Back to Journals » International Medical Case Reports Journal » Volume 16
Coexistence of Primary Umbilical Endometriosis and Endometrial Hyperplasia: A Case Report and Review of the Literature
Authors Tilahun T ![]() , Feyera J, Tamene M, Desalegn N, Oljira R
, Feyera J, Tamene M, Desalegn N, Oljira R
Received 5 March 2023
Accepted for publication 30 May 2023
Published 31 May 2023 Volume 2023:16 Pages 323—328
DOI https://doi.org/10.2147/IMCRJ.S411149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Temesgen Tilahun,1 Jiregna Feyera,1 Mathios Tamene,2 Nega Desalegn,3 Rut Oljira4
1Department of Obstetrics & Gynecology, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 2Department of Pathology, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 3Department of Anesthesia, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 4Department of Public Health, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia
Correspondence: Temesgen Tilahun, Department of Obstetrics & Gynecology, Institute of Health Sciences, Wollega University, P.O Box 395, Nekemte, Ethiopia, Tel +251912057186, Email [email protected]
Background: Unusual ectopic growth of endometrial tissue in the umbilicus of a patient who has not undergone surgery is known as primary umbilical endometriosis. When a patient presents with an umbilical nodule, whether or not they have symptoms, it is critical to have a high index of suspicion.
Case Summary: Here, we present a rare case of umbilical endometriosis with concurrent endometrial hyperplasia in a 40-year-old para II patient from Western Ethiopia. A total abdominal hysterectomy and umbilical nodule excision were performed under general anesthesia. After two months, she returned for a follow-up visit and was in good health.
Conclusion: Primary umbilical endometriosis may coexist with endometrial hyperplasia. Hence, in order to provide suitable comprehensive management, a thorough gynecological evaluation is required.
Keywords: umbilical endometriosis, umbilical nodule, endometrial hyperplasia
Introduction
Endometrial tissue that is present outside of the uterus is termed as endometriosis.1–3 The endometrial tissue might be implanted wherever. But pelvis is the most common site.1,2 Cutaneous endometriosis is the term for endometriotic implants that are present in the skin.2 The umbilicus is where cutaneous endometriosis most frequently occurs.4 Umbilical endometriosis accounts for about 0.5–1% of extragenital endometriosis.5–7 It can develop on its own, as in the case of primary umbilical endometriosis or follows prior surgery as in the case of secondary endometriosis.2,4 Villar initially identified primary umbilical endometriosis in 1886 and thus the umbilical nodule is referred as Villar’s nodule.4
Patients with umbilical endometriosis may not exhibit any symptoms or present with various complaints3,8,9 Here we present a case of umbilical endometriosis with concomitant endometrial hyperplasia and presented with typical triads of the umbilical nodule, cyclic pain, and bleeding from the umbilicus.
Case Presentation
This is a 40-year-old para 2 patient from Western Ethiopia who presented to Aba Sena Primary Hospital (ASPH) with triads of umbilical swelling, cyclic umbilical pain and bleeding for 5 months. Her menses comes every 29 days and stays for 5 days. She uses 2 to 3 pads over 24 hours. There is no history of lower abdominal pain.
She had no trauma to her abdomen or umbilicus. She denied bleeding from other body parts. She has no history of urinary or bowel complaints. Both her previous deliveries were spontaneous vaginal deliveries at local health center. She had unremarkable obstetrics complications. She was using jadelle for contraception, but she stopped using it two years before her current presentations. She had completed her family size. Her prior gynecologic, surgical and medical histories are not noteworthy.
She attended clinics and other health institutions where she received treatment with various drugs for the aforementioned ailments. She went to this owing to the lack of improvements.
On examination, she was healthy-looking. Her vital signs were blood pressure (BP) = 123/76mmHg, pulse rate (PR) =84 beats per minute, respiratory rate (RR) =18 breaths per minute, and temperature of 36.5°C. She had pink conjunctivae. Lympho-glandular system, chest, and cardiovascular system were normal. On abdominal examination, there was 2cm by 1.5cm non-tender brownish umbilical nodule (Figure 1). Speculum examination shows no lesion on cervix. The uterus is not enlarged on bimanual exam. On the integumentary system, she had no palmar pallor. On neurologic examination, she was oriented to time, person, and place. She had normal reflexes and no neurologic deficits.
 |
Figure 1 Primary umbilical nodule of a 40-year-old patient, Aba Sena Primary Hospital, Western Ethiopia, 2023. |
An ultrasound of the abdomen and pelvis revealed a 10.3mm thickening of the endometrium. An endometrial biopsy was performed as a result, and the results revealed endometrial hyperplasia without atypia. The surface epidermis of the umbilical nodule is lined by regular stratified squamous epithelium, and the underlying dermis contains nests of benign endometrial glands and stroma as well as hemosiderin pigments embedded in fibrous tissues suggesting endometriosis, according to fine needle aspiration cytology (FNAC) results (Figure 2). During the laboratory inquiry, the results of the chest X-ray (CXR), complete blood count, liver function tests, renal function tests, and urinalysis were all normal (Table 1).
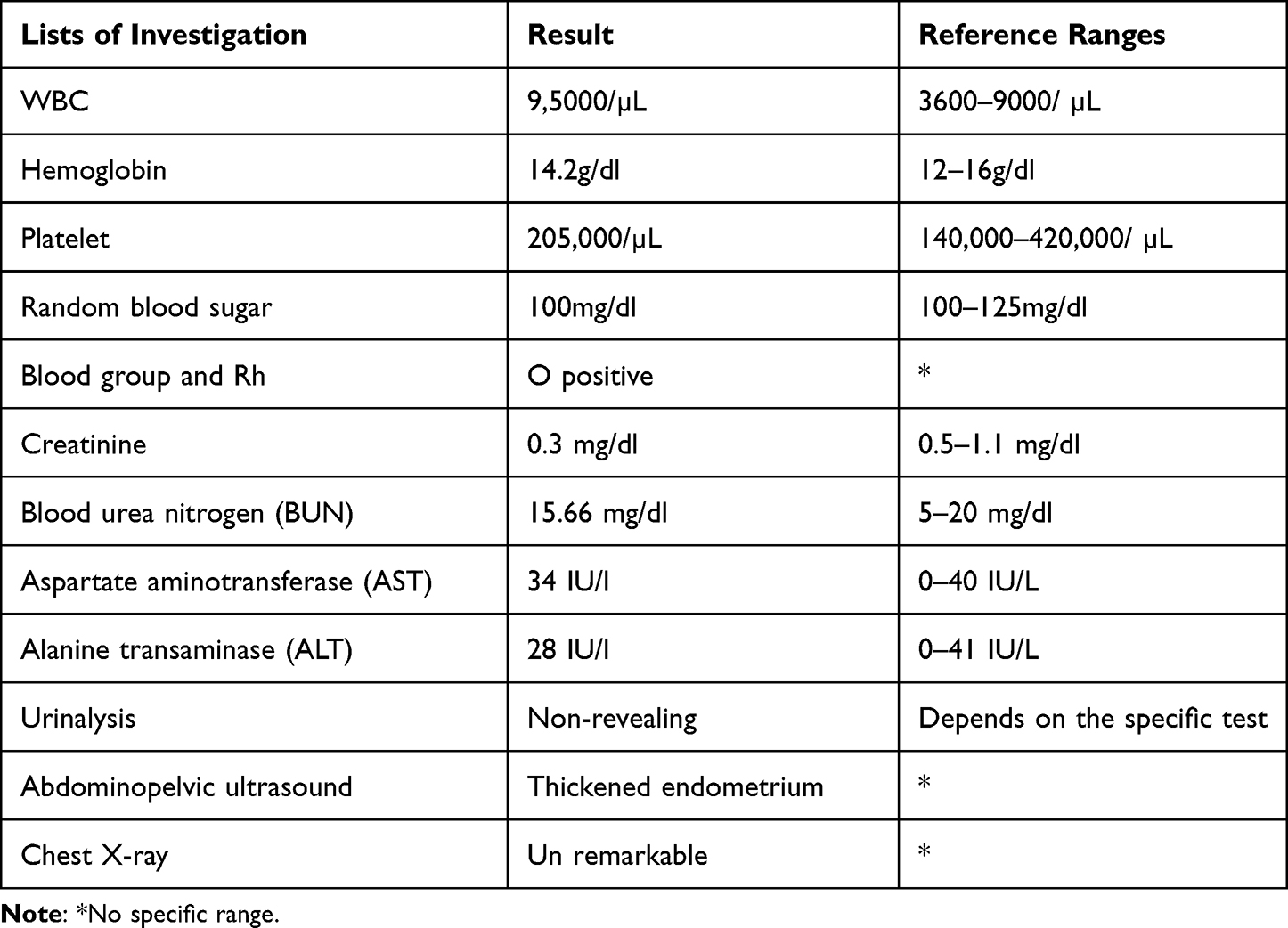 |
Table 1 Laboratory Investigation Results of a 40-Year-Old Patient with Primary Umbilical Endometriosis, Western Ethiopia, 2023 |
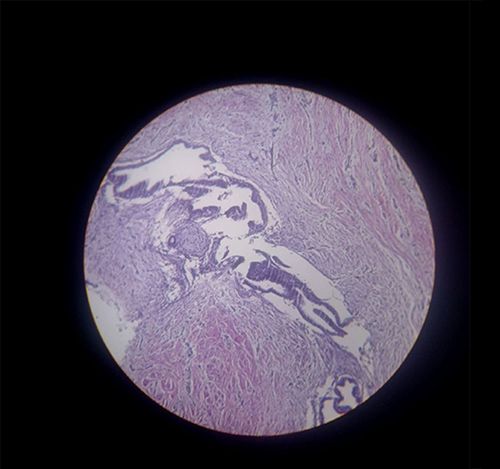 |
Figure 2 Histopathology of umbilical nodule showing benign endometrial tissue with skin overlying it. |
With the final diagnosis of primary umbilical endometriosis and endometrial hyperplasia, the patient was prepared for surgery. The uterus, ovaries, and tubes appear healthy intraoperatively. On the pelvic peritoneal surfaces, there were no adhesions or any signs of endometriosis. A total abdominal hysterectomy and umbilical nodule excision (Figure 3) were performed under general anesthesia. The patient’s surgical recovery went without a hitch, and on the fifth day, the hospital discharged the patient. After two months, she returned for a follow-up visit and was in good health. Subsequent follow up plan was also arranged.
 |
Figure 3 Excised primary umbilical nodule from a 40-year-old patient, Aba Sena Primary Hospital, Western Ethiopia, 2023. |
Discussion
A rare condition, 0.5–4% of cases of endometriosis are caused by umbilical endometriosis.3,5 Yet, the precise etiology is still unclear.10,11 There are various hypotheses on the pathophysiology of primary umbilical endometriosis, though.3,12 Endometrial cells can spread through the blood or lymphatic system from the peritoneum to the umbilicus through obliterated umbilical arteries, metaplasia of the urachus remnant, or the release of endometrial cells that can contaminate the emergence of the umbilical cord during labor and delivery.6,8,9
Umbilical endometriosis usually presents with painful umbilical mass with periodic discharge or bleeding.3,10 The patient in this case exhibits the classic trio of an umbilical nodule, cyclic pain, and bleeding, which is an intriguing aspect of the case. Endometrial hyperplasia is another noticeable feature, and it highlights the value of gynecological evaluation in patients with umbilical endometriosis in order to detect any pelvic involvement or other concurrent gynecologic disorders.3,8,13 In our case, the patient exhibited endometrial hyperplasia but there were no visible signs of pelvic endometriosis. Its coexistence has not yet been documented.
It might be challenging to distinguish clinically between primary umbilical endometriosis and other causes of an umbilical nodule. Umbilical nodules have a wide range of differential diagnoses, from benign conditions (such as granuloma, abscess, sebaceous cyst, lipoma, hemangioma, and umbilical hernia) to malignant conditions (such as Sister Mary Joseph nodule, melanoma, adenocarcinoma, sarcoma, and lymphoma).5,7,10,12 In our case, the patient presented with typical symptoms, and FNAC confirmed the diagnosis.
For the purpose of a clinical workup, the initial evaluation of primary umbilical endometriosis is essentially clinical. The current gold standard for its diagnosis is histopathological confirmation.10–12 A useful invasive diagnostic method is fine-needle aspiration cytology (FNAC). Yet, it can result in the nucleation of endometriotic tissue in new locations, worsening the disease.12,14 Moreover, the report can be 75% inconclusive.12 In our case, the nodule was reachable, making FNAC simple. The anatomical relationships between the nodule and the surrounding tissues can be investigated using radiological techniques such as magnetic resonance imaging, computerized tomography, and ultrasound.7,8,12
There is no clear guideline on the management of umbilical endometriosis.11 Most reports recommend surgical excision as a treatment of choice. Recurrence following excision is said to be uncommon.3,5,8,15 Hormone therapy can be administered prior to surgery to reduce symptoms and shrink big lesions, but it does not have a curative effect.16 For umbilical endometriosis, in our case, local excision was done.
Endometrial hyperplasia is a precancerous lesion of the endometrium that causes a proliferation of endometrial tissue and changes to the architecture of the glands and the relationship of the endometrial gland to the stroma.17 Endometrial hyperplasia is divided into simple and complex hyperplasia, with or without atypia, according to the World Health Organization.18 Progestins are typically used to treat endometrial hyperplasia without atypia, while hysterectomy is the best option for endometrial hyperplasia with atypia. It’s interesting to note that individuals who are concerned about their ability to have children might choose a fertility-sparing treatment for endometrial hyperplasia or early-stage endometrial cancer.19–21 In our situation, a total abdominal hysterectomy was performed because the patient had reached her optimal family size.
Conclusion
Rarely, endometrial hyperplasia may also coexist with primary umbilical endometriosis. Hence, in order to provide suitable comprehensive management, a thorough gynecological evaluation is required.
Abbreviations
CXR, chest x-ray; FNAC, Fine needle aspiration; ASPH, Aba Sena Primary Hospital.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Research Ethics Review Committee of Wollega University. The study protocol is performed per the relevant guidelines.
Consent for Publication
Written informed consent (consent to participate) was obtained from human participant for publication of this case report.
Authors’ Detail
TT is an Associate Professor of Obstetrics & Gynecology, Institute of Health Sciences, Wollega University; JF is an Assistant Professor of Obstetrics & Gynecology, Institute of Health Sciences, Wollega University; MT is an Assistant Professor of Pathology, Institute of Health Sciences, Wollega University; ND is an Assistant Professor of Anesthesia, Institute of Health Sciences, Wollega University; RO is a Lecturer, Department of Public Health, Institute of Health Sciences, Wollega University.
Acknowledgment
We thank the patient for allowing the publication of this case report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
No funding source.
Disclosure
There are no competing interests.
References
1. Gonzalez RH, Singh MS, Hamza SA. Cutaneous endometriosis: a case report and review of the literature. Am J Case Rep. 2021;22:e932493. PMID: 34547012; PMCID: PMC8476184. doi:10.12659/AJCR.932493
2. Agarwal N, Subramanian A. Endometriosis - morphology, clinical presentations and molecular pathology. J Lab Physicians. 2010;2:
3. Mohaghegh F, Hatami P, Rajabi P, et al. Coexistence of cutaneous endometriosis and ovarian endometrioma: a case report. J. Med Case Rep. 2022;16(256). doi:10.1186/s13256-022-03483-8
4. Victory R, Diamond MP, Johns DA. Villar’s nodule: a case report and systematic literature review of endometriosis externa of the umbilicus. J Minim Invasive Gynecol. 2007;14(1):23–32. PMID: 17218225. doi:10.1016/j.jmig.2006.07.014
5. Newme K, Hajong R, Newme R, Newme K. A case report on umbilical endometriosis. J Fam Med Prim Care. 2021;10(7):2716–2717. doi:10.4103/jfmpc.jfmpc_2375_20
6. Dridi D, Chiaffarino F, Parazzini F, et al. Umbilical endometriosis: a systematic literature review and pathogenic theory proposal. J Clin Med. 2022;11(4):995. PMID: 35207266; PMCID: PMC8879338. doi:10.3390/jcm11040995
7. Maharjan S, Satyal B, Baidya R. Spontaneous umbilical endometriosis: a case report. Europasian J Med Sci. 2022;4:16–17. doi:10.46405/ejms.v4i0.431
8. Mba SG, Omeke CA, Enebe JT, Anyanwu OC. Primary umbilical endometriosis coexisiting with multiple uterine fibroids: a case report. Int J Surg Case Rep. 2022;94:107129. doi:10.1016/j.ijscr.2022.107129
9. Dridi D, Buggio L, Donati A, et al. Clinical features and management of umbilical endometriosis: a 30 years’ monocentric retrospective study. Int J Environ Res Public Health. 2022;19:16754. doi:10.3390/ijerph192416754
10. Van den Nouland D, Kaur M. Primary umbilical endometriosis: a case report. Facts Views Vis Obgyn. 2017;9(2):115–119. PMID: 29209489; PMCID: PMC5707772.
11. Nora H, Indirayani I, Maulana R. Management options for primary umbilical endometriosis: a case report. Bali Med J. 2022;11(3):1760–1763. doi:10.15562/bmj.v11i3.3640
12. Capasso L, Sciascia V, Loiaco G, et al. Primary SUBCUTANEOUS umbilical endometriosis: case report and review of the literature. Case Rep Surg. 2020;2020:5. doi:10.1155/2020/8899618
13. Gin TJ, Gin AD, Gin D, Pham A, Cahill J. Spontaneous cutaneous endometriosis of the umbilicus. Case Rep Dermatol. 2013;5:368–372. doi:10.1159/000357493
14. Medeiros FD, Cavalcante DI, Medeiros MA, Eleutério J. Fine-needle aspiration cytology of scar endometriosis: study of seven cases and literature review. Diagn Cytopathol. 2011;39(1):18–21. doi:10.1002/dc.21319
15. Theunissen CI, IJpma FF. Primary umbilical endometriosis: a cause of a painful umbilical nodule. J Surg Case Rep. 2015;2015(3):rjv025. PMID: 25786440; PMCID: PMC4363684. doi:10.1093/jscr/rjv025
16. Makena D, Obura T, Mutiso S, Oindi F. Umbilical endometriosis: a case series. J Med Case Rep. 2020;14(1):142. PMID: 32892752; PMCID: PMC7487815. doi:10.1186/s13256-020-02492-9
17. Chandra V, Kim JJ, Benbrook DM, Dwivedi A, Rai R. Therapeutic options for management of endometrial hyperplasia. J Gynecol Oncol. 2016;27(1):e8. doi:10.3802/jgo.2016.27.e8
18. Auclair MH, Yong PJ, Salvador S, et al. Guideline No. 390-classification and management of endometrial hyperplasia. J Obstet Gynaecol Can. 2019;41(12):1789–1800. doi:10.1016/j.jogc.2019.03.025
19. Tanos P, Dimitriou S, Gullo G, Tanos V. Biomolecular and genetic prognostic factors that can facilitate fertility-sparing treatment (FST) decision making in early stage endometrial cancer (ES-EC): a systematic review. Int J Mol Sci. 2022;23(5):2653. PMID: 35269800; PMCID: PMC8910305. doi:10.3390/ijms23052653
20. Zaami S, Stark M, Signore F, Gullo G, Marinelli E. Fertility preservation in female cancer sufferers: (only) a moral obligation? Eur J Contracept Reprod Health Care. 2022;27(4):335–340. doi:10.1080/13625187.2022.2045936
21. Giampaolino P, Cafasso V, Boccia D, et al. Fertility-sparing approach in patients with endometrioid endometrial cancer grade 2 stage IA (FIGO): a qualitative systematic review. Biomed Res Int. 2022;2022:4070368. PMID: 36203482; PMCID: PMC9532104. doi:10.1155/2022/4070368
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.