Back to Journals » International Journal of General Medicine » Volume 18
Clinical Value of APRI and FIB-4 on Bleeding Risk and 30-Day Prognosis in Patients with Liver Cirrhosis Complicated with Esophagogastric Varices
Authors Tian Q, Liu Y, Cao Q, Cheng M, Zhang M, Zhu F, He Y
Received 10 June 2025
Accepted for publication 4 October 2025
Published 9 October 2025 Volume 2025:18 Pages 6153—6167
DOI https://doi.org/10.2147/IJGM.S545850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Hyam Leffert
Qiuhui Tian,1 Yu Liu,1 Qiumei Cao,1 Mingjing Cheng,2 Meixu Zhang,1 Fengying Zhu,1 Yukai He1
1The Department of Gastroenterology and Hepatology, Jiangjin Hospital, Chongqing University of Chinese Medicine, Chongqing, People’s Republic of China; 2The Department of Laboratory Medicine, Dali Prefecture People’s Hospital, Dali City, Yunnan, People’s Republic of China
Correspondence: Qiumei Cao, Department of Gastroenterology and Hepatology, Jiangjin Hospital, Chongqing University of Chinese Medicine, No. 458, Jinma Road, Degan Sub-District, Jiangjin District, Chongqing, People’s Republic of China, Email [email protected] Mingjing Cheng, Department of Clinical Laboratory Diagnostics, the Department of Laboratory Medicine, Dali Prefecture People’s Hospital, No. 35 Renmin South Road, Dali City, Yunnan Province, People’s Republic of China, Email [email protected]
Objective: To assess the clinical utility of aspartate transaminase-to-platelet ratio index (APRI) and fibrosis-4 index (FIB-4) in predicting both the risk and 30-day prognosis of esophagogastric variceal bleeding (EGVB) in patients with liver cirrhosis.
Methods: In this retrospective cohort study, 231 cirrhotic patients (92 with EGVB and 139 controls) were randomly allocated to derivation (n=162) and validation (n=69) cohorts (7:3 ratio). Independent predictors of EGVB were identified through multivariate regression analysis, and a nomogram model was developed. Model performance was evaluated through internal validation assessing discrimination (ROC analysis), calibration (calibration curves), and clinical utility (decision curve analysis). The bleeding cohort was stratified into non-survivors (n=31) and survivors (n=61), with multivariate COX regression and Kaplan-Meier analyses examining associations between APRI/FIB-4 and 30-day mortality.
Results: APRI, FIB-4, and WBC emerged as independent EGVB risk factors (P< 0.05). The nomogram model demonstrated excellent predictive performance (AUC=0.794), good calibration, and clinical applicability. Combined assessment of all three indicators yielded superior predictive value (AUC=0.750; 95% CI:0.672– 0.829) compared to individual markers. Multivariate COX analysis revealed progressively stronger associations between elevated APRI (HR=12.09) and FIB-4 (HR=12.53) with mortality risk (P< 0.001). Kaplan-Meier analysis confirmed significantly reduced survival in patients exceeding high-risk thresholds (APRI≥ 10.27, FIB-4≥ 19.03; log-rank P< 0.001).
Conclusion: APRI, FIB-4, and WBC serve as independent EGVB predictors. The developed nomogram provides an effective screening tool, while the identified high-risk thresholds (APRI≥ 10.27, FIB-4≥ 19.03) offer valuable clinical warning indicators, enabling improved early diagnosis and intervention strategies for EGVB.
Keywords: liver cirrhosis, esophageal and gastric varices, gastrointestinal hemorrhage, APRI, FIB-4, nomogram
Corrigendum for this paper has been published.
Introduction
Liver cirrhosis represents a progressive, systemic disorder arising from chronic liver injury, marked by diffuse hepatic fibrosis, pseudolobule formation, and aberrant vascular proliferation.1 Approximately 85% of individuals with decompensated cirrhosis develop portal hypertension–related varices, of whom 30% experience life-threatening hemorrhage upon rupture.2 Esophagogastric variceal bleeding (EGVB) represents the most life-threatening complication of liver cirrhosis and accounts for its predominant mortality,3 with 50% cumulative incidence and acute mortality reaching 35%.4 This gastrointestinal emergency represents a critical endpoint in portal hypertension pathophysiology. Despite substantial therapeutic advances in managing portal hypertension and esophagogastric variceal hemorrhage, the annual incidence of first bleeding remains at 12%, with rebleeding rates exceeding 20% within six weeks.5
Although gastroscopy remains the gold standard for diagnosing acute gastrointestinal hemorrhage,6 its invasive nature—coupled with procedural risks, patient apprehension, and potential anesthetic complications—limits widespread adoption in screening settings. The hepatic venous pressure gradient (HVPG) provides precise prognostic stratification in cirrhosis, yet its clinical adoption remains limited by the complexity and invasiveness of measurement protocols.7 Consequently, identifying reliable non-invasive prognostic biomarkers for cirrhotic patients with esophagogastric variceal hemorrhage remains a critical unmet need.
Serum hepatic enzymes offer a promising non-invasive approach for risk stratification in EGVB. Among these, the aspartate aminotransferase-to-platelet ratio index (APRI) and fibrosis-4 (FIB-4) index - derived from routine parameters including AST, ALT, platelet count, and age - have emerged as clinically validated tools for hepatic fibrosis assessment, with potential utility in predicting EGVB outcomes. Multiple clinical studies have established the APRI as a robust non-invasive marker for both staging hepatic fibrosis and differentiating hepatitis C-induced cirrhosis from earlier fibrotic stages.8,9 In addition, APRI is significantly associated with the risk of HBV-related liver cancer and esophagogastric varices,10,11 and is an independent predictor of in-hospital mortality in hepatitis B decompensated cirrhosis.12 In addition, a study involving 12055 patients undergoing hepatectomy confirmed that APRI could be used as a marker of liver dysfunction and predict 30-day mortality after surgery.13
FIB-4 is a noninvasive scoring system developed based on the data of patients with viral hepatitis C,14 and its application has been extended to predict the progression of a variety of liver diseases. In non-alcoholic fatty liver disease (NAFLD), it provides dual predictive capacity, stratifying risks for both hepatic decompensation and major adverse cardiovascular events.5 Notably, FIB-4 shows particular clinical value in portal hypertension management, significantly predicting high-grade esophageal varices (≥Grade 2; P=0.029) and associated hemorrhage risk.15
Emerging evidence has established the clinical utility of APRI and FIB-4 indices beyond liver fibrosis evaluation, demonstrating robust predictive value for disease progression across various hepatic pathologies. However, their prognostic potential for EGVB and mortality risk in cirrhosis remains poorly characterized. This study investigates the combined predictive capacity of APRI and FIB-4 for disease severity and 30-day outcomes in cirrhotic EGVB, with the ultimate goal of informing risk stratification protocols, guiding personalized therapeutic strategies, and optimizing acute management algorithms-critical factors influencing both short-term survival and long-term clinical trajectories.
Materials and Methods
Study Population
We conducted a retrospective cohort study of 331 consecutive patients with cirrhosis admitted to Jiangjin Hospital, Chongqing University of Chinese Medicine between January 2020 and October 2024. The diagnostic criteria for liver cirrhosis:1 (1) Histopathological confirmation of cirrhosis by liver biopsy; or (2) Meeting at least two of the following criteria, with exclusion of non-cirrhotic portal hypertension: a) Imaging evidence of liver nodularity, splenomegaly, collateral circulation, or other features suggestive of cirrhosis and/or portal hypertension; b) Endoscopic identification of esophageal or gastric varices; c) Liver stiffness measurement (LSM) values indicative of cirrhosis: LSM ≥12.0 kPa when ALT <1×ULN, or LSM ≥17.0 kPa when ALT is between 1–5×ULN; d) Biochemical evidence of impaired synthetic function: serum albumin <35 g/L and/or prolonged prothrombin time (PT >3 seconds above control); e) Platelet count <100×109/L without other explanatory causes. The diagnostic criteria for cirrhosis with acute EGVB:16 Patients must exhibit signs of acute gastrointestinal bleeding (eg, hematemesis, melena, or positive fecal occult blood) within 5 days prior to admission, along with endoscopic confirmation meeting at least one of the following: a) Active bleeding from varices; b) Presence of a “white nipple sign” over varices; c) Varices with adherent clots in the absence of other potential bleeding sources.
Inclusion criteria: All enrolled patients were required to have complete clinical datasets and to fulfil the above diagnostic criteria for both liver cirrhosis and acute EGVB. Exclusion criteria included: (1) Combined with malignant tumors such as liver cancer; (2) Combined with other chronic liver diseases (such as cholangitis, drug-induced liver injury, etc).; (3) Severe cardiopulmonary and renal dysfunction; (4) Use of drugs affecting the coagulation system within the past 6 months; (5) Gastrointestinal bleeding patients with non-cirrhotic esophagogastric variceal bleeding caused by gastrointestinal ulcer, gastrointestinal mucosal tear or acute erosive gastritis. All patients completed blood routine, liver function, blood coagulation, renal function, electrolytes, abdominal CT or abdominal color ultrasound examination during hospitalization, and upper gastrointestinal endoscopy during hospitalization. The study was approved by the ethics committee at the authors’ hospitals (20230920).
Methods
Clinical Data Collection
The following demographic and laboratory data were collected from the electronic medical record system within 24 hours of admission. General information: Age, gender. Blood routine: C-reactive protein (CRP), white blood cell count (WBC), platelet (PLT), hemoglobin (HGB). Biochemical indicators: direct bilirubin (DBIL), alanine aminotransferase (ALT), albumin (ALB). Coagulation function: prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), prothrombin time activity (PTA), international normalized ratio (INR), D-dimer (D-D). According to the results of imaging and B-ultrasound examination, small amount of ascites: ascites depth <3cm or no ascites; Moderate ascites: the depth of ascites was 3–10cm; Severe ascites: ascites depth >10cm. Hepatic encephalopathy (HE) was defined according to the clinical symptoms and signs of the patient. Albumin-bilirubin index (ALBI), fibrosis-4 (FIB-4) index and aspartate aminotransferase-to-platelet ratio (APRI) index were calculated according to the results of the first laboratory examination on admission: ALBI = −0.085 × albumin (g/L) + 0.66 × log total bilirubin (μmol/L); APRI = AST/ULN/platelet count × 100 (ULN was the upper limit of normal AST); FIB-4 = (age × AST (U/L))/(PLT (109/L) ×√ALT). All data were collected and reviewed independently by two or more authors. Missing items were supplemented after review of clinical records. Data that could not be completed were removed, and the complete case data set was analyzed.
Grouping Criteria
In this study, the dataset was divided into derivation and validation cohorts at a ratio of 7:3 using random sampling. The patients were divided into acute EGVB group (bleeding group) and non-bleeding group according to the clinical manifestations (abdominal pain, hematemesis, melena, etc.) and endoscopic diagnosis results during hospitalization. The inclusion criteria for the bleeding group were as follows: (1) Positive occult blood test in gastric juice, vomit or stool; (2) Acute decrease in hemoglobin level; (3) The location of bleeding was determined by endoscopic diagnosis. Patients who did not meet the above criteria were classified into the non-bleeding group. The bleeding group was further divided into survival group and death group according to 30-day prognosis.
Statistical Analysis
All statistical analyses were conducted using R software (version 4.2.2) and SPSS software (version 27.0). For quantitative data that conformed to a normal distribution, independent sample t-tests were used for inter-group comparisons. Data that did not conform to a normal distribution were expressed as median (Q1, Q3), and inter-group comparisons were performed using the Mann–Whitney U-test. Qualitative data were expressed as the number of cases (%), and inter-group comparisons were conducted using the χ²-test or Fisher’s exact probability method. Multivariate logistic regression analysis was used to screen for independent influencing factors of EGVB in patients with liver cirrhosis. Continuous variables, including WBC, APRI, and FIB-4, were dichotomized based on optimal cut-off values determined by receiver operating characteristic (ROC) curve analysis to facilitate risk stratification and diagnostic classification. This approach maximizes classification accuracy by balancing specificity and sensitivity. A nomogram was developed using the rms package in R software (v.4.2.2) to provide a visual representation of the contribution of each predictor variable to clinical outcomes. Each variable was assigned a score proportional to its regression coefficient, and the total score corresponds to an individual’s predicted probability of a specific event or survival rate. Model performance was evaluated through multiple approaches. First, discrimination was assessed using ROC analysis, with the area under the curve (AUC) quantifying the model’s ability to differentiate between outcomes. Calibration was evaluated via calibration curves, generated using Bootstrap resampling to enhance reliability. A curve closely aligned with the 45° diagonal indicates good agreement between predicted and observed probabilities; significant deviation suggests over- or underestimation of risk. Decision curve analysis (DCA) was employed to evaluate clinical utility across a range of threshold probabilities by quantifying net benefit, comparing model-guided decisions against strategies of intervening for all or no patients. To examine the association between APRI, FIB-4, and 30-day mortality, optimal cut-off values were again derived from ROC curves and variables were dichotomized. Cox proportional hazards models were constructed under three adjustment tiers: Model 1—unadjusted; Model 2—adjusted for age and sex; Model 3—additionally adjusted for laboratory parameters (WBC, HGB, PLT, CRP, PT, INR, PTA, APTT, TT, D-Dimer, ALT, ALB, DBIL) and ascites. Survival distributions were visualized using Kaplan–Meier curves and compared with Log rank tests. All analyses were two-sided, and P-values <0.05 were considered statistically significant.
Results
Baseline Characteristics
This study strictly followed the inclusion and exclusion criteria, and 231 cirrhotic patients were finally screened (Figure 1), including 92 patients in the bleeding group and 139 patients in the non-bleeding group. The analysis of baseline data (Table 1) showed that the levels of WBC, ALT, ALBL, APRI, and FIB-4 on admission in the bleeding group were significantly higher than those in the non- bleeding group, while the levels of PLT, HGB, APTT, ALB, and DBIL were significantly lower, and the incidence of HE and 30-day mortality in the bleeding group were higher (P<0.05). The subjects were divided into derivation (n=162) and validation (n=69) cohorts with a ratio of 7:3 by random sampling method. Based on clinical rationality, HGB and HE, two secondary indicators after hemorrhage, were excluded from the model construction in this study. As shown in Table 2, the age, WBC, ALT, ALBL, APRI and FIB-4 levels of patients in the bleeding group in the derivation cohort were significantly higher than those in the non-bleeding group, and the PLT, ALB and DBIL levels were significantly lower (P<0.05). The levels of ALT, ALBL, APRI and FIB-4 in the validation group were significantly increased, and the levels of PLT and ALB were significantly decreased (P<0.05).
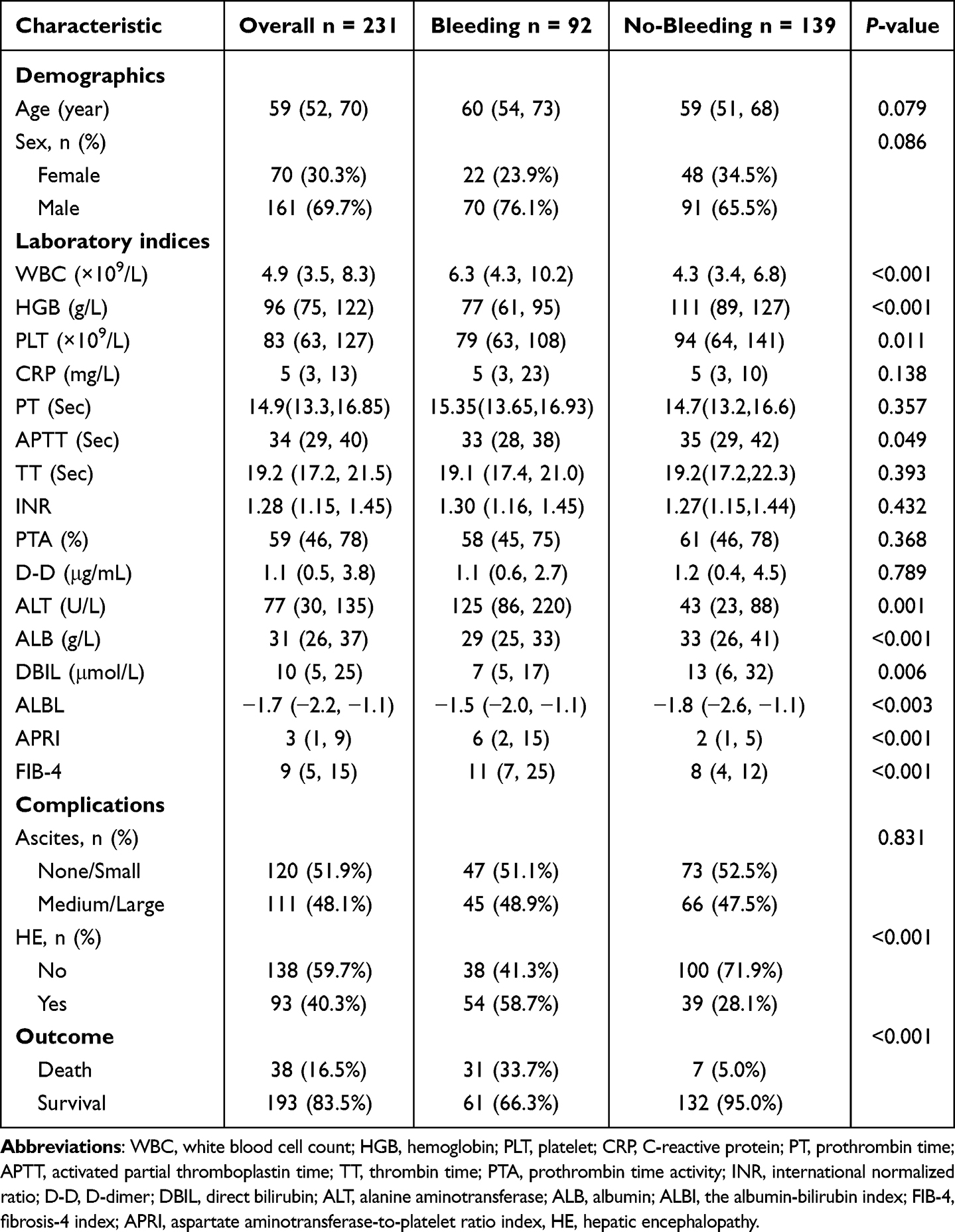 |
Table 1 Comparison of Baseline Data Between Cirrhotic Patients with Esophageal and Gastric Variceal Bleeding and Those Without Bleeding |
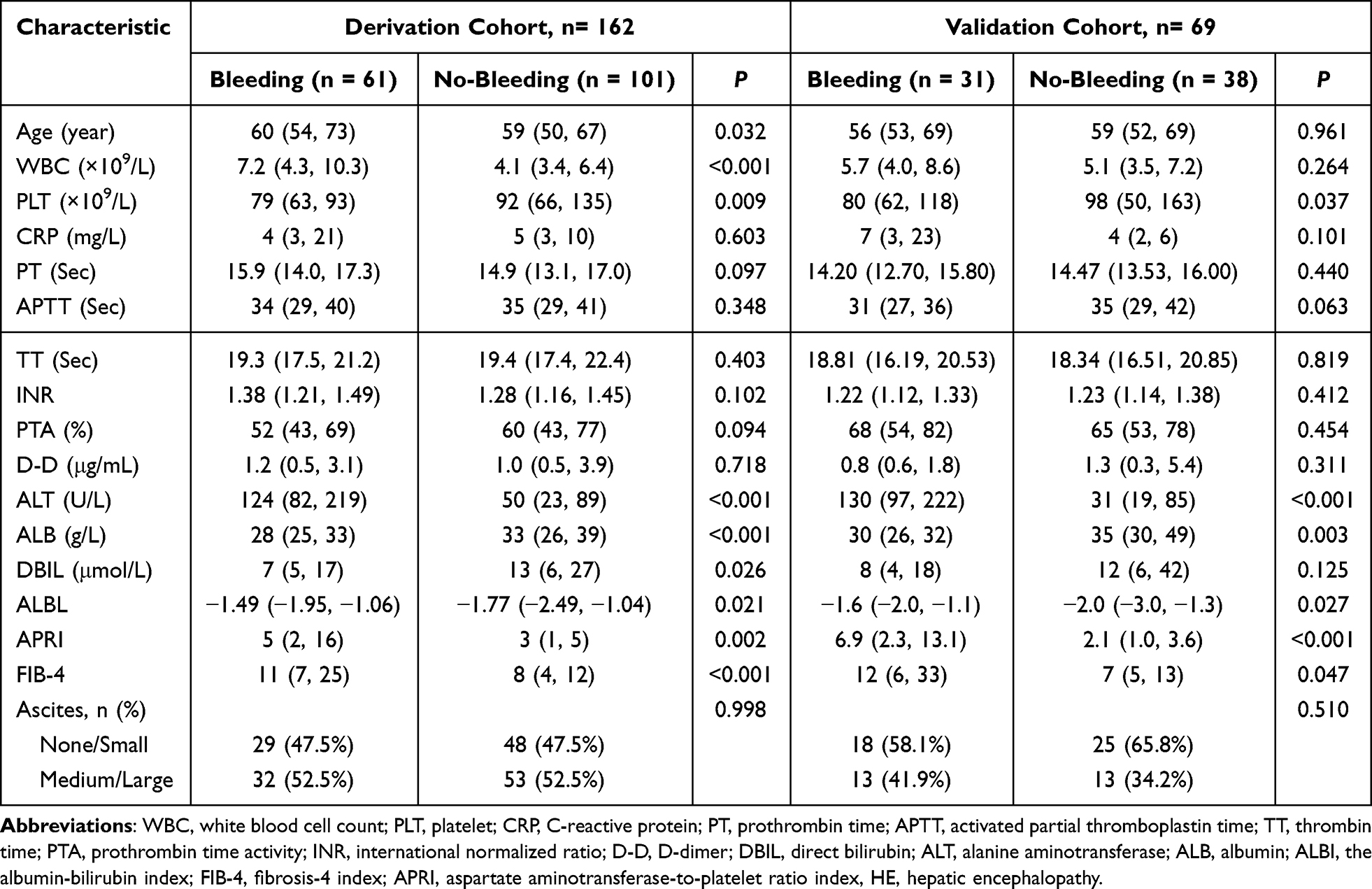 |
Table 2 Characteristics of Patients with Esophageal and Gastric Varices Due to Liver Cirrhosis in Derivation and Validation Cohorts |
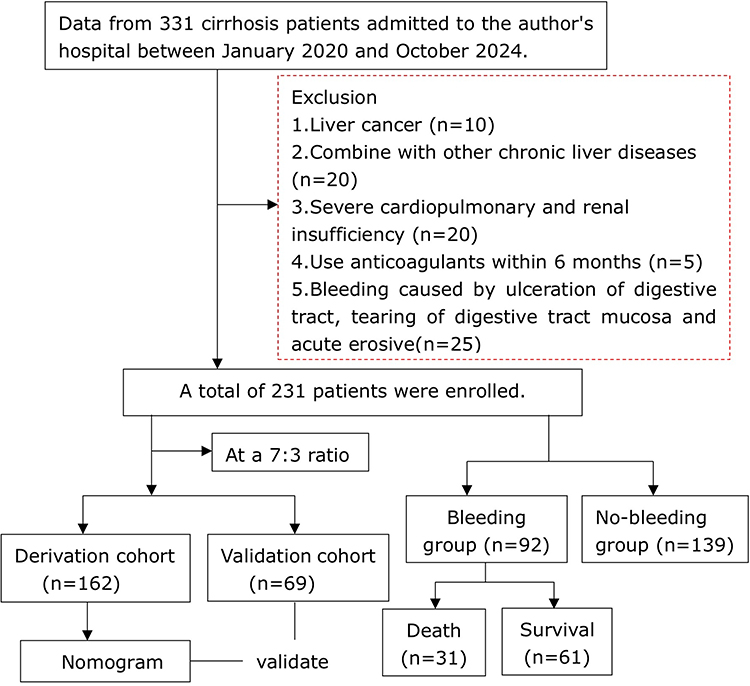 |
Figure 1 Flowchart of patient enrollment and study design. |
Independent Risk Factors for EGVB Patients with Liver Cirrhosis
Univariate Logistic regression of the derivation cohort (Table 3) indicated that age (OR=1.03, 95% CI: 1.01–1.06, P=0.018), WBC (OR=1.14, 95% CI: 1.05–1.23, P<0.001), ALBL (OR=1.52, 95% CI: 1.05–2.21, P=0.026), APRI (OR=1.10, 95% CI: 1.04–1.15, P<0.001), and FIB-4 (OR=1.07, 95% CI: 1.03–1.10, P<0.001) were risk factors for EGVB in liver cirrhosis, while ALB had a protective effect (OR=0.95, 95% CI: 0.92–0.99, P=0.013). After multivariate adjustment, only WBC (OR=1.18, 95% CI: 1.06–1.31, P=0.003), APRI (OR=1.09, 95% CI: 1.01–1.17, P=0.032), and FIB-4 (OR=1.08, 95% CI: 1.02–1.15, P=0.032) remained significant.
 |
Table 3 Risk Factor Analysis for Liver Cirrhosis Complicated by Esophageal Variceal Bleeding |
Model Construction and Performance Analysis
Based on the aforementioned analytical results, the optimal predictive cut-off values for WBC, APRI, and FIB-4 were determined using the Youden index derived from the ROC curve (Table 4). Subsequently, a nomogram-based prediction model was constructed utilizing these cut-off values (Figure 2). The model incorporated the following parameters: WBC (cut-off value of 3.81×10^9/L), APRI (cut-off value of 9.31), and FIB-4 (cut-off value of 19.75).
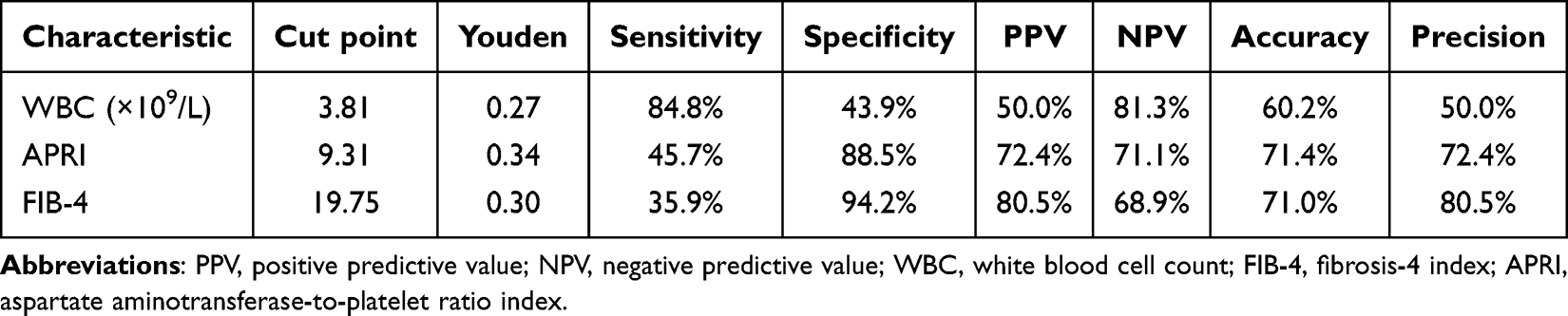 |
Table 4 Exploration of the Optimal Cut-off Point for a Single Evaluation Index in Patients with EGVB Due to Liver Cirrhosis |
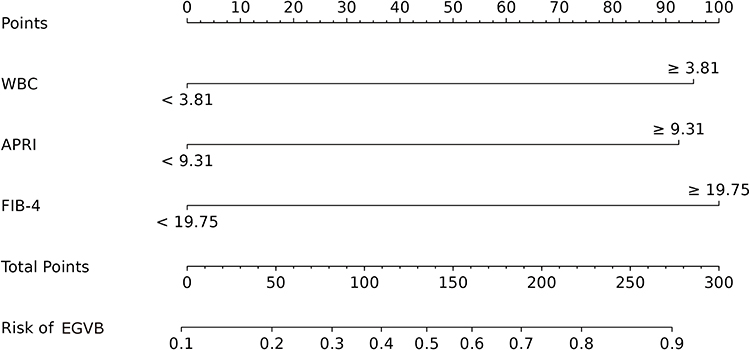 |
Figure 2 Nomogram model was constructed based on the risk factors screened by multivariate logistic regression analysis. |
The AUC of the derivation cohort model was 0.794 (95% CI: 0.727–0.861; Figure 3A), and the AUC of the validation cohort model was 0.829 (95% CI: 0.731–0.928; Figure 4A). The calibration of the model was assessed using calibration curves. The Bias-corrected line closely aligned with the Apparent line and approximated the Ideal line, indicating good agreement between predicted probabilities and observed outcomes (Figures 3B and 4B). Decision curve analysis (DCA) was employed to evaluate the clinical utility of the model. The results demonstrated that, compared with strategies of either intervening in all patients or none, applying the nomogram-based predictive intervention for patients with EGVB in liver cirrhosis yielded a higher net benefit (Figures 3C and 4C).
 |
Figure 3 Assess the diagnostic performance of the nomogram model derived from the derivation cohort. (A) ROC curve for evaluating the nomogram; (B) Calibration curve for the nomogram model; (C) DCA curve for the nomogram model. |
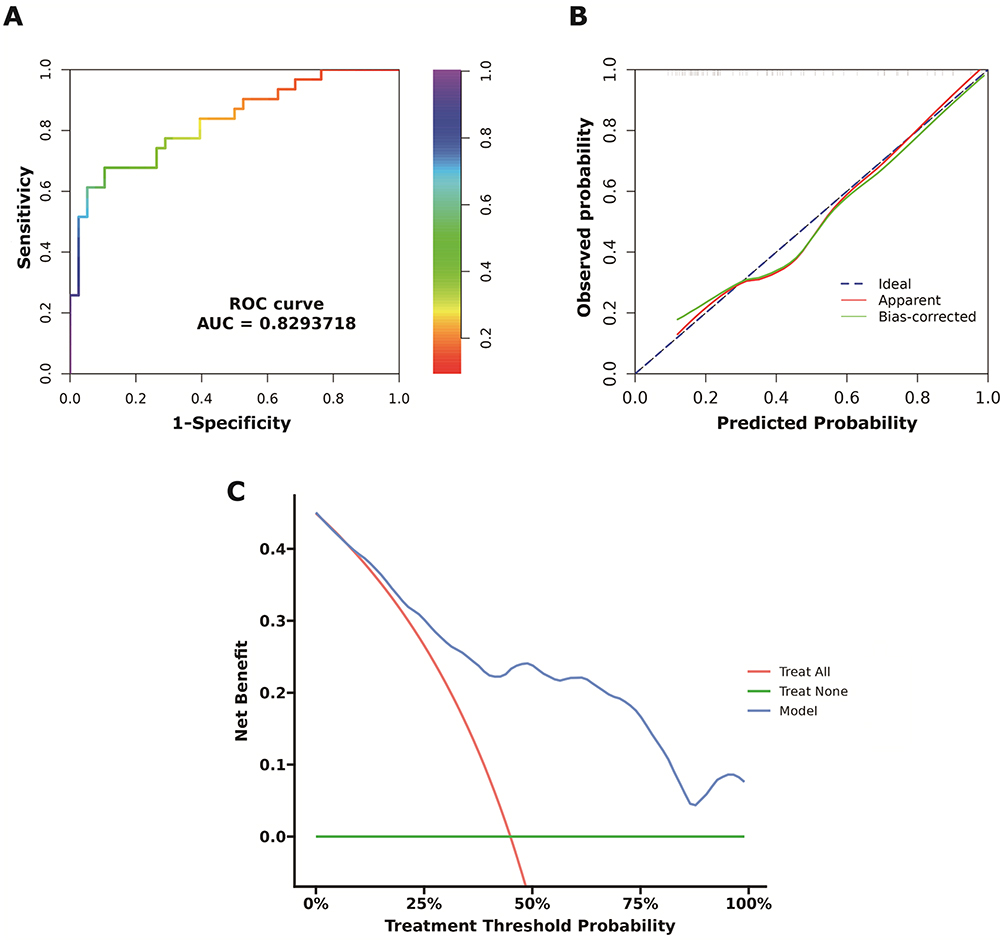 |
Figure 4 Assess the diagnostic performance of the nomogram model derived from the validation cohort. (A) ROC curve for evaluating the nomogram; (B) Calibration curve for the nomogram model; (C) DCA curve for the nomogram model. |
Further analysis revealed that in the derivation cohort, the combined detection of WBC, APRI, and FIB-4 yielded superior predictive efficacy (AUC = 0.750, 95% CI: 0.672–0.829) compared to single-index detection methods, including APRI alone (AUC = 0.643, 95% CI: 0.552–0.734), FIB-4 alone (AUC = 0.687, 95% CI: 0.601–0.772), and the combination of APRI and FIB-4 (AUC = 0.718, 95% CI: 0.635–0.801) (Figure 5A). Similarly, the same result is obtained in the validation cohort (Figure 5B). These findings substantiate that the integration of all three indices significantly enhances the predictive accuracy for EGVB in patients with cirrhosis.
 |
Figure 5 ROC curve of APRI, FIB-4, APRI + FIB-4 and APRI + FIB-4 + WBC for predicting EGVB in liver cirrhosis. (A) Derivation cohort; (B) Validation cohort. |
Baseline Characteristics of Deceased and Survived Patients with EGVB in Liver Cirrhosis
According to the 30-day prognosis, patients with bleeding were categorized into the death group (n=31) and the survival group (n=61). Anemia was stratified into four levels based on HGB concentration: mild (HGB > 90 g/L), moderate (HGB 60–90 g/L), severe (HGB 30–60 g/L), and extremely severe (HGB < 30 g/L). Compared with the survival group, the death group exhibited significantly higher levels of WBC, ALT, APRI, and FIB-4 (P < 0.05). Additionally, the death group demonstrated a marked reduction in HGB levels, predominantly characterized by severe and extremely severe anemia (P < 0.05) (Table 5).
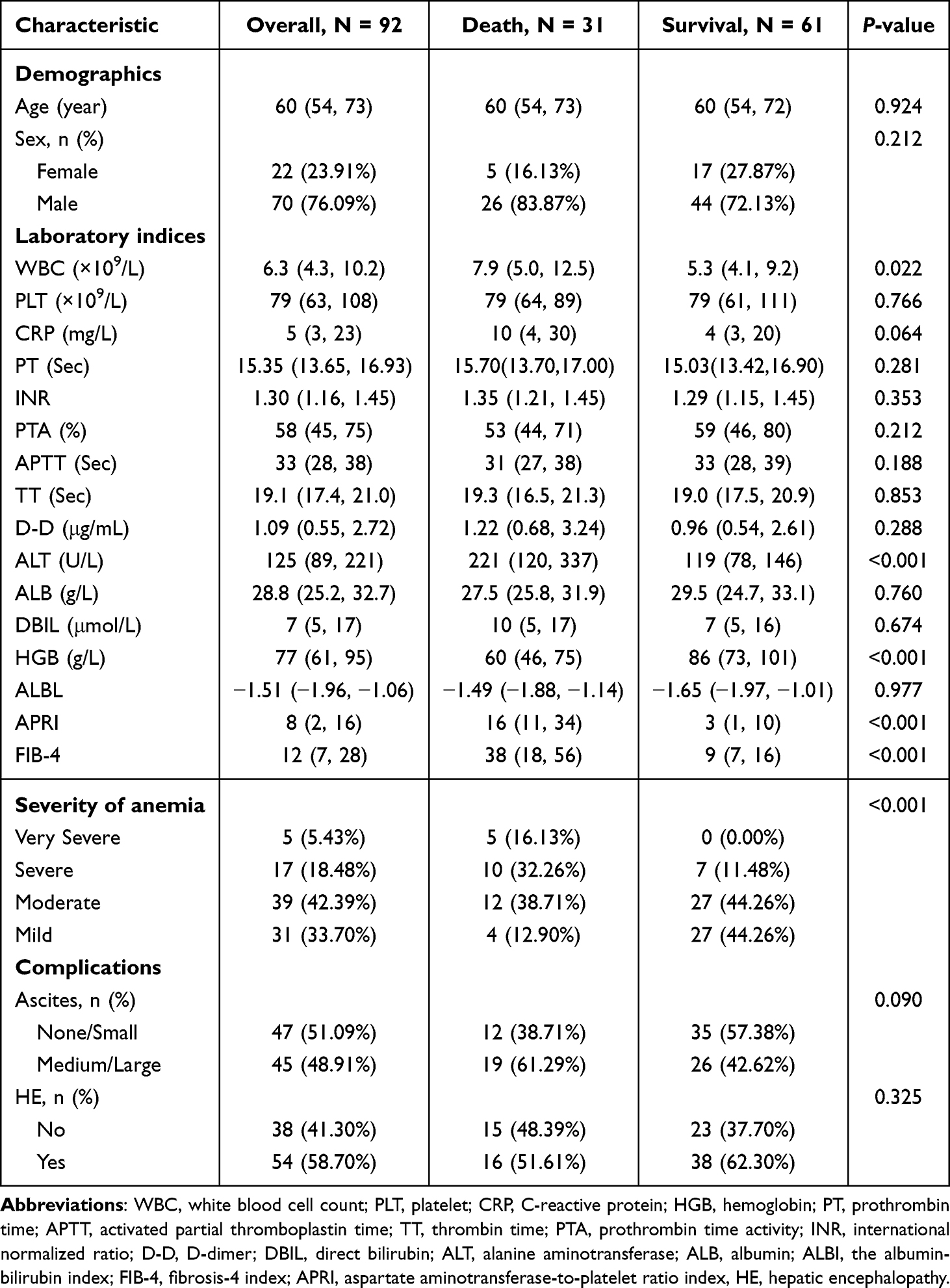 |
Table 5 Comparison of Baseline Data Between Deceased and Surviving Patients with Esophageal and Gastric Variceal Bleeding Due to Liver Cirrhosis |
Correlation of APRI and FIB-4 with 30-Day Prognosis in Cirrhotic Patients with EGVB
The optimal predictive thresholds for APRI and FIB-4 were determined using the Youden index derived from the ROC curve (Table 6). Multivariate COX regression analysis (Table 7) revealed that when APRI ≥ 10.27, the unadjusted model (Model 1) demonstrated a 6.70-fold increased risk of death compared to the APRI < 10.27 group (HR = 6.70, 95% CI: 2.87–15.64, P < 0.001). After adjusting for gender and age (Model 2), the HR increased to 7.03 (95% CI: 2.92–16.94, P < 0.001). Further adjustment for WBC, HGB, PLT, CRP, PT, INR, PTA, APTT, TT, D-D, ALT, ALB, DBIL, and ascites (Model 3), resulted in an even higher HR of 12.09 (95% CI: 3.26–44.74, P < 0.001). Similarly, for FIB-4 ≥ 19.03, the unadjusted model showed a 5.83-fold increased risk of death compared to the control group. Stepwise adjustments led to HR values of 6.57 (Model 2) and 12.53 (Model 3). Notably, as covariates were progressively adjusted, the positive correlation between APRI, FIB-4 and mortality risk continued to strengthen (P < 0.001), indicating that both indices are independent prognostic factors. This conclusion remained consistent when APRI and FIB-4 were analyzed as continuous variables. Kaplan-Meier survival analysis further confirmed significantly worse outcomes in patients with APRI ≥ 10.27 (Figure 6A) and FIB-4 ≥ 19.03 (Figure 6B) (Log-rank P < 0.001).
 |
Table 6 Exploration of the Optimal Cut-off Point for a Single Evaluation Index for Death Caused by EGVB in Patients with Liver Cirrhosis |
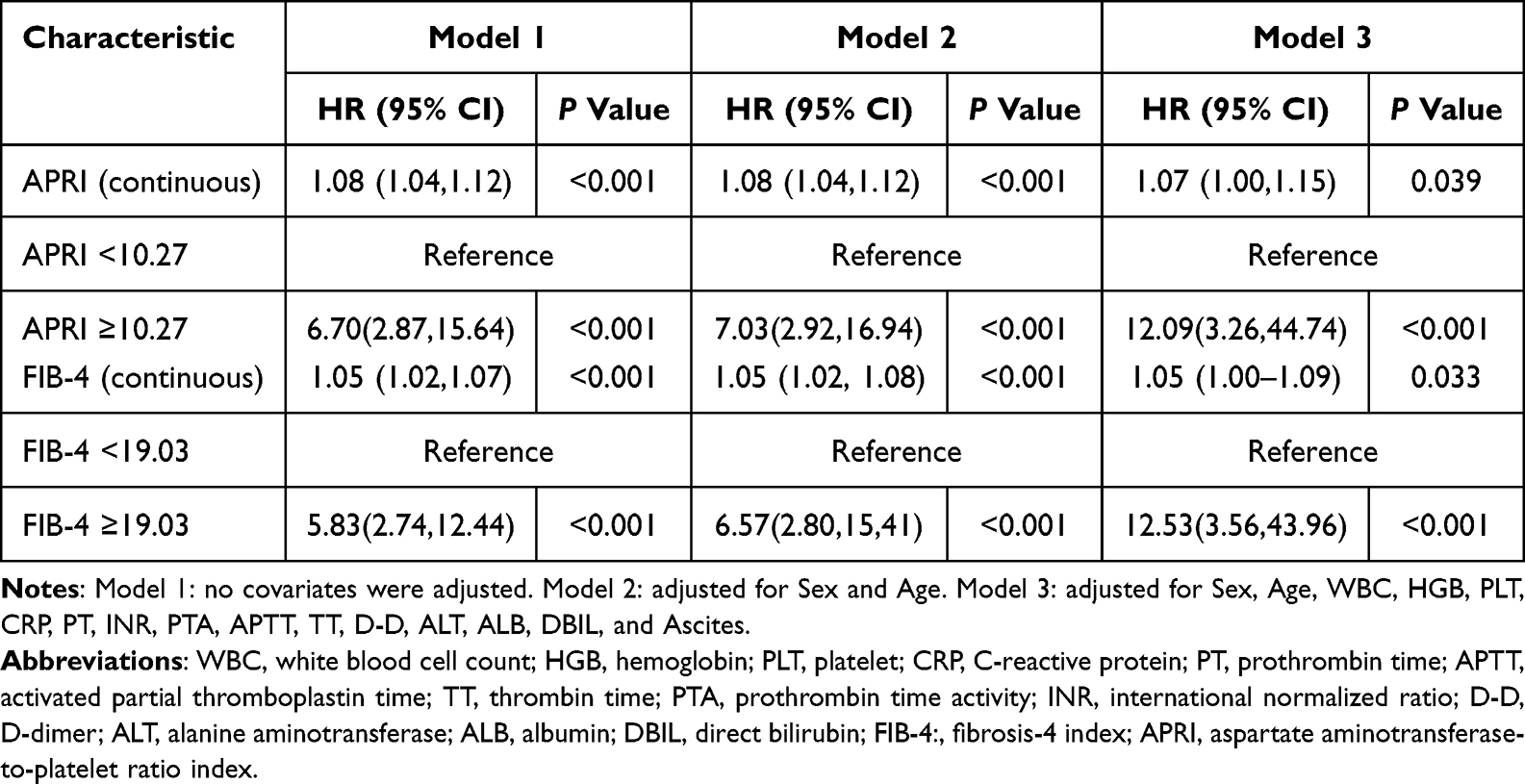 |
Table 7 Relationship Between APRI and FIB-4 with 30-Day Mortality in Cirrhotic Patients with EGVB |
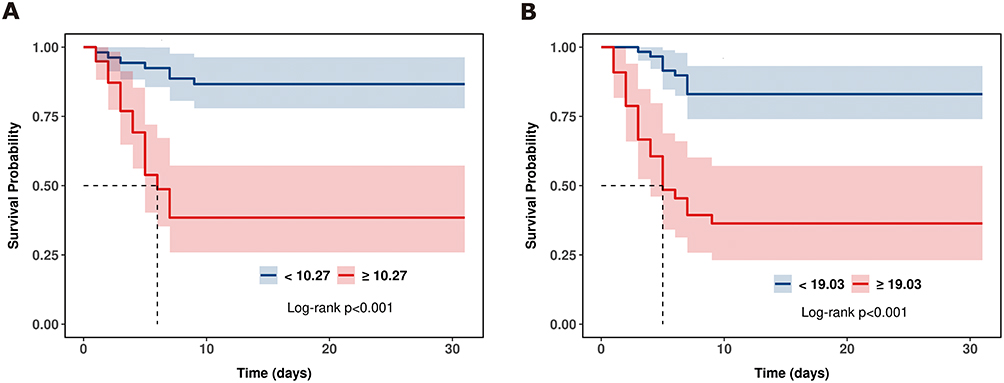 |
Figure 6 Correlation of APRI and FIB-4 with 30-day prognosis in cirrhotic patients with EGVB. (A) for APRI; (B) for FIB-4. |
Discussion
Using a retrospective cohort analysis, this study confirmed the value of APRI and FIB-4 as noninvasive serological markers for assessment of both EGVB risk and short-term prognosis in patients with liver cirrhosis. The key findings are summarized as follows: (1) Patients in the bleeding group exhibited significantly elevated WBC, ALT, ALBL, APRI, and FIB-4 levels, as well as reduced PLT, HGB, APTT, ALB, and Dbil. This group also showed a significantly higher incidence of both hepatic encephalopathy and 30-day mortality (P < 0.05). (2) Multivariate regression analysis identified APRI, FIB-4, and WBC as independent risk factors for EGVB (P < 0.05). (3) A nomogram model based on these indicators demonstrated strong discriminative ability, calibration, and clinical utility. (4) Cox regression analysis revealed significant associations between both APRI and FIB-4 and an increased risk of death (P < 0.001). Consistent with this, Kaplan-Meier survival curves indicated markedly reduced survival rates in patients with APRI ≥ 10.27 and FIB-4 ≥ 19.03 (log-rank P < 0.001).
The study found that the clinicopathological features of EGVB were more severe on admission. These included more pronounced liver injury, coagulopathy, anemia, and worse clinical outcomes (Table 1). These manifestations resemble the core pathophysiological changes observed in advanced liver cirrhosis.17 Although current guidelines strongly recommend endoscopy within 12 hours for suspected EGVB,18 the invasive nature, substantial cost, and limited availability of this procedure in underserved regions often impede timely diagnosis and follow-up. Therefore, the development of a simple, non-invasive model for diagnosing EGVB is of significant clinical importance.
APRI and FIB-4, both of which are well-established non-invasive indicators of liver fibrosis,19,20 are closely associated with the development and progression of EGVB.21 Consistent with previous reports, the present study demonstrated significantly elevated APRI and FIB-4 levels in patients with EGVB compared to non-bleeding controls, as well as in non-survivors relative to survivors, underscoring the association of these indicators with the severity and prognosis of EGVB. These observations are supported by the central pathophysiological role of progressive liver fibrosis in the promotion of intrahepatic vascular resistance, vasodilatory dysfunction, and increased portal blood flow, culminating in clinically significant portal hypertension (CSPH) and the formation of collateral circulation, key drivers of EGVB development.22 APRI and FIB-4 are computed from routinely measured parameters, including PLT, AST, and ALT, and reflect multiple dimensions of liver pathology. Notably, a PLT count ≥150×109/L, particularly when combined with transient elastography (TE), has been proposed for the reliable exclusion of CSPH in patients with advanced liver disease, potentially obviating the need for endoscopic surveillance.23 In addition, ALT and AST represent sensitive markers of hepatocyte damage and mitochondrial dysfunction, respectively.24 The combination of these parameters can thus enhance the prediction of both the severity of liver fibrosis and the risk of EGVB associated with cirrhosis-related disease.
Furthermore, this study identified elevated WBC as an independent risk factor for EGVB in patients with cirrhosis. WBC levels were significantly higher in the non-surviving EGVB group compared to survivors. This finding appears to contrast with the well-documented phenomenon of leukopenia, a frequent complication in cirrhosis typically attributed to hypersplenism, bone marrow suppression, and recurrent viral infections.25 Leukopenia is known to increase susceptibility to infections and bleeding events, potentially leading to sepsis or fatal hemorrhage.26,27 The observed elevated WBC levels in severe EGVB cases may also indicate inflammatory or stress responses associated with acute bleeding complications, suggestive of a distinct pathophysiology in this context.
There is as yet no consensus on the accurate assessment of EGVB-related risk factors in patients with liver cirrhosis. Various approaches to the evaluation of EVGB risk have been used, including radiomics, liver stiffness measurement (LSM), and the Glasgow-Blatchford score (GBS).28–30 However, these methods may have limitations in terms of accuracy, applicability, and cost in clinical practice.31 The development of novel, effective, and convenient predictive models that enable early, individualized, and precise interventions is thus needed. These tools have potential for lowering the rates of rebleeding and mortality, reducing the length of hospitalization, and decreasing healthcare costs. This study describes the construction of a nomogram based on APRI, FIB-4, and WBC levels. The nomogram showed excellent predictive performance and calibration, as well as significant clinical utility. The model is non-invasive, convenient, cost-effective, and well-suited for widespread clinical adoption.
Survival analyses indicated that both APRI and FIB-4 were reliable prognostic biomarkers in cirrhotic patients with EGVB. The optimal cut-off values of APRI ≥ 10.27 and FIB-4 ≥ 19.03 were effective for assessing increased risk of mortality, consistent with earlier findings.32 The application of these biomarkers may enhance early detection of high-risk patients and improve resource allocation. Enhanced monitoring and the implementation of proactive preventive strategies in these patients would improve clinical outcomes.
Limitations
This study has several limitations that warrant consideration. First, key confounding factors such as esophageal varices grading, portal vein diameter, and antiviral treatment were not incorporated into the analysis, which may introduce potential biases. Second, the study sample was restricted to patients with EGVB, thereby limiting the generalizability of the findings. Third, this retrospective study could not dynamically monitor biomarker changes, leaving their temporal variations and clinical relevance for EGVB risk prediction unassessed. Consequently, the current results should be further validated through multi-center, large-scale, and prospective studies.
Conclusion
This study identified APRI, FIB-4, and WBC as being strongly associated with EGVB and developed a nomogram model based on these variables. This model enables individualized prediction of bleeding risk, and its dynamic risk assessment function assists clinicians in identifying high-risk patients at an early stage and implementing preventive measures promptly, thereby reducing the incidence of bleeding events. The high-risk threshold (APRI ≥ 10.27, FIB-4 ≥ 19.03) can serve as a clinical warning indicator, offering new evidence-based support for the development of early intervention strategies for EGVB. By integrating routine laboratory parameters, this study achieves non-invasive and cost-effective risk assessment, demonstrating excellent clinical applicability and potential for widespread adoption.
Ethics Approval and Consent to Participate
This study conformed to the guidelines of the Helsinki Declaration. Ethics approval was obtained by the Ethics Committee of Jiangjin Hospital, Chongqing University of Chinese Medicine (NO.20230920). All patients induced in this study were informed of the research content and signed informed consent.
Acknowledgments
The authors would like to thank all the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Chongqing Medical Scientific Research Project (Joint Project of Chongqing Health Commission and Science and Technology Bureau) [No. 2024ZYYB003] and the Research Program of Chongqing Jiangjin District Science and Technology Bureau [No. ZYY2022017].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chinese Society of Hepatology,Chinese Medical Association. Chinese guidelines on the management of liver cirrhosis. Zhonghua Gan Zang Bing Za Zhi. 2019;27(11):846–865.
2. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65(1):310–335. doi:10.1002/hep.28906
3. Kumar R, Kerbert AJC, Sheikh MF, et al. Determinants of mortality in patients with cirrhosis and uncontrolled variceal bleeding. J Hepatol. 2021;74(1):66–79. doi:10.1016/j.jhep.2020.06.010
4. Wang DX, Wu XJ, Yu JZ, et al. Visualizing global progress and challenges in esophagogastric variceal bleeding. World J Gastrointest Surg. 2025;17(4):102020. doi:10.4240/wjgs.v17.i4.102020
5. Liu LZ, Sun J, Hou J, Chan HLY. Improvements in the management of chronic hepatitis B virus infection. Expert Rev Gastroenterol Hepatol. 2018;12(11):1153–1166. doi:10.1080/17474124.2018.1530986
6. Hwang JH, Shergill AK, Acosta RD, et al. American society for gastrointestinal endoscopy. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc. 2014;80(2):221–227. doi:10.1016/j.gie.2013.07.023
7. Bai Z, Li B, Lin S, et al. Development and validation of CAGIB score for evaluating the prognosis of cirrhosis with acute gastrointestinal bleeding: a retrospective multicenter study. Adv Ther. 2019;36(11):3211–3220. doi:10.1007/s12325-019-01083-5
8. Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–526. doi:10.1053/jhep.2003.50346
9. Shrivastava R, Sen S, Banerji D, Praharaj AK, Chopra GS, Gill SS. Assessment of non-invasive models for liver fibrosis in chronic hepatitis B virus related liver disease patients in resource limited settings. Indian J Pathol Microbiol. 2013;56(3):196–199. doi:10.4103/0377-4929.120359
10. Zhang X, Guan L, Tian H, et al. Risk factors and prevention of viral hepatitis-related hepatocellular carcinoma. Front Oncol. 2021;11:686962. doi:10.3389/fonc.2021.686962
11. Mai RY, Wang YY, Bai T, et al. Combination of ALBI and APRI to predict post-hepatectomy liver failure after liver resection for HBV-related HCC patients. Cancer Manag Res. 2019;11:8799–8806. doi:10.2147/CMAR.S213432
12. Mao W, Sun Q, Fan J, Lin S, Ye B. AST to platelet ratio index predicts mortality in hospitalized patients with hepatitis B-related decompensated cirrhosis. Medicine. 2016;95(9):e2946. doi:10.1097/MD.0000000000002946
13. Starlinger P, Ubl DS, Hackl H, et al. Combined APRI/ALBI score to predict mortality after hepatic resection. BJS Open. 2021;5(1):zraa043. doi:10.1093/bjsopen/zraa043
14. Sterling RK, Lissen E, Clumeck N, et al. APRICOT clinical investigators. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–1325. doi:10.1002/hep.21178
15. Tarannum S, Ilyas T, Tarannum Shaik S, et al. Assessment of the child-pugh score, model for end-stage liver disease score, fibrosis-4 index and AST to Platelet Ratio Index as Non-Endoscopic Predictors of the Presence of Esophageal Varices and Variceal Bleeding in Chronic Liver Disease Patients. Cureus. 2024;16(11):e73768.
16. Chinese Society of Spleen and Portal Hypertension Surgery. Expert consensus on the diagnosis and treatment of esophageal and gastric variceal rupture bleeding in cirrhotic portal hypertension (2024 edition). Zhonghua wai Ke Za Zhi. 2025;63(3):177–186. doi:10.3760/cma.j.cn112139-20241128-00535
17. Zampino R, Patauner F, Durante-Mangoni E. Clinical trajectories in liver cirrhosis: an evidence-based reappraisal for the internist. Eur J Internal Med. 2025.
18. Shiha G, Ibrahim A, Helmy A, et al. Asian-pacific association for the study of the liver (APASL) consensus guidelines on invasive and non-invasive assessment of hepatic fibrosis: a 2016 update. Hepatol Internat. 2025;11(1):1–30. doi:10.1007/s12072-016-9760-3.
19. Ballestri S, Mantovani A, Baldelli E, et al. Liver fibrosis biomarkers accurately exclude advanced fibrosis and are associated with higher cardiovascular risk scores in patients with NAFLD or viral chronic liver disease. Diagnostics. 2021;11(1):98. doi:10.3390/diagnostics11010098
20. Xiao G, Yang J, Yan L. Comparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: a systemic review and meta-analysis. Hepatology. 2015;61(1):292–302. doi:10.1002/hep.27382
21. Deng H, Qi X, Guo X. Diagnostic accuracy of APRI, AAR, FIB-4, FI, King, Lok, Forns, and FibroIndex scores in predicting the presence of esophageal varices in liver cirrhosis: a systematic review and meta-analysis. Medicine. 2015;94(42):e1795. doi:10.1097/MD.0000000000001795
22. Ginès P, Krag A, Abraldes JG, Solà E, Fabrellas N, Kamath PS. Liver cirrhosis. Lancet. 2021;398(10308):1359–1376. doi:10.1016/S0140-6736(21)01374-X
23. de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C. Baveno VII faculty. Baveno VII - renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974. doi:10.1016/j.jhep.2021.12.022
24. Xu Z, Xu B. Nonlinear association between AST/ALT ratio and 28-day all-cause mortality following ICU admission in critically ill cirrhotic patients: a retrospective cohort study. BMC Gastroenterol. 2025;25(1):367. doi:10.1186/s12876-025-03966-0
25. Newburger PE, Dale DC. Evaluation and management of patients with isolated neutropenia. Semin Hematol. 2013;50(3):198–206. doi:10.1053/j.seminhematol.2013.06.010
26. Su M, He M, Yang WC, et al. The therapeutic effect of leucogen in treating alcoholic liver cirrhosis with thrombocytopenia or leukopenia. Ann Saudi Med. 2025;45(1):9–17. doi:10.5144/0256-4947.2025.9
27. Triantos C, Kalafateli M, Assimakopoulos SF, et al. Endotoxin translocation and gut barrier dysfunction are related to variceal bleeding in patients with liver cirrhosis. Front Med Lausanne. 2022;9:836306. doi:10.3389/fmed.2022.836306
28. Peng YJ, Liu X, Liu Y, Tang X, Zhao QP, Du Y. Computed tomography-based multi-organ radiomics nomogram model for predicting the risk of esophagogastric variceal bleeding in cirrhosis. World J Gastroenterol. 2024;30(36):4044–4056. doi:10.3748/wjg.v30.i36.4044
29. Krishnan A. Improving radiomics-based models for esophagogastric variceal bleeding risk prediction in cirrhotic patients. World J Gastroenterol. 2025;31(11):101804. doi:10.3748/wjg.v31.i11.101804
30. Lin LY, Zeng DW, Liu YR, Zhu YY, Huang LL. Diagnostic value of liver stiffness measurement combined with risk scores for esophagogastric variceal bleeding in patients with hepatitis B cirrhosis. Eur J Radiol. 2024;173:111385. doi:10.1016/j.ejrad.2024.111385
31. Liang LX, Liang X, Zeng Y, Wang F, Yu XK. Establishment and validation of a nomogram for predicting esophagogastric variceal bleeding in patients with liver cirrhosis. World J Gastroenterol. 2025;31(9):102714. doi:10.3748/wjg.v31.i9.102714
32. Yokoyama S, Honda T, Ishizu Y, et al. Predicting early rebleeding and mortality after endoscopic hemostasis of esophagogastric varices: diagnostic performance of aspartate aminotransferase‐to‐platelet ratio index and model for end‐stage liver disease‐Na score - Yokoyama – 2024. J Hepato-Biliary-Pancreatic Sci. 2025;31(11):830–9. doi:10.1002/jhbp.12057.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.