Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Clinically Important Deterioration Among Patients with Chronic Obstructive Pulmonary Disease (COPD) Treated with Nebulized Glycopyrrolate: A Post Hoc Analysis of Pooled Data from Two Randomized, Double-Blind, Placebo-Controlled Studies
Authors Kerwin EM ![]() , Murray L, Niu X, Dembek C
, Murray L, Niu X, Dembek C
Received 17 June 2020
Accepted for publication 11 August 2020
Published 29 September 2020 Volume 2020:15 Pages 2309—2318
DOI https://doi.org/10.2147/COPD.S267249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Edward M Kerwin,1 Lindsey Murray,2 Xiaoli Niu,3 Carole Dembek3
1Clinical Research Institute of Southern Oregon, Medford, OR, USA; 2Evidera, Bethesda, MD, USA; 3Sunovion Pharmaceuticals Inc., Marlborough, MA, USA
Correspondence: Xiaoli Niu
Sunovion Pharmaceuticals Inc., 84 Waterford Dr, Marlborough, MA 01752, USA
Tel +1 508 357 7863
Email [email protected]
Purpose: Using a composite endpoint, pooled data from two 12-week Phase III placebo-controlled trials (GOLDEN 3, NCT02347761; GOLDEN 4, NCT02347774) were analyzed to determine whether glycopyrrolate inhalation solution (25 mcg and 50 mcg) administered twice daily (BID) via the eFlow® Closed System nebulizer (GLY) reduced the risk of clinically important deterioration (CID) in patients with moderate-to-very-severe COPD.
Methods: CID was defined as ≥ 100-mL decrease from baseline in post-bronchodilator trough forced expiratory volume in one second (FEV1), or ≥ 4-unit increase in baseline St. George’s Respiratory Questionnaire (SGRQ) total score, or moderate/severe exacerbation. The relative treatment effect of GLY versus placebo on the odds of CID (any and by component endpoints) was expressed as the odds ratio (OR) and 95% confidence interval (CI). Subgroups categorized by age (< 65/≥ 65 years), sex, smoking status (current/former), long-acting beta agonist (LABA) use, FEV1 (< 50%/≥ 50%), and peak inspiratory flow rate (PIFR) (< 60 L/min/≥ 60 L/min) were analyzed.
Results: Compared to placebo, GLY 25 mcg and 50 mcg BID over 12 weeks significantly reduced the risk of CID by 50% (OR: 0.50 [0.37– 0.68]) and 40% (OR: 0.60 [0.44– 0.80]), respectively. Subjects treated with GLY 25 mcg BID were 59% less likely to experience CID in FEV1 (OR: 0.41 [0.27– 0.62]) and 48% less likely to perceive CID in health status (OR: 0.52 [0.37– 0.73]). Statistically significant reductions were also observed at the higher dose. The incidence of moderate/severe exacerbations was low and comparable among the cohorts. GLY 25 mcg BID was significantly more effective than placebo (p< 0.05) in preventing CID irrespective of age, smoking status, LABA use, COPD severity, or PIFR. Subjects < 65 years (OR 0.45 [0.29– 0.68]) and those with PIFR < 60 L/min (OR 0.36 [0.20– 0.67]) exhibited the largest benefit.
Conclusion: Nebulized GLY over 12 weeks significantly reduced the risk of CID and provided greater short-term stability in patients with moderate-to-very-severe COPD.
Keywords: nebulized glycopyrrolate, clinically important deterioration, composite measure
Introduction
Chronic obstructive pulmonary disease (COPD) is a common condition characterized by frequently progressive airflow limitation, persistent respiratory symptoms, and high morbidity and mortality.1 Without effective management, the burden of pervasive symptoms, particularly dyspnea, can increase the risk of exacerbations, impair quality of life, and contribute to substantial health care costs.2,3 Recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD), inhaled long-acting beta-agonists (LABA) and long-acting muscarinic antagonists (LAMA) are central to the treatment strategy for alleviating symptoms, minimizing the frequency and severity of exacerbations, and improving health status and exercise tolerance.1 Lonhala® Magnair® (glycopyrrolate, GLY) inhalation solution (Sunovion Pharmaceuticals Inc., Marlborough, MA, USA) is a LAMA approved in the US for the long-term maintenance treatment of airflow obstruction in patients with COPD.4 The licensed recommended dose is 25 mcg administered twice daily (BID) using the eFlow® Closed System (Magnair®, PARI Pharma GmbH, Starnberg, Germany), a hand-held vibrating membrane nebulizer. The nebulizer is designed to deliver 1.0 mL of GLY within three minutes via normal breathing rather than a single-breath actuation5,6 Two replicate, 12-week, randomized, placebo-controlled Phase III trials in the US, Glycopyrrolate for Obstructive Lung Disease via Electronic Nebulizer (GOLDEN) 3 and GOLDEN 4 (NCT02347761 and NCT02347774, respectively), evaluated the safety and efficacy of nebulized GLY 25 mcg BID and 50 mcg BID (not licensed for commercial use) in patients with moderate-to-very-severe COPD (Figure 1). In both trials, GLY administered for 12 weeks was well tolerated and yielded statistically significant improvements from baseline over placebo in the forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and the St. George Respiratory Questionnaire (SGRQ) total score.6
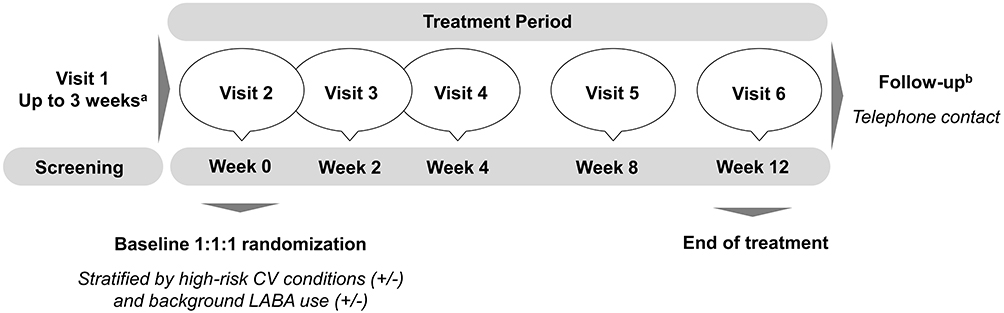 |
Figure 1 GOLDEN 3 and GOLDEN 4 study design. Notes: aFlexible, between 1 and 7 days. bContacted by telephone 5 to 7 days after the last study visit.Abbreviations: CV, cardiovascular; GOLDEN, Glycopyrrolate for Obstructive Lung Disease via Electronic Nebulizer; LABA, long-acting beta agonist. |
Considering the progressive nature of COPD, it is essential to determine whether bronchodilator therapies can improve airway stability and prevent disease worsening. Exacerbations and rapid decline in lung function can signify poor long-term prognosis in COPD.7,8 Further, deterioration in health status over one year, as demonstrated by an increase in SGRQ score exceeding the within-patient clinically meaningful change threshold,9 has been associated with an increased risk of hospitalization and mortality.10 To complement efficacy assessments, a composite endpoint for clinically important deterioration (CID) in COPD has been used to provide a more comprehensive, multidimensional measure of treatment effectiveness. The CID captures changes in lung function, health status, and exacerbations that can reflect temporary fluctuations in disease state or more sustained worsening.11,12 A post hoc analysis of pooled data from the GOLDEN 3 and GOLDEN 4 trials was performed to examine whether nebulized GLY (25 mcg and 50 mcg) BID administered for 12 weeks decreased the risk of CID compared to placebo in patients with moderate-to-very-severe COPD.
Methods
Full methods and patient eligibility criteria for the GOLDEN-3 (NCT02347761) and GOLDEN-4 (NCT02347774) trials have been published elsewhere.6 In brief, the studies included male or female current or past smokers (≥10 pack-year) aged ≥40 years. Eligible patients had a clinical diagnosis of moderate-to-very-severe COPD by the GOLD classification and met the post-bronchodilator spirometry criteria at screening (ie, FEV1 ≤80% of predicted normal, FEV1 >0.7 L, and FEV1/FVC ratio <0.70).1,6 Patients with severe comorbidities or exacerbations requiring hospitalization or increased COPD treatments within six weeks of screening were excluded. Approximately 30% of subjects (limited by protocol) continued background LABA medications with or without inhaled corticosteroids (ICS). The study protocols were approved by the Quorum Review IRB North American (US and Canada) Board (Panel II) prior to patient enrollment, and were conducted in accordance with the protocols, International Council for Harmonization Good Clinical Practice guidelines and the Declaration of Helsinki. All subjects or their legal representatives provided written informed consent.6
The current study analyzed pooled data for efficacy assessments conducted at baseline and at the end of the study (week 12). Applying criteria described by Singh et al,13 subjects were considered to experience CID if any of the following events occurred: 1) a ≥100-mL decrease from baseline in post-bronchodilator trough FEV1; 2) a ≥4-unit increase in the baseline SGRQ total score; or 3) a moderate or severe healthcare resource utilization (HCRU)-related exacerbation. An exacerbation was considered “moderate” if it required a clinic visit or treatment with antibiotics or oral corticosteroids with or without a clinic visit but no hospitalization, and “severe” if it necessitated an overnight stay in a hospital or emergency room. These component endpoints were based on the established within-patient clinically important change thresholds for FEV1 and the SGRQ and an expert consensus panel definition for exacerbations.9,12,14–16
Statistical Analysis
Statistical analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC). Analyses were conducted on the intent-to-treat population, defined as randomized patients who received at least one dose of the study treatment and had at least one post-dose pulmonary function assessment. Baseline patient demographics and clinical characteristics were summarized descriptively using the mean and standard deviation (SD) for continuous variables and the number of patients and proportion for categorical variables. The proportion of patients in each cohort experiencing CID and achieving the within-patient clinically meaningful change thresholds for each of the individual component endpoints was assessed at week 12.
Separate logistic regression models were analyzed to compare the risk of experiencing CID (ie, any CID and by the individual component measures) between each GLY cohort and the placebo (reference) cohort. Subgroup analyses were performed to examine the risk of experiencing CID in the cohorts stratified by baseline age (<65 or ≥65 years), sex (male or female), smoking status (current or former), background LABA use (yes/no), COPD severity (FEV1 ≥50% or <50%), and peak inspiratory flow rate (PIFR) (<60 or ≥60 L/min). Due to the small number of patients with GOLD 4 classification, aggregate data for the GOLD 3 and GOLD 4 subgroups were analyzed in the subgroup with FEV1 <50%. All models were adjusted for the presence (yes/no) of high cardiovascular risk conditions and background LABA use, baseline post-bronchodilator trough FEV1 (continuous variable), baseline SGRQ total score (continuous variable), and history (yes/no) of moderate or severe HCRU-related exacerbations in the prior 12 months. Results were expressed as the adjusted odds ratio (OR) and 95% confidence interval (CI). An OR >1.0 (excluding “1.0” in the 95% CI) indicated an increased risk of CID in a GLY cohort versus placebo, whereas an OR <1.0 (excluding “1.0“ in the 95% CI) signified a decreased risk of CID. A p-value <0.05 indicated statistical significance.
Results
Baseline Characteristics of the Pooled Study Cohorts
The pooled study population consisted of 1293 subjects randomized to GLY 25 mcg BID (N=431), GLY 50 mcg BID (N=432), or placebo BID (N=430) (Table 1). Baseline demographic and clinical characteristics, including the mean SGRQ total scores, were well matched across the cohorts. Subjects were predominantly male (54.7–57.2%), Caucasian (89.3–90.2%), and current smokers (50.7–55.7%). Nearly two-thirds (63.7–64.7%) had high cardiovascular risk conditions. Patients with moderate airflow obstruction (GOLD 2) comprised the majority (55.3–58.8%). More than one-third (35.6–36.6%) had severe COPD (GOLD 3), and 5.6–8.1% had very severe disease (GOLD 4). During the prior 12 months, 19.5% and 16.9% of patients who were randomized to GLY 25 mcg and 50 mcg BID, respectively, and 21.6% in the placebo cohort had experienced a COPD exacerbation. Utilization of background LABA was slightly higher than that of ICS (30.7–31.3% versus 28.2–29.5%, respectively).
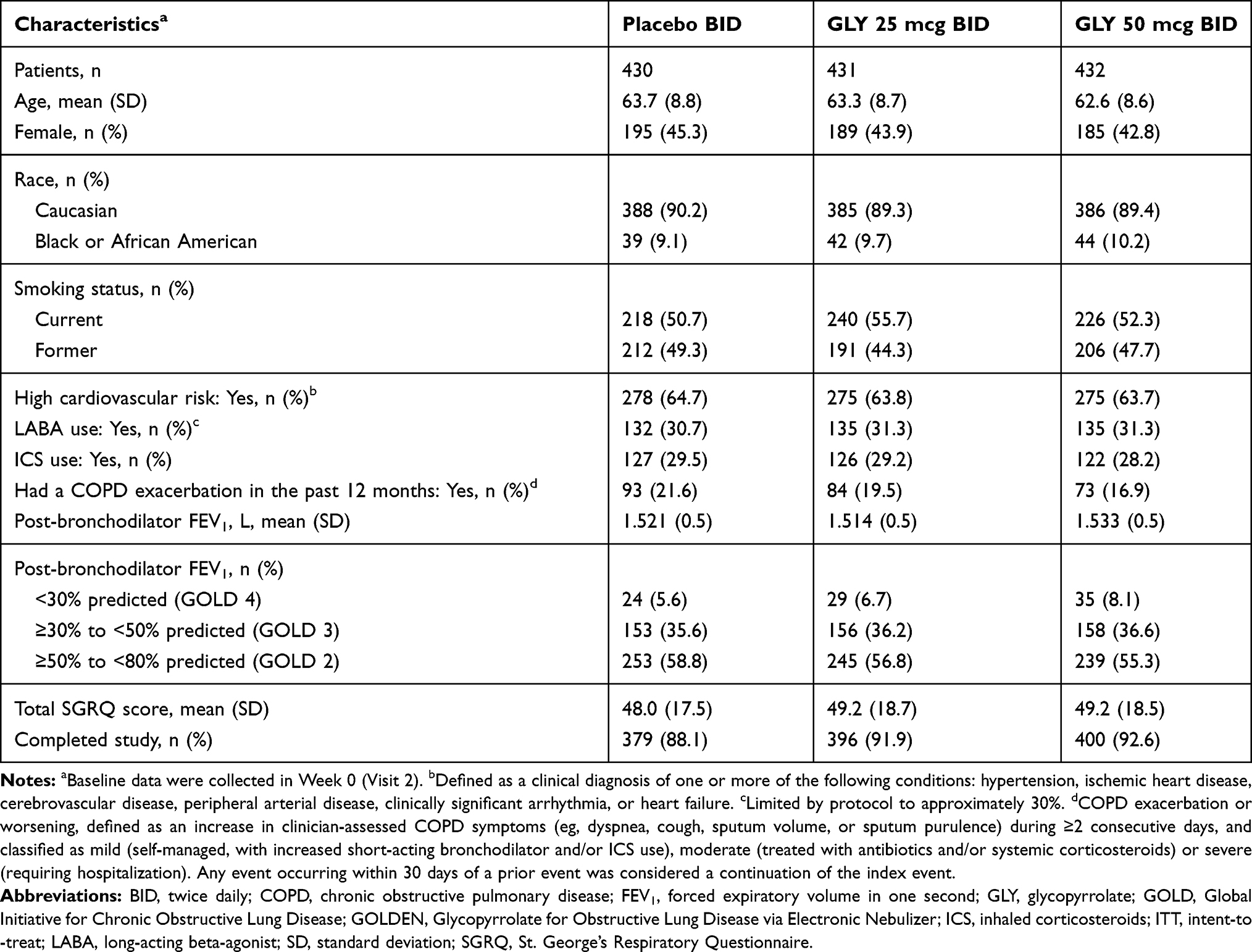 |
Table 1 Baseline Demographic and Clinical Characteristics of the Pooled GOLDEN 3 and GOLDEN 4 ITT Study Cohorts |
Effects of Nebulized GLY on the Risk of CID at 12 Weeks
At week 12, lower proportions of patients treated with GLY 25 mcg and 50 mcg BID had experienced ≥1 qualifying CID event compared to those who had received placebo (34.2% and 37.8%, respectively, versus 51.2%) (Table 2). Compared to placebo, treatment with GLY reduced the risk of any CID by 50% (OR: 0.5; 95% CI: 0.37–0.68) when administered at 25 mcg BID, and by 40% (OR: 0.60; 95% CI: 0.44–0.80) at 50 mcg BID (both, p<0.05) (Figure 2). Examining the CID component endpoints, patients treated with GLY BID, regardless of study dose, demonstrated sustained bronchodilator effects and maintained self-reported health status with lower proportions experiencing deterioration in trough FEV1 and SGRQ total score versus placebo. The risk of a ≥100-mL decline in trough FEV1 from baseline was reduced significantly by 59% (OR: 0.41; 95% CI: 0.27–0.62) with GLY 25 mcg BID, and by 52% (OR: 0.48; 95% CI: 0.32–0.72) with GLY 50 mcg BID (Figure 2), while the risk of a ≥4-unit increase (worsening) in the total SGRQ score was significantly decreased by 48% (OR: 0.52; 95% CI: 0.37–0.73) and 37% (OR: 0.67; 95% CI: 0.48–0.93), respectively (all, p<0.05). During the 12 weeks, less than 10% of patients in each cohort had experienced an HCRU-related moderate or severe exacerbation, resulting in no significant differences in the risk of this component endpoint between GLY BID and placebo (Table 2).
 |
Table 2 Proportions of Subjects Meeting Criteria for CID at Treatment Week 12 |
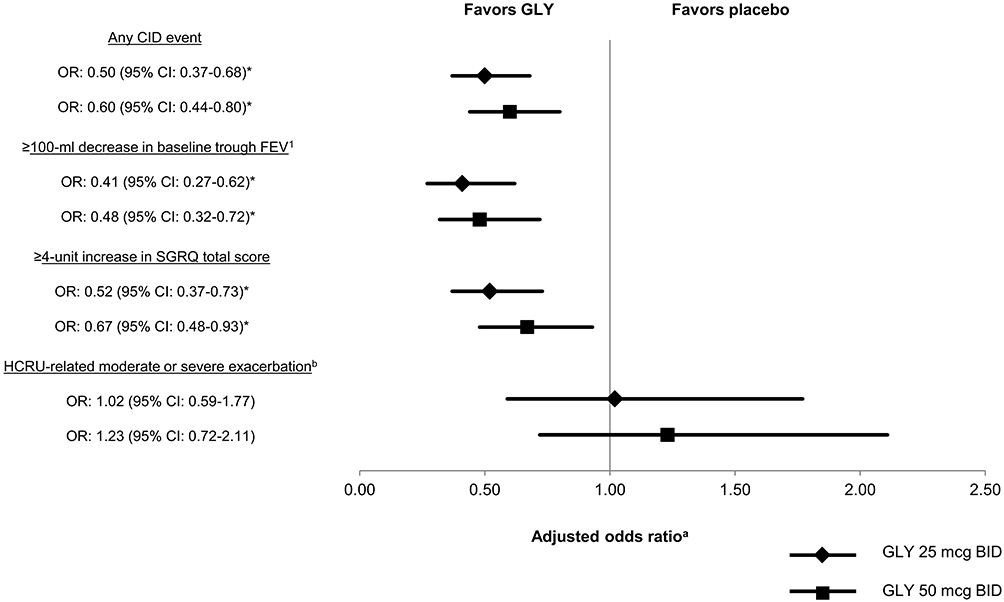 |
Figure 2 Risk (adjusted odds ratio)a of CID at week 12 of treatment with GLY (25 mcg BID and 50 mcg BID) compared to placebo. Notes: aOdds ratio (GLY/placebo), adjusted for high cardiovascular risk, LABA use, baseline FEV1, baseline SGRQ total score, and 12-month prior history of exacerbations. bDefined as an increase in clinician-assessed COPD symptoms (eg, dyspnea, cough, sputum volume, or sputum purulence) during at least two consecutive days, and classified as “moderate“ (treated with clinic visit, but no hospitalization, with or without antibiotics or oral corticosteroids) or “severe“ (requiring overnight stay in a hospital or emergency room). *p<0.05.Abbreviations: BID, twice daily; CI, confidence interval; CID, clinically important deterioration; FEV1, forced expiratory volume in one second; GLY, glycopyrrolate; HCRU, healthcare resource utilization; LABA, long-acting beta-agonist; OR, odds ratio; SGRQ, St. George’s Respiratory Questionnaire. |
Subgroup Analysis
In the subgroup analysis, the risks of CID were significantly lower (p<0.05) for GLY 25 mcg BID than placebo irrespective of age group, smoking status, background LABA use, COPD severity, or PIFR (Figure 3). Patients aged <65 years (OR 0.45, 95% CI 0.29, 0.68) and those with a PIFR <60 L/min (OR 0.36, 95% CI 0.20, 0.67) exhibited the most pronounced reductions in the risk of CID. Treatment with GLY 50 mcg BID also significantly decreased the risk of CID in most subgroups (Figure 4), except for the subgroup aged ≥65 years and females. The risk of CID in these subgroups was numerically lower but not significantly different from placebo. For both GLY regimens, patients <65 years, males, current smokers, and patients with PIFR <60 min/L experienced larger reductions in the risk of CID than the respective alternate subgroups. Treatment with the GLY 25 mcg BID had a greater impact on reducing CID in the subgroup with baseline FEV1 ≥50% predicted (versus FEV1 <50%) and was comparably effective in the subgroups with LABA and without LABA use. In contrast, larger effect sizes were observed in the 50 mcg BID subgroups with FEV1 <50% (versus FEV1 ≥50%) and no LABA use (versus LABA use).
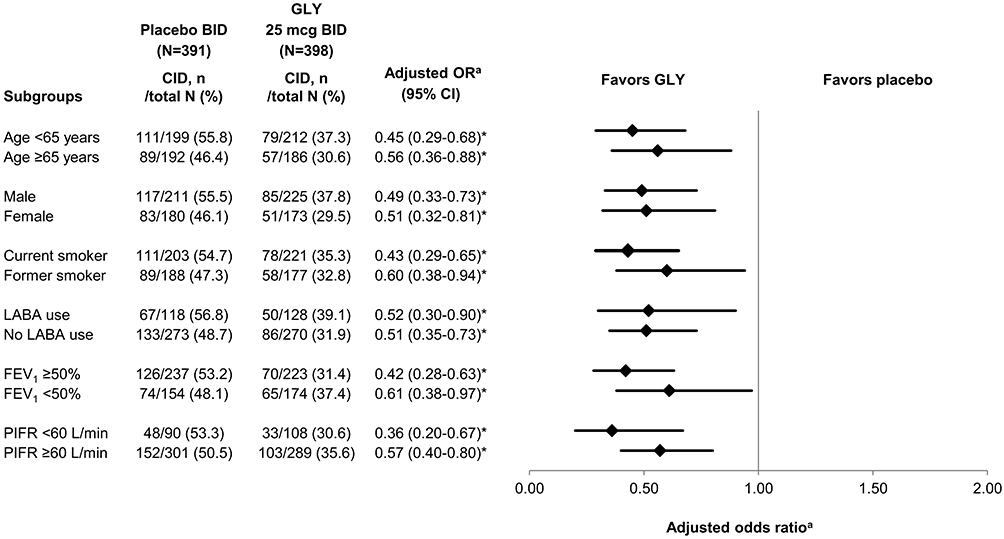 |
Figure 3 Subgroup analysis of the risk (adjusted odds ratio)a of CID at week 12 of treatment with GLY 25 mcg BID compared to placebo. Notes: aOdds ratio (GLY/placebo), adjusted for high cardiovascular risk, LABA use, baseline FEV1, baseline SGRQ total score, and 12-month prior history of exacerbations. *p<0.05.Abbreviations: BID, twice daily; CI, confidence interval; CID, clinically important deterioration; FEV1, forced expiratory volume in one second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GLY, glycopyrrolate; LABA, long-acting beta-agonist; OR, odds ratio; PIFR, peak inspiratory flow rate. |
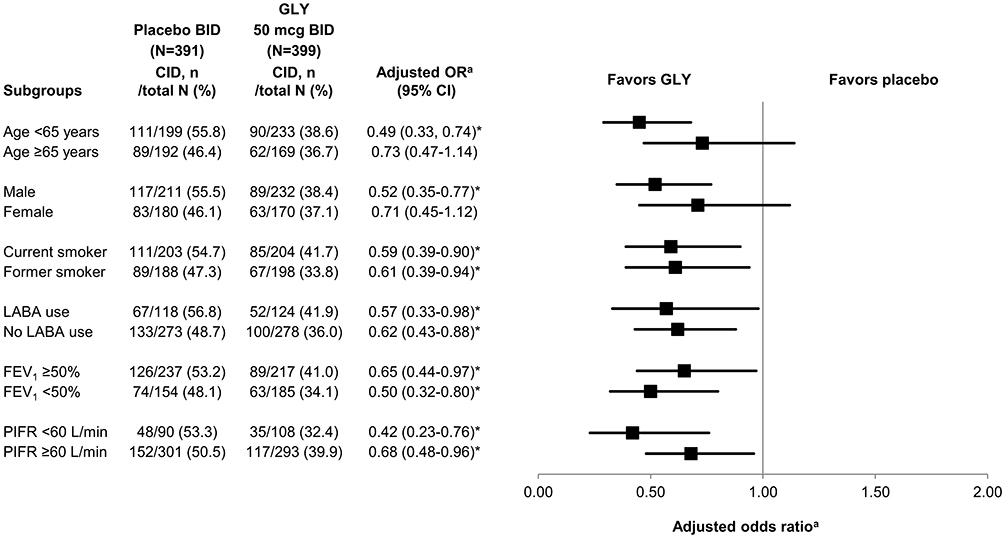 |
Figure 4 Subgroup analysis of the risk (adjusted odds ratio)a of CID at week 12 of treatment with GLY 50 mcg BID compared to placebo BID. Notes: aOdds ratio (GLY/placebo), adjusted for high cardiovascular risk, LABA use, baseline FEV1, baseline SGRQ total score, and 12-month prior history of exacerbations. *p<0.05.Abbreviations: BID, twice daily; CI, confidence interval; CID, clinically important deterioration; FEV1, forced expiratory volume in one second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GLY, glycopyrrolate; LABA, long-acting beta-agonist; OR, odds ratio; PIFR, peak inspiratory flow rate. |
Discussion
Quantifying the effectiveness of treatments in preventing worsening of COPD is essential given that minimizing the risk of progression is a primary goal of managing patients with stable disease.1 To provide a more comprehensive assessment in COPD, CID has emerged as an important composite endpoint that captures the multidimensional effects of treatment on key measures related to lung function, health status, and exacerbations. Each CID endpoint represents a clinically relevant event in COPD that may portend worse outcomes in the absence of effective intervention. Progressive decline in lung function is accelerated by exacerbations.7 COPD progression, however, is not restricted to deterioration in FEV1 and can manifest in worsening of patient-reported outcomes such health status and quality of life.17,18 Further, managing CID is critical as published evidence suggests that patients experiencing CID during the early months of bronchodilator therapy may experience poorer medium to long-term outcomes. A comparative study of indacaterol/glycopyrronium and salmeterol/fluticasone observed that CID during the first 12 treatment weeks was associated with significantly earlier and higher rates of moderate-to-severe exacerbations between 12 and 52 weeks (both, p<0.00001).15 A post hoc analysis of data from interventional and observational studies of fluticasone propionate/salmeterol found that at three years, the respective risk of CID in each component endpoint was significantly increased when CID in the endpoint occurred within 24 weeks. In contrast, no CID was significantly associated with higher quality of life scores and lower healthcare costs (all, p<0.001).11,19
In this post hoc analysis, patients with moderate-to-very severe COPD treated with GLY over 12 weeks were significantly less likely to experience CID compared to placebo with those treated with 25 mcg BID, the licensed regimen in the US, attaining a 50%-reduction in risk. Results of the subgroup analyses were largely consistent with the overall findings. At both GLY doses, reduction in the risk of CID was most pronounced for patients who had low PIFR (<60 L/min) at baseline, a finding which may be related to use of the nebulizer. Several studies have shown that individuals with poor inspiratory effort, such as the elderly and some patients with COPD, are unable to overcome the internal resistance of dry powder inhalers and therefore, have difficulty generating sufficient inspiratory flow for effective drug delivery.20–23 In these cases, the nebulizer’s vibrating membrane technology may offer an alternative mode as drug deposition is targeted to the lungs via regular tidal breathing.24 This nebulization method achieves a high percentage of aerosolized particles within the respiratory range, and does not require strong PIFR for device actuation or careful hand-breath coordination to achieve an effective dose. For these reasons, older patients with concomitant health conditions may likely also benefit from nebulized GLY. The comparative effectiveness of different inhalation devices in patients with COPD and poor inspiratory effort has not been established, and the choice of inhalation devices depends ultimately on a multitude of factors.25 However, a prospective, observational study in the US found that nearly one-third of patients hospitalized for a COPD exacerbation had a PIFR <60 min/L at discharge.23 It is possible that certain patients under such circumstances may benefit from inhalation devices that can enhance medication dispersal to the lungs.
Based on the ORs, treatment response to GLY appeared larger in the subgroup aged <65 years than in the subgroup ≥65 years. This was likely due to age-related differences in airflow capacity. Compared to older patients, younger patients generally have larger airflow capacity with FEV1 values averaging 2.0 liters.26 A 10% improvement in FEV1 in these younger patients could, therefore, represent an increase of 200 mL. FEV1 usually diminishes with normal aging and declines at accelerated rates up to −60 mL per year with cigarette smoking and COPD. As a result, airflow capacity is reduced in older patients (age ≥65) and may be as low as 1.0 liter.26 A 10% improvement in these patients could result in an increase of 100 mL. Therefore, a bronchodilator such as GLY would be expected to have a relatively larger positive FEV1 impact >100 mL in younger patients compared to older patients with COPD. Similarly, since younger patients likely experience greater net on-treatment milliliter improvements from baseline with nebulized GLY, they may be less likely to encounter net 100-mL declines meeting the FEV1 criteria for CID.
Examining the individual CID endpoints, patients treated with GLY were significantly more likely to maintain FEV1 and health status, but experienced no improvement in the risk of HCRU-related moderate or severe exacerbations over placebo. The latter may have been related to the low frequency of exacerbations during the study period and prior 12 months. Across all cohorts, deterioration in the total SGRQ score at week 12 was the strongest driver of CID (19.6–32.2%% of patients). A prior analysis of the pooled data from the GOLDEN 3 and GOLDEN 4 trials showed that GLY (25 mcg and 50 mcg BID) led to statistically significant improvements from baseline in the SGRQ total and component (Symptoms, Impacts, and Activity) scores compared to placebo.6,27 Change from baseline SGQR total score at week 12 was measured as the least squares mean and compared between GLY and placebo using analysis of variance. Applying the minimal clinically important difference criteria for SGRQ response (≥4 decrease in total score), the odds of improvement at week 12 were also significantly greater with both GLY 25 mcg (OR 1.68; 95% CI 1.24, 2.28) and 50 mcg (OR 1.36; 95% CI 1.00, 1.85) compared with placebo.27 In the present study, we identified a subset of patients who experienced CID in health status (based on the total SGRQ score). This finding highlights the potential utility of CID assessment in identifying “at-risk“ individuals who may be otherwise obscured in assessments of SGRQ response, and who might benefit from modifications in management.
Findings from this post hoc analysis are noteworthy as the data were pooled from two Phase III double-blind, placebo-controlled studies with robust replicate designs. Examining CID by the component endpoints also provided greater insight into how worsening in specific factors associated with COPD progression, ie, pulmonary function and health status, might be individually impacted during GLY treatment. Further, the analysis adds to the evidence supporting the utility of the composite CID endpoint for identifying therapies that prevent disease worsening, an important goal of management, particularly for patients who fail to achieve clinically meaningful responses to treatment.1,28
Study limitations include the 12-week study period of the GOLDEN 3 and GOLDEN 4 trials which precluded exploration of sustained CID. FEV1 and SGRQ were assessed only at baseline and at 12 weeks, the incidence of moderate or severe HCRU-related exacerbations was low, and fluctuations in disease state were not captured. Nonetheless, published evidence supports the merits of assessing and preventing early, short-term CID. Further, generalizability of the findings to patients with COPD managed in the real world is limited as the outcomes reflect those of the population selected for the Phase III trials. Both GOLDEN 3 and GOLDEN 4, however, were prospectively designed to enroll subjects representative of the general COPD population and included proportions of subjects who had very severe disease (post-bronchodilator FEV1% predicted <30%), continuing background LABA use with or without ICS, and high cardiovascular risk factors.6
Conclusion
Nebulized GLY (25 mcg and 50 mcg BID) administered over 12 weeks significantly reduced the risk of CID over placebo and was effective in preventing clinically meaningful worsening in FEV1 and patient-reported health status. These findings contribute to the evidence supporting the use of nebulized GLY BID as a maintenance treatment for patients with moderate-to-very-severe COPD. Assessment over a longer period may confirm a sustained effect in stabilizing disease.
Data Sharing Statement
Sunovion Pharmaceuticals Inc. is part of a clinical trial data sharing consortium that facilitates access for qualified researchers to selected anonymized clinical trial data. For up-to-date information on data availability, please visit https://www.clinicalstudydatarequest.com/Study-Sponsorts.aspx and click on “Sunovion”.
Acknowledgments
The authors would like to thank Vaidyanathan Ganapathy for input into the study design and interpretation of results and Ray Hsieh for data analysis support. The authors also kindly acknowledge Erin Williams for her medical writing contributions and Stratevi for logistical support in preparing this manuscript. The abstract of this paper was presented at the American Thoracic Society (ATS) Internal Conference, May 17–22, 2019 as a poster presentation. The poster’s abstract was published in American Thoracic Society Internal Conference Abstracts 2019 in the American Journal of Respiratory and Critical Care Medicine: https://doi.org/10.1164/ajrccm-conference.2019.199.1_MeetingAbstracts.A4524.
Disclosure
LM was employed by Evidera at the time this work was conducted, which provides consulting and other research services to pharmaceutical, device, government and non-government organizations. As an Evidera employee, she worked with a variety of companies and organizations and was expressly prohibited from receiving any payment or honoraria directly from these organizations for services rendered. EMK has participated in consulting, advisory boards, speaker panels, or received travel reimbursement from Amphastar, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline plc, Mylan, Novartis, Oriel, Pearl, Sunovion, Teva, and Theravance. He has conducted multicenter clinical research trials for approximately 40 pharmaceutical companies. CD and XN are employees of Sunovion. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: 2020 report. Available from: http://www.goldcopd.org.
2. Jenkins CR, Celli B, Anderson JA, et al. Seasonality and determinants of moderate and severe COPD exacerbations in the TORCH study. Eur Respir J. 2012;39(1):38–45. doi:10.1183/09031936.00194610
3. Punekar YS, Mullerova H, Small M, et al. Prevalence and burden of dyspnoea among patients with chronic pulmonary obstructive disease in five European countries. Pulm Ther. 2016;2(1):59–72. doi:10.1007/s41030-016-0011-5
4. Lonhala® Magnair® [prescribing information]. Lonhala® Magnair® [prescribing information]. Marlborough, MA: Sunovion Pharmaceuticals Inc; June 2019.
5. Pham S, Ferguson GT, Kerwin E, Goodin T, Wheeler A, Bauer A. In vitro characterization of the eFlow closed system nebulizer with glycopyrrolate inhalation solution. J Aerosol Med Pulm Drug Deliv. 2018;31(3):162–169. doi:10.1089/jamp.2017.1384
6. Kerwin E, Donohue JF, Goodin T, Tosiello R, Wheeler A, Ferguson GT. Efficacy and safety of glycopyrrolate/eFlow ((R)) CS (nebulized glycopyrrolate) in moderate-to-very-severe COPD: results from the glycopyrrolate for obstructive lung disease via electronic nebulizer (GOLDEN) 3 and 4 randomized controlled trials. Respir Med. 2017;132:238–250. doi:10.1016/j.rmed.2017.07.011
7. Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. doi:10.1136/thorax.57.10.847
8. Schmidt SA, Johansen MB, Olsen M, et al. The impact of exacerbation frequency on mortality following acute exacerbations of COPD: a registry-based cohort study. BMJ Open. 2014;4(12):e006720. doi:10.1136/bmjopen-2014-006720
9. Jones PW. St. George’s respiratory questionnaire: MCID. Copd. 2005;2(1):75–79. doi:10.1081/COPD-200050513
10. Wilke S, Jones PW, Mullerova H, et al. One-year change in health status and subsequent outcomes in COPD. Thorax. 2015;70(5):420–425. doi:10.1136/thoraxjnl-2014-205697
11. Paly VF, Naya I, Gunsoy NB, et al. Long-term cost and utility consequences of short-term clinically important deterioration in patients with chronic obstructive pulmonary disease: results from the TORCH study. Int J Chron Obstruct Pulmon Dis. 2019;14:939–951. doi:10.2147/COPD.S188898
12. Singh D, D’Urzo AD, Chuecos F, Munoz A, Garcia Gil E. Reduction in clinically important deterioration in chronic obstructive pulmonary disease with aclidinium/formoterol. Respir Res. 2017;18(1):106. doi:10.1186/s12931-017-0583-0
13. Singh D, Maleki-Yazdi MR, Tombs L, Iqbal A, Fahy WA, Naya I. Prevention of clinically important deteriorations in COPD with umeclidinium/vilanterol. Int J Chron Obstruct Pulmon Dis. 2016;11:1413–1424. doi:10.2147/COPD.S101612
14. Greulich T, Kostikas K, Gaga M, et al. Indacaterol/glycopyrronium reduces the risk of clinically important deterioration after direct switch from baseline therapies in patients with moderate COPD: a post hoc analysis of the CRYSTAL study. Int J Chron Obstruct Pulmon Dis. 2018;13:1229–1237. doi:10.2147/COPD.S159732
15. Anzueto AR, Kostikas K, Mezzi K, et al. Indacaterol/glycopyrronium versus salmeterol/fluticasone in the prevention of clinically important deterioration in COPD: results from the FLAME study. Respir Res. 2018;19(1):121. doi:10.1186/s12931-018-0830-z
16. Rodriguez-Roisin R. Toward a consensus definition for COPD exacerbations. Chest. 2000;117(Suppl 5):398S–401S. doi:10.1378/chest.117.5_suppl_2.398S
17. Nagai K, Makita H, Suzuki M, et al. Differential changes in quality of life components over 5 years in chronic obstructive pulmonary disease patients. Int J Chron Obstruct Pulmon Dis. 2015;10:745–757. doi:10.2147/COPD.S77586
18. Oga T, Nishimura K, Tsukino M, Sato S, Hajiro T, Mishima M. Longitudinal deteriorations in patient reported outcomes in patients with COPD. Respir Med. 2007;101(1):146–153. doi:10.1016/j.rmed.2006.04.001
19. Naya IP, Tombs L, Muellerova H, Compton C, Jones PW. Long-term outcomes following first short-term clinically important deterioration in COPD. Respir Res. 2018;19(1):222. doi:10.1186/s12931-018-0928-3
20. Mahler DA, Waterman LA, Ward J, Gifford AH. Comparison of dry powder versus nebulized beta-agonist in patients with COPD who have suboptimal peak inspiratory flow rate. J Aerosol Med Pulm Drug Deliv. 2014;27(2):103–109. doi:10.1089/jamp.2013.1038
21. Janssens W, VandenBrande P, Hardeman E, et al. Inspiratory flow rates at different levels of resistance in elderly COPD patients. Eur Respir J. 2008;31(1):78–83. doi:10.1183/09031936.00024807
22. Al-Showair RA, Tarsin WY, Assi KH, Pearson SB, Chrystyn H. Can all patients with COPD use the correct inhalation flow with all inhalers and does training help? Respir Med. 2007;101(11):2395–2401. doi:10.1016/j.rmed.2007.06.008
23. Sharma G, Mahler DA, Mayorga VM, Deering KL, Harshaw O, Ganapathy V. Prevalence of low peak inspiratory flow rate at discharge in patients hospitalized for COPD exacerbation. Chronic Obstr Pulm Dis. 2017;4(3):217–224. doi:10.15326/jcopdf.4.3.2017.0183
24. Kerwin EM, Donohue JF, Ferguson GT, Ganapathy V, Ozol-Godfrey A, Rajagopalan K. Satisfaction with the use of eFlow closed-system nebulizer in patients with moderate-to-very severe chronic obstructive pulmonary disease: findings from a long-term safety study. J Aerosol Med Pulm Drug Deliv. 2019;32(1):24–33. doi:10.1089/jamp.2018.1477
25. Tashkin DP. A review of nebulized drug delivery in COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2585–2596. doi:10.2147/COPD.S114034
26. Lange P, Celli B, Agusti A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl J Med. 2015;373(2):111–122. doi:10.1056/NEJMoa1411532
27. Ferguson GT, Kerwin EM, Donohue JF, et al. Health-related quality of life improvements in moderate to very severe chronic obstructive pulmonary disease patients on nebulized glycopyrrolate: evidence from the GOLDEN studies. Chronic Obstr Pulm Dis. 2018;5(3):193–207. doi:10.15326/jcopdf.5.3.2017.0178
28. Anzueto AR, Vogelmeier CF, Kostikas K, et al. The effect of indacaterol/glycopyrronium versus tiotropium or salmeterol/fluticasone on the prevention of clinically important deterioration in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1325–1337. doi:10.2147/COPD.S133307
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.