusti AG. Long-term effects of CPAP on daytime functioning in patients with sleep apnoea syndrome. Eur Respir J. 2000;15(4):676–681. doi:10.1034/j.1399-3003.2000.15d09.x
64. Schwartz DJ, Kohler WC, Karatinos G. Symptoms of depression in individuals with obstructive sleep apnea may be amenable to treatment with continuous positive airway pressure. Chest. 2005;128(3):1304–1309. doi:10.1378/chest.128.3.1304
65. Montserrat JM, Ferrer M, Hernandez L, et al. Effectiveness of CPAP treatment in daytime function in sleep apnea syndrome: a randomized controlled study with an optimized placebo. Am J Respir Crit Care Med. 2001;164(4):608–613. doi:10.1164/ajrccm.164.4.2006034
66. Bardwell WA, Ancoli-Israel S, Berry CC, Dimsdale JE. Neuropsychological effects of one-week continuous positive airway pressure treatment in patients with obstructive sleep apnea: a placebo-controlled study. Psychosom Med. 2001;63(4):579–584. doi:10.1097/00006842-200107000-00010
67. Lau EY, Eskes GA, Morrison DL, Rajda M, Spurr KF. Executive function in patients with obstructive sleep apnea treated with continuous positive airway pressure [published correction appears in J Int Neuropsychol Soc. 2011 Mar;17(2):382]. J Int Neuropsychol Soc. 2010;16(6):1077–1088. doi:10.1017/S1355617710000901
68. Heinzer R, Gaudreau H, Décary A, et al. Slow-wave activity in sleep apnea patients before and after continuous positive airway pressure treatment: contribution to daytime sleepiness. Chest. 2001;119(6):1807–1813. doi:10.1378/chest.119.6.1807
69. Morisson F, Décary A, Petit D, Lavigne G, Malo J, Montplaisir J. Daytime sleepiness and EEG spectral analysis in apneic patients before and after treatment with continuous positive airway pressure. Chest. 2001;119(1):45–52. doi:10.1378/chest.119.1.45
70. Weaver TE, Maislin G, Dinges DF, et al. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep. 2007;30(6):711–719. doi:10.1093/sleep/30.6.711
71. Costa YS, Lim ASP, Thorpe KE, et al. Investigating changes in cognition associated with the use of CPAP in cognitive impairment and dementia: a retrospective study. Sleep Med. 2023;101:437–444. doi:10.1016/j.sleep.2022.11.037
72. Pretl M, Hobzová M, Honnerová M, et al. Indikační kritéria pro léčbu poruch dýchání ve spánku pomocí přetlaku v dýchacích cestách u dospělých Dokument České společnosti pro výzkum spánku a spánkovou medicínu. [Indication criteria for the treatment of sleep-disordered breathing using excess pressure in the airways in adults Document of the Czech Society for Sleep Research and Sleep Medicine]. Neurologie pro praxis. 2013;14(1):38–41.
73. Storch EA, Roberti JW, Roth DA. Factor structure, concurrent validity, and internal consistency of the Beck Depression Inventory-Second Edition in a sample of college students. Depress Anxiety. 2004;19(3):187–189. doi:10.1002/da.20002
74. Preiss M, Vacir K. Beckova sebeposuzovací škála depresivity pro dospělé – BDI-II [Beck self-report depression scale for adults – BDI-II]. Brno: Psychodiagnostika; 1999.
75. Ociskova M, Prasko J, Kupka M, et al. Psychometric evaluation of the Czech Beck Depression Inventory-II in a sample of depressed patients and healthy controls. Neuro Endocrinol Lett. 2017;38(2):98–106.
76. Kamaradova D, Prasko J, Latalova K, et al. Psychometric properties of the Czech version of the Beck Anxiety Inventory - comparison between diagnostic groups. Neuro Endocrinol Lett. 2015;36(7):706–712.
77. Bates ME, Lemay EP. The d2 Test of attention: construct validity and extensions in scoring techniques. J Int Neuropsychol Soc. 2004;10(3):392–400. doi:10.1017/S135561770410307X
78. Brickenkamp R, Zillmer E. Test pozornosti - d2, 1. české vydání, Testcentrum, Praha, přeložil a upravil Balcar K [Attention test - d2, 1st Czech edition, Testcentrum, Praha, tranlasted and edited by Balcar K]; 2000. Czech.
79. Steinborn MB, Langner R, Flehmig HC, Huestegge L. Methodology of performance scoring in the d2 sustained-attention test: cumulative-reliability functions and practical guidelines. Psychol Assess. 2018;30(3):339–357. doi:10.1037/pas0000482
80. Bowie CR, Harvey PD. Administration and interpretation of the Trail Making Test. Nat Protoc. 2006;1(5):2277–2281. doi:10.1038/nprot.2006.390
81. Bezdicek O, Motak L, Axelrod BN, et al. Czech version of the Trail Making Test: normative data and clinical utility. Arch Clin Neuropsychol. 2012;27(8):906–914. doi:10.1093/arclin/acs084
82. Federmeier KD, Kutas M, Schul R. Age-related and individual differences in the use of prediction during language comprehension. Brain Lang. 2010;115(3):149–161. doi:10.1016/j.bandl.2010.07.006
83. Zhao Q, Guo Q, Hong Z. Clustering and switching during a semantic verbal fluency test contribute to differential diagnosis of cognitive impairment. Neurosci Bull. 2013;29(1):75–82. doi:10.1007/s12264-013-1301-7
84. Nikolai T, Bezdicek O, Markova H, et al. Semantic verbal fluency impairment is detectable in patients with subjective cognitive decline. Appl Neuropsychol Adult. 2018;25(5):448–457. doi:10.1080/23279095.2017.1326047
85. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
86. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–57.
87. Amorim P. Mini International Neuropsychiatric Interview (MINI): validação de entrevista breve para diagnóstico de transtornos mentains. Revista Brasileira de Psiquiatria. 2000;22(3):106–115. doi:10.1590/S1516-44462000000300003
88. Genzor S, Prasko J, Vanek J, Asswad AG, Nadjarpour S, Sova M. Adherence of obstructive sleep apnoea syndrome patients to positive airway pressure therapy - 10-year follow-up. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2022;166(4):441–446. doi:10.5507/bp.2021.041
89. Jackson-Koku G. Beck depression inventory. Occup Med. 2016;66(2):174–175. doi:10.1093/occmed/kqv087
90. Iacono Isidoro S, Salvaggio A, Lo Bue A, Romano S, Marrone O, Insalaco G. Immediate effect of CPAP titration on perceived health related quality of life: a prospective observational study. BMC Pulm Med. 2016;16(1):172. doi:10.1186/s12890-016-0336-8
91. Hobzova M, Hubackova L, Vanek J, et al. Cognitive function and depressivity before and after cpap treatment in obstructive sleep apnea patients. Neuro Endocrinol Lett. 2017;38(3):145–153.
92. Rezaeitalab F, Moharrari F, Saberi S, Asadpour H, Rezaeetalab F. The correlation of anxiety and depression with obstructive sleep apnea syndrome. J Res Med Sci. 2014;19(3):205–210.
93. Tombaugh TN. Trail Making Test A and B: normative data stratified by age and education. Arch Clin Neuropsychol. 2004;19(2):203–214. doi:10.1016/S0887-6177(03)00039-8
94. Meurice JC, Marc I, Sériès F. Efficacy of auto-CPAP in the treatment of obstructive sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1996;153(2):794–798. doi:10.1164/ajrccm.153.2.8564134
95. Montplaisir J, Bédard MA, Richer F, Rouleau I. Neurobehavioral manifestations in obstructive sleep apnea syndrome before and after treatment with continuous positive airway pressure. Sleep. 1992;15(6 Suppl):S17–S19. doi:10.1093/sleep/15.suppl_6.s17
96. Kylstra WA, Aaronson JA, Hofman WF, Schmand BA. Neuropsychological functioning after CPAP treatment in obstructive sleep apnea: a meta-analysis. Sleep Med Rev. 2013;17(5):341–347. doi:10.1016/j.smrv.2012.09.002
97. Parker JL, Appleton SL, Melaku YA, et al. Sleep macroarchitecture but not obstructive sleep apnea is independently associated with cognitive function in only older men of a population-based cohort. J Sleep Res. 2021;30(6):e13370. doi:10.1111/jsr.13370
98. Gelir E, Başaran C, Bayrak S, et al. Electrophysiological assessment of the effects of obstructive sleep apnea on cognition. PLoS One. 2014;9(2):e90647. doi:10.1371/journal.pone.0090647
99. Saunamäki T, Jehkonen M. A review of executive functions in obstructive sleep apnea syndrome. Acta Neurol Scand. 2007;115(1):1–11. doi:10.1111/j.1600-0404.2006.00744.x
100. Bawden FC, Oliveira CA, Caramelli P. Impact of obstructive sleep apnea on cognitive performance. Arq Neuropsiquiatr. 2011;69(4):585–589. doi:10.1590/s0004-282x2011000500003
101. Kotterba S, Rasche K, Widdig W, et al. Neuropsychological investigations and event-related potentials in obstructive sleep apnea syndrome before and during CPAP-therapy. J Neurol Sci. 1998;159(1):45–50. doi:10.1016/s0022-510x(98)00131-2
102. Angelelli P, Macchitella L, Toraldo DM, et al. The neuropsychological profile of attention deficits of patients with obstructive sleep apnea: an update on the daytime attentional impairment. Brain Sci. 2020;10(6):325. doi:10.3390/brainsci10060325
103. Nakamura ZM, Nash RP, Laughon SL, Rosenstein DL. Neuropsychiatric Complications of COVID-19. Curr Psychiatry Rep. 2021;23(5):25. doi:10.1007/s11920-021-01237-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.