Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Cognitive functioning in patients treated with electroconvulsive therapy
Authors Kalisova L ![]() , Kubinova M
, Kubinova M ![]() , Michalec J, Albrecht J
, Michalec J, Albrecht J ![]() , Madlova K, Raboch J
, Madlova K, Raboch J ![]()
Received 2 August 2018
Accepted for publication 24 September 2018
Published 8 November 2018 Volume 2018:14 Pages 3025—3031
DOI https://doi.org/10.2147/NDT.S182423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Lucie Kalisova, Marketa Kubinova, Jiri Michalec, Jakub Albrecht, Katerina Madlova, Jiri Raboch
Department of Psychiatry, First Faculty of Medicine, Charles University, General University Hospital in Prague, Prague, Czech Republic
Background: Electroconvulsive therapy (ECT) is an effective treatment method for severe mental illnesses. ECT has gone through significant modernization. Side effects of ECT have largely decreased. Temporary disturbance of cognitive performance can be still present as a side effect of electroconvulsive treatment.
Methods: Cognitive functioning in the sample of patients with severe and acute mental illness treated with electroconvulsive therapy (ECT) was assessed. Basic assessment of cognitive functions was applied in the beginning, in the middle, and at the end of ECT course treatment with the Montreal Cognitive Assessment (MoCA). Complex and detailed testing of cognitive functions using the MATRICS Consensus Cognitive Battery (MCCB) was done at two points in time – within the first week of and then 6 weeks after the end of ECT.
Results: Participants had cognitive deficits at baseline, which were most likely influenced markedly by the psychopathology of the illness itself. The improvement in cognition came together with the reduction in psychopathology; psychopathology scores were significantly reduced during ECT treatment. Compared to the baseline, all scores for cognitive testing were significantly improved but remained low in comparison with the controls. After 6 weeks, there was further significant improvement.
Conclusion: Our results confirm the safety and efficacy of ECT in the treatment of severe mental disorders.
Keywords: electroconvulsive therapy, cognition, side effects, MCCB
Introduction
Electroconvulsive therapy (ECT) is an effective method for the treatment of severe and/or treatment-resistant mental disorders.1,2 The effect of ECT on the brain is complex and diverse.3–5 Among the main indications of treatment are severe states of depression, catatonia, and depressive, manic or psychotic states resistant to treatment. ECT is also used with caution in situations in which we are aware of the harmful side effects of pharmacotherapy (in the case of polymorbid and elderly patients) or in which we are not able to wait for the effects of medication to take place (states involving severe suicidal, autoagressive, or heteroagressive risks or in specific states in which it is effective [neuroleptic malignant syndrome, and so on]).1,6
ECT has gone through and continues to go through significant modernization, and ECT’s side effects have significantly decreased. Its irreplaceability in the treatment of some mental health indications in psychiatry is verified by clinical practice as well as scientific research.
Severe side effects of ECT were minimized due to the modernization of the method (muscle relaxation, modern short-time anesthesia, technical parameters of the method, and so on). Currently, patients treated with modern ECT complain of mild side effects such as headaches and muscle aches.7
Mild temporary disturbance of cognitive performance can still be present as a side effect of electroconvulsive treatment and might be part of a mechanism of action due to changes in the hippocampus (neuroplasticity and neurogenesis).8,9 In general, the occurrence of cognitive side effects during ECT treatment seems to be mostly influenced by parameters connected to how the treatment is applied, such as the placement of electrodes, the length and amplitude of stimulus, pulse width, the dose of electric pulse, and the frequency of application. Changes in cognitive performance as a consequence of ECT are usually temporary and mild (often reaching only a sub-clinical level) and rarely influence normal life functioning. Symptoms of acute mental illness can also influence cognitive functioning, and it is difficult to distinguish the impact of mental illness from treatment side effects.
The most frequently occurring cognitive side effects mainly include postictal disorientation,10,11 temporary disturbance of anterograde memory, and less proven damage of retrograde memory, which can be longer lasting.12–20
The occurrence of cognitive side effects was proven to be influenced by different possible factors: 1) the technical parameters of ECT (right-unilateral [RUL] superior to bilateral, shorter pulse width, non-sine shape of wave, lower dose of electric current, and lower frequency of application of ECT),21–23 2) psychiatric illness and psychopathology,24,25 3) psychiatric medication, 4) type of anesthetic,26,27 and 5) age, overall state of brain (level of cognitive functioning), and cognitive reserve.28 Many parameters of treatment can be set and improved with the aim to minimize cognitive side effects.
The aim of this study was to assess the extent of cognitive disturbance during and after the end of ECT.
Methods
Inclusion criteria were that participants must be older than 18 years (no determined maximum age since ECT is also effective in older patients), capable of giving informed consent, and able to be tested for cognition. All diagnoses of acute mental illness, where ECT was recommended, were included. The diagnosis was set using ICD-10 by a qualified specialist in psychiatry. Several different clinicians were involved in a diagnostic process. Patients were divided into “depression” group (F31.4–6, F32.x, F33.x, F25.1, and F06.3), “psychosis” group (F2x.x except 25.0 and 25.1), and “mania” group (F30.x, F31.0–3) according to their diagnosis.
Participants in the control group were nonrandomly recruited from healthy, community-dwelling volunteers, with no relationship to the authors. They had no history of brain damage, psychiatric illness, chronic drug or alcohol abuse, or any medical illness that could affect neurocognitive function. They had a similar education level to the patients (expressed as years of education). The rationale for including a control group in the study was to control the practice effect due to repeated measures of cognitive performance. The control group was tested at the following two time points: Tc1 (the first scheduled visit) and Tc2 (6 weeks after the first visit).
All patients had some medication prior to and during ECT, but there was a tendency to minimalize the use of psychopharmacs that could influence the quality of electric seizure (benzodiazepines, anticonvulsants, and so on).
The sample of patients treated with ECT was screened with Montreal Cognitive Assessment (MoCA)29 1 day before the beginning of treatment (T1), 1 day before the fourth session (T2), 1 day after the last session (T3), and again after 6 weeks (T4) to assess cognitive functioning (maximum 30 points). This test was repeatedly approved as a test for the short and quick assessment of cognitive functioning. The advantage of this test is the option to use different variations of the test, which allows retesting after a short time.
A complex assessment of cognitive functions was tested in detail with the Czech version of the complex test battery, MATRICS Consensus Cognitive Battery (MCCB), within 1 week of (T3) and then 6 weeks after (T4) the end of ECT. The MCCB30 used in the study assessed vigilance, visual memory and learning, verbal memory and learning, working memory, speed of information processing, and executive functions. MCCB was primarily developed for the assessment of neurocognition in schizophrenia disorders but has since been widely used because it permits repeated testing within short time periods (has tests–retests). We excluded a test for social cognition from the battery, which seems to be specific for schizophrenia, and we did not have a purpose to test it in this study. The performance of both groups – patients and the control group – in the MCCB is expressed in normative T-scores (mean =50; SD =10; 50±10) corrected for age and gender of the participants of the study. The obvious differences in age and in the number of men between patients and the control group, therefore, should not affect the comparability of their performance.
The severity of illness was assessed with the 24-item Brief Psychiatric Rating Scale (BPRS).31 This scale has a 1–7 range for each item, in which 7 is the most severe pathology. The maximum total score is 168. Participants were assessed with BPRS at the same time as those with MoCA (T1, T2, T3, and T4) by a researcher/psychiatrist with training in the method.
Basic sociodemographic data, such as age, gender, and length of education, and treatment-connected parameters, such as treatment with ECT in the past (during previous hospitalizations), mean number of applications per ECT series, type of placement of electrodes, dose of energy, stimulus parameters, and type of anesthetics, were collected through questionnaires designed for the purpose of this study.
The results of complex cognitive testing obtained were compared with the control group. All controls were healthy and did not take medication influencing cognitive performance. They agreed to participate in the study and signed informed consent forms.
Statistical methods
A mixed-design ANOVA, controlling for group (patient and control group) vs cognitive performance interaction, was used to illuminate the potential learning effect on cognitive improvement from T3 to T4. We also performed an independent samples t-test for independent samples to compare patients with depression and psychosis in measures of cognitive performance. Moreover, Pearson’s correlation and descriptive statistics were used.
The study was approved by the ethical committee of General University Hospital in Prague.
Results
Forty-two patients (21 women and 21 men) with an average age of 50.2±16.1 years and the years of education of 14.2±2.9 years and with the most frequent diagnosis of severe depressive disorder (N=31; 74%), followed by psychosis (N=9; 21%) and mania (N=2; 5%), were included in the study. One-third of the patients (N=14; 33%) had undergone ECT treatment in the past.
The control group included 32 individuals; 12 (37.5%) of whom were female, the average age was 33.5±10.2 years, and years of education were 14.6±2.2.
The characteristics of ECT were as follows: the average number of ECT sessions/patients was 8.6 (4–17); the placement of electrodes in 100% cases was bitemporal; the pulse width was 0.48±0.09 (0.3–0.75); the average energy within the whole ECT (mC)/patient was 334.2±207.8; the stimulus frequency was 20–120 Hz; the pulse height was 0.8–0.9; and the used anesthetics were thiopenthal and propofol. All patients were treated with brief pulse square type waves, and the seizure threshold was set individually for each patient by titration. The Somatics Thymatron System IV and MECTA Spectrum 5,000Q devices were used. Bitemporal placement of electrodes was used for all patients.
Global cognitive performance of patients (N=42) increased through treatment from T1 to T4, as is expressed in the MoCA scores (T1=20.4±8.3; T2=23.7±4.3; T3=24.6±3; T4=27±2.2). Psychopathology improved during treatment from T1 to T4, as is seen in the BPRS scores (T1=64.2±15.5; T2=52.1±16.2; T3=35.9±12.5; T4=35.2±8.6). Based on the correlation analysis, cognitive deficit was also influenced by psychopathology. With the improvement in psychopathology, the cognitive performance measured with MoCA improved. We found a medium-to-large significant correlation between MoCA and BPRS at T1 and T2 (all r coefficients were around 0.5) (Table 1).
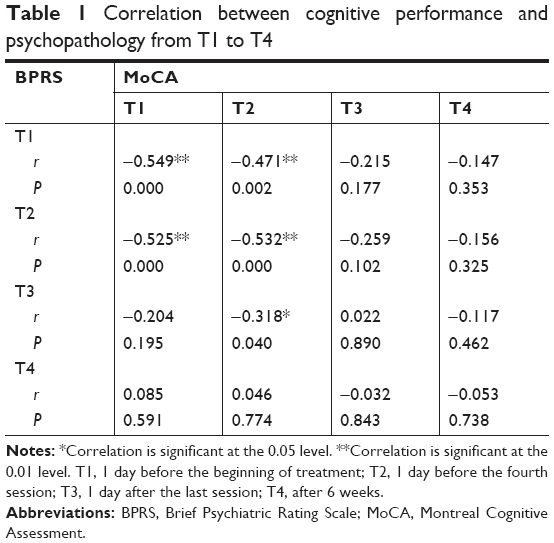 | Table 1 Correlation between cognitive performance and psychopathology from T1 to T4 |
Table 2 and Figure 1 summarize the cognitive performance of the sample of patients at T3 and T4 in comparison with controls using the comprehensive neuropsychological battery, MCCB. Cognitive performance decreased by −2 to −1 SD at T3 in patients with regard to general population norms. Norms for cognitive performance in MCCB were assessed according to gender- and age-based US norms. The Czech control group had cognitive performance similar to US norms (50±10 T-score), so we were able to use US norms as satisfactory reference norms in this study, ie, for the interpretation of the cognitive performance of patients, since it appears that they either do not overestimate or underestimate the cognitive performance of given participant.
 | Table 2 Cognitive performance in MCCB – comparison of patients and controls |
 | Figure 1 MATRICS performance of patients in the T3, T4, and control groups in Tc1 and Tc2 (within 6 weeks). |
The cognitive performance of patients in MCCB improved significantly at T4 (around 1 SD/10 points in T-scores in all domains). The improvement could not be explained by a practice effect at least in domains such as vigilance, speed of information processing, and visual memory and learning. In these cognitive domains, we found a significant effect depending on the group (clinical group vs control group) on the level of improvement, ie, the clinical group was improving significantly more than the control group: speed of processing (F=9.62; P=0.003); attention/vigilance (F=4.92; P=0.030); visual memory and learning (F=8.45; P=0.005). Nevertheless, cognitive performance remained deficient in a majority of domains in relation to norms (around 1 SD below normative mean, i.e., around 40 T-score) (Table 2 and Figure 1).
Table 3 shows a comparison of cognitive performance between patients from the psychosis and depression groups at T3 and T4. Although the groups differed with respect to their T-score means, there was only a significant difference with domain visual memory and learning at T3 and T4. The depression group performed better. Considering the Bonferroni correction for multiple comparisons, there was no other significant difference, although it shows trend to significance. It is necessary to note that the sample of patients with psychosis was very small (N=9).
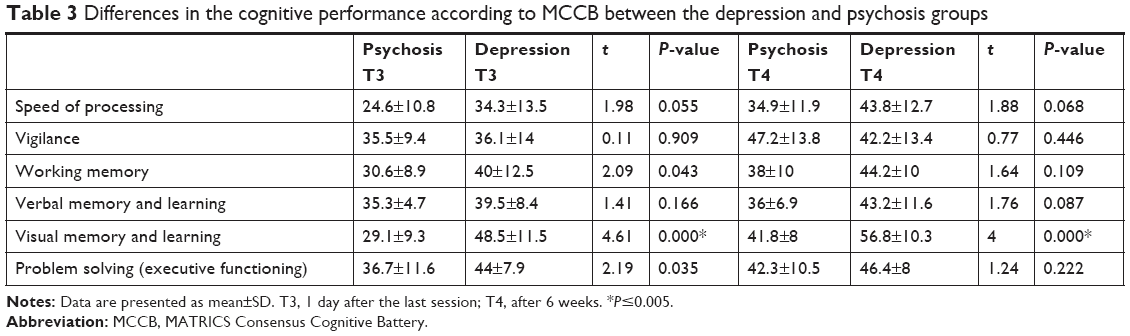 | Table 3 Differences in the cognitive performance according to MCCB between the depression and psychosis groups |
Cognitive performance of patients (N=42) during treatment (according to MoCA) did not correlate with the technical parameters of ECT (number of convulsions × total energy was set as a parameter during treatment). The strongest but still not significant correlation was found with the MoCA score at T3 (r=−0.22; P=0.171). The width of pulse variability proved to be too narrow for statistical evaluation and did not bring any results.
There was no difference between patients with propofol and thiopenthal anesthesia, although they differed in the dose of energy.
Discussion
Our results found cognitive deficits during ECT treatment in our sample, which improved during the treatment course and improved further within 6 weeks after the cessation of ECT. This is in concordance with previous studies of other authors assessing cognitive performance during ECT and studies on the effectiveness of ECT. The majority of studies on this topic mainly included patients with depression, and the majority of patients in our sample had severe depression. Semkovska, in a meta-analysis of 84 studies, including almost 3,000 patients, postulated that anterograde memory disturbance is worst within the first 3 days after ECT and improvement with relation to a state similar to before treatment was apparent after 15 days.13 In the review of Verwijk et al14 assessing neurocognitive side effects in the treatment with RUL ECT and with short and ultrashort pulses even showed improvement in anterograde memory (verbal and nonverbal) 1 and 6 months after ECT in relation to the pretreatment state. A multicentric study by Sackeim following many cognitive parameters, including several tests for anterograde memory in around 350 patients, reported persisting deficits only in speed information processing and autobiographic memory. Other cognitive domains went back to normal levels within 6 months after ECT. It also showed that disturbance of cognition differed due to the variability of methodology of the provision of ECT in observed centers (mainly technical parameters of treatment).15
In a prospective study, Kessler et al32 tested cognitive functions using MCCB before and again 6 weeks after ECT and compared groups of patients with bipolar depression (N=39) treated with medication and RUL ECT. In this study, they did not detect a significant difference between groups concerning MCCB results. Improvements in neurocognitive performance were significantly correlated with reductions in depression scores. It can be deduced that RUL ECT might not influence cognition by itself.
Mohn and Rund from Norway assessed cognitive functions using MCCB in a sample of depressive patients before ECT and 6 weeks after and 6 months after ECT.33,34 Cognitive performance improved significantly in mean levels of speed of processing, attention/vigilance, and visual learning after 6 weeks, and further improvement of results came in 6 months, when patients were also significantly better in the problem-solving domain. They reached similar results to our study.
According to our results, psychopathology scores remained unchanged between T3 and T4. This could be mean that cognition improves more slowly. We discussed our results in T3, and we arrived at some possible explanations. Patients with schizophrenia can have a stable residual cognitive deficit independent from ECT and their acute state.35 In our sample, patients with schizophrenia had worse results at T3 and T4, but only one domain at T4 was significantly lower than in the rest of the patients with different diagnoses.
Depression itself is connected with cognitive decline, which can continue longer term, even when affective symptoms have recovered.36
We did not find a connection between parameters connected to the ECT method and a cognitive decline in the utilized tests (MoCA and MCCB). In our study, we use brief/ultrabrief pulse and non-sine waves and assessed the threshold individually. In contrast, all patients had a bilateral placement of electrodes. Bilateral placement of electrodes was repeatedly proven as a factor influencing cognitive performance in comparison to RUL ECT.37 We did not find a difference between anesthetics used in regard to cognitive side effects, since some studies prefer propofol.26,38
Conclusion
Our results confirmed a prominent influence of psychopathology on cognitive performance in patients with acute severe mental disorders treated with ECT. Cognitive functioning improved with the treatment and further improved 6 weeks after the end of ECT. Our results confirm the safety and efficacy of ECT in the treatment of severe mental disorders.
Limitations of the study
Our sample has a diverse diagnostic profile, but the effectiveness of ECT and temporariness of cognitive side effects was proven.
Patients had pharmacotherapy and ECT concurrently. It is common practice in the Czech Republic, but it could partly influence the results (concerning effectiveness and also cognitive performance).
The sample is rather small; we await more robust results with a greater number of patients, but MCCB is a fairly complex and long-lasting procedure.
It would be nice to test MCCB before ECT also, but (as can be seen from psychopathology scores) patients would not be able to undergo such difficult assessment.
Retrograde (eg, autobiographic) memory was not tested, and, according to other studies,16–19 can be impaired with ECT.
A bilateral placement of electrodes was used, but RUL treatment should be used as it is safer for cognition.
Acknowledgment
This study was supported by the Ministry of Health of the Czech Republic VES 2015 15-30439A and RVO VFN 64165.
Disclosure
The authors report no conflicts of interest in this work.
References
Payne NA, Prudic J. Electroconvulsive therapy: Part I. A perspective on the evolution and current practice of ECT. J Psychiatr Pract. 2009;15(5):346–368. | ||
UK ECT Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet. 2003;361(9360):799–808. | ||
Prudic J. Electroconvulsive therapy. In: Saddock BJ, Saddock VA, editors. Comprehensive Textbook of Psychiatry. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:3285–3300. | ||
Sackeim HA. The anticonvulsant hypothesis of the mechanisms of action of ECT: current status. J ECT. 1999;15(1):5–26. | ||
Nobler MS, Oquendo MA, Kegeles LS, et al. Decreased regional brain metabolism after ect. Am J Psychiatry. 2001;158(2):305–308. | ||
Baghai TC, Möller HJ. Electroconvulsive therapy and its different indications. Dialogues Clin Neurosci. 2008;10(1):105–117. | ||
Devanand DP, Fitzsimons L, Prudic J, Sackeim HA. Subjective side effects during electroconvulsive therapy. Convuls Ther. 1995;11(4):232–240. | ||
Rami-González L, Bernardo M, Boget T. Subtypes of memory dysfunction associated with electroconvulsive therapy. Characteristics and neurobiological bases involved. J Ect. 2001;17:129–135. | ||
Mcclintock SM, Choi J, Deng ZD, Appelbaum LG, Krystal AD, Lisanby SH. Multifactorial determinants of the neurocognitive effects of electroconvulsive therapy. J Ect. 2014;30(2):165–176. | ||
Daniel WF, Crovitz HF. Disorientation during electroconvulsive therapy. Technical, theoretical, and neuropsychological issues. Ann N Y Acad Sci. 1986;462(1):293–306. | ||
Reti IM, Krishnan A, Podlisky A, et al. Predictors of electroconvulsive therapy postictal delirium. Psychosomatics. 2014;55(3):272–279. | ||
Ingram A, Saling MM, Schweitzer I. Cognitive side effects of brief pulse electroconvulsive therapy: a review. J Ect. 2008;24(1):3–9. | ||
Semkovska M, Mcloughlin DM. Objective cognitive performance associated with electroconvulsive therapy for depression: a systematic review and meta-analysis. Biol Psychiatry. 2010;68(6):568–577. | ||
Verwijk E, Comijs HC, Kok RM, Spaans HP, Stek ML, Scherder EJ. Neurocognitive effects after brief pulse and ultrabrief pulse unilateral electroconvulsive therapy for major depression: a review. J Affect Disord. 2012;140(3):233–243. | ||
Sackeim HA, Prudic J, Fuller R, Keilp J, Lavori PW, Olfson M. The cognitive effects of electroconvulsive therapy in community settings. Neuropsychopharmacology. 2007;32(1):244–254. | ||
Meeter M, Murre JM, Janssen SM, Birkenhager T, van den Broek WW. Retrograde amnesia after electroconvulsive therapy: a temporary effect? J Affect Disord. 2011;132(1–2):216–222. | ||
Sobin C, Sackeim HA, Prudic J, et al. Predictors of retrograde amnesia following ECT. Am J Psychiatry. 1995;152(7):995–1001. | ||
Fraser LM, O’Carroll RE, Ebmeier KP. The effect of electroconvulsive therapy on autobiographical memory: a systematic review. J Ect. 2008;24(1):10–17. | ||
O’Connor M, Lebowitz BK, Ly J, et al. A dissociation between anterograde and retrograde amnesia after treatment with electroconvulsive therapy: a naturalistic investigation. J Ect. 2008;24(2):146–151. | ||
Sackeim HA. Autobiographical memory and electroconvulsive therapy: do not throw out the baby. J Ect. 2014;30(3):177–186. | ||
Sackeim HA, Prudic J, Nobler MS, et al. Effects of pulse width and electrode placement on the efficacy and cognitive effects of electroconvulsive therapy. Brain Stimul. 2008;1(2):71–83. | ||
Peterchev AV, Rosa MA, Deng ZD. ECT stimulus parameters: rethinking dosage. J Ect. 2010;26(3):159. | ||
Tor PC, Bautovich A, Wang MJ, et al. A systematic review and meta-analysis of brief versus ultrabrief right unilateral electroconvulsive therapy for depression. J Clin Psychiatry. 2015;8(2):310–320. | ||
Brodaty H, Hickie I, Mason C, Prenter L. A prospective follow-up study of ECT outcome in older depressed patients. J Affect Disord. 2000;60(2):101–111. | ||
Mcdermott LM, Ebmeier KP. A meta-analysis of depression severity and cognitive function. J Affect Disord. 2009;119(1–3):1–8. | ||
Bauer J, Hageman I, Dam H, et al. Comparison of propofol and thiopental as anesthetic agents for electroconvulsive therapy: a randomized, blinded comparison of seizure duration, stimulus charge, clinical effect, and cognitive side effects. J Ect. 2009;25(2):85–90. | ||
Janke C, Bumb JM, Aksay SS, Thiel M, Kranaster L, Sartorius A. Ketamine as anesthetic agent in electroconvulsion therapy. Anaesthesist. 2015;64(5):357–364. | ||
Legendre SA, Stern RA, Solomon DA, Furman MJ, Smith KE. The influence of cognitive reserve on memory following electroconvulsive therapy. J Neuropsychiatry Clin Neurosci. 2003;15(3):333–339. | ||
Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. | ||
Nuechterlein KH, Green MF, Kern RS, et al. The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity. Am J Psychiatry. 2008;165(2):203–213. | ||
Overall JE, Gorham DR. The Brief Psychiatric Rating Scale (BPRS): recent developments in ascertainment and scaling. Psychopharmacol Bull. 1988;24:97–99. | ||
Kessler U, Schoeyen HK, Andreassen OA, et al. The effect of electroconvulsive therapy on neurocognitive function in treatment-resistant bipolar disorder depression. J Clin Psychiatry. 2014;75(11):e1306–e1313. | ||
Mohn C, Rund BR. Significantly improved neurocognitive function in major depressive disorders 6 weeks after ECT. J Affect Disord. 2016;202:10–15. | ||
Mohn C, Rund BR. Maintained improvement of neurocognitive function in major depressive disorders 6 months after ECT. Front Psychiatry. 2016;7:200. | ||
Kern RS, Gold JM, Dickinson D, et al. The MCCB impairment profile for schizophrenia outpatients: results from the MATRICS psychometric and standardization study. Schizophr Res. 2011;126(1–3):124–131. | ||
Hasselbalch BJ, Knorr U, Kessing LV. Cognitive impairment in the remitted state of unipolar depressive disorder: a systematic review. J Affect Disord. 2011;134(1–3):20–31. | ||
Kellner CH, Tobias KG, Wiegand J. Electrode placement in electroconvulsive therapy (ECT): A review of the literature. J Ect. 2010;26(3):175–180. | ||
Luo J, Min S, Wei K, et al. Propofol prevents electroconvulsive-shock-induced memory impairment through regulation of hippocampal synaptic plasticity in a rat model of depression. Neuropsychiatr Dis Treat. 2014;10:1847–1859. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.