Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Co-Occurring Psychiatric and Substance Use Disorders: Clinical Survey Among a Rural Cohort of Italian Patients
Authors Milano G, Vergani HM, Cattedra S, Carrozzino R, Mattioli F ![]() , Robbiano L, Martelli A
, Robbiano L, Martelli A ![]()
Received 9 July 2019
Accepted for publication 23 October 2019
Published 18 December 2019 Volume 2019:15 Pages 3453—3459
DOI https://doi.org/10.2147/NDT.S222567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Giulia Milano,1,* Hayley M Vergani,1,* Simone Cattedra,1 Roberto Carrozzino,2 Francesca Mattioli,1 Luigi Robbiano,1 Antonietta Martelli1
1Department of Internal Medicine, Clinical Pharmacology and Toxicology Unit, University of Genoa, Genoa, Italy; 2Department of Addiction, Health Service ASL2 Savonese, Savona, Italy
*These authors contributed equally to this work
Correspondence: Hayley M Vergani
Department of Internal Medicine, Clinical Pharmacology and Toxicology Unit, University of Genoa, Viale Benedetto XV, 2, Genoa I-16132, Italy
Tel +39 0103538850
Fax +39 0103538232
Email [email protected]
Purpose: Dual diagnosis (DD) is the co-occurrence of both a mental illness and a substance use disorder (SUD). Lots of studies have analysed the integrated clinical approach, which involves both psychiatry and toxicology medical experts. The purpose of this study is to analyse the socio-demographic characteristics and treatment strategies of patients with DD in a rural area of Italy.
Patients and Methods: Clinical data of 750 patients were collected in 2016 through the analysis of health plan records.
Results: The rate of co-occurring disorders is highly variable among people with SUD. In the considered area, patients with DD are 24%, of these only 46.1% have been treated with an integrated clinical program. Moreover, this percentage is further reduced (35.8%) if only patients with heroin use disorder are considered.
Conclusion: A comprehensive revision of DD treatment is needed, especially for people suffering from heroin use disorder and living in remote areas. Meticulous data analysis from other addiction health services of rural areas could be necessary to identify a science-based clinical intervention.
Keywords: dual diagnosis, integrated treatments, substance use disorder, social stigma, rural populations
Introduction
The terms “co-occurring” or “dual diagnosis (DD)” mean the co-occurrence in the same patient of both mental illness (MI) and substance use disorder (SUD).1 MI and SUD are strongly connected, with high prevalence rates of DD among patients with SUD, even if these epidemiological data vary significantly depending on multiple factors such as geographical areas, reference population, study settings, study methodology; moreover, the rate of people with DD seeking health treatment is influenced by several drivers, making realistic epidemiological analysis even more challenging.2 In fact, according to the epidemiological study conducted in 2011 by the Substance Abuse and Mental Health Services Administration, SAMHSA, only 44% of patients with DD was treated for either disorder.3 Just to report some examples of the high prevalence, and high prevalence variability of DD among patients with SUD found by European studies, comorbidity of schizophrenia and SUD prevalence is estimated to be 30–66%,4 comorbidity of depression and SUD prevalence is 12–80%,5 comorbidity of personality disorder and SUD prevalence is 45%.6 Although the absence of a defined epidemiological prevalence rate, the association between MI and SUD is clear.
Many theories have been proposed to explain the link between co-occurrence of SUD and MI, such as the interaction of genetic and environmental factors, which could make an individual more predisposed to these disorders, or the identification of MI as a risk factor for SUD or vice versa.2 One other interesting explanation model could be the “self-medication hypothesis”, which assumes that substances of abuse help individuals to relieve their psychiatric symptoms or negative emotions.7,8 This hypothesis is still under discussion in the scientific literature.9–13 Once discovered, the explanation of the link between co-occurrence of SUD and MI would probably help to develop prevention and treatment programs, but so far, the complex relationship remains largely unknown and poorly understood. Still, psychiatric problems are very common among people with SUD, and this comorbidity is a big challenge for medical doctors, in terms of prevention and treatment.14–16
Primarily, the first problem is how to establish the correct diagnosis, as sometimes symptoms due to substance’s withdrawal or intoxication cannot be clearly distinguished from those associated with MI or produced by psychological conditions.17–18
Secondly, one of the major challenges is how to treat individuals presenting both disorders. A universal agreement on a guideline for the assessment and treatment of the co-occurring disorder has still not been reached.19
Compared to patients with a single psychiatric disorder, dual-diagnosed patients have more complicated treatment processes and sometimes, in these patients, poorer compliance and outcomes are expected as well as higher clinical costs.20 In fact, DD is associated with increased psychiatric hospitalisations and greater propensity to hazardous behaviours which lead, in turn, to higher risk of parenterally transmitted diseases, unemployment and homelessness.2,21 The complexity of this comorbidity may need an integrated medical management and a multiple clinical approach.22
A fully integrated treatment approach, which means that patients are treated and managed by both psychiatrists and toxicologists, so that both psychiatric and substance use disorders are handled by specialized physicians with shared treatment programs, could be more effective than separate treatment plans;23–26 furthermore, uncoordinated services are perceived by patients with DD as one of the major difficulties to their recover.27 Separate programs indeed have some disadvantages: the patients would be in charge of managing two different services, which means coordinating double appointments, and perhaps different therapeutic approaches.2
In Italy, as in most countries, MI and SUD are managed separately: people with SUD are usually chronically managed as outpatients by the drug-treatment territorial services (Servizi Tossicodipendenze, SerT), whilst patients with MI are addressed by mental health territorial services (Centri di Salute Mentale, CMS).
Unfortunately, as the services are historically organized separately, integrated treatments are not easy to implement; moreover, these treatments require personnel, specific training, and adequate infrastructure which, in rural settings such as some Italian areas, are even harder to organize.28
Common perception is that in comparison to urban settings, rural communities are a safer environment in regards of SUD,29 nevertheless some authors reported that rural status confers several general disadvantages, such as less perceived risk, reduced exposure to prevention messages and specific disadvantages for health-care use measures, regardless of poverty and health-care supply.30,31 Besides, Chasnoff and colleagues reported that rural children are more likely to have mental health challenges, such as internalizing behaviours and anxiety or mood disorders, than urban children.32
All patients enrolled in our study lived in an Italian rural area suffering from socio-economic disadvantages: unemployment (due to industrial crisis of the late 1980s) and all medical and social problems linked to the elderly population (28.1% of the inhabitants are aged over 65, with a mean population age of 48.3).33
The aim of the current study is to analyse co-occurring patient’s characteristics, their clinical and socio-demographic situation, as well as clinical treatment strategies in the community addiction health centers (SerT). The first purpose was to find out how the substance use is connected to the environment and to mental illness and secondly, we focused specifically on all integrated clinical interventions proposed to patients with DD.
Materials and Methods
A large retrospective, exploratory and descriptive survey was conducted from April to December 2016 through data collection from selected patient’s medical histories: we enrolled patients with a current age ≥18 year and whose diagnosis obtained from their medical records, satisfied the DSM-5 diagnostic criteria for SUD (with the exception of tobacco cigarettes) and another MI.
Age, sex, substance of abuse, mental illness, type of treatment approach, and other main socio-demographic characteristics, such as educational level, marital status and employment situation were considered.
All subjects included in this analysis were treated in one of the four headquarters (Savona city, Albenga, Finale Ligure and Cairo Montenotte) of Savona’s community addiction health centers (SerT); Savona province, with a total population of 280,707 (ISTAT, 2016),34 is a rural area in the northwest of Italy. The study was approved by the institutional review board “Regional ethic committee – Liguria Region”. Patient’s written consent to review their medical records was collected and the privacy of the participants was guaranteed as collected data were anonymized and maintained with confidentiality. The study was carried out in compliance with the Declaration of Helsinki. A statistical analysis was performed using GraphPad Prism 5 V.502. All statistical tests used the 5% level of significance, and all p-values were two-tailed. Mean and percentages were used for descriptive statistics. Univariate comparisons for categorical data were made between groups using Fisher’s exact test and Student’s t-test for continuous variables.
Results
Clinical histories of 750 patients with SUD were analysed and 180 (24%) of them met the DSM-5 diagnostic criteria for another MI satisfying therefore the definition of patients with DD.
Subjects were predominantly male (n=126; 70%), Italians (n= 168; 93.3%), with a mean age of 45.7± 9.3 years (min= 22; max=74). Only a minority of patients had one or more children (n=71; 39.4%) and 135 subjects (75%) were unmarried at the time of clinical assessment. The majority of patients finished primary school (n= 168; 93.3%) and 84 patients (46.7%) were unemployed. Mean age, education level, state of employment, marital status did not statistically differ between genders, whilst women were more likely to have children than men (p=0.0016). Only 71 subjects (39.4%) had familiarity with SUD and/or MI (Table 1).
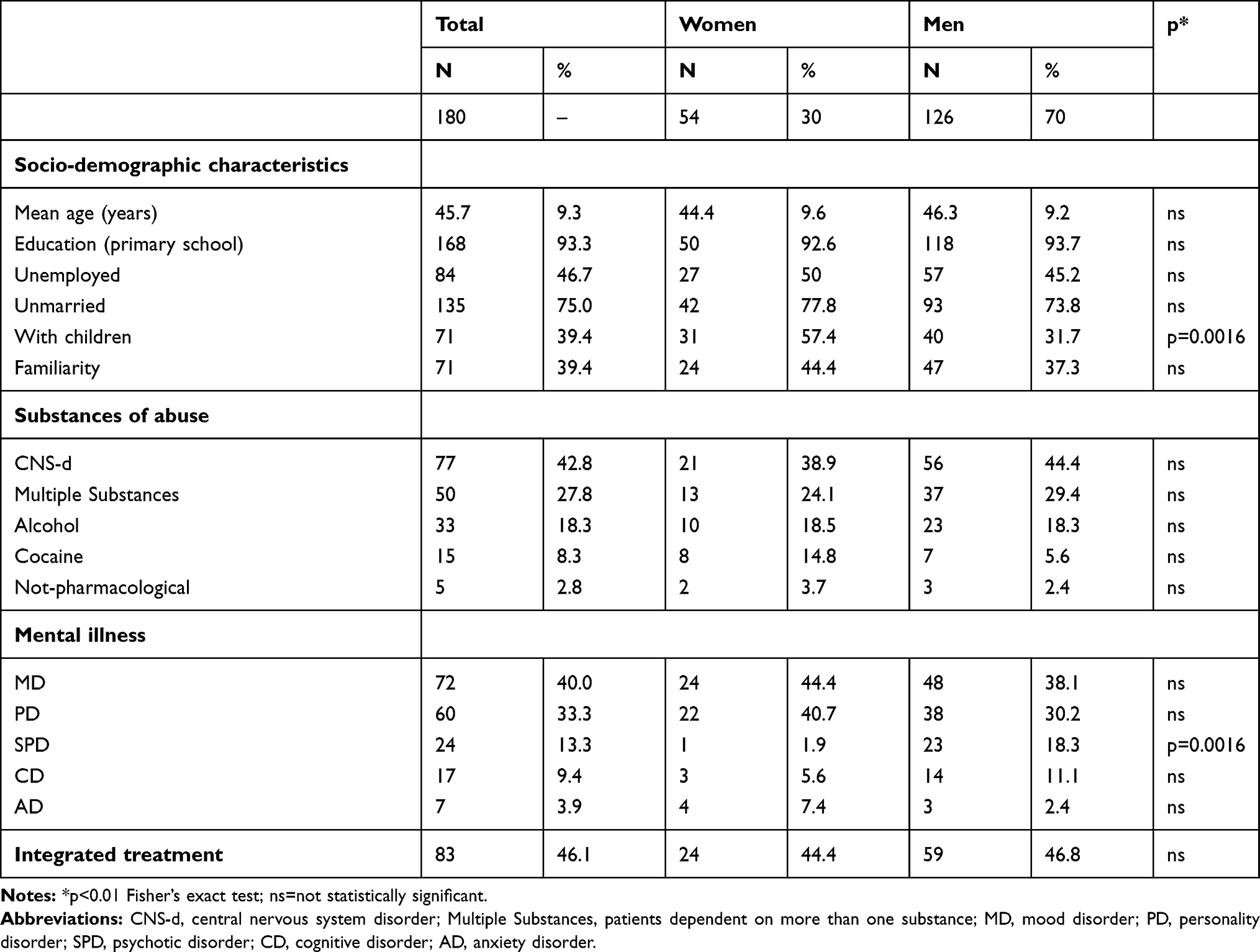 |
Table 1 Socio-Demographic and Descriptive Data |
All enrolled patients had heroin, cocaine, cannabis, alcohol and/or a non-pharmacological addiction (gambling and shopping). Specifically: 77 (42.8%) were dependent on central nervous system depressants (CNS-d), respectively, 68 patients (88.3%) had heroin and 9 cannabis use disorder; 50 patients (27.8%) had a multiple substance addiction, respectively, 25 subjects on heroin & cocaine, 21 on heroin & cocaine & cannabis, 1 on cocaine & cannabis and 3 were heroin & cannabis users, indeed basically almost all patients dependent on more than one substance (49 subjects) had heroin as one of their substance of abuse; 33 patients (18.3%) had an alcohol use disorder; 15 (8.3%) were dependent on cocaine; 5 patients (2.8%) had a non-pharmacological addiction, respectively, 4 subjects had a gambling disorder and 1 had a compulsive shopping disorder (Table 1).
In the same perspective the following psychiatric diseases were identified: 72 patients (40%) were diagnosed with a mood disorder (MD); 60 patients (33.3%) with a personality disorder (PD); 24 (13.3%) with schizophrenia or other psychotic disorder (SPD); 17 (9.4%) had a cognitive disorder (CD) and only 7 patients (3.9%) had an anxiety disorder (AD). Except for SPD, which was more common among males (p=0.0016), psychiatric disease prevalence did not statistically differ between genders.
The cross analysis of data shows that among patients with CNS-d addiction (N = 77), the majority had a PD (32.5%), then the remaining patients had a MD (31.2%), a SPD (22.1%), a CD (10.4%) and only 3.9% had an AD (Table 2). Among patients dependent on more than one substance (N = 50), 44% had a PD and 36% a MD. The remaining 20% of patients had CD (10%), SPD (6%) and AD (4%). Among subjects with alcohol use disorder (N = 33), the majority (57.6%) had a diagnosis of MD, 21.2% of PD, 9.1% of CD, 9.1% of SPD and only 3% of AD (Table 2).
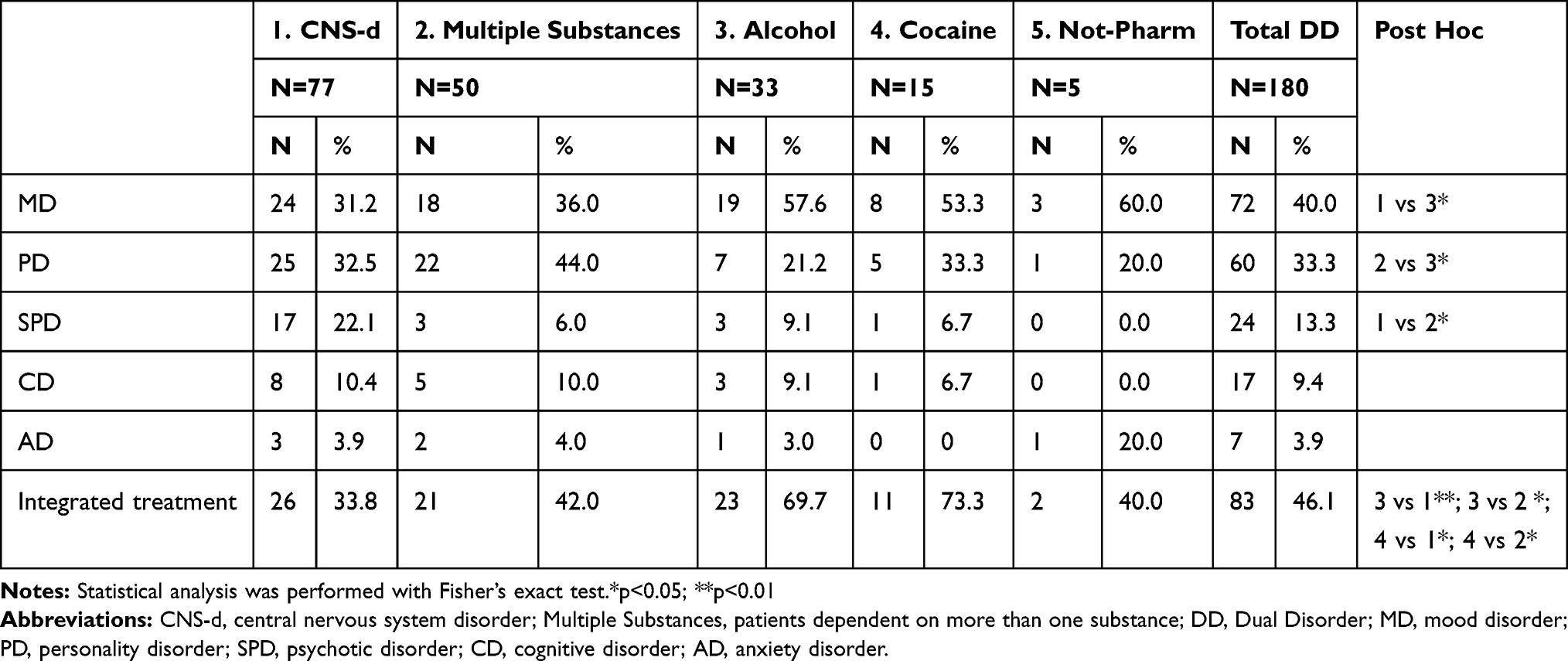 |
Table 2 Cross Analysis of Data |
Among people with cocaine use disorder (N = 15), 53.3% had a diagnosis of MD; 33.3% of PD; both SPD and CD were diagnosed in the 6.7% of patients.
Among the patients with a non-pharmacological addiction (N = 5), three had a diagnosis of MD, one of AD and a one of PD.
By comparing the prevalence of psychiatric diseases of patients with different substance addiction (Post hoc analysis, Table 2), we found that MD was more common in patients with a non-pharmacological addiction, but a statistical significant difference was detectable only between patients with alcohol use disorder and patients with CNS-d addiction (p<0.05); PD was more common in patients who had a multiple substance addiction, especially in respect with subjects with alcohol use disorder (p<0.05). Finally, SPD was statistically more common in patients on CNS-d than in patients with multiple substance addiction (p<0.05).
Only 83 subjects (46.1%) were steadily monitored and treated with an integrated program; this percentage is further reduced when considering only patients with CNS-d addiction (33.8%) and patients dependent on more than one substance (42%); patients dependent on cocaine or alcohol were more frequently involved in integrated programs, with 73.3% and 69.7% of patients treated, respectively. Statistical analysis showed the following significant difference in rate of integrated treatment when comparing the above-mentioned substance of abuse: subjects with alcohol use disorder are more involved in integrated treatments than patients on CNS-d (p<0.01) and patients dependent on more than one substance (p<0.05), similarly, subjects with cocaine use disorder are more involved than patients on CNS-d (p<0.05) and patients dependent on more than one substance (p<0.05).
Discussion
A European review estimated the rate of comorbidity in people with SUD to be as high as 50%,2 in our study, we found a DD rate of 24%. As mentioned in the introduction, DD prevalence rate varies considerably among different studies, because of several biases, making data very difficult to compare: the DD rate that we recorded, which seems to be far lower than the mean European prevalence reported, becomes immediately more in line with the 31% rate recorded in 2006 by the SIMI-Italia data collection system, a national study which collected data, similar to our study, in an Italian population of patients attending SerT.2 The rate of DD could also have been influenced by the socio-demographic characteristics of patients, such as rate of unemployment, education, mean population age and general economic conditions, as well as by the area of residence (i.e. rural settings/urban areas); to this purpose, available data suggest that a variety of socio/familiar/demographic factors are powerful predictors of difference in prevalence of SUD.35
Some authors report that rural populations have less social risk factors and deprivations than urban inhabitants,36 which could in part explain the particularly low prevalence of DD in our study. Furthermore, in remote and isolated areas there is a high rate of stigmatization,37–39 which may interfere with access to all treatment services and treatment seeking behaviours related to SUD,29,37 so that our data could underestimate the real extent of DD prevalence.
In addition to stigmatization, rural areas present also further barriers to the delivery of clinical services in mental health settings, such as economic, administrative and organizational impediments.40
Regional organization and collaboration between addiction health centers and mental health services are crucial to implement integrated treatments, which are demonstrated to be essential for improving the quality of life and clinical outcomes of DD patients.41
Literature reports that unfortunately only a minority of individuals with DD receive integrated interventions,24 intended as a multi-disciplinary treatment involving both the psychiatric and substance use health services.
In Italy, the addiction health services, which provide treatment in the areas of social work, psychology, nursing and medical toxicology (substance use) for people with SUD, do not usually include psychiatric health services.42 In line with the international literature, this study found out that the majority of DD patients (53.9%), living in the considered rural area, are only treated by the addiction health center teams, whilst only 46% of patients were treated with an integrated program.
Looking further into our data, we found out that access to this superior type of treatment varies among patients, depending on the substance of abuse. Specifically, integrated programs involved mainly patients on cocaine or alcohol (73.3% and 69.7% of patients, respectively), versus 42% of patients dependent on more than one substance and 33.8% of patients on CNS-d.
This last group of patients included cannabis users, of which 55.5% (5 out of 9 patients) were steadily monitored with an integrated program, and patients with heroin addiction, of which only 30.8% received the integrated intervention (21 out of 68 patients). As almost all patients dependent on more than one substance had heroin as one of their substance of abuse (49 out of 50 subjects), the percentage of all patients on heroin (adding “CNS-d” plus “patients dependent on more than one substance”) receiving an integrated treatment is 35.8%. This suggests that patients with co-occurrence heroin dependence, at least in comparison with DD people addicted to alcohol or cocaine, are less likely to receive integrated interventions.
Stigmatizing attitudes could be a possible explanation for this exclusion. In general, stigmatizing attitudes in the population may arise from the belief that addiction is a sort of “vice”, not a proper mental illness, thereby making it misunderstood. Woo et al. reported that patients in methadone maintenance treatment are stigmatized, with higher experiences of self- and perceived stigma associated with heroin use.43 Moreover, health-care workers were identified as one of the most important source of perceived stigma;44 this kind of “health-care stigma” can negatively interfere with access of heroin users to all health-care services.
Conclusion
An integrated approach for DD patients, which is considered to be more appropriate to improve adherence and clinical outcome, appears to be hardly available especially for those people living in remote areas and for patients with heroin addiction. Anyway, meticulous data analysis from other addiction health services from rural settings are necessary to analyse the situation and hopefully to establish a gold standard of practice.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that there are no known conflicts of interest.
References
1. Brems C, Johnson ME, Wells RS, Burns R, Kletti N. Rates and sequelae of the coexistence of substance use and other psychiatric disorders. Int J Circumpolar Health. 2002;61:224–244. doi:10.3402/ijch.v61i3.17456
2. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Comorbidity of substance use and mental disorders in Europe; 2015. Available from: http://www.emcdda.europa.eu/attachements.cfm/att_245096_EN_TDXD15019ENN.pdf.
3. Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2010 National Survey on Drug Use and Health: summary of National Findings; 2011. Available from: https://www.samhsa.gov/data/sites/default/files/NSDUHNationalFindingsResults2010-web/2k10ResultsRev/NSDUHresultsRev2010.pdf.
4. Green AI. Schizophrenia and comorbid substance use disorder: effects of antipsychotics. J Clin Psychiatry. 2005;66:21–26.
5. Torrens M, Martínez-Sanvisens D, Martínez-Riera R, Bulbena A, Szerman N, Ruiz P. Dual diagnosis: focusing on depression and recommendations for treatment. Addict Disord Their Treat. 2011;10:50–59. doi:10.1097/ADT.0b013e318215f322
6. Langås AM, Malt UF, Opjordsmoen S. In-depth study of personality disorders in first-admission patients with substance use disorders. BMC Psychiatry. 2012;12:180. doi:10.1186/1471-244X-12-180
7. Khantzian EJ. The self-medication hypothesis of addictive disorders: focus on heroin and cocaine dependence. Am J Psychiatry. 1985;142:1259–1264.
8. Khantzian EJ. The self-medication hypothesis of substance use disorders: a reconsideration and recent applications. Harv Rev Psychiatry. 1997;4:231–244. doi:10.3109/10673229709030550
9. Dervaux A, Baylé FJ, Laqueille X, et al. Is substance abuse in schizophrenia related to impulsivity, sensation seeking, or anhedonia? Am J Psychiatry. 2001;158:492–494. doi:10.1176/appi.ajp.158.3.492
10. Goswami S, Mattoo SK, Basu D, Singh G. Substance-abusing schizophrenics: do they self-medicate? Am J Addict. 2004;13:139–150. doi:10.1080/10550490490435795
11. Bizzarri JV, Rucci P, Sbrana A, et al. Substance use in severe mental illness: self-medication and vulnerability factors. Psychiatry Res. 2009;165:88–95. doi:10.1016/j.psychres.2007.10.009
12. Mariani JJ, Khantzian EJ, Levin FR. The self‐medication hypothesis and psychostimulant treatment of cocaine dependence: an update. Am J Addict. 2014;23:189–193. doi:10.1111/vsu.v23.2
13. Pettersen H, Ruud T, Ravndal E, Landheim A. Walking the fine line: self-reported reasons for substance use in persons with severe mental illness. Int J Qual Stud Health Well-Being. 2013;8:21968. doi:10.3402/qhw.v8i0.21968
14. Bizzarri JV, Casetti V, Panzani P, et al. Risky use and misuse of alcohol and cigarettes in psychiatric inpatients: a screening questionnaire study. Compr Psychiatry. 2016;70:9–16. doi:10.1016/j.comppsych.2016.05.011
15. Najt P, Fusar-Poli P, Brambilla P. Co-occurring mental and substance abuse disorders: a review on the potential predictors and clinical outcomes. Psychiatry Res. 2011;186:159–164. doi:10.1016/j.psychres.2010.07.042
16. Martins SS, Gorelick DA. Conditional substance abuse and dependence by diagnosis of mood or anxiety disorder or schizophrenia in the US population. Drug Alcohol Depend. 2011;119:28–36. doi:10.1016/j.drugalcdep.2011.05.010
17. Roncero C, Gómez-Baeza S, Vázquez JM, et al. Perception of Spanish professionals on therapeutic adherence of dual diagnosis patients. Actas Esp Psiquiatr. 2013;41:319–329.
18. Pani PP, Trogu E, Vigna-Taglianti F, et al. Psychopathological symptoms of patients with heroin addiction entering opioid agonist or therapeutic community treatment. Ann Gen Psychiatry. 2014;13:35. doi:10.1186/s12991-014-0035-x
19. Berenz EC, Coffe SF. Treatment of co-occurring posttraumatic stress disorder and substance use disorders. Curr Psychiatry Rep. 2012;14:469–477. doi:10.1007/s11920-012-0300-0
20. Sterling S, Chi F, Hinman A. Integrating care for people with co-occurring alcohol and other drug, medical, and mental health conditions. Alcohol Res Health. 2011;33:338–349.
21. Di Lorenzo R, Galliani A, Guicciardi A, et al. A retrospective analysis focusing on a group of patients with dual diagnosis treated by both mental health and substance use services. Neuropsychiatr Dis Treat. 2014;10:1479–1488. doi:10.2147/NDT.S65896
22. Kêdoté MN, Brousselle A, Champagne F. Use of health care services by patients with co-occurring severe mental illness and substance use disorders. Ment Health Subst Use. 2008;1:216–227. doi:10.1080/17523280802274886
23. Green CA, Yarborough MT, Polen MR, Janoff SL, Yarborough BJH. Dual recovery among people with serious mental illnesses and substance problems: a qualitative analysis. J Dual Diagn. 2015;11:33–41. doi:10.1080/15504263.2014.975004
24. Drake RE, O’Neal EL, Wallach MA. A systematic review of psychosocial research on psychosocial interventions for people with co-occurring severe mental and substance use disorders. J Subst Abuse Treat. 2008;34:123–138. doi:10.1016/j.jsat.2007.01.011
25. Ziedonis DM, Smelson D, Rosenthal RN, et al. Improving the care of individuals with schizophrenia and substance use disorders: consensus recommendations. J Psychiatr Pract. 2005;11:315–339. doi:10.1097/00131746-200509000-00005
26. Dixon LB, Dickerson F, Bellack AS, et al. The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements. Schizophr Bull. 2010;36:48–70. doi:10.1093/schbul/sbp115
27. Ness O, Borg M, Davidson L. Facilitators and barriers in dual recovery: a literature review of first-person perspectives. Adv Dual Diagn. 2014;7:107–117. doi:10.1108/ADD-02-2014-0007
28. Murthy P, Mahadevan J, Chand PK. Treatment of substance use disorders with co-occurring severe mental health disorders. Curr Opin Psychiatry. 2019;32:293–299. doi:10.1097/YCO.0000000000000510
29. Milano G, Saenz E, Clark N, et al. Report on the International Workshop on Drug Prevention and Treatment in Rural Settings Organized by United Nation Office on Drugs and Crime (UNODC) and World Health Organization (WHO). Subst Use Misuse. 2017;52:1801–1807. doi:10.1080/10826084.2017.1306564
30. Caldwell JT, Ford CL, Wallace SP, Wang MC, Takahashi LM. Intersection of living in a rural versus urban area and race/ethnicity in explaining access to health care in the United States. Am J Public Health. 2016;106:1463–1469. doi:10.2105/AJPH.2016.303212
31. Monnat SM, Rigg KK. Examining rural/urban differences in prescription opioid misuse among US adolescents. J Rural Health. 2016;32:204–218. doi:10.1111/jrh.2016.32.issue-2
32. Chasnoff IJ, Telford E, Wells AM, King L. Mental health disorders among children within child welfare who have prenatal substance exposure: rural vs. urban populations. Child Welfare. 2015;94:53–70.
33. ISTAT, National Institute of Statistics. Available from: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_INDDEMOG1#.
34. ISTAT, National Institute of Statistics. Available from: http://dati.istat.it/Index.aspx?QueryId=18967.
35. Judd FK, Jackson HJ, Komiti A, Murray G, Hodgins G, Fraser C. High prevalence disorders in urban and rural communities. Aust N Z J Psychiatry. 2002;36:104–113. doi:10.1046/j.1440-1614.2002.00986.x
36. Mueser KT, Essock SM, Drake RE, Wolfe RS, Frisman L. Rural and urban differences in patients with a dual diagnosis. Schizophr Res. 2001;48:93–107. doi:10.1016/S0920-9964(00)00065-7
37. Browne T, Priester MA, Clone S, Iachini A, DeHart D, Hock R. Barriers and facilitators to substance use treatment in the rural south: a qualitative study. J Rural Health. 2016;32:92–101. doi:10.1111/jrh.12129
38. Benoit C, McCarthy B, Jansson M. Stigma, sex work, and substance use: a comparative analysis. Sociol Health Illn. 2015;37:437–451. doi:10.1111/shil.2015.37.issue-3
39. King R. Science over stigma saving lives—implementation of Naloxone use in the school setting. NASN School Nurse. 2016;31:96–101. doi:10.1177/1942602X16628890
40. Guerrero EG, Padwa H, Lengnick-Hall R, Kong Y, Perrigo JL. Leadership and licensure for drug treatment and the implementation of co-occurring disorder treatment in community mental health centers. Community Ment Health J. 2015;51:554–566. doi:10.1007/s10597-015-9886-0
41. Lozano ÓM, Rojas AJ, Fernández Calderón F. Psychiatric comorbidity and severity of dependence on substance users: how it impacts on their health-related quality of life? J Ment Health. 2017;26:119–126. doi:10.1080/09638237.2016.1177771
42. Kavanagh DJ, McGrath J, Saunders JB, Dore G, Clark D. Substance misuse in patients with schizophrenia: epidemiology and management. Drugs. 2002;62:743–755. doi:10.2165/00003495-200262050-00003
43. Woo J, Bhalerao A, Bawor M, et al. “Don’t judge a book its cover”: a qualitative study of methadone patients’ experiences of stigma. Subst Abuse. 2017;11:1178221816685087.
44. Garcia-Portilla MP, Bobes-Bascaran MT, Bascaran MT, Saiz PA, Bobes J. Long term outcomes of pharmacological treatments for opioid dependence: does methadone still lead the pack? Br J Clin Pharmacol. 2014;77:272–284. doi:10.1111/bcp.2014.77.issue-2
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.