")
Back to Journals » Clinical Interventions in Aging » Volume 13
Clinical utility of the revised cardiac risk index in older Chinese patients with known coronary artery disease
Authors Che L , Xu L, Huang YG, Yu CH
Received 25 June 2017
Accepted for publication 30 October 2017
Published 22 December 2017 Volume 2018:13 Pages 35—41
DOI https://doi.org/10.2147/CIA.S144832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Lu Che, Li Xu, Yuguang Huang, Chunhua Yu
Department of Anesthesiology, Peking Union Medical College Hospital, Beijing, China
Objectives: The revised Cardiac Risk Index (RCRI) is the most widely used risk prediction tool for postoperative cardiac adverse events. We aim to explore the predictive ability of the RCRI in older Chinese patients with coronary artery disease (CAD) undergoing noncardiac surgery, which has not been previously evaluated.
Methods: We performed a multicenter, prospective study. We enrolled a total of 1,202 patients, aged >60 years, with a history of CAD who underwent noncardiac surgery. Perioperative data were extracted from an electronic database. The primary end point was defined as an occurrence of a postoperative major cardiac event (PoMCE) within 30 days. Logistic regression analysis was performed to evaluate the performance of the RCRI. A modified RCRI was created and compared with the original RCRI with regard to its ability to predict postoperative cardiac events.
Results: Of the enrolled patients, 4.3% experienced PoMCE. Most components of the RCRI were not predictive of postoperative cardiac events with the exception of insulin-dependent diabetes mellitus (odds ratio =2.38, 95% CI: 1.11–5.11; P=0.03). The RCRI performed no better than chance (area under the curve =0.53; 95% CI: 0.45–0.61) in identifying patients’ cardiac risk. The modified score had a higher discriminatory ability toward PoMCE (c index, 0.69 versus 0.53; P<0.01).
Conclusion: The original RCRI shows poor predictive ability in Chinese patients with CAD undergoing noncardiac surgery.
Keywords: cardiovascular risk factors, older patient, coronary artery disease, risk prediction model
Introduction
Globally, more than 300 million people undergo noncardiac surgery every year. Cardiac complications occur after at least 2% of elective noncardiac procedures and account for one-third of postoperative deaths.1 Coronary artery disease (CAD) is a major health problem in China. Based on the data from the 2008 Fourth Family Health Survey, the overall prevalence of CAD was 7.7‰. This finding indicated that there were more than 10 million subjects with CAD in Mainland China in 2008.2 The prevalence of cardiovascular disease among the surgical population in China is expected to increase in the next decade. Therefore, effective preoperative risk stratification that implements readily available clinical information is required for prioritization of patients.
The revised cardiac risk index (RCRI), also known as the Lee index, was originally published in 1999, and has been used worldwide since this time.3 The 2014 American College of Cardiology and American Heart Association Guideline recommends estimating the perioperative risk of adverse cardiac events with the RCRI.4 However, the RCRI was originally developed for all patients undergoing major noncardiac surgery rather than cardiac patients. Furthermore, the medical treatment strategy toward CAD has greatly evolved since the development of the RCRI. The discriminatory ability of this index in modern patients with CAD may be compromised.
The goals of this study were 1) to validate the RCRI in a multicenter cohort of patients with CAD undergoing noncardiac surgery and 2) to determine whether modification of the current risk factors or adoption of other risk factors would improve upon discrimination of cardiac risk prediction compared with the original RCRI.
Materials and methods
Study population
We performed a multicenter, prospective study of consecutive patients who underwent noncardiac surgery between March 1, 2008, and February 28, 2010. We included patients from five university-affiliated tertiary care hospitals in China. The details of the original study have been described previously.5 The local medical ethics committee of Peking Union Medical College Hospital approved this study. The original inclusion criterion was patients with a history of CAD undergoing intermediate-to high-risk noncardiac surgery based on the American College of Cardiology/American Heart Association guidelines. Original exclusion criteria included the following: 1) patients who underwent emergency surgery or low-risk surgery, 2) patients with American Society of Anesthesiologists classification of V or VI, and 3) patients with congenital heart disease or cardiomyopathy. For the present study, we further excluded patients with incomplete data that were necessary to extrapolate the RCRI. The primary outcome measure was the occurrence of a postoperative major cardiac event (PoMCE) within 30 days. PoMCEs were defined as cardiac death, nonfatal myocardial infarction, nonfatal cardiac arrest, and heart failure. All possible clinically relevant preoperative and intraoperative factors were extracted from the database and analyzed.
Statistical analysis
De-identified data on demographics, preoperative risk factors, intraoperative variables, postoperative monitoring variables, and 30-day postoperative cardiac complications were retrieved from the database. The RCRI score was calculated for each patient in accordance with the original study. Each component of the RCRI was assigned a score of 0 or 1 (1= yes, 0= no). The six components of the RCRI were as follows: 1) history of ischemic heart disease, 2) history of congestive heart failure, 3) history of cerebrovascular disease (stroke or transient ischemic attack), 4) history of diabetes requiring preoperative insulin use, 5) chronic kidney disease (creatinine levels >2 mg/dL), and 6) undergoing suprainguinal vascular, intraperitoneal, or intrathoracic surgery. All data analyses were conducted independently by investigators who did not participate in the original study. Normally distributed continuous variables are expressed as mean ± SD and were compared using the two-tailed Student’s t-test. Categorical variables are expressed as frequency (%), and were compared using chi-square analysis. Univariate analyses were performed to select possible risk factors for major adverse cardiac event (MACE). Multivariate logistic regression analysis was used to evaluate the predictive ability of the original RCRI model. A modified RCRI (mRCRI) was established by incorporating easily accessible clinical data that can be obtained from the preoperative period. A forward stepwise logistic regression analysis was performed. Each variable was sequentially added to the original RCRI. Variables with a P-value <0.05 were maintained. The generated models were then compared using receiver operating characteristic (ROC) curves and area under the curve analysis. The parameters with optimal predictive scores and those that maintained the highest discriminative capacity of the new model were selected. A value of P<0.05 was considered as significant. Statistical analyses were performed using Stata/MP 14.0 version (StataCorp., College Station, TX, USA).
Results
Demographic data
From the original dataset of 1,422 patients, 220 were excluded because of incomplete data. Among the included 1,202 patients (age, 69.5±5.3 years), 52 (4.3%) patients experienced PoMCE (Table 1). Baseline information analysis showed that age (>70 years), female sex, body mass index (BMI) <18 kg/m2, insulin-dependent diabetes mellitus, creatinine levels, incidence of intraoperative hypotension, and a long operation time were different between patients who did and those who did not experience PoMCE (Table 2).
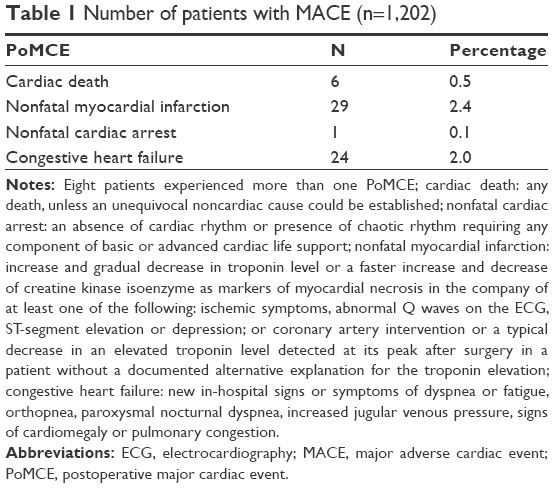 | Table 1 Number of patients with MACE (n=1,202) |
 | Table 2 Univariate analyses of preoperative risk factors of PoMCE |
Calculation of the RCRI
Rates of major cardiac adverse events with an RCRI <2 and ≥2 were 4.5% (n=314) and 4.2% (n=888), respectively (Table 3). The relationships of the six components included in the original RCRI model with PoMCE were evaluated by multivariate regression (Table 4). The modified model included six preoperative clinical factors, and each were allocated a score of 1 for the following: 1) history of myocardial infarction, 2) female sex, 3) insulin-dependent diabetes mellitus, 4) BMI <18 kg/m2, 5) age >70 years, and 6) atrial fibrillation. Another risk model involving a seventh intraoperative parameter (intraoperative hypotension) with a score of 1 was also investigated. Rates of PoMCE of different risk stratification methods are shown in Table 3. A high RCRI was not correlated with the incidence of PoMCE, while mRCRI and mRCRI+hypo were strongly correlated with the occurrence of PoMCE. An mRCRI ≥3 was associated with a tripled risk of PoMCE compared with an mRCRI <3 (odds ratio [OR] =3.10, 95% CI 1.64–5.90, P<0.01). Patients with an mRCRI+hypo ≥3 were 3.6 times more likely to develop PoMCE compared with patients with an mRCRI+hypo <3 (OR =3.63, 95% CI 2.06–6.41, P<0.01). ROC analysis was carried out for all three models. The RCRI had a poor discriminatory ability (ROC area 0.532, 95% CI 0.452–0.612), while the mRCRI showed significantly improved ability (ROC area 0.689, 95% CI 0.6210..757, P<0.05) to predict PoMCE within 30 days postoperatively. When the variable of intraoperative hypotension was added to stratify patients, the prognostic accuracy measured as the C statistic rose from 0.689 to 0.760 (P>0.05; Figure 1).
 | Table 3 Risk stratification by original and modified RCRIs |
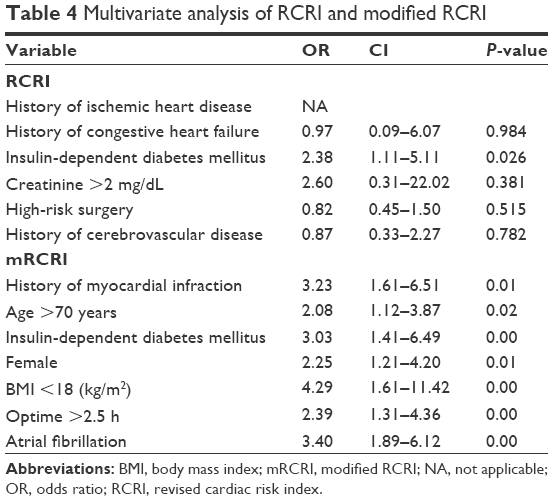 | Table 4 Multivariate analysis of RCRI and modified RCRI |
 | Figure 1 Comparison of the predictive ability of the RCRI and mRCRI by ROC analysis. |
Discussion
Myocardial injury after noncardiac surgery is associated with a marked increase in 30-day mortality, longer hospitalization, and increased health care costs.6 The previously reported incidence of postoperative cardiac complications in cardiac patients ranged from 3.9% to 10%.7–9 Patients with known ischemic heart disease are traditionally thought to have a higher cardiac risk. In our study, the incidence of PoMCE tended to fall in the lower range of previously reported data, despite the older age of the enrolled population. This finding is in accordance with earlier detection and more prompt intervention of CAD compared with a decade ago. Results from our study agree with previous findings that the presence of a history of CAD, transient ischemic attack, and diabetes does not predict mortality for patients undergoing noncardiac surgery.6 However, once combined with other specific risk factors, patients with known CADs are more vulnerable. Therefore, a good prediction tool should be used to guide preoperative evaluation and prioritization.
Modification of the original RCRI
The RCRI is the most widely used risk stratification method. However, an unsatisfactory performance of the RCRI has been shown and its implementation in the modern surgical setting has been questioned10 in vascular surgery and mixed noncardiac surgery.11–14 In this study, the ability of the original RCRI to predict PoMCE in older patients with known CAD is relatively poor, with no better accuracy than that would be obtained by chance. In our study, the individual traditional components of the RCRI were not significantly associated with PoMCE, with the exception of insulin-dependent diabetes. The bad performance and low accuracy of the RCRI were not unanticipated. Advances in surgical, as well as anesthesia, practice combined with a more elaborate management regimen of CAD, make modern cardiac patients inherently different from the 1990s when the original RCRI was developed and validated. The value of these original risk indicators in the RCRI may be diminishing over time. In earlier studies, the creatine kinase MB fraction was used to diagnose myocardial infarction, rather than troponins, which are more sensitive. Additionally, the original RCRI only considered in-patient complications, not 30-day event rates. A 30-day outcome, rather than in-hospital outcome parameters, should provide more clinical guidance.
Cerebrovascular disease
Conflicting results concerning the predictive power of cerebrovascular disease have been shown in other studies.15,16 In our study, a history of cerebrovascular disease failed to predict PoMCE in older patients with CAD who underwent noncardiac surgery. Traditionally, the degree of stenosis and atherosclerotic plaque formation were believed to be similar between the coronary artery and cerebrovasculature. However, stroke is inherently different from myocardial infarction. The classical theory of myocardial infarction is rupture of existing atherosclerotic plaques due to instability and subsequent exposure of a prothrombotic surface, platelet adherence, and vessel thrombosis.17,18 However, occurrence of stroke is more complicated and is affected by hemodynamic instability, comorbidity, such as atrial fibrillation, and intracranial vessel formation. A history of peripheral artery disease is suggested to be a good replacement factor for cerebrovascular disease in predicting cardiac risk in noncardiac surgery.19 Peripheral disease is independently predictive of cardiac injury in the presence of cerebrovascular disease,20 indicating the different nature of progression of disease.
Creatinine
Use of cutoff values of 2 mg/dL of creatinine, regardless of age, sex, and BMI, has been questioned.21 In our study, although overall creatinine levels were significantly different between patients with PoMCE and those without PoMCE, the cutoff value of 2 mg/dL failed to demonstrate predictive power. In fact, encountering patients with a creatinine level so high in modern clinical settings is rare. Use of the estimated glomerular filtration rate instead of creatine has been suggested.22 However, a study with strong clinical evidence on this issue has not been performed yet. Considering the poor performance of creatine levels >2 mg/dL, it has been removed from the original RCRI.
Adding new elements to the mRCRI
A risk prediction model must have a good discriminatory ability, while remaining easy to use. Multiple modifications have been proposed, including age,10 a history of peripheral vascular disease,20 functional capacity,23 preoperative N-terminal pro-brain natriuretic peptide levels,24 and a specific surgical procedural category. In our study, the mRCRI incorporating age, female sex, atrial fibrillation, a history of myocardial infarction, and intraoperative hypotension showed better ability in predicting PoMCE in Chinese patients with CAD.
Advanced age
Age is an independent predictor of cardiovascular events in the presence of RCRI risk factors and intraoperative risk factors.10 Increased age might control for an increased risk associated with a longer duration of exposure to a clinical risk factor. However, in our study, an age >70 years was strongly correlated with PoMCE after adjusting for the other components that are incorporated into the mRCRI. The lack of dynamic compensating ability of the cardiac vascular system among older people represents a unique cardiac risk. A large Danish national study reported an increased risk of MACE in patients with advanced age, with an OR of 1.9.25 As the life expectancy of the general population in China continues to grow, recognition of the risk of advanced age on cardiac events is important.
Atrial fibrillation
Perioperative cardiac management is often complicated by cardiac arrhythmias, and the most common type of arrhythmia is atrial fibrillation.26 Atrial fibrillation is common in older patients and patients with ischemic heart disease. The preoperative presence of atrial fibrillation may indicate previous myocardial infarction undetected by the patient. The China Acute Myocardial Infarction registry showed that the overall incidence of atrial fibrillation was 3.0% in Chinese patients with acute myocardial infarction during hospitalization.27 This study demonstrated an even higher presence of atrial fibrillation in patients with PoMCE. The CHADS2-VASc is able to predict mortality in patients with atrial fibrillation undergoing noncardiac surgery.28 Components of the CHADS2-VASc, including sex and age, have also been incorporated in the mRCRI. Without appropriate antithrombotic treatment, the risk of myocardial infarction due to coronary embolism is also increased. Incorporation of atrial fibrillation in this risk stratification model would help more patients to be prioritized.
Female sex
A previous study attributed a sex difference in perioperative cardiac risk to the fact that women enrolled in the study were generally older and had more baseline cardiovascular risk factors.29 In our study, female sex remained an independent predictor of PoMCE after adjustment for other risk factors in multivariate analysis. One retrospective registry of patients with ST segment elevation myocardial infarction showed that women have a longer time from symptom onset to hospital arrival and fewer complete revascularizations compared with men,30 indicating a lack of self-recognition and unwillingness to obtain prompt treatment. Underreported and undertreated comorbidities could be a possible reason for a higher perioperative cardiac risk. Another possible explanation is that because women in our study population were older, they were more likely to have lost the cardiac protective effect from estrogen after menopause.
Low body mass index
Overweight and obesity are risk factors for cardiovascular disease, including ischemic heart disease. However, a high BMI was not found to be a risk factor for perioperative cardiac morbidity in numerous previous studies.31 Underweight patients have a significantly increased risk of postoperative cardiac mortality and morbidity.32 This phenomenon has been termed as the obesity paradox because of the seemingly protective effect of high BMI in terms of adverse cardiac events. In our study, a low BMI, perhaps a consequence of underlying nutritional status, was an independent risk factor of PoMCE. Although the underlying mechanism of this finding requires further research, recognizing a low BMI as a cardiac risk factor for cardiac patients is important.
Intraoperative parameters
The effect of risk associated with surgery itself is crucial. In our study, univariate analysis showed that the risk of PoMCE among different surgery types was different. However, the original RCRI defines high-risk surgery as suprainguinal vascular, intraperitoneal, or intrathoracic surgery. This surgery component was not a predictor of PoMCE in this study. With advancement in the endoscopic minimally invasive technique, allocation of surgical risk is more complicated. Dangerous elements associated with surgery, including hemodynamic instability and severe physiological disturbance, cannot be defined by the operative site only. However, intraoperative parameters may be a more ideal replacement.
Cardiovascular risk prediction models rarely incorporate intraoperative physiological responses, such as hypotension, tachycardia, or hypothermia. Because preoperative risk factors are unlikely to predict intraoperative parameters, inclusion of intraoperative risk factors should be considered. Tachycardia and hypotension are thought to be associated with postoperative cardiac complications. In our cohort study, intraoperative hypotension was an independent risk factor for PoMCE. With the added predictive value of intraoperative hypotension, the predictive ability significantly improved. Additionally, a longer surgical time was associated with postoperative cardiac events. To the best of our knowledge, this is the first study to incorporate intraoperative parameters into a risk prediction model.
Conclusion
Patients with known CAD have unique challenges in terms of cardiac risk assessment and management. Identification of increased risk provides patients with information that helps them better understand the benefit-to-risk ratio of a procedure and may lead to interventions that decrease the risk. Some traditional risk prediction parameters in the RCRI are no longer suitable in the modern clinical setting and have poor prediction ability in older Chinese patients with CAD. A modified model incorporating advanced age, sex, atrial fibrillation, insulin-dependent diabetes, a history of myocardial infarction, and intraoperative parameters can possibly provide better predictive power. Additionally, this model could guide perioperative management of cardiac patients undergoing noncardiac surgery.
Limitations of this study
Because this was a post-hoc analysis, some important data related to PoMCE, such as (N-terminal pronatriuretic peptide) NT-pro brain natriuretic peptide and glomerular filtration rate, were not available in the database. The primary end point was 30-day postoperative cardiac events, and long-term prognoses of these patients were unknown. Although this was a multicenter study, the sample size of this study was still insufficient because the incidence of certain clinical events was too low to generate any statistically powerful results. Medication history was not included in this study due to no protective power against adverse cardiac events in previous study using the same database. However, in other trials, mediation was demonstrated to potentially influence prognosis. This problem may be better evaluated in future clinical trials with larger sample size.
Acknowledgments
We thank Ellen Knapp, PhD, from Liwen Bianji, Edanz Group China, for editing the English text of a draft of this manuscript. This study was funded by the Chinese Ministry of Health Special Fund for Public Welfare (No 200802030).
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Pannell LM, Reyes EM, Underwood SR. Cardiac risk assessment before non-cardiac surgery. Eur Heart J Cardiovasc Imaging. 2013;14(4):316–322. | ||
Weiwei C, Runlin G, Lisheng L, et al. Outline of the report on cardiovascular diseases in China, 2014. Eur Heart J Suppl. 2016;18 (supplF):F2–F11. | ||
Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043–1049. | ||
Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Developed in collaboration with the American College of Surgeons, American Society of Anesthesiologists, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Anesthesiologists, and Society of Vascular Medicine Endorsed by the Society of Hospital Medicine. J Nucl Cardiol. 2015;22(1):162–215. | ||
Xu L, Yu C, Jiang J, et al. Major adverse cardiac events in elderly patients with coronary artery disease undergoing noncardiac surgery: a multicenter prospective study in China. Arch Gerontol Geriatr. 2015;61(3):503–509. | ||
Roshanov PS, Walsh M, Devereaux PJ, et al. External validation of the revised cardiac risk index and update of its renal variable to predict 30-day risk of major cardiac complications after non-cardiac surgery: rationale and plan for analyzes of the VISION study. BMJ Open. 2017;7(1):e013510. | ||
Royo MB, Fleisher LA. Chasing myocardial outcomes: perioperative myocardial infarction and cardiac troponin. Can J Anaesth. 2016;63(2):227–232. | ||
Ma J, Xin Q, Wang X, Gao M, Wang Y, Liu J. Prediction of perioperative cardiac events through preoperative NT-pro-BNP and cTnI after emergent non-cardiac surgery in elderly patients. PLoS One. 2015;10(3):e0121306. | ||
Hoftman N, Prunean A, Dhillon A, Danovitch GM, Lee MS, Gritsch HA. Revised Cardiac Risk Index (RCRI) is a useful tool for evaluation of perioperative cardiac morbidity in kidney transplant recipients. Transplantation. 2013;96(7):639–643. | ||
Biccard B. Proposed research plan for the derivation of a new Cardiac Risk Index. Anesth Analg. 2015;120(3):543–553. | ||
Cuthbertson BH, Amiri AR, Croal BL, et al. Utility of B-type natriuretic peptide in predicting perioperative cardiac events in patients undergoing major non-cardiac surgery. Br J Anaesth. 2007;99(2):170–176. | ||
Ausset S, Auroy Y, Lambert E, et al. Cardiac troponin I release after hip surgery correlates with poor long-term cardiac outcome. Eur J Anaesthesiol. 2008;25(2):158–164. | ||
Leibowitz D, Planer D, Rott D, Elitzur Y, Chajek-Shaul T, Weiss AT. Brain natriuretic peptide levels predict perioperative events in cardiac patients undergoing noncardiac surgery: a prospective study. Cardiology. 2008;110(4):266–270. | ||
Wotton R, Marshall A, Kerr A, et al. Does the revised cardiac risk index predict cardiac complications following elective lung resection? J Cardiothorac Surg. 2013;8:220. | ||
Carabini LM, Zeeni C, Moreland NC, et al. Predicting major adverse cardiac events in spine fusion patients: is the revised cardiac risk index sufficient? Spine (Phila Pa 1976). 2014;39(17):1441–1448. | ||
Matsumoto S, Takayama T, Wakatsuki K, et al. Preoperative cardiac risk assessment and surgical outcomes of patients with gastric cancer. Ann Surg Oncol. 2016;23 (Suppl 2):S222–S229. | ||
Monahan TS, Shrikhande GV, Pomposelli FB, et al. Preoperative cardiac evaluation does not improve or predict perioperative or late survival in asymptomatic diabetic patients undergoing elective infrainguinal arterial reconstruction. J Vasc Surg. 2005;41(1):38–45; discussion 45. | ||
Back MR, Stordahl N, Cuthbertson D, Johnson BL, Bandyk DF. Limitations in the cardiac risk reduction provided by coronary revascularization prior to elective vascular surgery. J Vasc Surg. 2002;36(3):526–533. | ||
Botto F, Alonso-Coello P, Chan MT, et al; Vascular events In noncardiac Surgery patients cohort evaluation VISION Study Investigators. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564–578. | ||
Kirwin JD, Ascer E, Gennaro M, et al. Silent myocardial ischemia is not predictive of myocardial infarction in peripheral vascular surgery patients. Ann Vasc Surg. 1993;7(1):27–32. | ||
Davis C, Tait G, Carroll J, Wijeysundera DN, Beattie WS. The revised cardiac risk index in the new millennium: a single-center prospective cohort re-evaluation of the original variables in 9,519 consecutive elective surgical patients. Can J Anaesth. 2013;60(9):855–863. | ||
Mooney JF, Ranasinghe I, Chow CK, et al. Preoperative estimates of glomerular filtration rate as predictors of outcome after surgery: a systematic review and meta-analysis. Anesthesiology. 2013;118(4):809–824. | ||
Carli F, Minnella EM. Preoperative functional assessment and optimization in surgical patient. Changing the paradigm. Minerva Anesthesiol. 2017;83(2):214–218. | ||
Choi JH, Cho DK, Song YB, et al. Preoperative NT-proBNP and CRP predict perioperative major cardiovascular events in non-cardiac surgery. Heart. 2010;96(1):56–62. | ||
Hansen PW, Gislason GH, Jorgensen ME, et al. Influence of age on perioperative major adverse cardiovascular events and mortality risks in elective non-cardiac surgery. Eur J Intern Med. 2016;35:55–59. | ||
Cerit L. Recurrent acute myocardial infarction and atrial fibrillation. J Geriatr Cardiol. 2017;14(2):153–154. | ||
Dai Y, Yang J, Gao Z, et al; CAMI Registry study group. Atrial fibrillation in patients hospitalized with acute myocardial infarction: analysis of the china acute myocardial infarction (CAMI) registry. BMC Cardiovasc Disord. 2017;17(1):2. | ||
van Diepen S, Youngson E, Ezekowitz JA, McAlister FA. Which risk score best predicts perioperative outcomes in nonvalvular atrial fibrillation patients undergoing noncardiac surgery? Am Heart J. 2014;168(1):60–67.e5. | ||
Parashar A, Agarwal S, Krishnaswamy A, et al. Percutaneous intervention for myocardial infarction after noncardiac surgery: patient characteristics and outcomes. J Am Coll Cardiol. 2016;68(4):329–338. | ||
Otten AM, Maas AH, Ottervanger JP, et al. Is the difference in outcome between men and women treated by primary percutaneous coronary intervention age dependent? Gender difference in STEMI stratified on age. EurHeart J Acute Cardiovasc Care. 2013;2(4):334–341. | ||
Henke PK, Zamora-Berridi G, Englesbe MJ, et al. A case-cohort study of postoperative myocardial infarction: impact of anemia and cardioprotective medications. Surgery. 2014;156(4):1018–1026, 1029. | ||
Kiziloz H, Dorin R, Finnegan KT, Shichman S, Meraney A. The impact of body mass index on perioperative outcomes in robot-assisted laparoscopic partial nephrectomy. J Endourol. 2013;27(8):1000–1007. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.