Back to Journals » Infection and Drug Resistance » Volume 19
Clinically Suspected Whipple Disease Presenting with Acute Kidney Injury as the Initial Manifestation and Complicated by Severe Pneumonia Requiring Veno-Venous Extracorporeal Membrane Oxygenation
Authors Duan LJ, Feng B, Xia JD, Zhao JY, Zhang K
Received 22 March 2026
Accepted for publication 29 May 2026
Published 12 June 2026 Volume 2026:19 611236
DOI https://doi.org/10.2147/IDR.S611236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Li-Juan Duan,* Bing Feng,* Jia-Ding Xia, Jing-Yuan Zhao, Kun Zhang
Department of Intensive Care Unit, Affiliated Hospital of Chengde Medical University, Chengde, Hebei, 067000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kun Zhang, Department of Intensive Care Unit, Affiliated Hospital of Chengde Medical University, Chengde, Hebei, 067000, People’s Republic of China, Tel +86 18631405018, Email [email protected]
Background: Whipple disease (WD) is a chronic, multisystem infectious disorder caused by the Gram-positive bacterium Tropheryma whipplei (T. whipplei). Classical presentations most commonly include intermittent arthralgia or arthritis, often accompanied by chronic gastrointestinal symptoms such as abdominal pain and diarrhea. Owing to its broad clinical spectrum and the absence of pathognomonic features, early diagnosis remains challenging.
Case Report: This report describes a patient with T. whipplei infection who presented with acute kidney injury as the initial and predominant manifestation, an uncommon presentation of WD. The clinical course rapidly progressed to severe pneumonia and severe acute respiratory distress syndrome, necessitating veno-venous extracorporeal membrane oxygenation (ECMO) support. Following intensive management, renal function showed gradual improvement, evidenced by increased urine output and a reduction in serum creatinine levels, while chest imaging demonstrated mild radiological improvement. Despite these findings, the patient subsequently died after the family declined further treatment.
Conclusion: This case offers clinically relevant insights into an atypical presentation of clinically suspected WD. Acute kidney injury (AKI), manifested initially by reduced urine output and elevated serum creatinine, constituted the primary presentation. Moreover, there is a paucity of literature from China describing the use of ECMO in the management of WD-associated severe pneumonia. Accordingly, this case may provide a novel perspective on the management of critically ill patients with severe systemic complications of clinically suspected WD.
Keywords: acute kidney injury, ECMO, respiratory distress syndrome, severe pneumonia, Whipple disease
Background
Whipple disease (WD) is a rare, chronic, and recurrent systemic disorder caused by the Gram-positive bacterium Tropheryma whipplei (T. whipplei), with involvement of multiple organ systems.1 Within the past five years, no cases have been documented of T whipplei infection complicated by AKI and severe pneumonia necessitating ECMO support, nor have there been reports of WD presenting with AKI as the initial clinical symptom.
The pathogenesis of WD involves the invasion of intestinal macrophages by T. whipplei, which disrupts lysosomal degradation, triggers persistent systemic inflammation, and leads to granulomatous tissue infiltration across organs.2 Impaired cellular immunity, particularly reduced macrophage and T‑cell function, predisposes individuals to chronic infection and systemic dissemination.3 Owing to its heterogeneous and nonspecific clinical manifestations, WD is frequently misdiagnosed. The classic clinical triad consists of arthritis, gastrointestinal manifestations, and weight loss.4 Beyond the classic triad, WD exhibits diverse systemic manifestations: respiratory involvement (interstitial pneumonia, pleuritis) occurs in 10–30% of cases; renal manifestations, though rare, include glomerulonephritis and acute kidney injury secondary to immune‑mediated injury or sepsis; additional features include neurological deficits, ocular inflammation, and cardiac involvement, reflecting the multisystem tropism of T. whipplei.5,6 Notably, Corynebacterium striatum is a common nosocomial opportunistic pathogen frequently isolated from respiratory specimens in critically ill patients, and its detection by mNGS may represent either true co-infection or colonization/contamination in the setting of severe pneumonia. Distinguishing pathogenic T. whipplei from commensal/opportunistic Corynebacterium species is critical for accurate diagnosis and targeted antimicrobial therapy.
The present case report describes clinically suspected T. whipplei infection presenting with acute kidney injury (AKI, initially with reduced urine output) as the initial clinical symptom, followed rapidly by severe pneumonia and acute respiratory distress syndrome (ARDS), ultimately requiring extracorporeal membrane oxygenation (ECMO) support.
Case Report
Clinical Data
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from the patient’s next of kin, as the patient was deceased at the time of consent.
A 57-year-old male (height: 173 cm; weight: 78 kg; body mass index: 26.1 kg/m2) was admitted to the hospital on May 11, 2025, with a 5-day history of reduced urine output accompanied by fever and a 4-day history of dyspnea. The medical history was notable for hypertension and long-term alcohol consumption. There was no reported history of joint swelling or pain, abdominal pain, diarrhea, or other relevant comorbid conditions. At presentation, the predominant clinical manifestations included decreased urine output, fever, and progressively worsening dyspnea.
The patient initially presented to a local county hospital at 09:00 on May 10, 2025. Chest computed tomography (CT) demonstrated mild bilateral ground-glass opacities within the pulmonary interstitium, consistent with early interstitial lung involvement. Laboratory evaluation revealed a significantly elevated serum creatinine concentration of 589.62 μmol/L, indicating severe renal dysfunction.
Initial arterial blood gas analysis at the local hospital showed severe hypoxemia and metabolic disturbance; key values are summarized in Table 1.
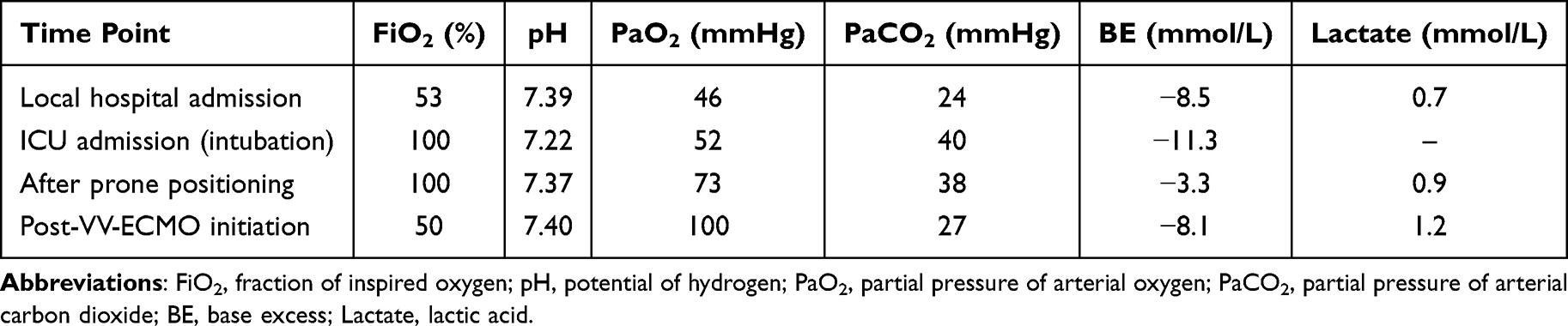 |
Table 1 Key Arterial Blood Gas Values During Hospitalization |
The patient was subsequently transferred to our hospital and formally admitted on May 11, 2025.
Physical examination revealed the following findings.
Vital Signs
Body temperature was 36.9°C, pulse rate was 92 beats per minute, respiratory rate was 35 breaths per minute, and blood pressure was 140/87 mmHg. Peripheral oxygen saturation was 88% while receiving supplemental oxygen via a face mask at a flow rate of 10 L/min.
Neurological Examination
The patient was alert and conscious. Bilateral pupils measured 3.0 mm in diameter and demonstrated intact pupillary light reflexes.
Respiratory System
Auscultation revealed coarse breath sounds in both lungs, with the presence of bilateral dry and moist rales.
Cardiovascular System
Heart rate was 92 beats per minute, and cardiac rhythm was regular.
Abdominal Examination
Central obesity was noted. The abdomen was soft, with no palpable liver or spleen. Bowel sounds were diminished.
Extremities
No edema was observed in the lower limbs. Pathological reflexes were absent bilaterally. Peripheral perfusion was preserved, with warm extremities.
On admission, the patient exhibited progressively worsening clinical symptoms. Arterial blood gas analysis demonstrated severe impairment of oxygenation, findings that were markedly disproportionate to the chest CT obtained at the local hospital, suggesting substantial progression of pulmonary involvement. To further assess the extent of lung injury, a follow-up chest CT was performed, which revealed a pronounced aggravation of diffuse ground-glass opacities involving both lungs.
Concurrent laboratory evaluation showed significant renal dysfunction, with a serum creatinine level of 690.74 μmol/L, markedly exceeding the established reference range of 44–106 μmol/L.
After admission, invasive mechanical ventilation was initiated, during which a small quantity of white mucoid sputum was aspirated. Following endotracheal intubation, arterial blood gas analysis was performed under conditions of an FiO2 of 100% and positive end-expiratory pressure (PEEP) set at 10 cmH2O. The results demonstrated a pH of 7.22, PaO2 of 52.00 mmHg, PaCO2 of 40 mmHg, HCO3− of 16.40 mmol/L, and a BE of −11.3 mmol/L, consistent with severe respiratory and metabolic derangements.
The Acute Physiology and Chronic Health Evaluation-II (APACHE-II) score was 27, corresponding to critical illness severity and an estimated mortality risk of 60.47%. Gastrointestinal endoscopy was not performed because the patient was critically ill with severe hypoxemia and hemodynamic instability, and the family declined additional invasive procedures. Although gastrointestinal involvement is classic for Whipple disease, clinical evaluation of the gut was deferred due to the patient’s unstable condition.
On admission, the patient’s respiratory distress was initially attributed to pulmonary infection. The etiology of the reduced urine output and elevated serum creatinine level was evaluated systematically. First, the patient did not report thirst, and both heart rate and blood pressure were largely within normal ranges. Peripheral perfusion was preserved, with warm extremities and a normal lactate level; there were no clinical features suggestive of shock, making prerenal AKI unlikely. Second, there were no significant abnormalities reported on prior intermittent health check-ups, and abdominal CT performed at the local hospital revealed no obstructive or structural abnormalities, thereby excluding postrenal AKI. On this basis, intrinsic acute kidney injury was suspected, with a broad differential etiology at admission, including severe systemic infection of unknown origin.
Diagnoses
1. Severe community-acquired pneumonia (CAP) complicated by type I respiratory failure; 2. AKI (suspected secondary to severe systemic infection, pathogen undefined at admission); 3. Acute respiratory distress syndrome (ARDS).
Treatment and Clinical Progress
Anti-Infection and Symptomatic Support Therapy
Empiric anti-infective treatment was initiated and consisted of the following agents:
① Ceftriaxone, 2.0 g, administered intravenously once daily.
② Moxifloxacin, 0.4 g, administered intravenously once daily.
③ Oseltamivir, 75 mg, administered via a nasogastric tube twice daily.
Bronchoscopy and Microbiological Evaluation
Flexible bronchoscopy was performed to obtain lower respiratory tract specimens. A small amount of white, jelly-like sputum was observed in the left lower lobe during the procedure. Bronchoalveolar lavage fluid was collected and subsequently analyzed using metagenomic next-generation sequencing (mNGS) to enhance the accuracy of pathogen identification in the context of suspected respiratory infections.
Respiratory Management
Deep sedation and adequate analgesia were maintained, and the patient remained on continuous invasive mechanical ventilation. High-level ventilatory support was required using synchronized intermittent mandatory ventilation combined with pressure support ventilation. Initial settings included a tidal volume [VT] of 400 mL per breath, PEEP of 14 mbar, pressure support [PS] of 10 mbar, respiratory rate of 16 breaths per minute, and an FiO2 of 100%.
Given an oxygenation index below 100 mmHg, prone positioning was initiated and implemented for more than 6 hours. As no significant improvement was observed after prone positioning, with the oxygenation index remaining below 80 mmHg, bedside ultrasonography was performed and showed essentially preserved cardiac systolic function. Criteria for veno-venous extracorporeal membrane oxygenation (VV-ECMO) were therefore met. After informed consent was obtained from the patient’s family, VV-ECMO was initiated to provide advanced respiratory support. Initial ECMO parameters included a rotation speed of 2930 rpm, blood flow of 3.5 L/min, sweep gas flow of 3.5 L/minute, and FiO2 of 100%. Systemic anticoagulation was maintained with continuous heparin sodium infusion, with activated clotting time monitored and maintained between 180 and 220 seconds.
Arterial blood gas parameters improved progressively after prone positioning and VV‑ECMO support; serial values are provided in Table 1. Ventilator parameters were subsequently adjusted to an FiO2 of 50%, PEEP of 12 cmH2O, PS of 10 cmH2O, and tidal volume of 420 mL per breath, resulting in an oxygenation index of 200 mmHg, representing a marked improvement compared with prior values. Intermittent positional ventilation and intensified airway management were continued.
Circulatory Management
Following the initiation of mechanical ventilation, the patient experienced a decrease in blood pressure exceeding 40 mmHg from baseline. Norepinephrine infusion was initiated to support hemodynamic stability, with the dose titrated to a maximum of 0.4 μg/kg/min. With ongoing therapeutic intervention, the vasopressor requirement was gradually reduced to 0.14 μg/kg/minute, and circulatory status subsequently stabilized.
Renal Function Monitoring
Urine output normalized within 48 hours, while serum creatinine peaked on admission and gradually decreased thereafter. Serial renal parameters are shown in Table 2.
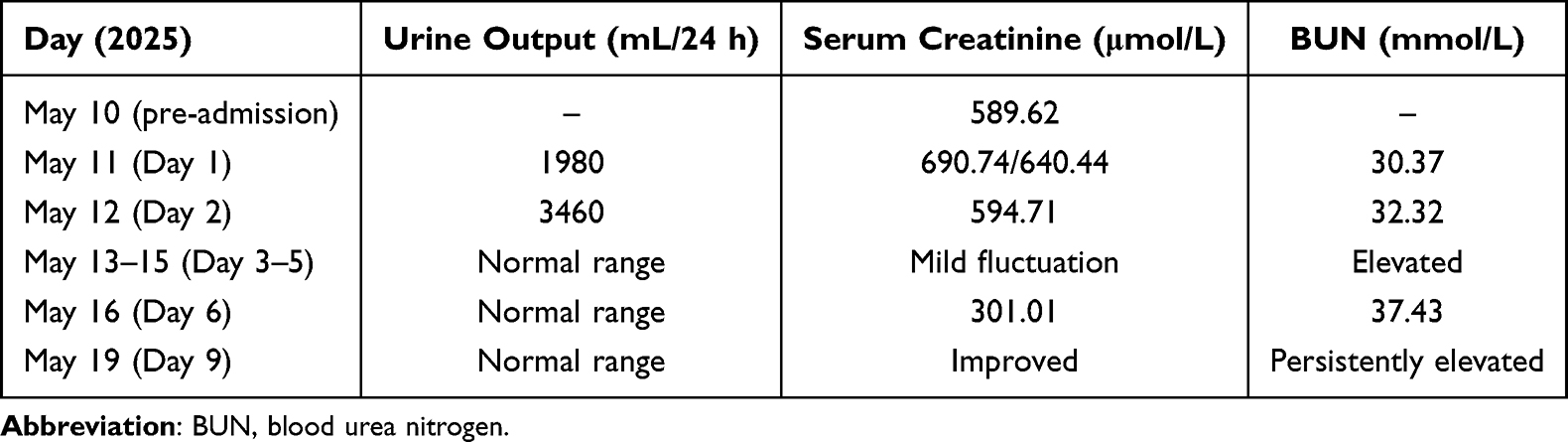 |
Table 2 Temporal Changes in Renal Function and Urine Output |
Day 2 After Admission
Inflammatory markers (WBC, neutrophils, PCT, CRP) showed an initial rise followed by a gradual decline; trends are summarized in Table 3. Accordingly, oseltamivir therapy was discontinued.
 |
Table 3 Trends in Inflammatory Biomarkers |
Day 3 After Admission
Hemodynamic parameters remained stable, allowing for the discontinuation of vasopressor support. Comprehensive immunological testing was unremarkable, including the antinuclear antibody profile, systemic vasculitis-related antibodies, antiphospholipid antibody profile, and the four tests related to rheumatoid arthritis. Serum immunoglobulin levels were within normal limits. Both the G test and GM test were negative, and nucleic acid testing for COVID-19 was negative. Urine output remained within the normal range, while serum creatinine showed a slight increase. Urine culture was further collected. The patient had normal routine urine test results and presented no urinary tract infection symptoms such as frequent micturition, urgent micturition or dysuria. Sputum culture demonstrated no growth of pathogenic bacteria.
Metagenomic next-generation sequencing (Sequencing Platform: Shanghai Baotong Medical LaboratoryMicrobial Profile) of bronchoalveolar lavage fluid results were as follows: DNA Test Result Details: Tropheryma whipplei 27,398 sequence reads, Corynebacterium striatum 314 sequence reads, Abiotrophia defectiva 6 sequence reads, Olsenella uli 5 sequence reads, Mycoplasma orale 3 sequence reads. RNA Test Result Details: Tropheryma whipplei 92 sequence reads, Corynebacterium striatum 4 sequence reads.
While Corynebacterium striatum was also detected, it is a common hospital-acquired colonizer in critically ill patients, and T. whipplei was considered the primary pathogen responsible for the severe pneumonia in this case. Doxycycline (0.1 g intravenously every 12 hours) was added as adjunctive anti-infection therapy, in accordance with standard treatment recommendations, while ceftriaxone (2.0 g intravenously once daily) was continued for its broad-spectrum antibacterial efficacy. Following identification of T. whipplei, the AKI etiology was reclassified as infection‑associated intrinsic AKI secondary to systemic T. whipplei infection. Further optimization of volume status was undertaken, while continuous ECMO support and intermittent prone positioning were maintained. ECMO, which has been effectively utilized in critical care settings, particularly in cases of ARDS refractory to conventional mechanical ventilation, was continued as part of the respiratory support strategy. Follow-up chest radiography indicated slight absorption and partial improvement of pulmonary lesions compared to prior imaging.
Day 6 After Admission
Renal function improved while blood urea nitrogen remained elevated, likely due to catabolic stress, high protein breakdown, and impaired renal tubular reabsorption during critical illness. The patient developed hypertension, necessitating continuous intravenous infusion of sodium nitroprusside for blood pressure control. The intensity of ECMO support was subsequently reduced.
Day 9 After Admission
Chest CT demonstrated areas of consolidation in the posterior segments of both lungs accompanied by mild improvement of localized exudative lesions in the bilateral upper lobes. Following a reduction in ECMO support intensity, adequate pulmonary oxygenation could not be maintained despite ongoing mechanical ventilation. After discussion, the patient’s family declined further therapeutic interventions. ECMO support was withdrawn per family request. Despite maximal conventional ventilation, the patient could not maintain adequate oxygenation and hemodynamic stability. The patient was discharged home and died approximately 2 hours later due to refractory hypoxemia and progressive respiratory failure.
The imaging changes observed during treatment are presented in Figure 1.
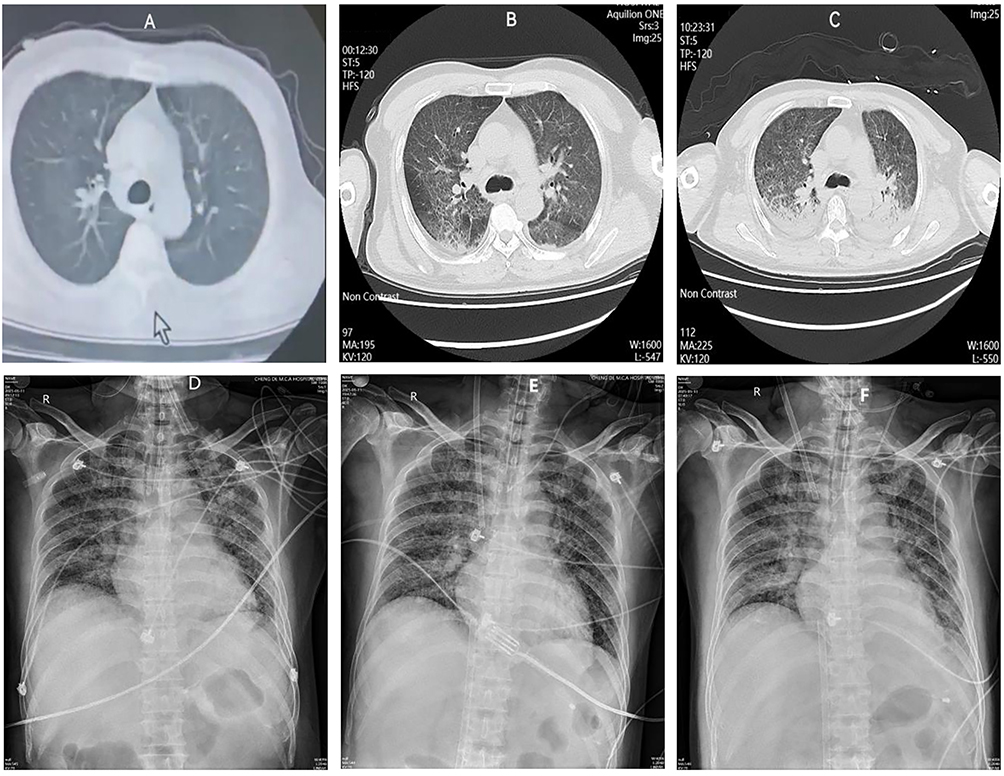 |
Figure 1 Serial changes in pulmonary imaging findings. Notes: (A–C) depict the CT manifestations of intrapulmonary lesions at different stages of treatment, whereas (D–F) illustrate chest radiographic changes over the same period. (A) Chest CT at the referring hospital (May 10, 2025); (B) Chest CT on admission (May 11, 2025); (C) Chest CT prior to discharge (May 19, 2025); (D) Chest radiograph following initiation of mechanical ventilation (May 11, 2025); (E) Chest radiograph after ECMO cannulation (May 11, 2025); (F) Chest radiograph after treatment (May 13, 2025). |
The diagnosis of AKI was established, and temporal changes in urine output and serum creatinine are illustrated in Figure 2. Pulmonary infection was documented, and infection-related indicator trends are shown in Figure 3.
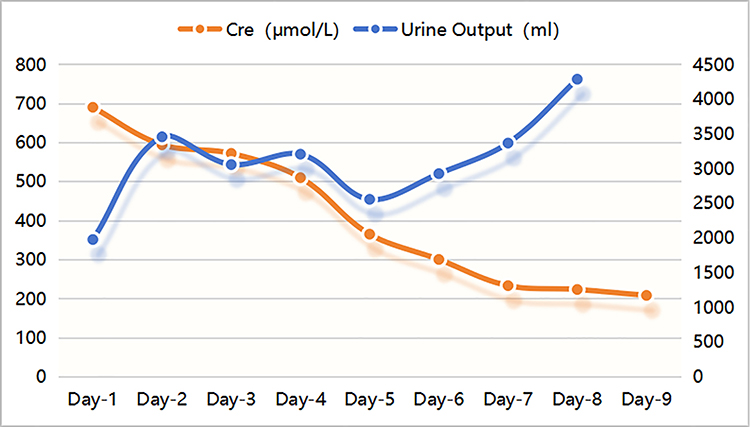 |
Figure 2 Temporal changes in serum creatinine levels and urine output and their clinical implications. |
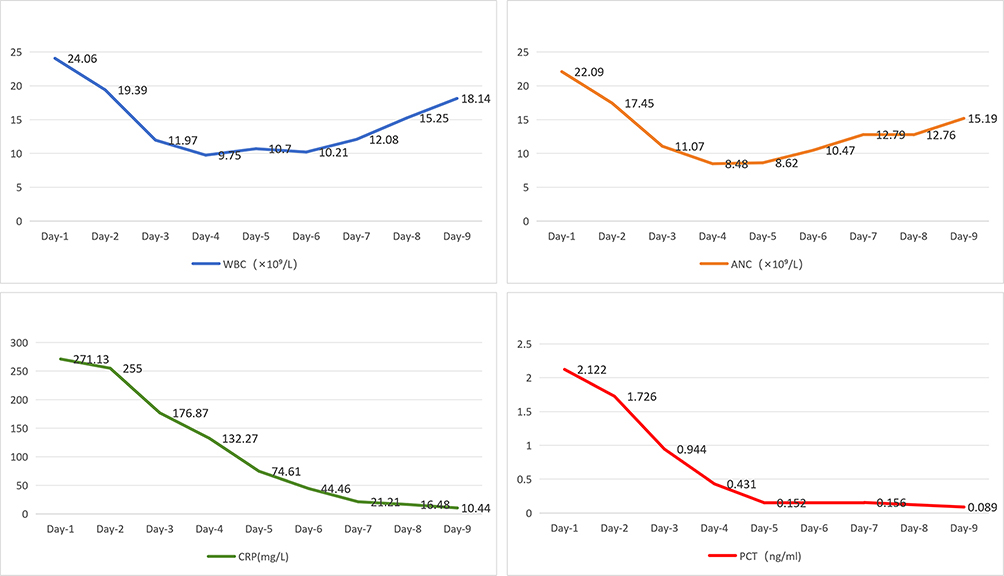 |
Figure 3 Trends in infection-related biomarkers during hospitalization. |
Discussion
The clinical presentation of WD is heterogeneous and lacks pathognomonic features. Classical WD most often manifests with intermittent arthralgia, arthritis, or other joint-related symptoms, frequently accompanied by chronic gastrointestinal symptoms such as abdominal pain and diarrhea.7–9 The condition predominantly affects middle-aged males. In approximately 80% to 90% of cases with classical WD, seronegative arthritis and arthralgia remain the main clinical manifestations.6,10–16
Given the widespread environmental distribution of T. whipplei, exposure and infection are relatively common. Primary infection may present as an acute illness, with clinical manifestations including bacteremia, gastroenteritis, or pneumonia.5,11–13
Several studies have reported detection of T. whipplei in the feces of children presenting with diarrhea in the absence of other identifiable enteric pathogens.17 Carriage of T. whipplei has also been documented in the feces and saliva of healthy individuals.18,19 In rural regions of Senegal and Ghana in Africa, asymptomatic carriage rates are relatively high, and the prevalence of T. whipplei detected in the feces of children with diarrhea is approximately twice that observed in asymptomatic children.20–22 Traditional microbiological methods are limited, making mNGS a valuable adjunct for identifying unusual pathogens in critical illness.
Clinically, WD can involve multiple organ systems, and some patients present with nonspecific symptoms.23,24 This report describes a middle-aged male with acute pulmonary infection in whom AKI was the predominant initial presentation, followed by rapidly progressive severe pneumonia and ARDS. Microbiological investigations, including sputum culture, serological tests for respiratory pathogens, multiplex nucleic acid testing for respiratory pathogens, and blood cultures, were all negative. Owing to the patient’s critical condition, gastrointestinal endoscopy was not performed. Furthermore, comprehensive evaluation for immune-related disorders yielded negative results.15,25–27
Metagenomic next-generation sequencing of bronchoalveolar lavage fluid detected T. whipplei. In conjunction with radiological improvement of pulmonary lesions and a progressive decline in infection-related biomarkers following anti-infective therapy, was highly suspected to be severe T. whipplei–associated pneumonia. In this case, bronchoscopy and bronchoalveolar lavage were performed, but histopathological examination of tissue invasion was not conducted due to the patient’s critical condition and family refusal of invasive procedures. Therefore, T. whipplei infection was clinically suspected rather than definitively confirmed. We acknowledge that mNGS detection alone does not establish pathogenicity, as high T. whipplei read counts have been reported in respiratory samples without clinical correlation. However, the diagnosis was supported by the following: (1) absence of other pathogens on routine microbiological tests; (2) consistent clinical course of severe pneumonia and ARDS; (3) improvement in clinical and radiological parameters after targeted anti-T. whipplei therapy; and (4) exclusion of alternative causes including immune-mediated diseases. The patient required VV-ECMO for respiratory support. With intensive treatment, renal function showed gradual recovery, as evidenced by increased urine output and declining serum creatinine levels, and pulmonary radiological findings showed mild improvement. Despite these changes, the patient died after the family declined further medical intervention.
Notably, the interpretation of T. whipplei detected by mNGS requires caution, as asymptomatic pharyngeal and gastrointestinal colonization is well documented in healthy individuals, with carriage rates up to 20–40% in some populations.3,28 High sequencing reads alone do not equate to pathogenicity, and respiratory tract colonization without disease has been repeatedly reported.23,29 Therefore, the possibility of incidental detection cannot be excluded in this critically ill patient. Similarly, the clinical significance of Corynebacterium striatum remains unclear. While this species is often regarded as a nosocomial colonizer, it has been increasingly recognized as an opportunistic pathogen in ventilated and immunocompromised patients, occasionally causing true pneumonia and bacteremia. In the present case, we cannot fully rule out a dual infection or a contributing pathogenic role of C. striatum, although the clinical and radiological response to doxycycline favors T. whipplei as the dominant pathogen.
This study has several important limitations. First, no histopathological evidence of tissue invasion was obtained, and the diagnosis of Whipple disease remains clinically suspected rather than definitive. Second, mNGS cannot distinguish colonization from true infection, and high T. whipplei reads may represent asymptomatic carriage in critically ill hosts. Third, the pathogenic contribution of Corynebacterium striatum could not be definitively excluded. Fourth, targeted therapy was initiated empirically, and long-term follow-up was unavailable due to family withdrawal of care. These limitations should be considered when interpreting the findings.
Conclusion
This case highlights that Whipple disease should be considered in the differential diagnosis of unexplained acute kidney injury accompanied by severe pneumonia, even in the absence of classic gastrointestinal or articular symptoms. Metagenomic next‑generation sequencing facilitates early pathogen identification in critically ill patients with unclear etiology, while multidisciplinary collaboration between nephrology, pulmonology, and critical care teams is essential for optimizing management. Given the limitations of relying solely on mNGS and the risk of asymptomatic T. whipplei colonization, future research should focus on refining diagnostic pathways that distinguish true infection from colonization and improve early recognition of atypical presentations.
Abbreviations
WD, Whipple disease; T. whipplei, Tropheryma whipplei; ECMO, veno-venous extracorporeal membrane oxygenation; AKI, acute kidney injury; ARDS, acute respiratory distress syndrome; CT, Chest computed tomography; PEEP, positive end-expiratory pressure; APACHE-II, Acute Physiology and Chronic Health Evaluation-II; CAP, Severe community-acquired pneumonia; mNGS, metagenomic next-generation sequencing; VV-ECMO, veno-venous extracorporeal membrane oxygenation.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This retrospective case report was approved by the Institutional Review Board of Affiliated Hospital of Chengde Medical University, which waived the requirement for full ethics review. Written informed consent for publication was obtained from the patient’s next of kin. All patient data were fully anonymized to protect privacy. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Li-Juan Duan and Bing Feng are co-first authors for this study. We thank our collaborator Kun Zhang, from the Division of Evaluation and Control, for performing the electron microscope analysis.
Funding
2025 Government-Funded Clinical Medicine Outstanding Talent Development Program (Project Number: ZF2025250).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Whipple GH. A hitherto undescribed disease characterized anatomically by deposits of fat and fatty acid in the intestinal and mesenteric lymphatic tissues. Bull Johns Hopkins Hosp. 1907;18:382–10.
2. Dolmans RA, Boel CH, Lacle MM, Kusters JG. Clinical manifestations, treatment, and diagnosis of Tropheryma whipplei infections. Clin Microbiol Rev. 2017;30(2):529–555. doi:10.1128/CMR.00033-16
3. Raoult D, Birg ML, La Scola B, et al. Cultivation of the bacillus of Whipple’s disease. N Engl J Med. 2000;342(9):620–625. doi:10.1056/NEJM200003023420903
4. Fenollar F, Birg ML, Gauduchon V, Raoult D. Culture of Tropheryma whipplei from human samples: a 3-year experience (1999 to 2002). J Clin Microbiol. 2003;41(8):3816–3822. doi:10.1128/JCM.41.8.3816-3822.2003
5. Boumaza A, Ben Azzouz E, Arrindell J, Lepidi H, Mezouar S, Desnues B. Whipple’s disease and Tropheryma whipplei infections: from bench to bedside. Lancet Infect Dis. 2022;22(10):e280–e291. doi:10.1016/S1473-3099(22)00128-1
6. Fenollar F, Puéchal X, Raoult D. Whipple’s disease. N Engl J Med. 2007;356(1):55–66. doi:10.1056/NEJMra062477
7. Bousbia S, Papazian L, Auffray JP, et al. Tropheryma whipplei in patients with pneumonia. Emerg Infect Dis. 2010;16(2):258–263. doi:10.3201/eid1602.090610
8. Raoult D, Fenollar F, Rolain JM, et al. Tropheryma whipplei in children with gastroenteritis. Emerg Infect Dis. 2010;16(5):776–782. doi:10.3201/eid1605.091801
9. Fenollar F, Mediannikov O, Socolovschi C, et al. Tropheryma whipplei bacteremia during fever in rural West Africa. Clin Infect Dis. 2010;51(5):515–521. doi:10.1086/655677
10. Lagier JC, Lepidi H, Raoult D, Fenollar F. Systemic Tropheryma whipplei: clinical presentation of 142 patients with infections diagnosed or confirmed in a reference center. Medicine. 2010;89(5):337–345. doi:10.1097/MD.0b013e3181f204a8
11. Marth T, Moos V, Müller C, Biagi F, Schneider T. Tropheryma whipplei infection and Whipple’s disease. Lancet Infect Dis. 2016;16(3):e13–e22. doi:10.1016/S1473-3099(15)00537-X
12. Fleming JL, Wiesner RH, Shorter RG. Whipple’s disease: clinical, biochemical, and histopathologic features and assessment of treatment in 29 patients. Mayo Clin Proc. 1988;63(6):539–551. doi:10.1016/s0025-6196(12)64884-8
13. Marth T, Raoult D. Whipple’s disease. Lancet. 2003;361(9353):239–246. doi:10.1016/S0140-6736(03)12274-X
14. Puéchal X. Whipple’s disease. Ann Rheum Dis. 2013;72(6):797–803. doi:10.1136/annrheumdis-2012-202684
15. Fenollar F, Lagier JC, Raoult D. Tropheryma whipplei and Whipple’s disease. J Infect. 2014;69(2):103–112. doi:10.1016/j.jinf.2014.05.008
16. Puéchal X. Whipple disease and arthritis. Curr Opin Rheumatol. 2001;13(1):74–79. doi:10.1097/00002281-200101000-00012
17. Fenollar F, Trani M, Davoust B, et al. Prevalence of asymptomatic Tropheryma whipplei carriage among humans and nonhuman primates. J Infect Dis. 2008;197(6):880–887. doi:10.1086/528693
18. Fenollar F, Keita AK, Buffet S, Raoult D. Intrafamilial circulation of Tropheryma whipplei, France. Emerg Infect Dis. 2012;18(6):949–955. doi:10.3201/eid1806.111038
19. Fenollar F, Amphoux B, Raoult D. A paradoxical Tropheryma whipplei Western blot differentiates patients with whipple disease from asymptomatic carriers. Clin Infect Dis. 2009;49(5):717–723. doi:10.1086/604717
20. Lagier JC, Fenollar F, Raoult D. Acute infections caused by Tropheryma whipplei. Future Microbiol. 2017;12:247–254. doi:10.2217/fmb-2017-0178
21. Vinnemeier CD, Klupp EM, Krumkamp R, et al. Tropheryma whipplei in children with diarrhoea in rural Ghana. Clin Microbiol Infect. 2016;22(1):65.e1–65.e3. doi:10.1016/j.cmi.2015.09.022
22. Gautret P, Lagier JC, Benkouiten S, Fenollar F, Raoult D, Brouqui P. Does Tropheryma whipplei contribute to travelers’ diarrhea?: a PCR analysis of paired stool samples in French travelers to Senegal. Travel Med Infect Dis. 2014;12(3):264–267. doi:10.1016/j.tmaid.2014.01.009
23. Niemczyk S, Filipowicz E, Wozniacki L, et al. Renal amyloidosis in Whipple disease: a case report. Cases J. 2009;2:8444. doi:10.4076/1757-1626-2-8444
24. Fenollar F, Raoult D. Whipple’s disease. Clin Diagn Lab Immunol. 2001;8(1):1–8. doi:10.1128/CDLI.8.1.1-8.2001
25. Raoult D, Ogata H, Audic S, et al. Tropheryma whipplei Twist: a human pathogenic Actinobacteria with a reduced genome. Genome Res. 2003;13(8):1800–1809. doi:10.1101/gr.1474603
26. Schoedon G, Goldenberger D, Forrer R, et al. Deactivation of macrophages with interleukin-4 is the key to the isolation of Tropheryma whippelii. J Infect Dis. 1997;176(3):672–677. doi:10.1086/514089
27. Schneider T, Moos V, Loddenkemper C, Marth T, Fenollar F, Raoult D. Whipple’s disease: new aspects of pathogenesis and treatment. Lancet Infect Dis. 2008;8(3):179–190. doi:10.1016/S1473-3099(08)70042-2
28. Keita AK, Raoult D, Fenollar F. Tropheryma whipplei as a commensal bacterium. Future Microbiol. 2013;8(1):57–71. doi:10.2217/fmb.12.124
29. Ramzan NN, Loftus E, Burgart LJ, et al. Diagnosis and monitoring of Whipple disease by polymerase chain reaction. Ann Intern Med. 1997;126(7):520–527. doi:10.7326/0003-4819-126-7-199704010-00004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.