")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 14
Clinical Utility of Urinary Biomarkers for Prediction of Acute Kidney Injury and Chronic Renal Dysfunction After Open Abdominal Aortic Aneurysm Repair
Authors Obata Y, Kamijo-Ikemori A, Inoue S
Received 1 June 2021
Accepted for publication 3 September 2021
Published 17 September 2021 Volume 2021:14 Pages 371—384
DOI https://doi.org/10.2147/IJNRD.S322916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Yumi Obata,1 Atsuko Kamijo-Ikemori,2 Soichiro Inoue1
1Department of Anesthesiology, St. Marianna University School of Medicine, Kawasaki, Kanagawa, Japan; 2Department of Anatomy, St. Marianna University School of Medicine, Kawasaki, Kanagawa, Japan
Correspondence: Yumi Obata Email [email protected]
Purpose: We examined the clinical utility of perioperative monitoring of urinary liver-type fatty acid binding protein (L-FABP), neutrophil gelatinase-associated lipocalin (NGAL), and albumin, for prediction of acute kidney injury (AKI) and prediction of chronic renal dysfunction in patients undergoing open surgical repair (OSR) of an abdominal aortic aneurysm.
Patients and Methods: Urine and serum samples were obtained perioperatively from 64 such patients (n=64). Patients in whom OSR-related AKI (defined by the Kidney Disease Improving Global Outcomes criteria) occurred were identified. Renal function was evaluated 3 years after OSR in patients with OSR-related AKI.
Results: The urinary biomarkers examined increased to maximum levels by 2 hours after aortic cross-clamping (AXC), regardless of whether AKI occurred. Notably, the serum creatinine (Cr) levels increased significantly immediately after OSR in patients with AKI (n=19) (vs that in patients without AKI). In patients with AKI, the increased serum Cr elevation rate, the urinary L-FABP levels 2 hours after AXC and immediately after OSR, and a reduction in eGFR documented 3 years after OSR were significantly greater in patients who underwent suprarenal AXC (n=11) than in those who underwent infrarenal AXC (n=8). Furthermore, urinary L-FABP levels 2 hours after AXC correlated significantly with the reductions in eGFR 3 years after OSR in patients with AKI.
Conclusion: Urinary L-FABP, NGAL and albumin concentrations 2 hours after AXC may be useful for early detection of OSR-related AKI. Furthermore, the increase in urinary L-FABP 2 hours after AXC may be predictive of chronic renal dysfunction in patients with OSR-related AKI.
Keywords: urinary liver-type fatty acid binding protein, L-FABP, urinary neutrophil gelatinase-associated lipocalin, NGAL, acute kidney injury, AKI, chronic renal dysfunction, open abdominal aortic aneurysm repair
Introduction
Patients diagnosed with abdominal aortic aneurysm (AAA) are increasing in number due to the growing aging population and to the sensitivity of various imaging modalities for early detection of the disorder. There are two surgical approaches to AAA, endovascular aneurysm repair (EVAR) and open surgical repair (OSR). EVAR, a minimally invasive procedure, had, for a time, taken precedence over OSR for treatment of infrarenal AAA. However, two recent long-term randomized controlled studies revealed that EVAR, in comparison to OSR, provided no long-term survival benefit.1,2 Therefore, OSR continues as the standard approach to AAA, even infrarenal AAA. Unfortunately, the relatively high incidence of acute kidney injury (AKI) associated with OSR remains a crucial problem,3 and suprarenal aortic cross-clamping (AXC) is reported to be a significant independent risk factor for occurrence of AKI.4
AKI was once considered transient and reversible and assumed to have a good renal prognosis. However, even slight renal dysfunction is now widely understood to be related not only to subsequent chronic kidney disease (CKD)5 and end-stage renal disease6 but also to all-cause mortality and morbidity.4,7 No radical treatment for AKI exists, making early discrimination of patients at increased risk for AKI necessary so that steps can be taken to minimize the chance that AKI will occur.8 Reliable biomarker for early detection of OSR-related AKI and for prediction of chronic renal dysfunction after OSR is needed.
Urinary liver-type fatty acid binding protein (L-FABP) has been identified as an excellent biomarker for tubular damage associated with AKI and with CKD,9,10 and it has since been approved as such by the Ministry of Health, Labour and Welfare in Japan. We have shown urinary L-FABP to be a sensitive biomarker for early detection of AKI after OSR, in that urinary L-FABP elevation occurs before serum creatinine (Cr) elevation.11 Another urinary biomarker, neutrophil gelatinase-associated lipocalin (NGAL), has been reported to predict occurrence of AKI after OSR performed for infrarenal AAA,12 but there has been at least one contradictory report regarding the clinical usefulness of urinary NGAL.13 Furthermore, changes in the level of each urinary biomarker, depending on whether AXC is suprarenal or infrarenal, and relations between increases in urinary biomarker levels in the acute phase and chronic renal dysfunction have not been adequately investigated.
We conducted a study to determine the clinical utility of measuring urinary biomarkers L-FABP, NGAL, and albumin for early detection of OSR-related AKI. We also aimed to show changes in urinary biomarker levels with respect to suprarenal AXC vs infrarenal AXC. Further, we aimed to clarify the relations between acute-phase increases in urinary marker levels and chronic renal dysfunction in patients who suffer OSR-related AKI.
Methods
The study protocol was approved by the Institutional Review Board of St. Marianna University School of Medicine (No 1966, No 4107) and registered in the UMIN Clinical Data Registry (ID 000006584, 000026215). Written informed consent was obtained from all patients who were enrolled in the study. This study was conducted in accordance with the Declaration of Helsinki.
Study Design
The study was conducted prospectively in a university hospital setting. Consecutive patients scheduled for OSR (n=64) between October 2011 and May 2017 were enrolled. Excluded from the study were patients undergoing dialysis or requiring emergency surgery. AKI was defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria and based on the increase in serum Cr over the 48 hours immediately following OSR.14 In addition, patients in whom OSR-related AKI occurred were examined for chronic renal dysfunction at the 3-year mark after OSR.
Anesthesia
None of the patients undergoing OSR was premedicated. All patients received epidural anesthesia before the surgery. An epidural catheter was inserted via the Th9/10, Th10/11, or Th11/12 intervertebral space. General anesthesia was induced with remifentanil and propofol. Tracheal intubation was facilitated with rocuronium. Anesthesia was maintained with sevoflurane in an oxygen-air mixture and remifentanil. Levobupivacaine (0.125% or 0.25%) was administered intraoperatively via epidural catheter. Dopamine, prostaglandin E1, and carperitide were infused continuously during the surgery in all patients.
Sample Collection
Urine samples (10 mL) were obtained before the surgery, after anesthesia induction, 2 hours after AXC, immediately after the surgery, 4 hours after the surgery, and on postoperative day (POD) 2 for measurement of urinary L-FABP, urinary NGAL, urinary albumin, and urinary Cr. In addition, serum samples were obtained before the surgery, immediately after the surgery, and on PODs 1, 2, and 3 for measurement of serum Cr. Furthermore, serum Cr was evaluated for estimation of the glomerular filtration rate (eGFR) 3 years after OSR in patients in whom AKI occurred.
Assay of Urinary and Serum Markers
Urinary L-FABP levels were determined by enzyme-linked immunosorbent assay (ELISA) (Human L-FABP ELISA kit; CMIC, Tokyo, Japan). Urinary NGAL levels were also determined by ELISA (Human NGAL ELISA kit; Enzo Life Sciences, Inc, NY, USA). Urinary albumin was measured by immunonephelometry, and serum Cr was measured by an enzymatic method. All assays were performed in the clinical laboratory of St. Marianna University Hospital. eGFR was calculated according to the Japanese-coefficient of the modified Chronic Kidney Disease Epidemiology Collaboration equation: eGFR = 194 × (creatinine)−1.094 × (age)−0.287 × (0.739 if female).15
Measurement of Urinary Markers and the Rate of Increase in Serum Cr with Respect to Suprarenal AXC or Infrarenal AXC in Patients in Whom AKI Occurred
Urinary markers were monitored in all patients for 2 days after OSR. Patients were then divided between those in whom AKI occurred and those in whom AKI did not occur, and the AKI group patients were divided between those who underwent suprarenal AXC and those who underwent infrarenal AXC. The rate of increase in serum Cr was measured in these two AKI patient subgroups as follows:
Serum Cr elevation rate = [(highest serum Cr level observed during the 2 days after OSR) – (serum Cr levels before OSR)]/(time from the start of OSR to time of the peak serum Cr) and reported as mg/dl/hour.
Change in eGFR in the Chronic Phase in the AKI Group Patients
Progression to chronic renal dysfunction was evaluated in AKI group patients, particularly with respect to whether they underwent suprarenal AXC or infrarenal AXC. Chronic renal dysfunction was assessed at 3 years after OSR on the basis of change in eGFR from before the surgery to 3 years after the surgery.
Evaluation of the Urinary L-FABP Levels 2 Hours After AXC in Relation to Change in eGFR in the AKI Group Patients
For patients in whom OSR-related AKI occurred, correlation between the urinary L-FABP concentration 2 hours after AXC and change in eGFR documented at 3 years was assessed.
Statistical Analyses
Study variables are expressed as median (interquartile range [IQR]) values. Between-group differences in study variables, including patients’ clinical characteristics, were analyzed by Mann–Whitney U-test or chi-square test, as appropriate. Within-group differences were analyzed by Wilcoxon signed-rank test. Kruskal–Wallis test, followed by Steel test, was used for logistic regression analysis and was performed on parameters that had a significant difference in univariate regression analysis to determine the independent factors associated with AKI. Model calibration was tested using the Hosmer-Lemeshow test. Correlation was established on the basis of Spearman’s rank correlation coefficient. Receiver-operating characteristic curves (ROCs) were plotted to identify cut-off biomarker levels best predictive of the occurrence of OSR-associated AKI. Clinical variables shown by unadjusted univariate analysis to differ significantly between the AKI group and non-AKI group were subjected to forward selection multivariable logistic regression analysis to identify risk factors for occurrence of AKI.
All statistical analyses were performed with IBM SPSS Statistics, version 21.0 (IBM, Tokyo, Japan), and p < 0.05 was considered significant.
Results
Characteristics of Patients in Whom AKI Occurred
As noted above, AKI occurred postoperatively in 19 (29.7%) of the 64 patients enrolled in the study, and the AKI was determined to be of stage 1, which was defined as more than 0.3 mg/dl increase in serum Cr within 48 hrs, in all 19 patients (Table 1). No patient required postoperative renal replacement therapy.
 |
Table 1 Patient Characteristics and Clinical Outcomes in AKI Vs Non-AKI Group |
Male sex was more prevalent (p < 0.001), age was greater (p < 0.001), suprarenal AXC was more prevalent (p < 0.001), presence of diabetes mellitus was more prevalent (p = 0.012), presence of ischemic heart disease was more prevalent (p = 0.027), operation time was longer (p = 0.017), urinary output was lower (p = 0.024), and the preoperative urinary albumin concentration was higher (p = 0.022) in the AKI group than in the non-AKI group (Table 1).
Postoperative Changes in Renal Function and Urinary Biomarkers
In assessing urinary L-FABP levels (Figure 1), we found that the concentration in the AKI group increased significantly from the preoperative value to its maximum value, which was reached 2 hours after AXC (p < 0.001). Despite subsequent decreases in the urinary L-FABP levels in this group, the levels 4 hours after the surgery and on POD 2 were significantly higher than the preoperative concentration. We found the urinary L-FABP concentration in the non-AKI group to be significantly increased 4 hours after the surgery. The urinary L-FABP levels in the AKI group were significantly higher than those in the non-AKI group 2 hours after AXC, immediately after the surgery, 4 hours after the surgery, and on POD 2 (p < 0.001, <0.001, <0.001, and <0.001, respectively).
 |
Figure 1 Box and whisker plot showing urinary L-FABP (liver-type fatty acid-binding protein), urinary NGAL (neutrophil gelatinase-associated lipocalin), urinary albumin, and serum Cr (creatinine) levels measured pre-operation, post anesthesia induction, 2 hours after AXC, immediately after the surgery, 4 hours after the surgery, and on POD 2 in the AKI and non-AKI patient groups. Median and interquartile range values are shown. *p < 0.05 vs the level in the non-AKI group at the same time point; †p < 0.05 vs the respective preoperative level in the same (AKI) group; ‡p < 0.05 vs the respective preoperative level in the same (non-AKI) group. Abbreviations: AKI, acute kidney injury; Pre-op, preoperative value; Post-induction, post-anesthesia induction value; 2-h post-AXC, 2 hours post aortic cross clamping value; Post-op, immediate postoperative value; 4-h post-op, 4 hours postoperative value; POD, postoperative day. |
In assessing urinary NGAL levels (Figure 1), we found no significant increase over the preoperative levels at any time point in either the AKI group or the non-AKI group. However, urinary NGAL levels were significantly higher from 2 hours after AXC to POD 2 in the AKI group than in the non-AKI group (Figure 1).
With respect to urinary albumin (Figure 1), we found no significant increase in the concentration at any time point in the AKI group, but the concentration was significantly higher in the AKI group than in the non-AKI group before the surgery (p = 0.002), after anesthesia induction (p = 0.003), 2 hours after AXC (p < 0.001), immediately after the surgery (p = 0.009), 4 hours after the surgery (p < 0.001), and on POD 2 (p < 0.001). In the non-AKI group, the urinary albumin levels 2 hours after AXC were significantly higher than the preoperative concentration.
In assessing serum Cr levels (Figure 1), we found no significant within-group difference between levels measured at the various time points in the AKI group patients. However, in comparing serum Cr levels between the AKI group and non-AKI group patients, we found the concentration in the AKI group to be significantly higher immediately after the surgery and on PODs 1, 2, and 3 than the concentration on each of those same days in the non-AKI group (p < 0.001, <0.001, <0.001, and <0.001, respectively).
Performance of the Urinary Markers for Predicting Occurrence of AKI
ROC analysis (Table 2) showed urinary L-FABP measured at either of two time points to be predictive of the occurrence of AKI (AUC > 0.80): measurement at 2 hours after AXC (AUC = 0.82) and at 4 hours after the surgery (AUC = 0.81). Urinary NGAL measured at one time point was shown to be predictive of the occurrence of AKI: measurement at 2 hours after AXC (AUC = 0.83). Urinary albumin measured at either of two time points was shown to be predictive of the occurrence of AKI: measurement at 2 hours after AXC (AUC = 0.81) and on POD 2 (AUC = 0.81).
 |
Table 2 AUC Vs Time |
Cut-off Urinary Marker Values for Predicting Occurrence of AKI
In seeking to determine the best cut-off values for each of the three biomarkers found to be predictive of the occurrence of AKI, we determined sensitivity, specificity, positive predictive value, and negative predictive value of levels measured at each of the five time points noted above (Table 3). Levels of urinary L-FABP, urinary NGAL, and urinary albumin measured 2 hours after AXC were found to have the best predictive values, at cut-off points of 150.5 μg/g Cr, 48.7 mg/g Cr, and 607.2 mg/g Cr, respectively.
 |
Table 3 Biomarkers Levels Predictive of AKI |
Multivariable Logistic Regression Analysis for Prediction of AKI
Multivariable logistic regression analysis of factors associated with occurrence of AKI, ie, the 2-hour post-AXC increases in urinary L-FABP, urinary NGAL, and urinary albumin, were shown to be independently predictive of postoperative AKI (OR: 1.0001, CI: 10,001–1001, p = 0.006; OR: 1.00001, CI: 1.00001–1.00002, p = 0.004; OR: 1.001, CI: 1.00001–1.001, p = 0.014, respectively). Age, suprarenal (vs infrarenal) AXC, presence of diabetes mellitus or ischemic heart disease, operation time, and low urinary output were also shown to be independently predictive of postoperative AKI. Notably, the odds associated with suprarenal AXC was shown to be much greater than the odds associated with the other variables analyzed.
Urinary Markers and Renal Dysfunction with Respect to Suprarenal vs Infrarenal AXC in AKI Group Patients
Because suprarenal AXC was shown to be an independent risk factor for occurrence of AKI, changes in urinary markers and renal function were evaluated in the AKI group patients in relation to suprarenal vs infrarenal AXC. Of the 19 patients with postoperative AKI, 11 (64.7%) underwent suprarenal AXC, and 8 (17.0%) underwent infrarenal AXC. AXC time (p = 0.049) and the serum Cr elevation rate were significantly greater among patients who underwent suprarenal AXC than among those who underwent infrarenal AXC (p = 0.005) (Table 4 and Figure 2).
 |
Table 4 Patient Characteristics and Clinical Outcomes in Suprarenal Vs Infrarenal AKI Group |
 |
Figure 2 Box and whisker plot showing the serum Cr elevation rate for AKI group patients who underwent suprarenal AXC and those who underwent infrarenal AXC. Median and interquartile range values are shown. *p < 0.05 vs the infrarenal group. Abbreviations: AKI, acute kidney injury; AXC, aortic cross-clamping; Cr, creatinine. |
Urinary L-FABP increased to its maximum value by 2 hours after AXC in the AKI group patients, regardless of whether they underwent suprarenal or infrarenal AXC. The urinary L-FABP levels were significantly increased 2 hours after AXC and on POD 2 among the AKI patients who underwent suprarenal AXC, but there was no significant change in urinary L-FABP among the AKI group patients who underwent infrarenal AXC. Further, in the AKI group patients who underwent suprarenal AXC, the urinary L-FABP levels 2 hours after AXC (5710 [1890–9090] μg/gCr), immediately after the surgery (1020 [213–1810] μg/gCr), 4 hours after the surgery (233 [209–568] μg/gCr)), and on POD 2 (72 [52–134] μg/gCr) were significantly higher than corresponding values in AKI group patients who underwent infrarenal AXC (163 [8.0–1350] μg/gCr, 55 [23–300] μg/gCr, 75 [41–452] μg/gCr, and 27 [19–68] μg/gCr, respectively) (p = 0.001, p = 0.01, p = 0.025, and p= 0.043, respectively) (Figure 3) although the urinary L-FABP levels were significantly lower after anesthesia induction in patients who underwent suprarenal AXC than in those who underwent infrarenal AXC (5.1 [4.1–9.0] μg/gCr vs.12 [9–74] μg/gCr, respectively; p = 0.039) (Figure 3).
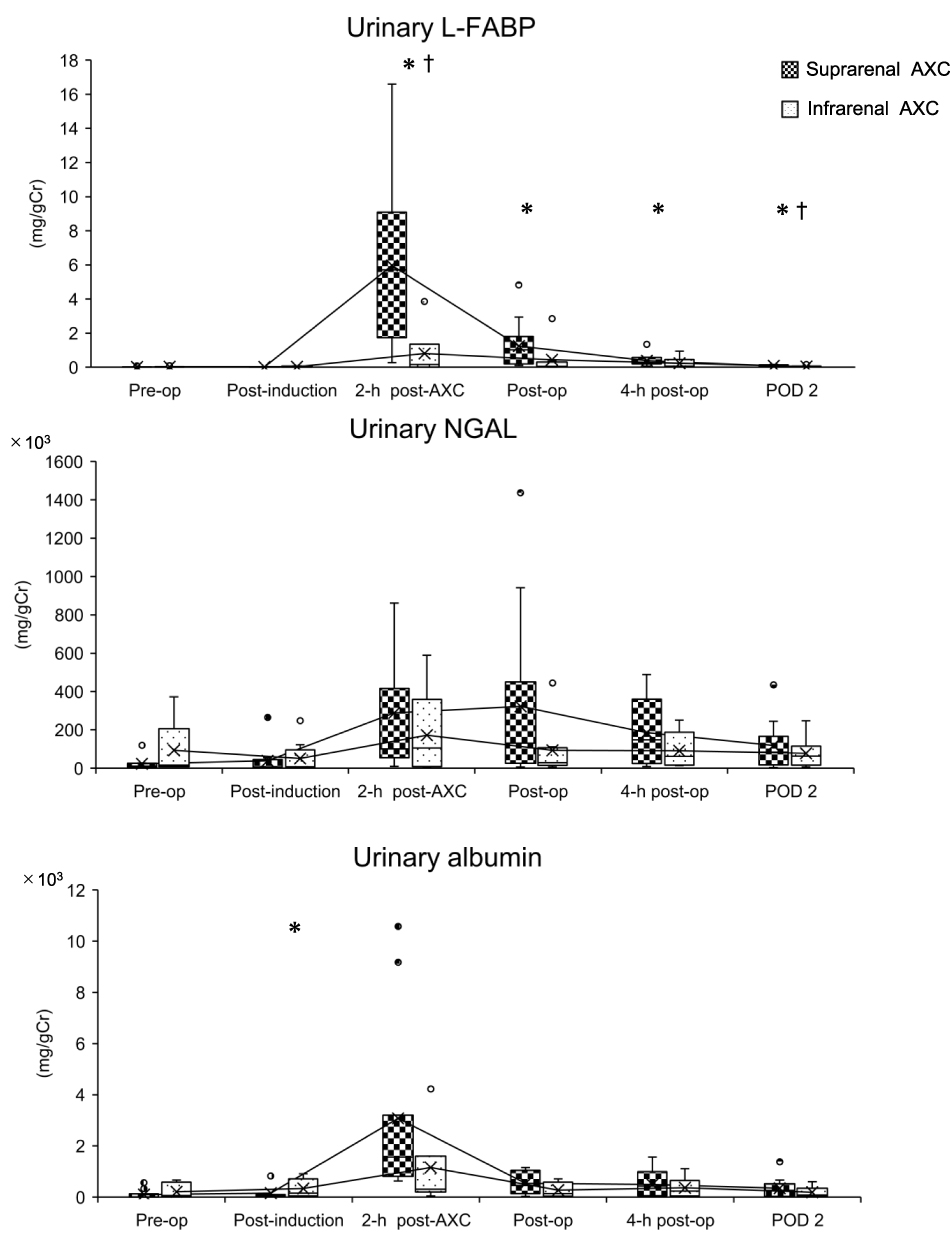 |
Figure 3 Box and whisker plots showing urinary L-FABP (liver-type fatty acid-binding protein), urinary NGAL (neutrophil gelatinase-associated lipocalin), and urinary albumin levels measured pre-operation, post anesthesia induction, 2 hours after AXC, immediately after the surgery, 4 hours after the surgery, and on POD 2 in the AKI group patients who underwent suprarenal AXC and in those who underwent infrarenal AXC. Median and interquartile range values are shown. *p < 0.05 vs the infrarenal AXC group at the same time point; †p < 0.05 vs the preoperative concentration in the same (suprarenal AXC) group. Abbreviations: Pre-op, preoperative value; Post-induction, value post anesthesia induction; 2-h post-AXC, value 2 hours after aorta cross clamping; Post-op, immediate postoperative value; 4-h post-op, 4 hours postoperative value; AKI, acute kidney injury; AXC, aortic cross-clamping; POD, postoperative day. |
Whereas urinary NGAL increased to its maximum value immediately after the surgery (131.0 [26.3–450.1] mg/gCr) among the AKI group patients who underwent suprarenal AXC, none of the measured urinary NGAL levels differed significantly between AKI group patients who underwent suprarenal AXC and those who underwent infrarenal AXC (Figure 3).
The maximum urinary albumin levels, reached by 2 hours after AXC in the AKI group patients, did not differ significantly between those who underwent suprarenal AXC and those who underwent infrarenal AXC (1570 [946.6–3205] mg/gCr vs 310.4 [205.3–1605] mg/gCr, respectively). The urinary albumin concentration after anesthesia induction, however, was significantly lower in patients who underwent suprarenal AXC than in those who underwent infrarenal AXC (53 [12–103] mg/gCr vs 153 [62–709] mg/gCr, respectively; p = 0.046) (Figure 3).
Cut-off Urinary L-FABP Values for Prediction of AKI in Patients Having Undergone Suprarenal vs Infrarenal AXC
Cut-off values for urinary L-FABP 2 hours after AXC predicting occurrence of AKI differed, depending on whether suprarenal AXC (1306.0 μg/gCr, AUC = 0.709) or infrarenal AXC (150.5 μg/gCr, AUC = 0.740) was performed (Table 5). The cut-off urinary L-FABP concentration 2 hours after AXC showed high sensitivity for prediction of AKI in patients who underwent suprarenal AXC and high specificity for prediction of AKI in those who underwent infrarenal AXC (Table 5).
 |
Table 5 Urinary L-FABP Levels at 2 Hours Post-AXC for Prediction of AKI |
Change in eGFR in AKI Group Patients Who Underwent Suprarenal AXC and Those Who Underwent and Infrarenal AXC
Whereas GFR levels 3 years after OSR were similar between patients who underwent suprarenal AXC (41.5 [32.1–56.5] mL/min) and those who underwent infrarenal AXC (32.4 [22.5–69.0] mL/min) (Table 4), a significant decrease in eGFR from before OSR to 3 years after OSR was observed in patients who underwent suprarenal ACX (p = 0.014) (Table 4 and Figure 4A) but not in those who underwent infrarenal AXC (p = 0.120) (Table 4 and Figure 4B).
 |
Figure 4 (A and B) Box and whisker plots showing eGFR before the surgery and 3 years after the surgery in AKI group patients who underwent suprarenal AXC and those who underwent infrarenal AXC. Median and interquartile range values are shown. (C) Regression line showing correlation between changes in eGFR and urinary L-FABP (liver-type fatty acid-binding protein) levels measured 2 hours after AXC. *p < 0.05 vs the preoperative value. Abbreviations: eGFR, estimated glomerular filtration rate; AKI, acute kidney injury; AXC, aortic cross-clamping. |
Correlation Between Urinary L-FABP Levels 2 Hours After AXC and Change in eGFR in AKI Group Patients
Significant correlation was found between urinary L-FABP levels 2 hours after AXC and changes in eGFR documented 3 years after OSR (Rs =−0.720, p = 0.001) (Figure 4C).
Discussion
In summary, our main study findings were as follows: (1) Although the serum Cr concentration immediately after OSR was significantly higher in patients in whom AKI occurred than in patients in whom AKI did not occur, the urinary L-FABP, NGAL, and albumin concentrations reached maximum values before the notable serum Cr elevation was detected. (2) Although suprarenal AXC, but not urinary markers, was identified as an independent risk factor for occurrence of AKI, the serum Cr elevation rate was greater for patients who underwent suprarenal AXC than for those who underwent infrarenal AXC. (3) Urinary L-FABP levels, but not concentrations of other urinary markers, were found to be significantly higher at various time points in the AKI group patients who underwent suprarenal AXC than in those who underwent infrarenal AXC. (4) Urinary L-FABP cut-off values 2 hours after AXC for early detection of OSR-related AKI were found to differ, depending on whether suprarenal or infrarenal AXC was performed. (5) Reduction in the eGFR 3 years after OSR was greater for AKI group patients who underwent suprarenal AXC than for those who underwent infrarenal AXC, and urinary L-FABP levels 2 hours after AXC correlated significantly with the eGFR reductions.
Our study results indicate that urinary L-FABP, NGAL and albumin levels 2 hours after AXC may be useful for early detection of OSR-related AKI and that the urinary L-FABP concentration 2 hours after AXC may need to be assessed in consideration of whether the AXC is suprarenal or infrarenal. Further, the urinary L-FABP concentration 2 hours after AXC may be predictive of chronic renal dysfunction in patients with OSR-related AKI.
We reported previously that the post-OSR increases in urinary L-FABP and albumin occur before the increase in serum Cr,11 and this timing was confirmed in the present study. Furthermore, early urinary NGAL elevation was shown. Because the levels of both urinary L-FABP and NGAL 2 hours after AXC were significantly higher in the AKI group patients than in the non-AKI group patients, measuring these markers at 2 hours after AXC may be meaningful for early prediction of AKI. Regarding urinary albumin, the increased values were seen significantly earlier, before the surgery and after anesthesia induction, in the AKI group patients than in the non-AKI group patients. However, because the urinary albumin AUCs for predicting occurrence of AKI at these time points were smaller than at other time points, measurement of urinary albumin 2 hours after AXC may be of the best predictive value.
Renal hypoperfusion induced during OSR is widely known as a major cause of AKI16,17 and AKI appears to occur more often in association with suprarenal AXC than in association with infrarenal AXC,4,17 a finding supported by the present study. Furthermore, AKI can lead to chronic renal dysfunction.18,19 Although neither severe AKI nor death occurred in any of our patients, and preoperative renal function was similar between those who underwent suprarenal AXC and those who underwent infrarenal AXC, deterioration of renal function in both the acute and chronic phase was significantly greater in patients who underwent suprarenal AXC than in those who underwent infrarenal AXC. In addition, suprarenal AXC was found to be a significant, independent risk factor for occurrence of AKI. Renal ischemia time and intraoperative blood loss have been reported to be associated with OSR-related AKI when the surgery involves suprarenal AXC,17 and the severity of acute renal dysfunction affects the degree of chronic renal dysfunction.18,19 Although the estimated blood loss volume was similar between our patients who underwent infrarenal AXC and those who underwent suprarenal, the longer clamp time required for suprarenal AXC may explain, at least in part, the frequent occurrence of AKI and the deterioration in renal function.
Urinary L-FABP, unlike other biomarkers examined, may reflect renal hypoperfusion.20,21 Performance of urinary L-FABP and that of NGAL are reportedly dissimilar, with urinary L-FABP correlating linearly with hypoperfusion and hepatic injury markers (lactate, liver transaminases, and bilirubin) urinary NGAL correlating linearly with inflammatory markers (white blood cell count and C-reactive protein).22 The difference in changes in urinary L-FABP associated with suprarenal vs infrarenal AXC and that influence the degree of renal hypoperfusion and both acute and chronic renal function suggests that urinary L-FABP has potential to accurately reflect the degree of renal hypoxia due to OSR.
Use of sevoflurane, remifentanil, and levobupivacaine (administered epidurally) might have influenced our patients’ renal hemodynamics. Although Peyton et al reported no significant relation between epidural anesthesia and renal complications following major abdominal surgery,23 we found significant differences in urinary albumin and L-FABP levels after anesthesia induction between our AKI patients and non-AKI group patients and with respect to suprarenal AXC vs infrarenal AXC in the AKI group. Therefore, further study is needed to clarify the effects of various anesthesia protocols on urinary markers.
Our study results should be considered in light of our study limitations. First is the fact that the study was carried out at a single center and did not include a large number of patients. Slight serum Cr elevation of in the AKI group patients who underwent infrarenal AXC was not related to chronic renal dysfunction for a relatively short duration, 3 years after OSR. Second, the AKI was mild, and the relation between urinary markers and the severity of AKI defined by the KDIGO criteria was not assessed. In addition, no patient required renal replacement therapy and none died during the chronic period after OSR, and therefore, the usefulness of urinary L-FABP for predicting hard end points of CKD after OSR was not clarified. Finally, use of various vasoactive drugs during OSR was not controlled for. Renal function in the chronic phase was evaluated at only one time point, ie, at 3 years after OSR, and urinary biomarkers were not measured during the chronic phase. Further, neither blood pressure nor blood glucose nor medical treatment was documented in the chronic phase after AKI. These are related to renal protection. A large-scale long-term multicenter study that covers these matters is needed.
In conclusion, urinary L-FABP, NGAL and albumin levels 2 hours after AXC may be useful for early detection of OSR-related AKI. Because the increase in urinary L-FABP may vary in response to suprarenal vs infrarenal AXC but is a critical factor strongly related to renal hypoperfusion leading to renal dysfunction, urinary L-FABP should be evaluated in light of the clamp site. Furthermore, urinary L-FABP elevation documented 2 hours after AXC may be predictive of chronic renal dysfunction in patients who suffer OSR-related AKI.
Acknowledgments
We thank Prof. Takeshi Tateda and Dr. Kiyoshi Chiba for his help in conducting the study. We thank Prof. Tina Tajima for her help in reviewing and editing the manuscript, and we also thank Ms. Sachi Shinmi for her technical assistance. In addition, we thank Dr. Yasushi Masumori, Dr. Hiroyuki Kobayashi, Dr. Atsuko Kato, Dr. Eriko Amano, and Dr. Kosuke Hamabe for the sample collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lederle FA, Freischlag JA, Kyriakides TC, et al. Group OVACS: long-term comparison of endovascular and open repair of abdominal aortic aneurysm. N Engl J Med. 2012;367(21):1988–1997. doi:10.1056/NEJMoa1207481
2. Patel R, Sweeting MJ, Powell JT, Greenhalgh RM. investigators Et: endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomised controlled trial. Lancet. 2016;388(10058):2366–2374. doi:10.1016/S0140-6736(16)31135-7
3. Tang Y, Chen J, Huang K, et al. The incidence, risk factors and in-hospital mortality of acute kidney injury in patients after abdominal aortic aneurysm repair surgery. BMC Nephrol. 2017;18(1):184. doi:10.1186/s12882-017-0594-6
4. Patel VI, Lancaster RT, Ergul E, et al. Postoperative renal dysfunction independently predicts late mortality in patients undergoing aortic reconstruction. J Vasc Surg. 2015;62(6):1405–1412. doi:10.1016/j.jvs.2015.07.084
5. Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int. 2012;81(5):442–448. doi:10.1038/ki.2011.379
6. Chawla LS, Amdur RL, Shaw AD, Faselis C, Palant CE, Kimmel PL. Association between AKI and long-term renal and cardiovascular outcomes in United States veterans. Clin J Am Soc Nephrol. 2014;9(3):448–456. doi:10.2215/CJN.02440213
7. Nathan DP, Brinster CJ, Jackson BM, et al. Predictors of decreased short- and long-term survival following open abdominal aortic aneurysm repair. J Vas Surg. 2011;54(5):1237–1243. doi:10.1016/j.jvs.2011.05.028
8. Nadim MK, Forni LG, Bihorac A, et al. Cardiac and vascular surgery-associated acute kidney injury: the 20th international consensus conference of the ADQI (Acute Disease Quality Initiative) group. J Am Heart Assoc. 2018;7(11):e008834. doi:10.1161/JAHA.118.008834
9. Matsui K, Kamijo-Ikemori A, Imai N, et al. Clinical significance of urinary liver-type fatty acid-binding protein as a predictor of ESRD and CVD in patients with CKD. Clin Exp Nephrol. 2016;20(2):195–203. doi:10.1007/s10157-015-1144-9
10. Matsui K, Kamijo-Ikemori A, Sugaya T, Yasuda T, Kimura K. Usefulness of urinary biomarkers in early detection of acute kidney injury after cardiac surgery in adults. Circ J. 2012;76(1):213–220. doi:10.1253/circj.CJ-11-0342
11. Obata Y, Kamijo-Ikemori A, Ichikawa D, et al. Clinical usefulness of urinary liver-type fatty-acid-binding protein as a perioperative marker of acute kidney injury in patients undergoing endovascular or open-abdominal aortic aneurysm repair. J Anesth. 2016;30(1):89–99. doi:10.1007/s00540-015-2095-8
12. Brinkman R, HayGlass KT, Mutch WA, Funk DJ. Acute kidney injury in patients undergoing open abdominal aortic aneurysm repair: a pilot observational trial. J Cardiothorac Vasc Anesth. 2015;29(5):1212–1219. doi:10.1053/j.jvca.2015.03.027
13. Rampoldi B, Tessarolo S, Giubbilini P, et al. Neutrophil gelatinase-associated lipocalin and acute kidney injury in endovascular aneurysm repair or open aortic repair: a pilot study. Biochem Med. 2018;28(1):010904. doi:10.11613/BM.2018.010904
14. Kellum JA, Lameire N, Aspelin P, et al. Kidney disease: improving global outcomes (KDIGO) practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
15. Matsuo S, Imai E, Horio M, et al. Collaborators developing the Japanese equation for estimated GFR: revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982–992. doi:10.1053/j.ajkd.2008.12.034
16. Wahlberg E, Dimuzio PJ, Stoney RJ. Aortic clamping during elective operations for infrarenal disease: the influence of clamping time on renal function. J Vas Surg. 2002;36(1):13–18. doi:10.1067/mva.2002.123679
17. Yokoyama N, Nonaka T, Kimura N, et al. Acute kidney injury following elective open aortic repair with suprarenal clamping. Ann Vasc Dis. 2020;13(1):45–51. doi:10.3400/avd.oa.19-00095
18. Tanabe J, Ogura Y, Nakabayashi M, et al. The possibility of urinary liver-type fatty acid-binding protein as a biomarker of renal hypoxia in spontaneously diabetic torii fatty rats. Kidney Blood Press Res. 2019;44(6):1476–1492. doi:10.1159/000503926
19. Yamamoto T, Noiri E, Ono Y, et al. Renal L-type fatty acid-binding protein in acute ischemic injury. J Am Soc Nephrol. 2007;18(11):2894–2902. doi:10.1681/ASN.2007010097
20. Asada T, Isshiki R, Hayase N, et al. Impact of clinical context on acute kidney injury biomarker performances: differences between neutrophil gelatinase-associated lipocalin and L-type fatty acid-binding protein. Sci Rep. 2016;6(1):33077. doi:10.1038/srep33077
21. Ishani A, Nelson D, Clothier B, et al. The magnitude of acute serum creatinine increase after cardiac surgery and the risk of chronic kidney disease, progression of kidney disease, and death. Arch Intern Med. 2011;171(3):226–233. doi:10.1001/archinternmed.2010.514
22. Lassnigg A, Schmidlin D, Mouhieddine M, et al. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15(6):1597–1605. doi:10.1097/01.ASN.0000130340.93930.DD
23. Peyton PJ, Myles PS, Silbert BS, Rigg JA, Jamrozik K, Parsons R. Perioperative epidural analgesia and outcome after major abdominal surgery in high-risk patients. Anesth Analg. 2003;96(2):548–554. doi:10.1213/00000539-200302000-00046
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.