Back to Journals » Infection and Drug Resistance » Volume 19
Clinicopathologic Features of Genitourinary Malakoplakia and Analytical Utility of the MetaPath Assay
Received 19 November 2025
Accepted for publication 5 February 2026
Published 12 February 2026 Volume 2026:19 582917
DOI https://doi.org/10.2147/IDR.S582917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Lin He, Fen Li
Department of Pathology, Sichuan University Affiliated Chengdu Second People’s Hospital, Chengdu Second People’s Hospital, West China School of Medicine, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China
Correspondence: Fen Li, Department of Pathology, Sichuan University affiliated Chengdu Second People’s Hospital, Chengdu Second People’s Hospital, West China School of Medicine, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China, Email [email protected]
Purpose: To describe the clinicopathological spectrum of genitourinary malakoplakia (MPL) and to evaluate the feasibility and clinical impact of metagenomic pathogen detection (MetaPath) performed on archival formalin-fixed paraffin-embedded (FFPE) tissue.
Patients and Methods: Clinical imaging, histopathology, immunohistochemistry, special stains and MetaPath results were retrospectively analysed in five MPL cases diagnosed between January 2019 and August 2025.
Results: The cohort comprised four men and one woman with a median age of 65.4 years. Four lesions arose in the prostate and one in the bladder. Histology showed chronic granulomatous inflammation with numerous eosinophilic histiocytes containing 5– 10 μm targetoid Michaelis–Gutmann bodies. CD68 and CD163 were diffusely positive; PAS and iron stains highlighted the inclusions. MetaPath identified pathogens in 3/5 (60%) FFPE specimens (Escherichia coli in two, Pseudomonas aeruginosa in one). Antibiotic regimens were adjusted according to MetaPath results. After a median follow-up of 6 months (range 4– 8) all patients remained symptom-free.
Conclusion: MPL is frequently misdiagnosed as malignancy. MetaPath can reliably detect pathogens in archival tissue and guide targeted antimicrobial therapy, representing a valuable adjunct to conventional culture.
Keywords: malakoplakia, Michaelis–Gutmann body, malakoplakia concurrent with prostate cancer, metagenomic pathogen detection technology, special stains
Introduction
Malakoplakia (MPL) is a rare chronic granulomatous disorder that most frequently involves the genitourinary tract.1 Since its first description by Michaelis and Gutmann in 1902 the pathognomonic Michaelis–Gutmann (M-G) body has remained the histological cornerstone of diagnosis.2 The aetiology is incompletely understood; impaired macrophage killing of Gram-negative bacteria—especially Escherichia coli—is considered central.3–5 Consequently, demonstration of the causative organism would strengthen both diagnostic certainty and therapeutic precision.
Conventional urine or blood cultures often fail to identify the responsible pathogen, particularly when antibiotics have been administered or when only archival tissue is available. Metagenomic next-generation sequencing (mNGS) has recently been applied to fresh clinical samples, but its sensitivity in formalin-fixed paraffin-embedded (FFPE) tissue is limited because of human DNA over-representation and DNA fragmentation.6–8 MetaPath is a novel capture-based metagenomic assay that enriches microbial reads and depletes host nucleic acids, thereby allowing pathogen detection from FFPE specimens.9–11
We report the largest single-centre genitourinary MPL series to date and provide the first proof-of-concept that MetaPath can reliably identify pathogens in FFPE lesions, guiding targeted antibiotic therapy.
Materials and Methods
Study Cohort
After Institutional Review Board approval (2020105) we retrieved all MPL cases diagnosed at Chengdu Second People’s Hospital between January 2019 and August 2025. Inclusion required (i) typical histology with M-G bodies, (ii) archived FFPE tissue and (iii) available clinical follow-up.
Histopathology, Special Stains and Immunohistochemistry
Sections (4 µm) were stained with H&E, PAS and iron. Immunohistochemistry was performed on an automated Leica Autostainer Link 48 using antibodies against CD68, CD163, PCK, PSA, NKX3.1, p63, 34βE12, P504S, S100, ALK, Langerin, CD1a and Ki67 (Maixin Biotech, Fuzhou, China). Appropriate positive and negative controls were included. All slides were independently reviewed by two experienced pathologists.
MetaPath Workflow
DNA was extracted from five 4 µm FFPE curls as previously described.9 Libraries were prepared by mechanical fragmentation (350 bp), end-repair, adapter ligation and eight-cycle PCR. Pools were enriched with the MetaPath capture panel (KingCreate, China) targeting 3,125 clinically relevant pathogens. Sequencing (100-bp single-end) aimed at ≥300,000 reads per sample was performed on an Illumina MiniSeq. Raw reads were demultiplexed (bcl2fastq v2.20), quality-filtered (Fastp; Q ≥20) and mapped to GRCh38 to remove human sequences. Remaining reads were aligned to an in-house NCBI pathogen database. A pathogen was called when ≥3 unique genomic regions were covered at ≥10 RPM. Results were visually confirmed with IGV.
Results
Baseline characteristics are summarised in Table 1. Median age was 65.4 years; four patients presented with voiding difficulty and one with left flank pain. Pre-operative PSA ranged 1.0–10.8 ng/mL. Imaging suggested bladder tumour (n = 1) or prostatic hyperplasia/cancer (n = 4).
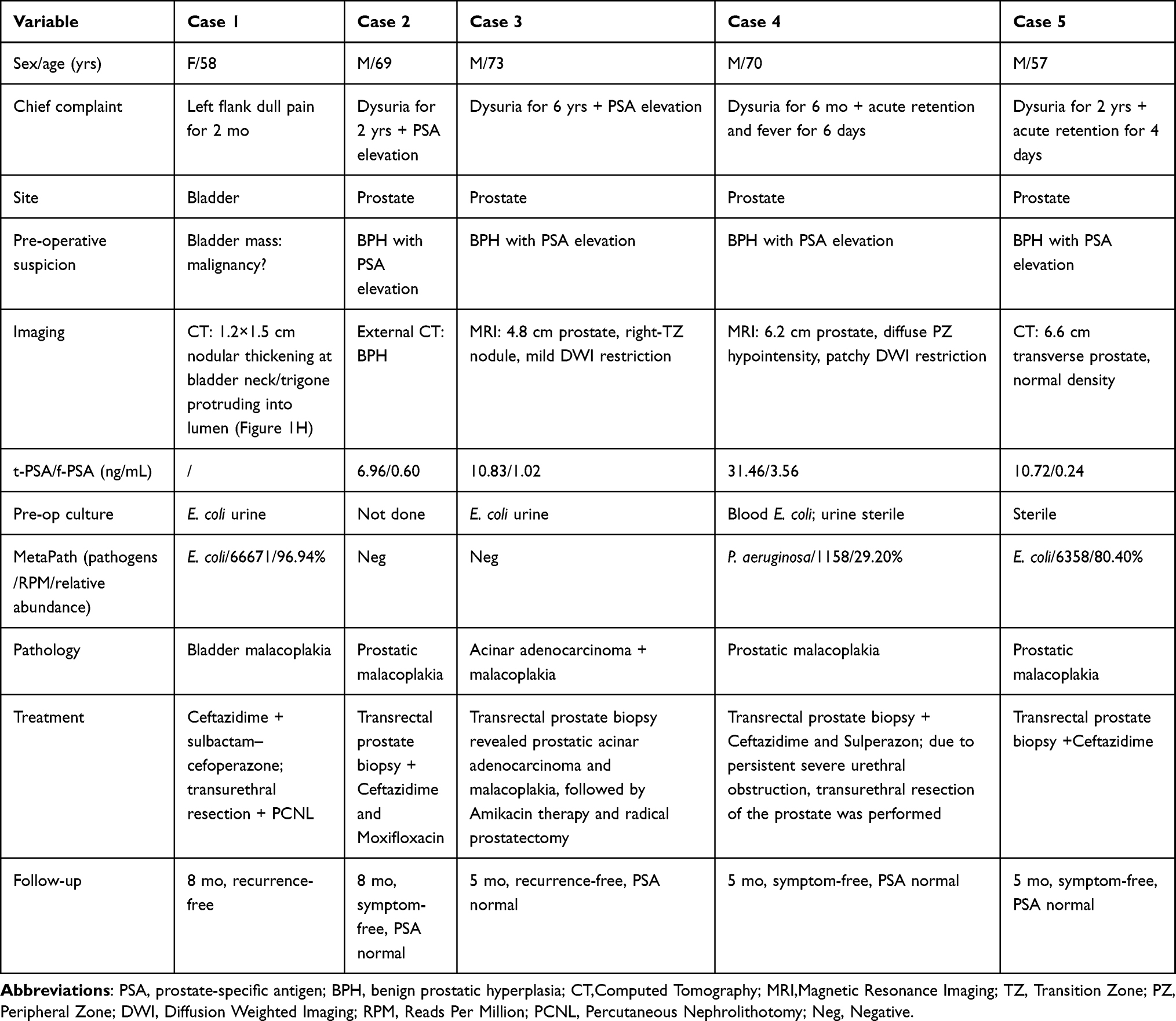 |
Table 1 Clinicopathological Summary of the Five Genitourinary Malacoplakia Patients |
Histology
All specimens showed sheets of eosinophilic histiocytes with abundant granular cytoplasm and extracellular 5–10 µm targetoid M-G bodies (Figure 1A and B). Background infiltrates included sparse lymphocytes, plasma cells and neutrophils. Histiocytes showed diffuse positivity for CD68 (Figure 1C) and CD163, low Ki67 index, and were negative for S100 (Figure 1D), PCK, PSA, NKX3.1, p63, 34βE12, P504S, ALK, Langerin and CD1a. Epithelial, neuroendocrine and Langerhans markers were negative. PAS and iron stains confirmed M-G bodies (Figure 1E and F).
 |
Figure 1 Representative images of case 1and 3 (bladder and prostate malakoplakia). (A) Diffuse infiltrate of eosinophilic histiocytes (H&E) (red arrow); overlying bladder mucosa (blue arrow). (B) Targetoid Michaelis–Gutmann bodies (red arrow), histiocyte nuclei and nucleoli (blue arrows). (C) CD68 diffusely positive (red arrow); bladder mucosa (blue arrow). (D) S100 negative (red arrow) in histiocytes bladder mucosa (blue arrow). Antigen-presenting or inflammatory mediator cells positive (black arrows). (E) PAS staining (red arrow). (F) Iron staining (red arrow). (G) MetaPath coverage plot for Escherichia coli. E. coli, 66,671 reads, relative abundance 96.87%, coverage 0.49% (25,543/5,223,257 bp), with uniform genome-wide distribution. (H) CT showing nodular thickening of the bladder neck (red arrow). (I) Concurrent prostatic adenocarcinoma (P504S staining) (red arrow); normal prostatic glands exhibit weak cytoplasmic staining (blue arrows). (J) Concurrent prostatic adenocarcinoma (p63 staining) (red arrow); basal cells of normal glands positive (blue arrows). |
MetaPath Findings
Pathogens were identified in 3 of 5 cases (60%): Escherichia coli in Cases 1 (66,671 RPM, 96.9% relative abundance; Figure 1G) and 5 (6,358 RPM, 80.4% relative abundance), and Pseudomonas aeruginosa in one case (1,158 RPM, 29.2% relative abundance). No clinically relevant fungi, viruses, or parasites were detected. Cases 2 and 3 showed only low-level skin commensals below the detection threshold.
Concordance with Cultures
Pre-operative mid-stream urine was positive for E. coli in 3/4 patients (75%). Blood culture yielded E. coli in case 4. MetaPath and urine culture were concordant in 2/3 positive cases; case 4 displayed mixed organisms (E. coli in blood vs P. aeruginosa in tissue), suggesting polymicrobial infection.
Treatment and Outcome
Antibiotic regimens were adjusted according to MetaPath and resistance genes (Table 1). All patients received antimicrobials that achieve high intracellular concentration (ceftazidime, cefoperazone-sulbactam or amikacin). After 4–8 months’ follow-up all remained symptom-free; PSA normalised in the four prostate cases and imaging showed no residual mass.
Discussion
Clinical presentation of malakoplakia varies by site. Bladder lesions typically appear as solitary yellowish plaques or nodules mimicking malignancy, producing abdominal pain, abdominal mass, or irritative voiding symptoms;12 case 1 showed a nodular mass at the bladder neck/trigone (Figure 1H) and was pre-operatively suspected of cancer. Prostatic malakoplakia usually presents with dysuria;13 cases 2–5 all had dysuria and elevated PSA, raising pre-operative concern for prostate cancer. Histologically, all specimens showed eosinophilic histiocytic infiltrates forming non-necrotising granulomas; many histiocytes contained 5–10 µm spherical inclusions (M–G bodies) with targetoid lamination. PAS and iron stains confirmed their presence, and immunohistochemistry excluded other disorders, fulfilling diagnostic criteria for malakoplakia.
Malakoplakia is classically linked to Gram-negative bacteria, especially Escherichia coli, that reach the tissue via the urinary or gastrointestinal tract and trigger a localized inflammatory response.4 Although urine cultures can document urinary infection, defining the species, burden and resistance profile of the pathogens provides more direct insight into disease pathogenesis and therapy. In 2021, Yan Z14 reported the first renal allograft malakoplakia verified by both histopathology and metagenomic detection of E. coli sequences in urine and graft tissue; however, metagenomic identification of pathogens directly within lower urinary-tract or prostatic malakoplakia lesions has not previously been described.
MetaPath identified pathogens in 3/5 cases (60%): E. coli in two (66,671 and 6,358 RPM; 96.9% and 80.4% relative abundance) and P. aeruginosa in one (1,158 RPM; 29.2% relative abundance). The 10-fold higher bacterial load in case 1 versus case 5 suggests a correlation between microbial burden and lesion severity. Although the read count for P. aeruginosa in case 4 was low, the assignment confidence was 99%. Cases 2 and 3 yielded only skin commensals, likely introduced during transperineal biopsy; advanced fibrosis may also reduce organism numbers, causing false negatives. MetaPath delivered results within 2–3 days and, by targeting lesional tissue, provided direct evidence of intralesional organisms; however, contamination and commensal overgrowth must be excluded. Mid-stream urine cultures were positive for E. coli in 3/4 patients (75%). Concordance with MetaPath was complete for case 1. In case 4, blood culture grew E. coli whereas MetaPath detected P. aeruginosa, indicating polymicrobial infection with a dominant and a residual pathogen. Case 5 had negative urine culture but E. coli was recovered by MetaPath, underscoring its superior sensitivity for low-density infections. Therapy guided by species and resistance-gene predictions achieved microbiological and clinical cure without adverse events. Combining meticulous micro-dissection with histological validation minimises misinterpretation.
Prostatic malakoplakia (PM) concurrent with prostate cancer (PCa) is exceedingly rare. Only 25 cases have been reported; five remained recurrence-free, one progressed at 3 years, one progressed without surgery, and 18 were lost to follow-up. Five men developed sepsis or sudden prostatic enlargement ≥2 weeks after biopsy, implying PM may be a rare post-biopsy complication, yet its impact on PCa prognosis remains undefined.15–17 In case 3, biopsy revealed both PCa (Figure 1I and J) and PM; radical specimen showed bilateral cancer, whereas PM was confined to the apex, indicating topographically distinct coexistence. Two preceding catheterisations for urinary retention likely precipitated PM. All four prostatic PM cases presented with elevated PSA; imaging and clinical findings could not distinguish PM from PCa, and definitive diagnosis required histopathology. PSA normalised in every case after targeted therapy. Persistently elevated or rebound PSA after treatment should prompt exclusion of concomitant PCa.
Differential Diagnoses of Malakoplakia
1) Urothelial carcinoma: Painless gross haematuria; cystoscopy shows frond-like or nodular masses. Cytologically atypical, disordered urothelial cells invade stroma; positive for GATA-3/uroplakin III. Malakoplakia lacks epithelial atypia and consists of sheets of histiocytes. 2) Xanthogranulomatous cystitis: Polypoid masses; lipid-laden foamy histiocytes, lymphocytes, plasma cells, occasional multinucleated giant cells and follicles; no M–G bodies. 3) Tuberculosis: Caseating granulomas with Langerhans giant cells; no eosinophilic histiocytic granules or M–G bodies; acid-fast bacilli positive. 4) Rosai–Dorfman disease: Emperipolesis present; S100-positive histiocytes; negative CD1a/Langerin; no M–G bodies. 5) Langerhans cell histiocytosis: Children; lytic bone lesions, rarely bladder. Reniform nuclei; CD1a⁺/Langerin⁺ histiocytes; no M–G bodies. 6) Granular-cell tumour: Polygonal cells with abundant eosinophilic granules, small nuclei, perivascular lymphocytes; CD68+/PAS+, S100+/CD56+/NSE+; no M–G bodies. 7) Malakoplakia with concurrent malignancy: Both lesions coexist; abundant histiocytes must not obscure co-existing epithelial or mesenchymal malignancy (illustrated in case 3).
Malakoplakia carries a favourable prognosis but a high relapse rate. No multicentre randomised trials exist; management is therefore tailored to site, severity and symptoms. Antibiotics that accumulate intracellularly within macrophages—eg β-lactams (cephalosporins) or trimethoprim–sulfamethoxazole—are first-line and achieve high cure rates.18 For multidrug-resistant isolates, abscess formation or sepsis, MetaPath profiling or blood-culture data guide pathogen-specific and resistance-guided therapy.19 Among our patients, case 5 harboured aminoglycoside-resistance genes (amikacin, gentamicin, tobramycin, streptomycin); the remaining four lacked definitive resistance determinants. Case 3 received amikacin; the others ceftazidime or cefoperazone–sulbactam, with rapid clinical response. When mass effect persists or antibiotics fail, combined surgical excision and antimicrobial therapy improves outcome.20 Cases 1, 3, 4 and 5 underwent complete resection followed by targeted antibiotics and remain recurrence-free with durable symptom relief.
Conclusion
Malakoplakia is frequently misdiagnosed as neoplasia. Histomorphology, special stains and immunohistochemistry provide the diagnostic cornerstone, while MetaPath rapidly identifies FFPE-resident pathogens and tailors antibiotic therapy, representing a valuable adjunct to conventional assays.
Data Sharing Statement
All data generated or analysed during this study are included in this published article. Raw sequencing reads are available from the corresponding author on reasonable request and under institutional data-transfer agreement.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Chengdu Second People’s Hospital (Approval No. 2020105).
Consent to Participate
Written informed consent to participate in this study was obtained from all individual participants.
Consent to Publish
Patients signed informed consent regarding publishing their data and images.
Acknowledgments
The authors sincerely thank all the patients and their family members for participating in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Chengdu Municipal Health Commission (Grant No. 2020190).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee M, Ko HM, Rubino A, Lee H, Gill R, Lagana SM. Malakoplakia of the gastrointestinal tract: clinicopathologic analysis of 23 cases. Diagn Pathol. 2020;15(1):97. doi:10.1186/s13000-020-01013-y
2. Michaelis L, Gutmann C. Ueber Einschlüsse in Blasentumoren. Z Klin Med. 1902;47:208–7.
3. Jung YS, Chung DY, Kim EJ, Cho NH. Ultrastructural evidence of the evolutional process in malakoplakia. Histol Histopathol. 2020;35(2):177–184. doi:10.14670/HH-18-150
4. Polisini G, Delle Fave RF, Capretti C, et al. Malakoplakia of the urinary bladder: a review of the literature. Arch Ital Urol Androl. 2022;94(3):350–354. doi:10.4081/aiua.2022.3.350
5. Simhadri PK, Contractor R, Chandramohan D, et al. Malakoplakia in kidney transplant recipients: three case reports. World J Nephrol. 2025;14(2):100530. doi:10.5527/wjn.v14.i2.100530
6. Su LD, Chiu CY, Gaston D, et al. Clinical metagenomic next-generation sequencing for diagnosis of central nervous system infections: advances and challenges. Mol Diagn Ther. 2024;28(5):513–523. doi:10.1007/s40291-024-00727-9
7. Sun N, Zhang J, Guo W, et al. Comparative analysis of metagenomic next-generation sequencing for pathogenic identification in clinical body fluid samples. BMC Microbiol. 2025;25(1):165. doi:10.1186/s12866-025-03887-8
8. Shi Y, Wang G, Lau HC, Yu J. Metagenomic sequencing for microbial DNA in human samples: emerging technological advances. Int J Mol Sci. 2022;23(4):2181. doi:10.3390/ijms23042181
9. Li M, Chen J, Zhang L, et al. Clinicopathological characteristics and diagnostic performance of metagenomic pathogen detection technology in mycobacterial infections among HIV patients. Front Cell Infect Microbiol. 2025;15:1584189. doi:10.3389/fcimb.2025.1584189
10. Metsky HC, Siddle KJ, Gladden-Young A, et al. Capturing sequence diversity in metagenomes with comprehensive and scalable probe design. Nat Biotechnol. 2019;37(2):160–168. doi:10.1038/s41587-018-0006-x
11. Yang Y, Walls SD, Gross SM, Schroth GP, Jarman RG, Hang J. Targeted sequencing of respiratory viruses in clinical specimens for pathogen identification and genome-wide analysis. Methods Mol Biol. 2018;1838:125–140. doi:10.1007/978-1-4939-8682-8_10
12. He Q, Wang Y, Chen X, et al. malacoplakia of the bladder combined with infected renal calculi: a case report. Front Surg. 2023;10:1044963. doi:10.3389/fsurg.2023.1044963
13. Subbaraya S, Sawant A, Pawar P, Patil S. Malakoplakia prostate presenting as urinary retention: a report of two cases and review of the literature. BMJ Case Rep. 2021;14(7):e243927. doi:10.1136/bcr-2021-243927
14. Yan Z, Deng W, Wang Y, et al. Case report: malacoplakia due to E. coli with Cryptococcus albidus infection of a transplanted kidney in a patient with recurrent urinary tract infection. Front Med. 2021;8:721145. doi:10.3389/fmed.2021.721145
15. Rances OT, So JS. A rare case of prostatic malakoplakia associated with prostate adenocarcinoma: a case report and review of literature. Acta Med Indones. 2023;55(3):339–342.
16. Medlicott S, Magi-Galluzzi C, Jimenez RE, Trpkov K. Malakoplakia associated with prostatic adenocarcinoma: report of 4 cases and literature review. Ann Diagn Pathol. 2016;22:33–37. doi:10.1016/j.anndiagpath.2016.03.004
17. Acosta AM, Sangoi AR, Maclean F, et al. Prostatic malakoplakia: clinicopathological assessment of a multi-institutional series of 49 patients. Histopathology. 2022;81(4):520–528. doi:10.1111/his.14729
18. Ye H, Yu L, Chen Y. Ureteral calculus complicated by bladder malakoplakia: a case report. Medicine. 2025;104(25):e42926. doi:10.1097/MD.0000000000042926
19. Yang Q, Chen X, Kou G, Ji X. A rare case of prostatic malakoplakia with multidrug-resistant Escherichia coli: a case report. BMC Infect Dis. 2024;24(1):1226. doi:10.1186/s12879-024-10144-2
20. Wang HK, Hang G, Wang YY, Wen Q, Chen B. Bladder malacoplakia: a case report. World J Clin Cases. 2022;10(23):8291–8297. doi:10.12998/wjcc.v10.i23.8291
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.