Back to Journals » International Journal of General Medicine » Volume 19
Clinical Significance of the C-Reactive Protein-Triglyceride-Glucose Index in Cardiovascular Disease, Stroke, Cardiovascular-Kidney-Metabolic Syndrome, Cancer, Diabetes, and Osteoporosis: A Narrative Review
Authors Yang S, Yao X, Chai J, Lu H, Tang W, Wu Z ![]() , He W, Xie Y
, He W, Xie Y
Received 3 April 2026
Accepted for publication 28 May 2026
Published 5 June 2026 Volume 2026:19 614184
DOI https://doi.org/10.2147/IJGM.S614184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Satish Nair
Sheng Yang,* Xuxin Yao,* Jiali Chai, Haoxuan Lu, Wenbin Tang, Ziyi Wu, Wenming He, Yanqing Xie
Department of Cardiology, The First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang Province, 315000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanqing Xie, Department of Cardiology, The First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang Province, 315000, People’s Republic of China, Fax +86 1396834 2283, Email [email protected]
Objective: This narrative review aimed to summarize and critically appraise current evidence on the clinical significance of CTI in cardiovascular disease, stroke, cardiovascular-kidney-metabolic syndrome, cancer, diabetes, and osteoporosis.
Methods: PubMed and Web of Science databases were searched from January 2022, when CTI was first proposed, to January 2026. Search terms combined “C-reactive protein-triglyceride glucose index”, “CTI”, “CRP-TyG”, “insulin resistance”, “inflammation”, and disease-specific terms including cardiovascular disease, coronary heart disease, heart failure, stroke, cardiovascular-kidney-metabolic syndrome, cancer, diabetes, osteoporosis. Eligible studies reported CTI-specific clinical associations, prognostic performance, or relevant mechanistic evidence. Because this was a narrative review, no meta-analysis was performed.
Results: Current evidence is dominated by observational studies. Elevated CTI is consistently associated with higher cardiometabolic risk and poorer outcomes in cardiovascular disease, coronary heart disease, heart failure, stroke, cardiovascular-kidney-metabolic syndrome, cancer, and diabetes. Emerging data also suggest a potential relationship between higher CTI and reduced bone mineral density or osteoporosis, particularly among patients with type 2 diabetes mellitus. However, reported associations differ by glycometabolic status, disease stage, sex, age, and study design, and standardized CTI thresholds remain unavailable.
Conclusion: CTI is a simple, accessible index that may help characterize the inflammatory-metabolic burden underlying several chronic diseases. Its clinical value is most plausible as a complementary risk-stratification tool rather than a stand-alone diagnostic marker. Future studies should validate disease-specific thresholds, test whether CTI improves established prediction models, and determine whether interventions that reduce CTI translate into better clinical outcomes.
Keywords: C-reactive protein-triglyceride glucose index, insulin resistance, chronic disease, research progress
Introduction
With the accelerating ageing of the global population, the incidence and mortality of chronic diseases continue to rise, placing a substantial burden on public health systems worldwide. Cardiovascular disease (CVD),1 stroke,2 chronic kidney disease (CKD),3 cancer,4 and diabetes mellitus remain among the leading contributors to global morbidity and mortality.5 Although these conditions differ in clinical presentation and organ involvement, many share two interrelated pathophysiological processes: insulin resistance (IR) and chronic low-grade inflammation.6
The triglyceride-glucose (TyG) index has been widely used as a practical surrogate marker of IR because it is derived from routinely measured fasting triglycerides (TG) and fasting plasma glucose (FPG).7 In parallel, C-reactive protein (CRP) is a well-established clinical marker of systemic inflammation.8–10 However, metabolic dysfunction and inflammation rarely operate in isolation. Hyperglycemia, dyslipidemia, adipose tissue dysfunction, oxidative stress, and inflammatory cytokine activation can reinforce one another, producing a self-perpetuating inflammatory-metabolic cycle.11 Therefore, a single biomarker may not adequately capture the combined biological burden driving chronic disease progression.
Against this background, Ruan et al proposed the C-reactive protein-triglyceride-glucose index (CTI) in 2022 as a composite indicator integrating CRP with the TyG-related TG-FPG product. CTI is calculated as: CTI = 0.412 x ln[CRP (mg/L)] + ln[TG (mg/dL) x FPG (mg/dL)/2].12 In theory, this formula combines information on systemic inflammation, lipid metabolism, and glucose metabolism in a single logarithmic index.
Despite rapid growth in CTI-related studies, the current evidence base remains fragmented. Most studies are observational, disease-specific, and heterogeneous in study population, outcome definition, covariate adjustment, and proposed cut-off values. Some findings also appear to differ by glycometabolic status; for example, CTI may show stronger predictive value in non-diabetic or prediabetic individuals than in those with established diabetes, where competing vascular and metabolic risk factors may obscure its independent contribution. In addition, few studies have assessed dynamic or cumulative CTI exposure, and no randomized trial has established CTI as a modifiable therapeutic target. These uncertainties limit direct clinical translation.
Therefore, this narrative review aims to summarize and critically appraise current evidence on CTI in cardiovascular disease, stroke, cardiovascular-kidney-metabolic syndrome, cancer, diabetes, and osteoporosis; clarify the mechanistic rationale linking inflammation and metabolic dysfunction; compare consistent and inconsistent findings across disease areas; and identify practical limitations and future research priorities for clinical application (Table 1).
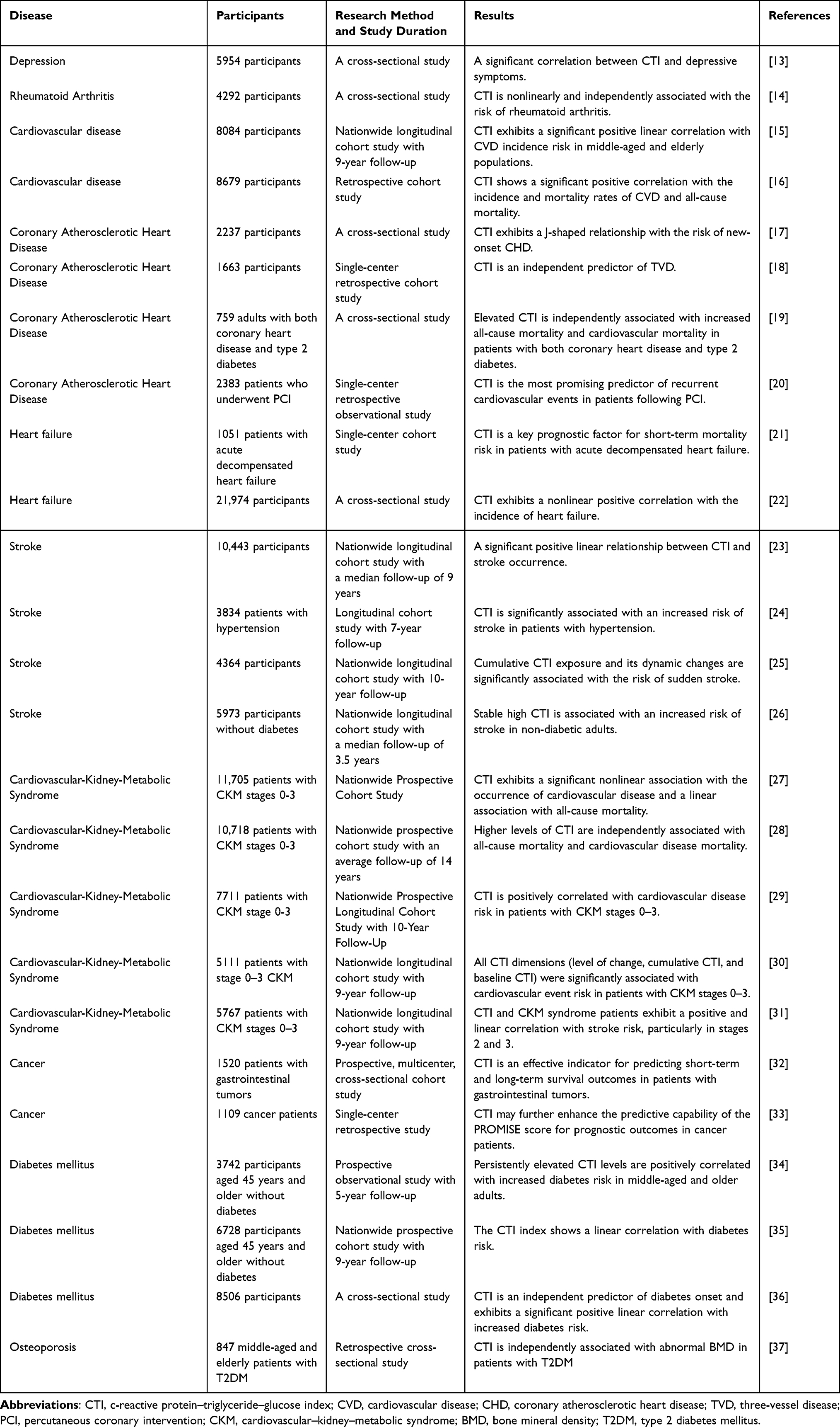 |
Table 1 The Relationship Between CTI and Different Diseases Was Summarized in Table |
Methods
Literature Search and Study Selection
This narrative review was conducted to summarize current clinical and mechanistic evidence regarding the C-reactive protein–triglyceride–glucose index (CTI) in major chronic diseases. A comprehensive literature search was performed using PubMed and Web of Science databases, covering publications from January 2022 to January 2026. The starting year was selected because CTI was first proposed in 2022.
The search strategy used both free-text terms and disease-related keywords. CTI-related terms included “C-reactive protein-triglyceride glucose index”, “CTI”, “CRP-TyG”, “insulin resistance”, “inflammation”. These terms were combined with disease-specific terms including “cardiovascular disease”, “coronary heart disease”, “heart failure”, “stroke”, “cardiovascular-kidney-metabolic syndrome”, “CKM”, “cancer”, “malignancy”, “diabetes”, “osteoporosis”. The reference lists of relevant articles were also manually screened to identify additional eligible studies.
Studies were considered eligible if they evaluated CTI calculated from C-reactive protein, triglycerides, and fasting plasma glucose, and if they reported CTI-related associations with disease risk, prognosis, mortality, disease severity, or other clinically relevant outcomes. Human studies involving adult populations were prioritized. Mechanistic studies were also included when they provided relevant evidence on inflammation, insulin resistance, metabolic dysfunction, endothelial injury, or chronic disease progression. Only English-language publications were included.
Duplicate records, conference abstracts without sufficient data, editorials, letters without original CTI-related evidence, and studies that did not specifically evaluate CTI were excluded. Non-human studies were excluded from the clinical synthesis but were used selectively as supportive mechanistic evidence when relevant. Studies in which C-reactive protein mainly reflected acute infection, trauma, perioperative inflammation, or other acute inflammatory conditions rather than chronic low-grade inflammation were also excluded.
Data Extraction and Evidence Synthesis
For each CTI-specific study, the following information was extracted: first author, publication year, data source, study design, study population, sample size, disease category, CTI calculation method, clinical outcomes, adjustment variables, dose–response or threshold findings, subgroup analyses, and main conclusions. The included studies were grouped according to disease category, including cardiovascular disease, coronary heart disease, heart failure, stroke, cardiovascular-kidney-metabolic syndrome, cancer, diabetes mellitus, and osteoporosis or osteopenia.
Because this study was designed as a narrative review rather than a systematic review or meta-analysis, no pooled effect estimates were calculated, and no formal risk-of-bias scoring system was applied. Greater interpretive weight was given to prospective studies, multicenter cohorts, large-sample analyses, and studies with comprehensive adjustment for potential confounders. The evidence synthesis focused on the consistency of findings, heterogeneity across populations, biological plausibility, disease-specific clinical relevance, and potential applicability of CTI in risk stratification and prognosis assessment.
C-Reactive Protein–Triglyceride–Glucose Index
The CTI is a novel composite biomarker first proposed by Ruan et al in 202212 This index was developed to integrate inflammatory and metabolic parameters into a unified mathematical model, thereby enabling a sensitive and specific assessment of systemic inflammatory burden and IR status. The CTI is calculated based on FPG, TG, and CRP levels, using the following formula: 0.412 × ln[CRP (mg/L)] + ln[TG (mg/dL) × FPG (mg/dL)/2]. As a comprehensive systemic evaluation tool, CTI has rapidly demonstrated promising clinical applicability in multiple disease domains, including cardiovascular diseases,38 stroke,26 malignancies,32 depression,13 and rheumatoid arthritis,14 by simultaneously capturing the dual characteristics of metabolic dysfunction and chronic inflammatory activation (Figure 1).
 |
Figure 1 Association of CTI index with different diseases. Created with BioGDP.com.39 Abbreviations: CTI, c-reactive protein–triglyceride–glucose index; FPG, fasting plasma glucose; TG, triglycerides; CRP, c-reactive protein; CHD, coronary atherosclerotic heart disease; CKM, cardiovascular–kidney–metabolic syndrome. |
The conceptual framework of CTI is grounded in the intricate and bidirectional interplay between inflammation and IR. First, CRP, a classical and widely used biomarker of systemic inflammation, has long been employed to evaluate the relationship between chronic inflammatory states and cardiovascular diseases. Substantial evidence indicates that elevated CRP levels are closely associated with an increased risk of acute cardiovascular events, such as myocardial infarction, and that its dynamic changes directly reflect the intensity of systemic inflammatory responses.40 Second, IR is not only a core pathological feature of type 2 diabetes mellitus (T2DM), but also a central driving force underlying multiple metabolic disorders and atherosclerotic cardiovascular diseases. Under conditions of IR, adipose tissue dysfunction leads to marked upregulation of pro-inflammatory cytokines, including tumor necrosis factor-α (TNF-α), monocyte chemoattractant protein-1 (MCP-1), interleukin-6 (IL-6), and CRP itself.
Importantly, metabolic abnormalities and inflammatory activation do not exist as independent processes, but rather form a self-perpetuating and mutually reinforcing “vicious cycle.” At the molecular level, this interaction is primarily mediated by the activation of key signaling pathways such as nuclear factor-kappa-B (NF-κB) and c-Jun N-terminal kinase (JNK). These pathways can be triggered by metabolic stress signals, including hyperglycemia and hyperlipidemia, leading to excessive production of inflammatory mediators. Conversely, sustained inflammatory responses further aggravate IR by impairing insulin signaling transduction.41 This deleterious feedback loop ultimately results in persistent endothelial dysfunction and accelerates the progression of atherosclerosis.
Compared with CRP alone or TyG alone, CTI may offer broader biological coverage because it captures both inflammatory and metabolic dimensions. Nevertheless, this does not mean that CTI should replace established biomarkers or risk models. Rather, current evidence supports its evaluation as a complementary tool that may improve risk stratification in selected populations after external validation, calibration, and determination of disease-specific thresholds.
CTI and Cardiovascular Disease
Cardiovascular disease (CVD) remains the leading cause of mortality worldwide and constitutes a major global public health burden. According to the World Health Organization, CVD accounts for approximately one-third of all deaths globally.42 Given the complex and multifactorial pathogenesis of CVD, the identification of reliable biomarkers for early risk stratification and prognostic evaluation in high-risk populations is of paramount clinical importance. In recent years, the CTI, as a novel comprehensive metabolic–inflammatory indicator, has attracted increasing attention in CVD risk assessment and outcome prediction owing to its unique ability to integrate systemic inflammation, lipid metabolism, and glucose metabolism into a single quantitative metric.
Several large-scale cohort studies have consistently confirmed a robust association between elevated CTI levels and increased CVD risk. Zhang et al demonstrated in a cohort of 8084 participants that CTI was significantly and positively associated with incident CVD in a dose–response manner Specifically, each one-unit increment in CTI was associated with a 44% increase in CVD risk (HR = 1.44, 95% CI: 1.17–1.78), and a significant stepwise increase in CVD incidence was observed across ascending CTI quartiles (P for trend < 0.001).15 Similarly, Sun et al further reported that CTI was not only a strong predictor of CVD mortality (HR = 228) and all-cause mortality (HR = 2.14), but was also closely associated with multiple adverse cardiovascular outcomes, including congestive heart failure (OR = 3.66), coronary heart disease (OR = 2.82), angina pectoris, acute myocardial infarction, and stroke. Notably, these associations remained robust and consistent across different age and sex subgroups, underscoring the stability and generalizability of CTI as a prognostic indicator.16
It is noteworthy that heterogeneity exists regarding the predictive performance of CTI among populations with different glycometabolic statuses. Zhang et al observed that the association between CTI and CVD risk was more pronounced in individuals aged 45–60 years, in women, and in those without chronic comorbidities15 In contrast, Sun et al found that although non-diabetic individuals with elevated CTI exhibited a markedly increased risk of CVD, this association failed to reach statistical significance in patients with diabetes mellitus16 This discrepancy may be attributable to the presence of profound metabolic disturbances, microvascular dysfunction, hypertension, and obesity in diabetic patients, which act as strong competing or confounding risk factors and may partially obscure the independent predictive value of CTI as a single composite marker. Collectively, these findings suggest that maintaining CTI within an optimal range may represent an effective strategy for reducing CVD incidence and related mortality, particularly in non-diabetic populations.
CTI and Coronary Atherosclerotic Heart Disease
Coronary atherosclerotic heart disease (CHD) is fundamentally a consequence of progressive atherosclerotic lesions within the coronary arteries. Its pathophysiological basis involves the dynamic interplay of multiple processes, including endothelial injury, lipid accumulation, chronic inflammatory activation, smooth muscle cell proliferation, and extracellular matrix remodeling. Together, these processes drive plaque formation, progression, and destabilization, ultimately leading to plaque rupture, thrombosis, and acute cardiovascular events.43 In recent years, the CTI, as a novel integrative inflammatory–metabolic indicator, has demonstrated substantial clinical value in risk prediction, disease severity assessment, and prognostic stratification of CHD.
Chen et al conducted the first systematic evaluation of the association between CTI and incident CHD in metabolically heterogeneous populations and revealed a J-shaped relationship between CTI levels and the risk of new-onset CHD Notably, this association was particularly pronounced among individuals classified as metabolically unhealthy normal weight (MUNW). Further mediation analyses indicated that the C-reactive protein–albumin–lymphocyte (CALLY) index partially mediated the association between CTI and CHD. Importantly, the predictive performance for incident CHD was significantly improved when CTI (≥ 9.887) and CALLY (< 1.221) were used in combination, highlighting the complementary value of integrated inflammatory–nutritional and metabolic assessment.17 These findings strongly support the potential utility of CTI for identifying high-risk CHD phenotypes within metabolically heterogeneous populations.
Beyond disease occurrence, CTI is also closely associated with the anatomical severity of coronary artery disease. Three-vessel disease (TVD), defined as ≥ 50% stenosis in the left anterior descending, left circumflex, and right coronary arteries, is generally indicative of more extensive coronary involvement and is associated with poorer prognosis and higher mortality.44 Available evidence suggests that CTI levels are significantly and positively correlated with the risk of TVD, particularly in male patients and those with diabetes mellitus.18 These observations indicate that CTI, as an integrated inflammatory–metabolic marker, exhibits relatively stable and robust predictive value for the severity of coronary artery disease across different clinical subgroups.
At the prognostic level, CTI appears to outperform traditional single metabolic or inflammatory markers. Recent studies have shown that in high-risk populations with concomitant CHD and type 2 diabetes mellitus, elevated CTI levels are independently and linearly associated with increased risks of both all-cause and cardiovascular mortality, even after comprehensive adjustment for demographic characteristics and clinical confounders.19 Compared with the TyG index alone, CTI incorporates an explicit assessment of systemic inflammatory status, thereby enabling more sensitive identification of vulnerable individuals who may not be adequately captured by conventional metabolic indices alone. Furthermore, CTI has demonstrated significant value in risk stratification for major adverse cardiovascular and cerebrovascular events (MACCEs) in patients undergoing percutaneous coronary intervention (PCI). Mechanistic analyses suggest that systemic inflammation plays a substantial mediating role in TyG-related MACCE risk, with CRP acting as a key mediator, further underscoring the critical contribution of inflammatory pathways to the adverse prognostic impact of metabolic dysfunction.20
CTI and Heart Failure
Heart failure (HF), as the terminal stage of multiple cardiovascular diseases, severely impairs patients’ quality of life and is associated with extremely high morbidity and mortality. With the continuous increase in the prevalence of underlying cardiovascular conditions such as hypertension, atrial fibrillation, and coronary heart disease, the HF population is not only expanding but also exhibiting a concerning trend toward younger age at onset. Accumulating evidence indicates that IR and chronic low-grade inflammation constitute central pathophysiological drivers in the initiation and progression of HF.45 A complex and bidirectional interaction exists between these two processes: chronic inflammation promotes ectopic lipid deposition through the autocrine and paracrine actions of inflammatory cells, thereby aggravating IR and forming a self-perpetuating “inflammation–metabolism” vicious cycle. Chronic inflammation may promote ectopic lipid deposition through adipose tissue dysfunction. Inflammatory mediators such as TNF-α, IL-6, IL-1β, and free fatty acids activate JNK, NF-kappaB, and related stress pathways, which impair insulin signaling and reduce the ability of adipocytes to safely store triglycerides. This promotes lipolysis and increases circulating free fatty acids. When subcutaneous adipose storage capacity is exceeded or dysfunctional, excess lipids accumulate in non-adipose tissues such as the liver, skeletal muscle, myocardium, pancreas, and epicardial or perivascular fat. These ectopic lipid intermediates further aggravate mitochondrial dysfunction, insulin resistance, and myocardial remodeling, thereby strengthening the biological rationale for CTI in heart failure risk assessment.46 This deleterious loop ultimately contributes to myocardial remodeling, structural abnormalities, and progressive functional deterioration.47
In the setting of acute decompensated heart failure (ADHF), prospective studies have demonstrated that the CTI plays a critical role in clinical risk stratification. Zhang et al reported that CTI levels in patients with ADHF were significantly and positively associated with short-term mortality risk, and that this risk gradient was further amplified in patients with concomitant diabetes mellitus, suggesting that metabolic–inflammatory interactions may synergistically worsen clinical outcomes in the presence of metabolic comorbidities That study systematically evaluated the combined effects of CTI and its individual components (the TyG index and CRP) on all-cause mortality risk. The results revealed a significant nonlinear positive association between CTI and 30-day all-cause mortality in ADHF patients (P = 0.02), with a distinct threshold effect observed in those with diabetes. In contrast, a more linear increasing trend was observed in non-diabetic ADHF patients (P = 0.72), indicating potential heterogeneity in risk patterns according to glycometabolic status.21
Beyond short-term prognosis, the relationship between CTI and the long-term risk of HF has also been substantiated in population-based studies. Available evidence indicates that each one-unit increment in CTI is associated with a 27.9% increase in the risk of incident HF, exhibiting a nonlinear dose–response relationship. Notably, when CTI reaches or exceeds 11.657, the association with HF risk shifts from moderate to strong, suggesting a clinically meaningful threshold effect. This finding implies that individuals with CTI ≥ 11.657 may represent a particularly high-risk subgroup and should be considered for intensified early screening and targeted preventive intervention strategies for HF.22
CTI and Stroke
Stroke is one of the leading causes of mortality and long-term disability worldwide and imposes a substantial burden on public health systems, particularly in the context of population ageing.48 Among the various subtypes, ischemic stroke represents the most prevalent pathological form and is characterized by a complex pathophysiological process involving inflammatory activation, oxidative stress, endothelial dysfunction, and cellular metabolic disturbances.49 Given the comprehensive ability of the CTI to reflect both vascular inflammatory status and systemic metabolic burden, increasing attention has been directed toward its potential application in stroke risk stratification and prevention.
Huo et al conducted a large-scale cohort study and were the first to demonstrate a significant and positive linear association between CTI levels and the risk of incident stroke Notably, this association remained robust and consistent across different sex subgroups and among middle-aged and older adults.23 In specific high-risk populations, Tang et al performed a 7-year prospective follow-up study involving 3834 hypertensive individuals without a prior history of stroke and found that each one-unit increase in CTI was associated with a 21% higher risk of stroke (HR = 121, 95% CI: 1.08–1.37). Moreover, compared with participants in the lowest quartile of CTI, those in the highest quartile exhibited a 66% higher risk of stroke.24 Collectively, these findings indicate that CTI serves as an independent and clinically meaningful predictor of stroke susceptibility, particularly in patients with hypertension.
Beyond baseline CTI levels, long-term cumulative exposure and dynamic changes in CTI appear to exert an even more profound influence on stroke risk. Yang et al introduced the cumulative effects of CTI (cuCTI) in a nationwide cohort study to quantify the long-term burden of metabolic and inflammatory dysregulation The results demonstrated a significant positive association between cuCTI and incident stroke, with individuals in the highest quartile showing a 90% higher risk compared with those in the lowest quartile (P < 0.001). Furthermore, trajectory analysis revealed that among non-diabetic individuals, only the “persistently elevated” CTI trajectory was significantly associated with an increased risk of stroke, whereas isolated or transient elevations in CTI did not confer a comparable risk. Mediation analyses further indicated that the adverse effect of persistently high CTI on stroke risk was partially mediated by hypertension (19.36%) and dyslipidemia (8.92%). These findings suggest that incorporating dynamic CTI measures into traditional risk prediction models may substantially enhance the accuracy of stroke risk assessment and underscore the importance of maintaining persistently low CTI levels over time.25
In addition, accumulating evidence suggests that the association between CTI and stroke risk is significantly modified by glycometabolic status. One study reported that in individuals with normal glucose tolerance or prediabetes, CTI was strongly and independently associated with stroke risk, whereas in patients with established diabetes mellitus, this association was markedly attenuated or even absent.23 This phenomenon may be attributable to the profound metabolic derangements, microvascular injury, and cumulative vascular toxicity inherent to diabetes itself, which may overshadow or mask the incremental predictive value of CTI as a composite indicator. Taken together, these observations suggest that CTI may be particularly useful for stroke risk screening and early prevention in non-diabetic and prediabetic populations.
CTI and Cardiovascular-Kidney-Metabolic Syndrome
Cardiovascular–Kidney–Metabolic syndrome (CKM) represents a systemic disorder driven by complex interactions among metabolic risk factors, CKD, and CVD. This syndrome results in multi-organ impairment and markedly increases the risk of adverse cardiovascular events and mortality. Its core pathophysiology involves a progressive cascade initiated by biological, social, and environmental exposures, culminating in adipose tissue dysfunction. This dysfunction, in turn, promotes systemic inflammation, oxidative stress, and IR, collectively forming the central mechanistic basis for CKM progression and deterioration.50
Ou et al were the first to explore the clinical value of the CTI in patients with CKM stages 0–3 Their study revealed a nonlinear association between CTI and CVD incidence, characterized by a distinct threshold effect with an inflection point around 8.602. Below this threshold, CVD risk increased sharply with rising CTI, whereas above the inflection point, the association weakened. Additionally, each one-unit increment in CTI was associated with a substantial increase in all-cause mortality risk, with some analyses indicating elevations as high as 111%, demonstrating a clear linear dose–response relationship. Importantly, CTI’s prognostic utility remained independent of estimated glomerular filtration rate (eGFR). Although eGFR declines progressively with advancing CKD stages, CTI retained significant risk stratification capability within eGFR-matched strata, suggesting that CTI captures upstream pathophysiological drivers—such as systemic inflammation and metabolic dysregulation—rather than merely reflecting downstream renal dysfunction.27 Age-stratified analyses further revealed that CTI’s predictive value for mortality was more pronounced in individuals under 60 years old, highlighting its potential utility for early risk identification and timely intervention.28
In addition, cuCTI provides insight into the long-term inflammatory and metabolic burden in CKM populations. One cohort study demonstrated that each one-unit increase in cuCTI was associated with a 16% increase in CVD risk (HR = 1.16, 95% CI: 1.06–1.27), and individuals in the highest quartile exhibited a 42% higher risk compared with the lowest quartile.29 Long-term cumulative exposure further amplified risk: each standard deviation increase in cuCTI corresponded to a 21% higher CVD risk, slightly exceeding the 18% risk predicted by baseline CTI alone.30 These findings underscore the importance of maintaining low CTI levels over time to improve long-term prognosis. Gender-specific analyses revealed slightly higher hazard ratios in women (HR = 1.25) than in men (HR = 1.23), potentially reflecting the predominantly perimenopausal or postmenopausal age structure of the cohort. Estrogen is known to exert vasoprotective effects through enhanced endothelial nitric oxide production, anti-inflammatory actions, and regulation of lipid metabolism; postmenopausal estrogen decline may render women more susceptible to the inflammatory–metabolic burden captured by CTI.29
The predictive value of CTI extends to cerebrovascular outcomes. Studies examining stroke incidence within CKM populations demonstrated a significant positive association between elevated CTI levels and stroke risk (HR = 1.33). Notably, CTI outperformed the TyG index alone in predicting both 5-year and 7-year stroke risk. Stage-stratified analyses further revealed that the association between CTI and stroke was significant in patients with CKM stage 2 (HR = 1.27) and stage 3 (HR = 1.25), but not in those with stages 0–1.31 This stage-specific effect likely reflects the fact that metabolic and inflammatory impairments in early-stage CKM have not yet reached the threshold necessary to induce cerebrovascular injury, whereas in later stages, the cumulative effects of insulin resistance and chronic inflammation allow CTI’s predictive capacity to be fully manifested.
CTI and Cancer
Chronic inflammation and insulin resistance are recognized as key drivers in the initiation, progression, and prognosis of malignant tumors.51 As a novel composite indicator integrating systemic inflammatory burden with metabolic dysfunction, the CTI has gained increasing attention for its potential role in tumor prognosis assessment. Ruan et al demonstrated that CTI exhibits superior predictive performance compared with either CRP or the TyG index alone in evaluating cancer patient outcomes, suggesting that it more comprehensively captures disruptions in the immune–metabolic tumor microenvironment.52
Multiple studies have confirmed the independent prognostic value of CTI in malignant tumors. In a large multicenter study involving 1520 patients with gastrointestinal malignancies, CTI was shown to reliably predict both short-term and long-term survival outcomes. Elevated CTI levels were significantly associated with increased mortality risk in patients with both upper and lower gastrointestinal tumors (HR = 1.51–1.98) and demonstrated superior discriminatory ability in predicting 90-day and 180-day mortality rates.32 Similarly, Uyar et al reported in a large cohort of patients admitted for unplanned hospitalizations that high CTI independently predicted 90-day all-cause mortality (OR = 285). Importantly, when CTI was combined with the established PROMISE score, predictive accuracy for short-term mortality was substantially enhanced, indicating that CTI can serve not only as an independent prognostic marker but also as a valuable complement to existing clinical assessment tools. This integration enables more precise risk stratification and may guide timely intervention strategies for high-risk oncology patients.33
CTI and Diabetes Mellitus
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by impaired glucose homeostasis, which, over time, leads to a spectrum of complications including retinopathy, neuropathy, cardiovascular disease, and diabetic nephropathy. In 2021, DM accounted for approximately 170,000 deaths in China.53
Emerging evidence highlights the prognostic value of the CTI in predicting new-onset diabetes. A 5-year prospective cohort study demonstrated that each one-unit increase in baseline CTI was associated with a 35% higher risk of developing diabetes (HR = 1.35). Moreover, individuals with “persistently high” CTI exposure exhibited a 2.25-fold higher incidence of diabetes compared with those maintaining “persistently low” levels.34 These findings indicate that CTI reflects not merely transient metabolic fluctuations, but rather the cumulative burden of chronic inflammation and metabolic stress, which is a key factor in pancreatic β-cell dysfunction and progressive glucose intolerance.
A 9-year follow-up study by Shan et al further confirmed that CTI outperforms the TyG index alone in predicting incident diabetes, emphasizing the added value of incorporating CRP as an inflammatory marker to complement traditional metabolic indicators35 Consistently, a large-scale analysis based on the NHANES database demonstrated a robust linear positive association between CTI levels and diabetes prevalence, with evidence of a gender-specific interaction effect. A nomogram derived from these data exhibited excellent discriminatory ability in the validation cohort (AUC = 0.92), highlighting the potential of CTI as a precise screening tool for early identification of individuals at high risk due to chronic inflammation and metabolic dysregulation.36
CTI and Osteoporosis
Osteoporosis and osteopenia are common age-related metabolic bone disorders characterized by reduced bone mineral density (BMD), deterioration of bone microarchitecture, and increased susceptibility to fragility fractures.54 Although traditionally regarded as skeletal disorders, increasing evidence suggests that bone metabolism is closely associated with systemic inflammation, insulin resistance, adipokine imbalance, oxidative stress, and diabetes-related vascular injury. These pathophysiological processes substantially overlap with the inflammatory-metabolic pathways reflected by the CTI.
Direct evidence regarding the association between CTI and bone health remains limited but is emerging. A recent retrospective cross-sectional study involving 847 middle-aged and elderly patients with type 2 diabetes mellitus directly investigated the relationship between CTI and osteoporosis. In that study, CTI levels were significantly higher in patients with abnormal BMD than in those with normal BMD, and the prevalence of osteoporosis increased progressively across CTI quartiles. CTI was also negatively correlated with BMD. After adjustment for potential confounders, elevated CTI remained independently associated with an increased risk of osteoporosis, and receiver operating characteristic analysis demonstrated moderate discriminatory ability for identifying abnormal BMD.37 However, because the current evidence is derived from a single-center cross-sectional study in patients with type 2 diabetes mellitus, further prospective and multicenter studies are required to determine whether CTI can predict incident osteoporosis, accelerated BMD loss, or fragility fractures in broader populations.
Several mechanisms may explain this association. Hyperglycemia and insulin resistance can impair osteoblast differentiation, promote advanced glycation end-product accumulation, and reduce bone formation.55,56 Chronic inflammation may further enhance osteoclastogenesis and bone resorption through cytokines such as TNF-α, IL-6, and IL-1β.57,58 CRP-related inflammatory activity may also reflect an immune-metabolic environment that favors bone loss.57 Furthermore, studies using insulin-resistance surrogate markers, such as the triglyceride-glucose body mass index and other insulin-resistance indices, have reported associations with BMD and osteoporosis-related risk, supporting the biological plausibility that metabolic dysfunction contributes to skeletal fragility.59,60 Therefore, CTI may represent an integrated marker linking diabetes, inflammation, and skeletal fragility.
Nevertheless, these findings should be interpreted with caution. Existing CTI-BMD evidence is primarily cross-sectional and concentrated in patients with type 2 diabetes mellitus; therefore, causality, fracture-prediction performance, sex-specific applicability, and generalizability to non-diabetic populations remain uncertain.37 At present, CTI should be considered a potential adjunctive indicator of inflammatory-metabolic risk rather than a replacement for dual-energy X-ray absorptiometry, fracture assessment tool, or established osteoporosis risk-assessment tools. Future studies should determine whether CTI predicts incident fractures, improves existing fracture-risk models, and whether reductions in CTI are associated with preservation of BMD or reduced skeletal risk.
Discussion
This review demonstrates that CTI is a biologically plausible and clinically accessible biomarker that reflects inflammation-metabolic dysregulation across a wide range of chronic disease categories. The available evidence most consistently supports associations between elevated CTI and adverse cardiovascular outcomes, stroke risk, cardiovascular-kidney-metabolic syndrome–related events, cancer prognosis, incident diabetes mellitus, and osteoporosis. These findings support the view that, in the progression of chronic diseases, inflammation and insulin resistance act synergistically rather than independently.
However, the evidence is not uniform. First, the magnitude and shape of associations vary across studies. Some studies report linear associations, whereas others identify nonlinear or threshold effects. Second, diabetes status appears to modify the predictive value of CTI in several settings. In non-diabetic or prediabetic individuals, CTI may identify early inflammatory-metabolic risk, whereas in established diabetes, long-standing hyperglycemia, microvascular injury, renal dysfunction, obesity, and medication effects may reduce the incremental predictive contribution of CTI. Third, the clinical thresholds proposed in individual studies are not interchangeable because of differences in population characteristics, assay platforms, outcome definitions, and statistical modeling. These issues explain why CTI should not yet be used as a stand-alone diagnostic or treatment-decision tool.
The most important modifiable factor for reducing CTI has not been established in interventional trials. Mathematically, because TG and FPG enter the logarithmic metabolic term with greater direct weighting than CRP, proportional reductions in TG and FPG would be expected to reduce CTI more than the same proportional reduction in CRP. Biologically, however, the components are interdependent: weight loss, regular physical activity, improved diet quality, reduced visceral adiposity, better glycemic control, triglyceride lowering, and treatment of chronic inflammatory conditions may reduce CTI simultaneously. Therefore, the most practical strategy is not to target a single component in isolation, but to reduce the upstream drivers of insulin resistance and chronic inflammation.
The clinical value of CTI will depend on whether it adds information beyond established risk models. Future studies should test incremental discrimination, calibration, decision-curve benefit, and reclassification when CTI is added to conventional predictors such as age, sex, blood pressure, lipid profile, glycemic status, kidney function, smoking, body mass index, and disease-specific scores. In addition, longitudinal studies should distinguish baseline CTI from cumulative CTI exposure and dynamic CTI trajectories, because persistent inflammatory-metabolic burden may be more clinically relevant than a single measurement.
Several limitations must be acknowledged. CTI incorporates CRP, an acute-phase reactant that can be elevated by infection, trauma, autoimmune disease, cancer activity, or recent procedures. CTI also does not identify the source of inflammation, the type of lipid abnormality, or the specific mechanism of insulin resistance. Most available studies are observational, so residual confounding and reverse causality cannot be excluded. Finally, the formula requires standardized measurement units and careful handling of low or undetectable CRP values because logarithmic transformation is used. These limitations should be clearly considered before CTI is translated into routine clinical practice.
Conclusion
CTI is an accessible composite biomarker that integrates CRP, TG, and FPG to reflect the combined inflammatory and metabolic burden underlying multiple chronic diseases. Current evidence suggests that elevated CTI is associated with higher risk or poorer prognosis in cardiovascular disease, stroke, CKM syndrome, cancer, diabetes, and possibly osteoporosis. The major contribution of this review is to synthesize these rapidly expanding disease-specific findings into a unified inflammatory-metabolic framework and to clarify where the evidence is consistent, where it is heterogeneous, and where clinical translation remains premature.
At present, CTI should be viewed as a complementary risk-stratification tool rather than a stand-alone diagnostic marker or therapeutic target. Before routine clinical use, future studies should establish standardized disease-specific thresholds, validate CTI in diverse populations, evaluate whether it improves established risk models, and determine whether interventions that reduce CTI can improve clinical outcomes. These steps are essential for moving CTI from an observational biomarker toward a clinically actionable indicator of chronic inflammatory-metabolic risk.
Abbreviations
CTI, c-reactive protein–triglyceride–glucose index; CVD, cardiovascular disease; CKD, chronic kidney disease; IR, insulin resistance; TyG, triglyceride–glucose; CRP, c-reactive protein; TG, triglycerides; FPG, fasting plasma glucose; T2DM, type 2 diabetes mellitus; TNF-α, tumor necrosis factor-α; MCP-1, monocyte chemoattractant protein-1; IL-6, interleukin-6; NF-κB, nuclear factor-kappa-B; JNK, c-Jun N-terminal kinase; HR, hazard ratio; Cl, confidence interval; OR, odds ratio; CHD, coronary atherosclerotic heart disease; MUNW, metabolically unhealthy normal weight; CALLY, c-reactive protein–albumin–lymphocyte; TVD, three-vessel disease; MACCE, major adverse cardiovascular and cerebrovascular events; PCI, percutaneous coronary intervention; HF, heart failure; ADHF, acute decompensated heart failure; cuCTI, cumulative effects of c-reactive protein–triglyceride–glucose index; CKM, cardiovascular–kidney–metabolic syndrome; eGFR, estimated glomerular filtration rate; DM, diabetes mellitus; AUC, area under the curve; BMD, bone mineral density.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by International Sci-tech Cooperation Projects under the “Innovation Yong jiang 2035” (2024H010).
Disclosure
The authors declare no conflicts of interest related to this review article.
References
1. Global Burden of Cardiovascular Diseases and Risks 2023 Collaborators. Global, Regional, and National Burden of Cardiovascular Diseases and Risk Factors in 204 Countries and Territories, 1990-2023. J Am College Cardiol. 2025;86(22):2167–14. doi:10.1016/j.jacc.2025.08.015
2. Yang S, Deng M, Ren X, et al. Global burden of disease study highlights the global, regional and national trends of stroke. J Neurol Neurosurg. 2025;97(1):13–24. doi:10.1136/jnnp-2025-335954
3. Mark PB, Stafford LK, Grams ME. Global, regional, and national burden of chronic kidney disease in adults, 1990-2023, and its attributable risk factors: a systematic analysis for the Global Burden of Disease Study 2023. Lancet. 2025;406(10518):2461–2482. doi:10.1016/S0140-6736(25)01853-7
4. LM Force, JM Kocarnik, ML May. The global, regional, and national burden of cancer, 1990-2023, with forecasts to 2050: a systematic analysis for the Global Burden of Disease Study 2023. Lancet. 2025;406(10512):1565–1586. doi:10.1016/S0140-6736(25)01635-6
5. Chew NWS, Ng CH, Tan DJH, et al. The global burden of metabolic disease: data from 2000 to 2019. Cell Metab. 2023;35(3):414–428.e413. doi:10.1016/j.cmet.2023.02.003
6. Dhondge RH, Agrawal S, Patil R, Kadu A, Kothari M. A Comprehensive Review of Metabolic Syndrome and Its Role in Cardiovascular Disease and Type 2 Diabetes Mellitus: mechanisms, Risk Factors, and Management. Cureus. 2024;16(8):e67428. doi:10.7759/cureus.67428
7. Sánchez-García A, Rodríguez-Gutiérrez R, Mancillas-Adame L, et al. Diagnostic Accuracy of the Triglyceride and Glucose Index for Insulin Resistance: a Systematic Review. Int J Endocrinol. 2020;2020:4678526. doi:10.1155/2020/4678526
8. Kraaijenhof JM, Nurmohamed NS, Nordestgaard AT, et al. Low-density lipoprotein cholesterol, C-reactive protein, and lipoprotein(a) universal one-time screening in primary prevention: the EPIC-Norfolk study. Eur Heart J. 2025;46(39):3875–3884. doi:10.1093/eurheartj/ehaf209
9. Nowak KL, Chonchol M. Targeting Inflammation in CKD. Am J Kidney Dis. 2025;86(6):803–813. doi:10.1053/j.ajkd.2025.06.019
10. Feng JR, Li X, Han C, et al. C-Reactive Protein Induces Immunosuppression by Activating FcγR2B in Pulmonary Macrophages to Promote Lung Metastasis. Cancer Res. 2024;84(24):4184–4198. doi:10.1158/0008-5472.CAN-24-0253
11. Chen Y, Huang T, Wang J, Guo C, Gao J, Feng X. Association between C-reactive protein-triglyceride glucose index and risk of sarcopenia in older adults: findings from CHARLS and NHANES. Exp Gerontology. 2025;213:113003. doi:10.1016/j.exger.2025.113003
12. Ruan GT, Xie HL, Zhang HY, et al. A Novel Inflammation and Insulin Resistance Related Indicator to Predict the Survival of Patients With Cancer. Front Endocrinol. 2022;13:905266. doi:10.3389/fendo.2022.905266
13. Huang C, You H, Zhang Y, et al. Association between C-reactive protein-triglyceride glucose index and depressive symptoms in American adults: results from the NHANES 2005 to 2010. BMC Psychiatry. 2024;24(1):890. doi:10.1186/s12888-024-06336-4
14. Xie H, Liu Q, Xu X, et al. Nonlinear Association Between the C-Reactive Protein-Triglyceride-Glucose Index and Rheumatoid Arthritis Risk: the Mediating Role of Body Mass Index. Mediators Inflammation. 2025;2025(1):8729780. doi:10.1155/mi/8729780
15. Zhang L, Li S, Liu D, et al. The relationship between C-reactive protein-triglyceride-glucose index and cardiovascular disease: insights from the China health and retirement longitudinal study (CHARLS). Cardiovascular Diabetol. 2025;24(1):410. doi:10.1186/s12933-025-02960-w
16. Sun Y, Guo Y, Ma S, et al. Association of C-reactive protein-triglyceride glucose index with the incidence and mortality of cardiovascular disease: a retrospective cohort study. Cardiovascular Diabetol. 2025;24(1):313. doi:10.1186/s12933-025-02835-0
17. Chen Y, Jia W, Guo J, et al. Association between the C-reactive protein-triglyceride glucose index and new-onset coronary heart disease among metabolically heterogeneous individuals. Cardiovascular Diabetol. 2025;24(1):316. doi:10.1186/s12933-025-02876-5
18. Hou L, Li Y, Liu Q. C-reactive protein-triglyceride glucose index in predicting three-vessel coronary artery disease risk: a retrospective study using machine learning approaches. Annals Med. 2025;57(1):2584308. doi:10.1080/07853890.2025.2584308
19. Tang N, Chen X, Li H, et al. Association of C reactive protein triglyceride glucose index with mortality in coronary heart disease and type 2 diabetes from NHANES data. Sci Rep. 2025;15(1):24687. doi:10.1038/s41598-025-10184-x
20. Gao A, Peng B, Gao Y, et al. Evaluation and comparison of inflammatory and insulin resistance indicators on recurrent cardiovascular events in patients undergoing percutaneous coronary intervention: a single center retrospective observational study. Diabetol Metab Syndr. 2025;17(1):157. doi:10.1186/s13098-025-01687-8
21. Zhang N, Xie L, Zhang S, et al. Inflammatory storm and metabolic disorders: unraveling heterogeneity in mortality risk for comorbid diabetes mellitus and heart failure via the C-reactive protein-triglyceride-glucose index. Front Endocrinol. 2025;16:1689238. doi:10.3389/fendo.2025.1689238
22. Cheng N, Ma Z, Chen Y, Jin L, Chen L. C-reactive protein-triglyceride glucose index and heart failure in US adults from NHANES 2001-2010. Sci Rep. 2025;15(1):26363. doi:10.1038/s41598-025-08389-1
23. Huo G, Tang Y, Liu Z, Cao J, Yao Z, Zhou D. Association between C-reactive protein-triglyceride glucose index and stroke risk in different glycemic status: insights from the China Health and Retirement Longitudinal Study (CHARLS). Cardiovascular Diabetol. 2025;24(1):142. doi:10.1186/s12933-025-02686-9
24. Tang S, Wang H, Li K, et al. C-reactive protein-triglyceride glucose index predicts stroke incidence in a hypertensive population: a national cohort study. Diabetol Metab Syndr. 2024;16(1):277. doi:10.1186/s13098-024-01529-z
25. Yang Y, Liu A. Associations of cumulative exposure and dynamic trajectories of the C-reactive protein-triglyceride-glucose index with incident stroke in middle-aged and older Chinese adults: a longitudinal analysis based on CHARLS. Cardiovascular Diabetol. 2025;24(1):386. doi:10.1186/s12933-025-02945-9
26. Li J, Tian X, Zhao D, Zhong L. Change in C-reactive protein-triglyceride glucose index and risk of stroke among middle-aged and older adults free of diabetes: a national cohort study. NMCD. 2025;35(12):104372. doi:10.1016/j.numecd.2025.104372
27. Ou H, Wei M, Li X, Xia X. C-reactive protein-triglyceride glucose index in evaluating cardiovascular disease and all-cause mortality incidence among individuals across stages 0-3 of cardiovascular-kidney-metabolic syndrome: a nationwide prospective cohort study. Cardiovascular Diabetol. 2025;24(1):296. doi:10.1186/s12933-025-02848-9
28. Ying Q, He F, Wu L, Wei Q, Xu J. C-reactive protein-triglyceride glucose index predicts mortality in cardiovascular-kidney-metabolic syndrome stage 0-3: a prospective cohort study. Diabetol Metab Syndr. 2025;17(1):382. doi:10.1186/s13098-025-01947-7
29. Lu Z, Li L, Wang X, Lv L, Rong S, Li B. Association between C-reactive protein-triglyceride glucose index and Future cardiovascular disease risk in a population with cardiovascular-Kidney-metabolic syndrome stage 0–3. Sci Rep. 2025;15(1):31152. doi:10.1038/s41598-025-17173-0
30. Chen J, Yan L, He L, Wang W. Association between different dimensions of the C-reactive protein-triglyceride-glucose index and future cardiovascular disease risk in individuals with cardiovascular-kidney-metabolic syndrome stages 0-3: a nationwide cohort study. Diabetol Metab Syndr. 2025;17(1):299. doi:10.1186/s13098-025-01882-7
31. Xu Y, Chen S, Zhu J, et al. C-reactive protein-triglyceride glucose index and stroke risk in early cardiovascular-kidney-metabolic syndrome: a National cohort study. BMC Cardiovascular Disorders. 2025;25(1):634. doi:10.1186/s12872-025-05143-3
32. Ruan GT, Shi JY, Xie HL, et al. Prognostic importance of an indicator related to systemic inflammation and insulin resistance in patients with gastrointestinal cancer: a prospective study. Front Oncol. 2024;14:1394892. doi:10.3389/fonc.2024.1394892
33. Uyar GC, Mirallas O, Başkurt K, et al. Prediction of 90-day mortality among cancer patients with unplanned hospitalisation: a retrospective validation study of three prognostic scores. Lancet Regional Health Europe. 2025;54:101317. doi:10.1016/j.lanepe.2025.101317
34. Zhou YF, Zeng QT, Zhang XT, Wang FX. Cumulative of c-reactive protein-triglyceride glucose index exposure and risk of diabetes in middle-aged and older Chinese adults: findings from a national longitudinal cohort. Diabetol Metab Syndr. 2025;18(1). doi:10.1186/s13098-025-02056-1
35. Shan Y, Liu Q, Gao T. Application of the C-reactive protein-triglyceride glucose index in predicting the risk of new-onset diabetes in the general population aged 45 years and older: a national prospective cohort study. BMC Endocr Disord. 2025;25(1):126. doi:10.1186/s12902-025-01947-8
36. Xi L, Zhao J, Wang Y. Determining the association of C-reactive-protein-triglyceride-glucose index and diabetes using machine learning and LASSO regression: a cross-sectional analysis of NHANES 2001 to 2010 results. Medicine. 2025;104(38):e44815. doi:10.1097/MD.0000000000044815
37. Zhang Y, Jing Y. Association between C-reactive protein-triglyceride glucose index and abnormal BMD in middle-aged and elderly patients with type 2 diabetes mellitus: a cross-sectional study. Front Med. 2025;12:1615596. doi:10.3389/fmed.2025.1615596
38. Zheng R, Wang T, Liu M, Cao X. Relationship between C-reactive protein triglyceride glucose index and cardiovascular disease risk: a cross-sectional analysis with machine learning. BMC Med Inf Decis Making. 2025;25(1):424. doi:10.1186/s12911-025-03265-4
39. Jiang SLH, Zhang L. Generic Diagramming Platform (GDP): a comprehensive database of high-quality biomedical graphics. Nucleic Acids Res. 2025;53(D1):D1670–D1676. doi:10.1093/nar/gkae973.
40. Daios S, Anastasiou V, Moysidis DV, et al. The Prognostic Role of C-Reactive Protein Velocity in Patients with First Acute Myocardial Infarction. J Clin Med. 2025;14(21):7633. doi:10.3390/jcm14217633
41. Zhang B, Gu Y, Chen Y, et al. Association between C-reactive protein-triglyceride glucose index and testosterone levels among adult men: analyses of NHANES 2015-2016 data. Sexual Med. 2025;13(1):qfaf012. doi:10.1093/sexmed/qfaf012
42. Roth GA, Mensah GA, Fuster V. The Global Burden of Cardiovascular Diseases and Risks: a Compass for Global Action. J Am College Cardiol. 2020;76(25):2980–2981. doi:10.1016/j.jacc.2020.11.021
43. Zaman S, Wasfy JH, Kapil V, et al. The Lancet Commission on rethinking coronary artery disease: moving from ischaemia to atheroma. Lancet. 2025;405(10486):1264–1312. doi:10.1016/S0140-6736(25)00055-8
44. Min JK, Dunning A, Lin FY, et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: an International Multicenter Registry) of 23,854 patients without known coronary artery disease. J Am College Cardiol. 2011;58(8):849–860. doi:10.1016/j.jacc.2011.02.074
45. Lopaschuk GD, Karwi QG, Tian R, Wende AR, Abel ED. Cardiac Energy Metabolism in Heart Failure. Circulation Res. 2021;128(10):1487–1513. doi:10.1161/CIRCRESAHA.121.318241
46. Gkrinia EMM, Belančić A. The Mechanisms of Chronic Inflammation in Obesity and Potential Therapeutic Strategies: a Narrative Review. Curr Iss Mol Biol. 2025;47(5):357. doi:10.3390/cimb47050357
47. Wu H, Ballantyne CM. Metabolic Inflammation and Insulin Resistance in Obesity. Circulation Res. 2020;126(11):1549–1564. doi:10.1161/CIRCRESAHA.119.315896
48. Li XY, Lv JJ, Zhao Y, et al. Global Burden of Stroke Attributable to Low Physical Activity/High Body Mass Index Among People Aged 55 Years and Older. Stroke. 2024;55(8):2075–2085. doi:10.1161/STROKEAHA.123.046180
49. Pacinella G, Bona MM, Todaro F, Ciaccio AM, Daidone M, Tuttolomondo A. Tracing Inflammation in Ischemic Stroke: biomarkers and Clinical Insight. Int J Mol Sci. 2025;26(19):9801. doi:10.3390/ijms26199801
50. Ndumele CE, Rangaswami J, Chow SL, et al. Cardiovascular-Kidney-Metabolic Health: a Presidential Advisory From the American Heart Association. Circulation. 2023;148(20):1606–1635. doi:10.1161/CIR.0000000000001184
51. Lee DY, Rhee EJ, Chang Y, et al. Impact of systemic inflammation on the relationship between insulin resistance and all-cause and cancer-related mortality. Metabolism. 2018;81:52–62. doi:10.1016/j.metabol.2017.11.014
52. Ruan GT, Deng L, Xie HL, et al. Systemic inflammation and insulin resistance-related indicator predicts poor outcome in patients with cancer cachexia. Cancer Metabol. 2024;12(1):3. doi:10.1186/s40170-024-00332-8
53. Chen Y, Wang G, Hou Z, Liu X, Ma S, Jiang M. Comparative diabetes mellitus burden trends across global, Chinese, US, and Indian populations using GBD 2021 database. Sci Rep. 2025;15(1):11955. doi:10.1038/s41598-025-96175-4
54. Ensrud KE, Crandall CJ. Osteoporosis. Ann Internal Med. 2024;177(1):Itc1–itc16. doi:10.7326/AITC202401160
55. Ravindran S, Wong SK, Mohamad NV, Chin KY. A Review of the Relationship Between Insulin and Bone Health. Biomedicines. 2025;13(6):1504. doi:10.3390/biomedicines13061504
56. Upadhyay P, Kumar S. Diabetes and Bone Health: a Comprehensive Review of Impacts and Mechanisms. Diabetes/Metab Res Rev. 2025;41(5):e70062. doi:10.1002/dmrr.70062
57. Ye W, Cheng S, Xiao J, Yu H. High-sensitivity C-reactive protein could be a potential indicator of bone mineral density in adolescents aged 10-20 year. Sci Rep. 2022;12(1):7119. doi:10.1038/s41598-022-11209-5
58. Zhivodernikov IV, Kirichenko TV, Markina YV, Postnov AY, Markin AM. Molecular and Cellular Mechanisms of Osteoporosis. Int J Mol Sci. 2023;24(21). doi:10.3390/ijms242115772
59. Wen Z, Li Y, Xu L, et al. Triglyceride Glucose-Body Mass Index Is a Reliable Indicator of Bone Mineral Density and Risk of Osteoporotic Fracture in Middle-Aged and Elderly Nondiabetic Chinese Individuals. J Clin Med. 2022;11(19):5694. doi:10.3390/jcm11195694
60. Li M, Gao L, Liu Y, et al. Relationship between insulin resistance surrogates and bone mineral density in postmenopausal women. Climacteric. 2025;28(2):154–161. doi:10.1080/13697137.2025.2455164
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.