")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Clinical utility of secukinumab in moderate-to-severe scalp psoriasis: evidence to date
Authors Kivelevitch D , Amin S, Menter A
Received 20 November 2018
Accepted for publication 13 March 2019
Published 24 April 2019 Volume 2019:12 Pages 249—253
DOI https://doi.org/10.2147/CCID.S165040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Dario Kivelevitch,1 Sima Amin,2 Alan Menter1
1Baylor University Medical Center, Dallas, TX, USA; 2Texas A&M College of Medicine, Bryan, TX, USA
Abstract: Psoriasis is an immune-mediated inflammatory dermatosis commonly affecting the scalp and fringes of the face, neck and ears. It may be difficult to treat and the presence of extensive and highly visible lesions may significantly influence psychosocial well-being. Secukinumab, a monoclonal antibody that selectively targets interleukin-17A and has been shown to provide robust and sustained efficacy for whole body psoriasis. In this review, we evaluate the evidence to date of secukinumab in patients with moderate-to-severe scalp psoriasis. A comprehensive Cochrane database and PubMed searches of all available literature in English through September 2018 was performed using the search terms: “psoriasis”, “scalp” and “secukinumab”. Based on current evidence, we conclude that secukinumab is efficacious and well-tolerated treatment for patients with moderate-to-severe scalp psoriasis. Further studies are however warranted.
Keywords: secukinumab, psoriasis, scalp, therapy
Introduction
Psoriasis is a chronic immune-mediated disease affecting the skin and joints with numerous associated systemic comorbidities including obesity, diabetes, metabolic syndrome and heart disease. Psoriasis affects 3.2% of the population worldwide.1 There are several clinical variants of psoriasis with plaque psoriasis being the most common, present in approximately 80% of the psoriasis patients. Scalp psoriasis together with intertriginous, palmoplantar and nail psoriasis are in general considered difficult to treat. Scalp psoriasis can affect up to 80% of the psoriasis patients and is the first site of involvement in up to 25% of the cases.2,3 While the head and neck represent only 10% of the body’s surface area, the consequences of scalp psoriasis may be disproportionate to the area affected.4 The use of scoring systems specific to the body site helps in assessing more precisely the severity of psoriasis in these difficult to treat locations.5 Additionally, the assessment of a more comprehensive evaluation of the psoriasis disease burden can be obtained by using patient-reported outcomes.
Scalp psoriasis has been shown to impair quality of life regardless of the severity of psoriasis on other affected body regions.6 In addition to pain, pruritus, cracking, bleeding and shedding of scale, it can also increase psychosocial burden especially in patients with visible lesions.4,7 While psoriasis is traditionally a highly symmetrical condition affecting both sides of the limbs equally (ie, knees and elbows), it is seldom symmetrical on the scalp due to persistent scratching of predominantly one side of the head (Koebner phenomenon). Psychological burdens of psoriasis include negative impact on work or school attendance and performance, reduced self-esteem, negative social interaction and interference with daily routines.4,7,8
Treatment of scalp psoriasis is challenging, as clinical response is frequently insufficient. Current treatment modalities include phototherapy, topical corticosteroids topical vitamin D analogs systemic agents including methotrexate, cyclosporine and apremilast and available biologic agents.4
Secukinumab is a human IgG1 monoclonal antibody that selectively binds to and neutralizes interleukin (IL)-17A. It is FDA approved for the treatment of adult plaque psoriasis, psoriatic arthritis and ankylosing spondylitis. IL-17A is a key cytokine of Th17 cells that participates in keratinocyte stimulation to produce chemokines, cytokines and other proinflammatory mediators and sustains chronic inflammation.9 The dose of secukinumab is 300 mg by self-administered subcutaneous injection at weeks 0, 1, 2, 3 and 4 followed by 300 mg every 4 weeks.10 The safety and efficacy of secukinumab in patients with moderate-to-severe plaque psoriasis has been well demonstrated in phase 3 studies.7,11–14 In this review, we evaluate the evidence to date of the efficacy of secukinumab in patients with moderate-to-severe scalp psoriasis.
Method of literature search
A comprehensive Cochrane database and PubMed central and PubMed searches of all available literature in English through September 2018 was performed using a combination of the following search terms: “psoriasis”, “scalp” and “secukinumab”. Only clinical trials, case series and reports were considered in our search. A total of three articles matched the search criteria and were included in this review, two were results of a single randomized controlled clinical trial, the third article was a case report. The remainder of the publications found were either reviews of the literature or out of the scope of this article (Figure 1).
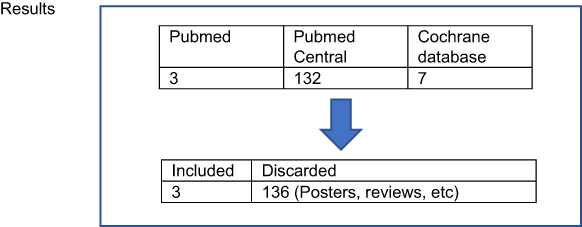 | Figure 1 Literature search |
Review of evidence
A phase 3b randomized controlled trial (RCT) analyzed the effects of secukinumab in moderate-to-severe scalp psoriasis.15 Adult patients with moderate-to-severe scalp psoriasis of ≥6 months duration, inadequately controlled by topical treatments, or systemic therapies were eligible to participate in the trial. It is worth noting that both patients with or without plaque psoriasis elsewhere on the body were equally eligible. Moderate-to-severe scalp psoriasis was defined as a Psoriasis Scalp Severity Index (PSSI) score of ≥12, with ≥30% of the scalp surface area affected and an Investigator’s Global Assessment modified 2011 (IGA mod 2011) (scalp only) score of ≥3. The objectives of the study included determining the number of patients that achieved an improvement of 90% in the PSSI (PSSI 90), and an IGA mod 2011 score of 0 (clear) or 1 (almost clear) at week 12. Additionally, the following patient-reported outcomes were evaluated: scalp pain, itching and scaling at baseline and thereafter at weeks 1, 2, 3, 4, 8 and 12. Quality of life (QOL) was assessed at baseline and then every 4 weeks using the patient-reported Scalpdex. A total of 102 patients were randomized 1:1 to either secukinumab 300 mg or placebo at baseline, weeks 1, 2 and 3, and then every 4 weeks for 24 weeks.16 At 12 weeks, patients on placebo who did not achieve a PSSI 90 were switched to secukinumab 300 mg until week 24. Patients on placebo that achieved PSSI 90 continued on placebo until the end of the study. All groups remain blinded during the course of the study.
Baseline characteristics such as age, gender, BMI and baseline PSSI and Psoriasis Area and Severity Index (PASI) scores were similar among both groups.
Clinical efficacy: At week 12, PSSI 90 was achieved by 52.9% of the patients in the secukinumab group vs 2% in the placebo group. At week 24, the percentage of treated patients that achieved PSSI 90 reached 58.8%. The IGA scalp score of 0/1 was achieved by 56.9% in the secukinumab group vs 5.9% in the placebo group. Additionally, at 12 weeks, 35% of the patients in the secukinumab group achieved a PSSI 100 compared to 0% in the placebo group, and at week 24 the rate of patients with PSSI 100 reached 47.2% (p<0.001).
Patient-reported outcomes: Overall, QOL improvement was significantly higher in the secukinumab treated group compared to placebo (p<0.001). Patients treated with secukinumab also recorded a statistically significant greater mean improvement in scalp itching, scaling and pain compared to placebo (p<0.001). There were no new safety signals with secukinumab during the 24 weeks of the trial.
Additionally, a case report presented a scalp psoriasis patient successfully treated with secukinumab. The patient presented psoriasis lesions on the scalp with a surface area affected ≥30%. After 16 weeks of treatment with secukinumab 300 mg, the patient was clear of lesions. At 52 weeks the patient maintained clear of his psoriasis.17
Conclusion
Scalp psoriasis has a large negative impact on psychosocial aspects and overall quality of life of patients with moderate-to-severe psoriasis.6,18 Scalp involvement is present in up to 80% of the psoriasis patients3 and is considered among the difficult to treat areas in psoriasis patients. Clinical trials for the treatment of plaque psoriasis with biologic agents including adalimumab, etanercept, infliximab, ustekinumab, ixekizumab, guselkumab and risankizumab have also shown significant reduction of the mean PSSI with a significant number of patients achieving scalp clearance.19–23 Furthermore, a pooled analysis of 4 phase III RCT (ERASURE, FIXTURE, FEATURE and JUNCTURE) assessed the efficacy of secukinumab for head and neck psoriasis in patients with moderate-to-severe psoriasis.7 This sub-analysis did not assess scalp psoriasis separated from other areas of the head and neck. At 52 weeks, head and neck PASI 90 and 100 responses were achieved by 76.0% and 68.7% of the patients receiving secukinumab 300 mg, respectively. At Week 52, whole body PASI 90 and100 responses were achieved by 68.1% and 40.8% of the patients receiving secukinumab 300 mg, respectively. Most of these studies were sub-analyses of larger RCTs designed for patients with plaque-type psoriasis anywhere in the skin.3,24 Furthermore, in many of those RCT patients were allowed to use topical treatments. In contrast, the inclusion criteria for the RCT described above was designed to include patients solely based on the severity of scalp psoriasis regardless of body plaque psoriasis and the use of any topical treatment during the study was not allowed.23,25,26 Patients in this trial had severe scalp psoriasis with a mean scalp surface area affected of 60% and a mean PSSI of 33.2. Additionally, 89% of the patients in this study had a baseline PASI score of 9.24, lower than the requirement systemic clinical trials have. Therefore, result comparisons between other scalp psoriasis studies and the one we have reviewed should be performed cautiously. The clinical trial described in this review showed that treatment with secukinumab 300 mg, achieved significantly greater PSSI 90, PSSI 100 and IGA mod 2011 scalp 0 or 1 scores than placebo at week 12. These responses were sustained up to week 24. Significant clinical responses to secukinumab were observed as early as 3 weeks after starting treatment. Secukinumab is efficacious and well tolerated in moderate-to-severe scalp psoriasis even when used alone without concomitant treatment for scalp psoriasis. Additionally, there were no new safety signals during the 24 weeks of treatment with secukinumab. The safety profile of secukinumab in this study was similar to that seen in previous phase 3 trials.11–13 Patients treated with secukinumab also reported significant improvement of psoriasis scalp pain, itching, scaling and scalp-related quality of life as early as 1 week for scaling and week 2 for pain, and itching. Improvements in scalp-related quality of life, pain, itching and scaling were maintained through week 12.16 Despite many moderate-to-severe psoriasis patients being treated with biologic agents, there is limited evidence regarding the effectiveness of biologic agents for specifically treating scalp psoriasis and its associated symptoms. The clinical trial discussed in this review focused not only on physical findings but also on subjective symptoms, providing evidence for the treatment of several under recognized and undertreated subjective manifestations such as itch and pain, which can have a deep impact in our patients’ quality of life.
In conclusion, secukinumab is an efficacious and well-tolerated treatment for patients with moderate-to-severe scalp psoriasis. Further trials and registries will be required to assess the longer-term safety and efficacy of secukinumab in scalp psoriasis.
Disclosure
Dr. Alan Menter has been on the Advisory Board, a consultant, investigator, speaker and receives grants and an honoraria from Abbott Labs, Amgen, Boehringer Ingelheim, Janssen Biotech Inc, LEO Pharma, and Sienna. Dr. Menter has been on the Advisory Board, an investigator and receives grants and honoraria from Boehringer Ingelheim. Dr. Menter has been an investigator and receives grants from Celgene and Merck. Dr. Menter has also been a consultant, investigator and a speaker and receives honoraria from Eli Lilly, Novartis, and UCB. The authors report no other conflicts of interest in this work.
References
1. Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512–516. doi:10.1016/j.jaad.2013.11.013
2. Kaur I, Handa S, Kumar B. Natural history of psoriasis: a study from the Indian subcontinent. J Dermatol. 1997;24(4):230–234.
3. Papp K, Berth-Jones J, Kragballe K, Wozel G, de la Brassinne M. Scalp psoriasis: a review of current topical treatment options. J Eur Acad Dermatol Venereol. 2007;21(9):1151–1160. doi:10.1111/j.1468-3083.2007.02424.x
4. Crowley J. Scalp psoriasis: an overview of the disease and available therapies. J Drugs Dermatol. 2010;9(8):912–918.
5. Frez ML, Asawanonda P, Gunasekara C, et al. Recommendations for a patient-centered approach to the assessment and treatment of scalp psoriasis: a consensus statement from the Asia Scalp Psoriasis Study Group. J Dermatolog Treat. 2014;25(1):38–45. doi:10.3109/09546634.2012.742176
6. Zampieron A, Buja A, Fusco M, et al. Quality of life in patients with scalp psoriasis. G Ital Dermatol Venereol. 2015;150(3):309–316.
7. Kircik L, Fowler J, Weiss J, Meng X, Guana A, Nyirady J. Efficacy of secukinumab for moderate-to-severe head and neck psoriasis over 52 weeks: pooled analysis of four phase 3 studies. Dermatol Ther (Heidelb). 2016;6(4):627–638. doi:10.1007/s13555-016-0139-0
8. Koo J, Marangell LB, Nakamura M, et al. Depression and suicidality in psoriasis: review of the literature including the cytokine theory of depression. J Eur Acad Dermatol Venereol. 2017. doi:10.1111/jdv.14460
9. Lynde CW, Poulin Y, Vender R, Bourcier M, Khalil S. Interleukin 17A: toward a new understanding of psoriasis pathogenesis. J Am Acad Dermatol. 2014;71(1):141–150. doi:10.1016/j.jaad.2013.12.036
10.
11. Paul C, Lacour J-P, Tedremets L, et al. Efficacy, safety and usability of secukinumab administration by autoinjector/pen in psoriasis: a randomized, controlled trial (JUNCTURE). J Eur Acad Dermatol Venereol. 2015;29(6):1082–1090. doi:10.1111/jdv.12751
12. Langley RG, Elewski BE, Lebwohl M, et al. Secukinumab in plaque psoriasis–results of two phase 3 trials. N Engl J Med. 2014;371(4):326–338. doi:10.1056/NEJMoa1314258
13. Blauvelt A, Prinz JC, Gottlieb AB, et al. Secukinumab administration by pre-filled syringe: efficacy, safety and usability results from a randomized controlled trial in psoriasis (FEATURE). Br J Dermatol. 2015;172(2):484–493. doi:10.1111/bjd.13348
14. Thaci D, Blauvelt A, Reich K, et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J Am Acad Dermatol. 2015;73(3):400–409. doi:10.1016/j.jaad.2015.05.013
15. Bagel J, Duffin KC, Moore A, et al. The effect of secukinumab on moderate-to-severe scalp psoriasis: results of a 24-week, randomized, double-blind, placebo-controlled phase 3b study. J Am Acad Dermatol. 2017;77(4):667–674. doi:10.1016/j.jaad.2017.05.033
16. Feldman SR, Green L, Kimball AB, et al. Secukinumab improves scalp pain, itching, scaling and quality of life in patients with moderate-to-severe scalp psoriasis. J Dermatolog Treat. 2017;28(8):716–721. doi:10.1080/09546634.2017.1329502
17. Platsidaki E, Kostopoulos N, Marnelakis I, Panagakis P. Secukinumab shows significant efficacy in two patients with difficult-to-treat areas of psoriasis: a Greek experience. Dermatol Online J. 2018;24(3):17.
18. Lebwohl MG, Bachelez H, Barker J, et al. Patient perspectives in the management of psoriasis: results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis Survey. J Am Acad Dermatol. 2014;70(5):871–881.e30. doi:10.1016/j.jaad.2013.12.018
19. Khobzey K, Liskova I, Szegedi A, et al. Effectiveness of adalimumab in the treatment of scalp and nail affection in patients with moderate to severe plaque psoriasis in routine clinical practice. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26(1):11–14.
20. Bagel J, Lynde C, Tyring S, Kricorian G, Shi Y, Klekotka P. Moderate to severe plaque psoriasis with scalp involvement: a randomized, double-blind, placebo-controlled study of etanercept. J Am Acad Dermatol. 2012;67(1):86–92. doi:10.1016/j.jaad.2011.07.034
21. Kalb RE, Blauvelt A, Sofen HL, et al. Effect of infliximab on health-related quality of life and disease activity by body region in patients with moderate-to-severe psoriasis and inadequate response to etanercept: results from the PSUNRISE trial. J Drugs Dermatol. 2013;12(8):874–880.
22. Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405–417. doi:10.1016/j.jaad.2016.11.041
23. Langley RG, Rich P, Menter A, et al. Improvement of scalp and nail lesions with ixekizumab in a phase 2 trial in patients with chronic plaque psoriasis. J Eur Acad Dermatol Venereol. 2015;29(9):1763–1770. doi:10.1111/jdv.12996
24. Griffiths CE, Reich K, Lebwohl M, et al. Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis (UNCOVER-2 and UNCOVER-3): results from two phase 3 randomised trials. Lancet. 2015;386(9993):541–551. doi:10.1016/S0140-6736(15)60125-8
25. Thaci D, Unnebrink K, Sundaram M, Sood S, Yamaguchi Y. Adalimumab for the treatment of moderate to severe psoriasis: subanalysis of effects on scalp and nails in the BELIEVE study. J Eur Acad Dermatol Venereol. 2015;29(2):353–360. doi:10.1111/jdv.12553
26. Rich P, Gooderham M, Bachelez H, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with difficult-to-treat nail and scalp psoriasis: results of 2 phase III randomized, controlled trials (ESTEEM 1 and ESTEEM 2). J Am Acad Dermatol. 2016;74(1):134–142. doi:10.1016/j.jaad.2015.09.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.