")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Clinical Utility of Deutetrabenazine as a Treatment Option for Chorea Associated with Huntington’s Disease and Tardive Dyskinesia
Received 7 January 2023
Accepted for publication 16 November 2023
Published 1 December 2023 Volume 2023:19 Pages 1019—1024
DOI https://doi.org/10.2147/TCRM.S279332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Samuel Frank,1 Aljoharah Alakkas2
1Department of Neurology, Beth Israel Deaconess Medical Center/Harvard Medical School, Boston, MA, USA; 2Department of Neurology, National Neuroscience Institute, King Fahad Medical City, Riyadh, K.S.A
Correspondence: Samuel Frank, Department of Neurology, Beth Israel Deaconess Medical Center/Harvard Medical School, 330 Brookline Ave, Kirstein 228, Boston, MA, 02215, USA, Tel +1 617-667-4889, Fax +1 617-975-5454, Email [email protected]
Abstract: Deutetrabenazine (DTBZ) is used for the treatment of tardive dyskinesia (TD) and chorea in Huntington’s Disease (HD). Four pivotal clinical trials showed the efficacy of DTBZ in these conditions. Long term follow-up studies confirmed evidence of overall safety and continued efficacy of this drug. Indirect comparisons revealed relative superiority of DTBZ over TBZ in terms of safety, but direct comparisons of safety and efficacy between the VMAT2 and dopamine blocking agents is lacking. Deutetrabenazine is safe and effective in the treatment of TD and chorea in HD in doses up to 72 mg daily and for up to three years in duration.
Keywords: chorea, tardive dyskinesia, hyperkinetic movement disorders, VMAT2 inhibitors
Introduction
Chorea is an involuntary hyperkinetic movement disorder characterized by rapid, irregular movements flowing randomly from one body region to another1,2. Chorea is the hallmark of Huntington disease (HD), a rare, fatal degenerative brain disease. Disease-modifying treatments for HD are not available. Thus, the treatment is usually symptomatic, including suppressing chorea. The pathophysiology behind chorea is complex; however, it is thought that an excess of dopamine contributes to the development of this hyperkinetic movement3,4. Dopamine receptor blockers or dopamine-depleting agents can be used to treat chorea if it is affecting the patient’s quality of life, interfering with function or causing safety issues. Dopamine receptor blockers are associated with an increased risk of tardive dyskinesia, and therefore, to reduce chorea, clinicians may prefer to prescribe presynaptic dopamine depleting agents.
Tardive dyskinesia (TD) is a hyperkinetic movement disorder secondary to exposure to dopamine receptor blockers. The blockage of dopamine receptors leads to its upregulation and hypersensitization.1,2 Thus, modulating the dopaminergic system using dopamine-depleting agents might be useful. Presynaptic dopamine-depleting agents include reserpine, tetrabenazine (TBZ), valbenazine (VBZ), and deutetrabenazine (DTBZ). This review focuses on the use of DTBZ in the treatment of chorea associated with Huntington’s disease (HD) and tardive dyskinesia. We will summarize current evidence for use and provide clinical pearls, recognizing that this narrative is a summary of available studies on DTBZ in HD and TD may include personal bias.
Vesicular Monoamine Transporter (VMAT) Inhibitors
Neuronal transmission requires the release of neurotransmitters from the presynaptic neuron to the postsynaptic neuron. The uptake of neurotransmitters into presynaptic vesicles is performed by vesicular monoamine transporters (VMATs).3 VMAT1 is expressed in both the central nervous system (CNS) and the peripheral nervous system (PNS), while VMAT2 is predominantly expressed in the CNS.4,5 While reserpine is rarely used today, there are three reversible and selective VMAT2 inhibitors on the world market today (Table 1).
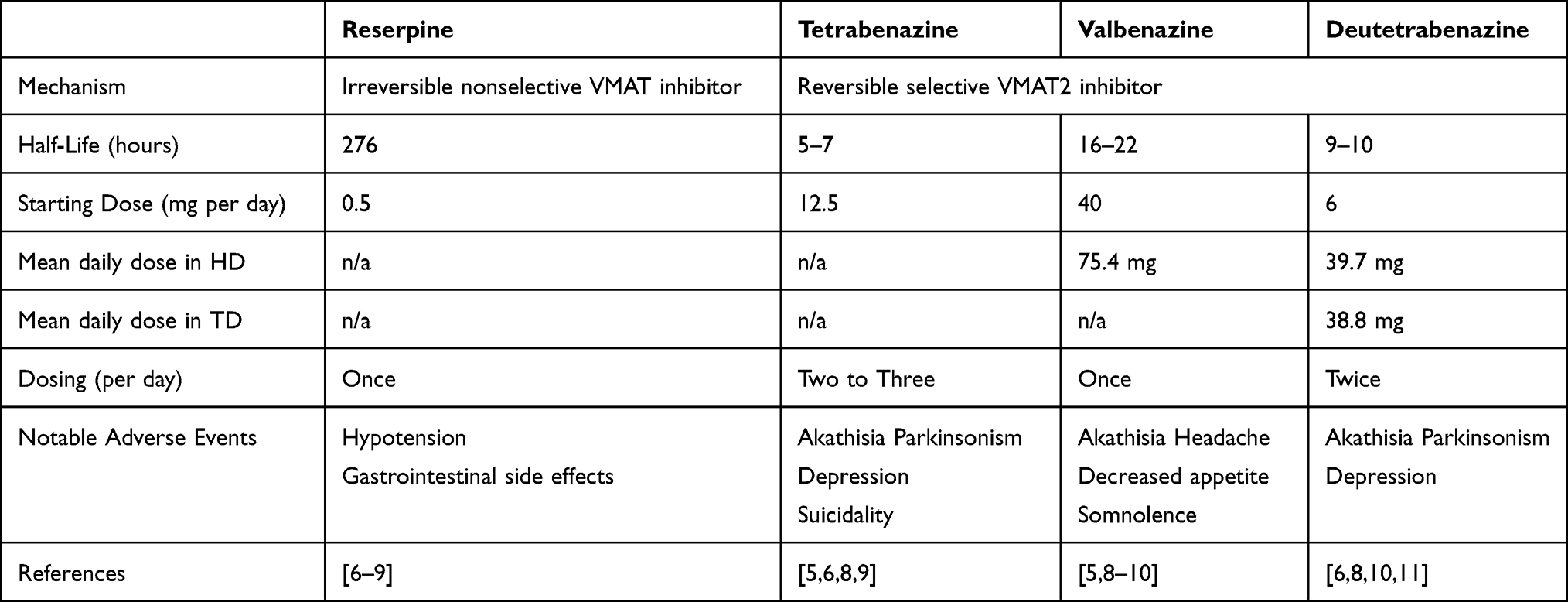 |
Table 1 Vesicular Monoamine Transporter Inhibitors |
Deutetrabenazine
Pharmacokinetics
DTBZ is a highly selective, deuterium containing VMAT2 inhibitor. It has the same chemical structure as tetrabenazine, but the molecule is formed with six sites containing deuterium rather than hydrogen. Deuteration prolongs the drug’s half-life and reduces metabolic variability.12 DTBZ is metabolized in the liver to α-dihydrodeutetrabenazine and β-dihydrodeutetrabenazine. These two metabolites are active and act by reversibly inhibiting VMAT2. Peak plasma concentrations of these metabolites are reached in 3–4 hours, and the half-life is around 9–10 hours.11,13,14
Dosing and Drug Interactions
DTBZ is dosed twice a day and comes in three strengths (6, 9, and 12 mg). The recommended starting dose is 6 mg/day.11 This is increased weekly by 6 mg/day till sufficient control of the chorea is achieved. The maximum dosage is 24 mg twice a day.11 The maximum studied was 72 mg per day.15
In regards to drug interactions, CYP2D6 inhibitors (eg, paroxetine, fluoxetine, and bupropion) can increase the levels of DTBZ metabolites.11 Thus, it is recommended that individuals taking CYP2D6 inhibitors not exceed 36 mg/day.11 In addition, the coadministration of DTBZ with the nonselective VMAT inhibitor reserpine is contraindicated. The reason is that the combination can lead to a considerable reduction in monoamine levels in the CNS.11
Clinical Utility of Deutetrabenazine in Huntington’s Disease (HD)
HD is an autosomal-dominant neurodegenerative disorder. This is caused by CAG repeat expansion in the HTT gene in chromosome 4.16,17 The manifestations of HD include a triad of motor, cognitive, and behavioral changes. Early in the outward manifestation of the disease, chorea is a prominent motor manifestation.17
Unfortunately, given the absence of disease-modifying therapies, treatments for HD focus on symptom management. As noted above, the hyperdopamine state likely plays a role in the development of chorea. Thus, VMAT2 inhibitors are used for the symptomatic treatment of HD-related chorea.
Of note, the impact of chorea on individuals is variable. Two individuals may experience the same severity of chorea, with one grading the chorea as bothersome and another being unaware of his chorea. If chorea is bothersome, symptomatic treatment is warranted, as it can have a detrimental effect on quality of life or safety.16
Efficacy of Deutetrabenazine in Treating HD Symptoms
The safety and efficacy of DTBZ in HD has been evaluated in a small number of studies, summarized in Table 2. Deutetrabenazine was initially evaluated in a 12-week double-blind placebo-controlled study, First-HD. The inclusion criteria included a Unified HD Rating Scale (UHDRSä) total maximal chorea (TMC) score of ≥ 8 and a UHDRSä total functional capacity score of ≥ 5.18 Patients with untreated psychiatric illnesses or a history of suicidal thoughts were excluded from this study.18 The study enrolled a total of 90 participants with a mean age of 53.7 years and a mean DTBZ dosage of 39.7 mg/day.18 The baseline characteristics except for a higher Berg balance test score in the DTBZ group were overall similar.18 The study showed that DTBZ was superior to the placebo in decreasing TMC (–4.4 vs –1.9; mean between group difference = −2.5 units [P < 0.001]).18 Adverse events in this study were similar between DTBZ and the placebo.18
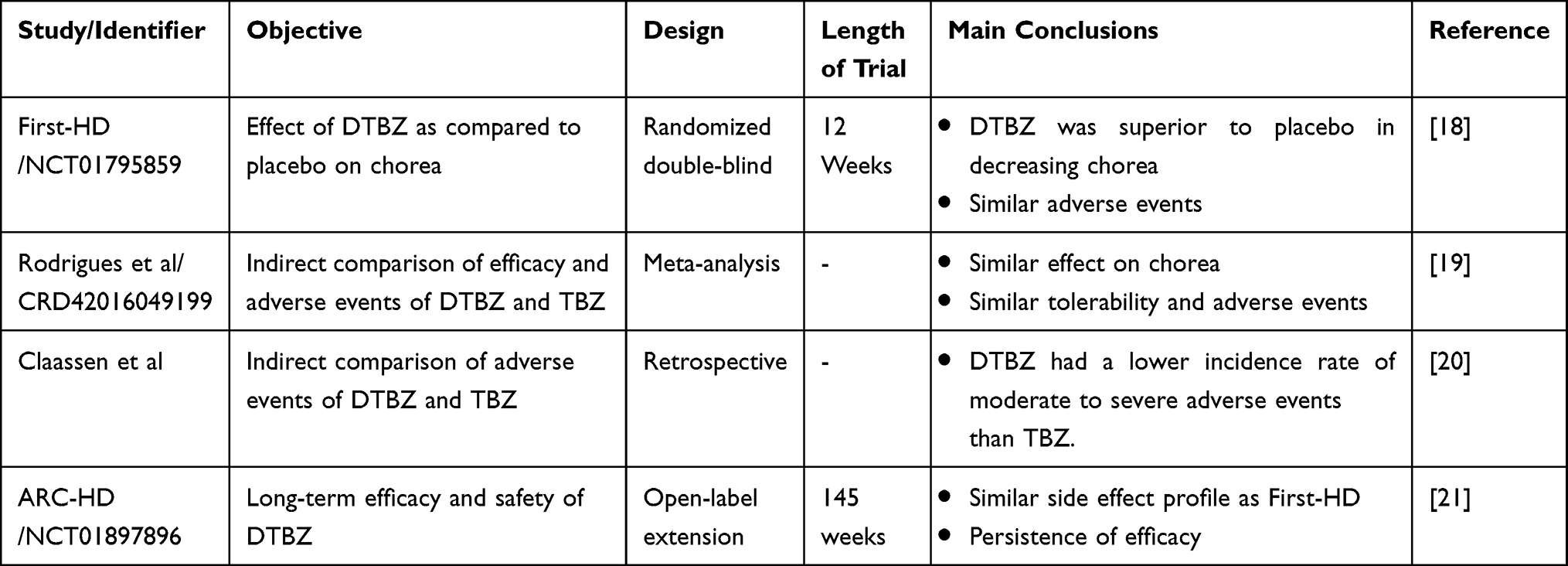 |
Table 2 Summary of Published Studies of Deutetrabenazine in Huntington Disease |
While there has not yet been a clinical trial to directly compare the safety and efficacy of TBZ versus DTBZ, one meta-analysis and one retrospective study has attempted this comparison. Data from the TETRA-HD and First-HD trials were used.18,22 These two studies share similar methodologies that allow for a reasonable comparison. The inclusion criteria for these studies were similar, except that the required total TMC in the TETRA-HD study was slightly higher (≥ 10).22
The meta-analysis found no difference between DTBZ and TBZ on improvement in chorea.19 There was also no significant difference in the odds of adverse events. However, when using rating scales, depression and somnolence were significantly higher in the TBZ group than in the DTBZ group (mean difference: 0.94 and 2.1, respectively).19 The retrospective study showed that the DTBZ group had a lower incidence rate of moderate to severe adverse events than the TBZ group.20 These included fewer depression, somnolence, and motor adverse events (parkinsonism and akathisia) in the DTBZ group.20 The risk difference of mild adverse events, diarrhea, and coughing was higher in the DTBZ group.20 It is important to note that the meta-analysis used OR, while the retrospective study used risk difference, which might explain the discrepancy between the two studies. Overall, these reports suggest that DTBZ is slightly better tolerated than TBZ. However, it is important to note that these trials were short and thus a longer-term tolerability study is warranted.
In addition, an open-label extension study (ARC-HD) was conducted.21 The study included patients who completed the First-HD trial (rollover) and patients who converted overnight from a stable dose of tetrabenazine (switch). A total of 119 patients were enrolled and followed for 145 weeks including an initial eight week titration. The average UHDRS total motor scores were –7.1 and –2.4 in the rollover and switch groups, respectively.21 Common adverse events (≥ 4% either cohort) included somnolence (Rollover, 20%; Switch, 30%), depression (32%; 22%), anxiety (27%; 35%), insomnia (23%; 16%), and akathisia (6%; 11%). Adverse events of interest included suicidality (9%; 5%) and parkinsonism (4%; 8%). Mean dose at week 8 was 38.1 mg (Rollover) and 36.5 mg (Switch). Mean dose across cohorts after titration was 37.6 mg; at the final visit, mean dose across cohorts was 45.7 mg. Patients showed minimal change in the UHDRSÔ total maximal chorea scores with stable dosing from weeks 8–145 or at the end of treatment, but total motor score increased versus week 8 (mean change [standard deviation]: 8.2 [11.9]). There were no unexpected adverse events upon drug withdrawal, and mean (standard deviation) total maximal chorea scores increased 4.7 (4.6) units from week 8 to 1-week follow-up.21
To summarize, DTBZ is effective for the treatment of HD-related chorea. It appears to have a short- and longer-term favorable side-effect profile. There have been indirect comparisons between DTBZ with TBZ, but future studies will be needed to compare the effectiveness of TBZ, VBZ and DTBZ in treating HD-related chorea.
Clinical Utility of Deutetrabenazine in Treating Tardive Dyskinesia
Tardive syndrome (TS) includes both motor and sensory phenomena that occur secondary to dopamine-blocking agents.23 One form of TS is tardive dyskinesia. TD is characterized by a stereotypical movement in the oral-buccal-lingual region and possibly includes choreiform movements of other body regions (eg, neck, trunk, and limbs).23
TD is common in patients being treated with dopamine blocking agents, with an estimated prevalence of 25.3%. The prevalence is slightly higher with first-generation antipsychotics compared to second-generation antipsychotics at 30% versus 20.7%, respectively.24
The pathophysiology behind the development of TD is not fully understood; however, one plausible theory is that the blockage of D2 receptors leads to the upregulation and hypersensitization of this receptor.1,2 This, in turn, results in excessive striato-thalamo-cortical stimulation leading to these hyperkinetic movements.1,2 Thus, modulating the dopaminergic system using dopamine-depleting agents, such as VMAT2 inhibitors, might be useful. Below we will review the efficacy of DTBZ in treating TD symptoms.
Efficacy of Deutetrabenazine in Tardive Dyskinesia
There are limited studies of DTBZ completed in tardive dyskinesia, summarized in Table 3. Two randomized control trials evaluated the efficacy of DTBZ in treating tardive dyskinesia. The ARM-TD was a 12-week placebo-controlled trial. Patients were randomized to receive either DTBZ or a matching placebo and stratified by use of dopamine receptor antagonists. The primary endpoint was a change in the abnormal involuntary movement scale (AIMS). A total of 117 patients were randomized, 58 received DTBZ, and 59 received the placebo. DTBZ was titrated by 6 mg/day per week, if needed, to a maximum dose of 24 mg twice a day. The mean DTBZ dose at the end of the titration period was 38.8 mg/day. At 12 weeks, there was a statistically significant difference in the change mean of AIMS in the DTBZ group compared to the placebo at −3 versus −1.6.25 There was no significant difference between the placebo and DTBZ in regard to patient and clinical global impression of change (CGIC).25
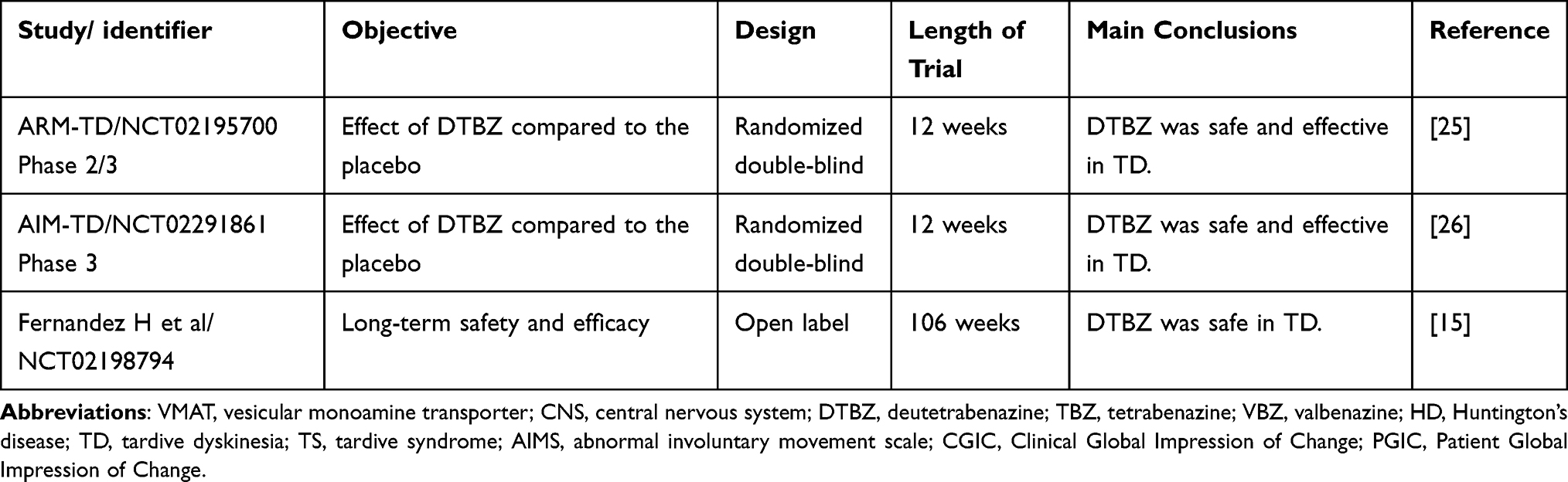 |
Table 3 Summary of Published Studies of Deutetrabenazine in Tardive Dyskinesia |
The AIM-TD was also a 12-week trial with similar inclusion and exclusion criteria as the ARM-TD study. This study included 298 patients who were randomized 1:1:1:1 with 12, 24, or 36 mg/day of DTBZ versus placebo. At 12 weeks, there was a statistically significant change in the mean AIMS score in the DTBZ group compared to the placebo group in patients taking 24 and 36 mg/day dosages. There were similar rates of adverse events between DTPC and the placebo.
To determine the long-term safety and tolerability of DTBZ, an open-label single-arm trial was conducted.15 This included 343 subjects; 111 were previously on a placebo, and 232 were previously on DTBZ. The patients were followed for a total of 106 weeks. Over the course of the trial, a total of 105 patients dropped out of the study. Furthermore, 233 patients experienced an adverse event. Of these, the most common were anxiety, somnolence, and depression. There were six deaths; three were considered unrelated to the study drug, and three were considered unlikely to be related to the study drug. Of those that were considered unlikely related to the study drug, the cause of death was cardiac arrest, ventricular tachycardia, and cardiopulmonary insufficiency.
There have been no head-to-head trials comparing VBZ versus DTBZ in treating TD. However, an indirect comparison was conducted using pooled data from published clinical trials.27 The clinical trials included were KINECT2 and 3 for the VBZ group and AIM-TD and ARM-TD for the DTBZ group.27 These trials were similar overall, except in study duration and some inclusion criteria. The study duration of the DTBZ trials was 12 weeks, while that for the VBZ trials was six weeks. In addition, participants were included in the DTBZ trials if they had an AIMS total score of more than six, while in the VBZ trials, they needed to have moderate to severe dyskinesia determined qualitatively. Lastly, VBZ allowed for the use of concomitant anticholinergics; however, DTBZ did not. In this indirect study, the mean change from baseline in AIMS total score favored VBZ 80 mg at 6 weeks over 24 and 36 mg doses of DTBZ at both 8 and 12 weeks.27 Statistical significance was reached when comparing VBZ 80 mg at six weeks and DTBZ 36 mg at 8 weeks. The AIMS response of more than 50% improvement favored VBZ over DTBZ in the pooled analysis; however, this was not statistically significant.27 Safety outcomes showed similar tolerability for both drugs.27 Based on this analysis, VBZ 80 mg per day might be more efficacious for TD symptoms than DTBZ. It may also yield a clinical response earlier than DTBZ. However, these results need to be interpreted with caution, as the studies were indirectly compared, and the studies included were not completely similar.
In conclusion, DTBZ had a significant response in improving dyskinesia in TD. It was generally well tolerated. Long-term safety and efficacy remain to be determined, given the high attrition rate in the long-term follow-up studies. In addition, true comparisons of DTBZ and VBZ in terms of efficacy in treating TD remain to be seen. It does seem that VBZ has the advantage of decreased dosing intervals, and faster effects. However, DTBZ allows for more titration.
Conclusion
Deutetrabenazine is safe and effective in the treatment of TD and chorea in HD in doses usually used up to 48 mg daily and for up to three years in duration. Indirect comparisons revealed relative superiority of DTBZ over TBZ in terms of safety, but direct comparisons of safety and efficacy between the VMAT2 and dopamine blocking agents is lacking. Until effective disease modifying therapies are available, symptomatic therapies will need to continue to be developed and improved.
Disclosure
SF received salary support as the medical monitor for the TETRA-HD trial and principal investigator for the FIRST-HD and ARC-HD trials. He has served as a consultant to Teva Pharmaceuticals. AA reports no conflicts of interest in this work.
References
1. Stahl SM. Neuronal traffic signals in tardive dyskinesia: not enough “stop” in the motor striatum. CNS Spectr. 2017;22(6):427–434. doi:10.1017/S109285291700061X
2. Frei K. Tardive dyskinesia: who gets it and why. Parkinsonism Relat Disord. 2019;59:151–154. doi:10.1016/j.parkreldis.2018.11.017
3. Wimalasena K. Vesicular monoamine transporters: structure-function, pharmacology, and medicinal chemistry. Med Res Rev. 2011;31(4):483–519. doi:10.1002/med.20187
4. Benarroch EE. Monoamine transporters. Structure Regulation Clin Implications. 2013;81(8):761–768.
5. Jankovic J. Dopamine depleters in the treatment of hyperkinetic movement disorders. Expert Opin Pharmacother. 2016;17(18):2461–2470. doi:10.1080/14656566.2016.1258063
6. Kenney C, Jankovic J. Tetrabenazine in the treatment of hyperkinetic movement disorders. Expert Rev Neurother. 2006;6(1):7–17. doi:10.1586/14737175.6.1.7
7. Reserpine [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Available from: https://www.ncbi.nlm.nih.gov/books/NBK557767/.
8. Termsarasab P. Chorea. Continuum. 2019;25(4):1001–1035. doi:10.1212/CON.0000000000000763
9. Citrome L. Tardive dyskinesia: placing vesicular monoamine transporter type 2 (VMAT2) inhibitors into clinical perspective. Expert Rev Neurother. 2018;18(4):323–332. doi:10.1080/14737175.2018.1455504
10. Niemann N, Jankovic J. Real-World Experience With VMAT2 Inhibitors. Clin Neuropharmacol. 2019;42(2):37–41. doi:10.1097/WNF.0000000000000326
11. Heo Y-A, Scott LJ. Deutetrabenazine: a Review in Chorea Associated with Huntington’s Disease. Drugs. 2017;77(17):1857–1864. doi:10.1007/s40265-017-0831-0
12. Sampaio C, Borowsky B, Reilmann R. Clinical trials in Huntington’s disease: interventions in early clinical development and newer methodological approaches. Mov Disorders. 2014;29(11):1419–1428. doi:10.1002/mds.26021
13. Citrome L. Deutetrabenazine for tardive dyskinesia: a systematic review of the efficacy and safety profile for this newly approved novel medication—What is the number needed to treat, number needed to harm and likelihood to be helped or harmed? Int J Clin Pract. 2017;71(11):46.
14. Richard A, Frank S. Deutetrabenazine in the treatment of Huntington’s disease. Neurodegener Dis Manag. 2019;9(1):31–37. doi:10.2217/nmt-2018-0040
15. Fernandez HH, Stamler D, Davis MD, et al. Long-term safety and efficacy of deutetrabenazine for the treatment of tardive dyskinesia. J Neurol Neurosurg Psychiatry. 2019;90(12):1317–1323. doi:10.1136/jnnp-2018-319918
16. Testa CM, Jankovic J. Huntington disease: a quarter century of progress since the gene discovery. J Neurol Sci. 2019;396:52–68. doi:10.1016/j.jns.2018.09.022
17. Bates GP, Dorsey R, Gusella JF, et al. Huntington disease. Nat Rev Dis Primers. 2015;1(1):15005.
18. Frank S, Testa CM, Stamler D; Huntington Study Group. Effect of Deutetrabenazine on Chorea Among Patients With Huntington Disease: a Randomized Clinical Trial. JAMA. 2016;316(1):40–50. doi:10.1001/jama.2016.8655
19. Rodrigues FB, Duarte GS, Costa J, Ferreira JJ, Wild EJ. Tetrabenazine Versus Deutetrabenazine for Huntington’s Disease: twins or Distant Cousins? Movement Disorders Clin Practice. 2017;4(4):582–585. doi:10.1002/mdc3.12483
20. Claassen DO, Carroll B, De Boer LM, et al. Indirect tolerability comparison of Deutetrabenazine and Tetrabenazine for Huntington disease. J Clin Mov Disord. 2017;4(3). doi:10.1186/s40734-017-0051-5
21. Frank S, Testa CM, Stamler D, et al. Long-Term Efficacy and Safety of Deutetrabenazine for Chorea in Huntington’s Disease: results From the ARC-HD Open-label Study. CNS Spectr. 2021;26(2):164–165. doi:10.1017/S1092852920002655
22. Huntington Study Group. Tetrabenazine as antichorea therapy in Huntington disease: a randomized controlled trial. Neurology. 2006;66(3):366–372. doi:10.1212/01.wnl.0000198586.85250.13
23. Frei K, Truong DD, Fahn S, Jankovic J, Hauser RA. The nosology of tardive syndromes. J Neurol Sci. 2018;389:10–16. doi:10.1016/j.jns.2018.02.008
24. Carbon M, Hsieh CH, Kane JM, Correll CU. Tardive Dyskinesia Prevalence in the Period of Second-Generation Antipsychotic Use: a Meta-Analysis. J Clin Psychiatry. 2017;78(3):e264–e78. doi:10.4088/JCP.16r10832
25. Fernandez HH, Factor SA, Hauser RA, et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: the ARM-TD study. Neurology. 2017;88(21):2003–2010. doi:10.1212/WNL.0000000000003960
26. Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Psychiatry. 2017;4(8):595–604. doi:10.1016/S2215-0366(17)30236-5
27. Aggarwal S, Serbin M, Yonan C. Indirect treatment comparison of valbenazine and deutetrabenazine efficacy and safety in tardive dyskinesia. J Comp Eff Res. 2019;8(13):1077–1088. doi:10.2217/cer-2019-0059
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.