")
Back to Journals » Clinical Ophthalmology » Volume 17
Clinical Risk Score for Prediction of Urgency in Carotid Cavernous Sinus Fistulas
Authors Supasai P, Kanjana K, Yospaiboon Y
Received 31 May 2023
Accepted for publication 5 July 2023
Published 10 July 2023 Volume 2023:17 Pages 1945—1952
DOI https://doi.org/10.2147/OPTH.S419844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pawasoot Supasai, Kanwasee Kanjana, Yosanan Yospaiboon
KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Yosanan Yospaiboon, KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, 123 Mitraparb Highway, Khon Kaen, 40002, Thailand, Tel +66-4336-3010, Fax +66-4334-8383, Email [email protected]
Purpose: To develop a clinical risk score for the prediction of urgency in patients with carotid cavernous sinus fistulas (CCFs) and test for the discriminative ability of the diagnostic prediction.
Methods: The medical charts of 60 patients with CCFs were retrospectively reviewed. The clinical characteristics of direct and dural CCFs were analyzed by logistic regression. The clinical risk score was developed from the coefficient in the multivariable regression model and used to predict direct CCFs which were more urgent than the dural type. The score prediction was reported as an area under the receiver operating characteristic (AuROC) curve and 95% confidence interval (95% CI).
Results: In a univariable analysis, the clinical characteristics which increased the risk of direct CCFs were age, gender, trauma, underlying diseases, visual acuity (VA) at presentation, bruit, chemosis, and dilated retinal vessels. However, in multivariable analysis, the significant predictors were limited to age, trauma, bruit, underlying diseases and logMAR VA. Regression coefficient of each predictor was converted to a risk score and summation of scores from these predictors for each patient was calculated. The total risk score predicted the urgent direct CCFs correctly with AuROC of 97.77% (95% CI; 93.57, 100).
Conclusion: The clinical risk score for the prediction of urgent direct CCFs has been developed and used in the patients with CCFs in our setting. The discriminative ability of the score prediction is high. This simple clinical risk score may help clinicians suspect direct CCFs and urgently refer the patients to have prompt angiography and treatment.
Keywords: clinical risk score, cavernous sinus, carotid cavernous fistulas, prediction, urgency
Introduction
Carotid cavernous sinus fistulas (CCFs) are abnormal vascular connections between the internal carotid artery or external carotid artery and the cavernous sinus.1 Barrow et al classified CCFs into direct and indirect or dural CCFs, based on the angiographic anatomy of the shunt.2 The CCFs arising directly from the carotid artery are direct type, while those originating from branch vessels of the carotid artery are dural type. Direct CCFs usually have acute onset, rapid progression and hence need for urgent treatment. Indirect or dural CCFs tend to be gradual onset, chronic in the course and usually lead to a delay in diagnosis and treatment. The clinical features depend on the extent of abnormal arterial flow and the increased venous pressure in the orbital venous system. The ocular features that occur most frequently are dilated episcleral vessels, chemosis, ptosis, orbital pain, external ophthalmoplegia, proptosis, bruit, secondary glaucoma, dilated retinal veins and intraretinal hemorrhage.3–11 Conjunctival injection is often the most common ocular manifestation in the early course, and patients are usually misdiagnosed as conjunctivitis. Moreover, most patients complain of visual symptoms, either slightly blurred vision or severe visual loss.5–7 This visual involvement may indicate the severity of the diseases and need for urgent treatment.
The standard imaging modality in the diagnosis of CCFs is cerebral angiography. Noninvasive imaging with computerized tomography or magnetic resonance imaging scan is typically done first. Evidence of cavernous sinus enlargement, proptosis, and superior ophthalmic vein dilation are suggestive of CCFs.2,6 However, the absence of these abnormalities does not exclude the diagnosis of CCFs. If there is a high degree of clinical suspicion, catheter cerebral angiography should be performed to specifically demonstrate the location of the shunts. In remote areas where radiologic imaging and angiography are not available, it seems more difficult to detect the urgency of direct CCFs early in the course. Precautious detection of these rapidly progressive CCFs may still be important to help clinicians to recognize the diseases and urgently refer them to the better-equipped hospital for appropriate treatment. This study aims to develop a clinical risk score for clinicians to recognize these rapidly progressive direct CCFs and test the discriminative ability of the scoring system used in the patients with CCFs.
Patients and Methods
This study was an extended study of our previous report on comparison of clinical characteristics between direct and dural CCFs.12 It followed the tenets of the Declaration of Helsinki and was approved by the Khon Kaen University Ethics Committee for Human Research. Medical records of all patients diagnosed as CCFs at the KKU Eye Center, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand, from January 2015 to December 2020 were retrospectively reviewed. Although ethics committee did not require patient consent to review the medical record, the case report forms had no linkage to the patient identities and the privacy of the patients was respected. The inclusion criteria were patients diagnosed as direct and dural CCFs, which were confirmed by radiographic imaging and angiography. The patients who were suspected of CCFs and later proved to be other diagnosis and who had incomplete data were excluded from the study.
The collected data included age, gender, duration of symptoms, history of trauma and underlying diseases. The data on eye examination included best-corrected visual acuity (BCVA), intraocular pressure (IOP), chemosis, dilated episcleral vessels, proptosis, ophthalmoplegia, bruit, dilated retinal vessels, and other retinal abnormalities.
Statistical Analysis
The data were analyzed using Stata version 16.1 (Stata Corp, College Station, TX77845 USA). Clinical characteristics of patients with direct and dural CCFs were compared for evidence of differences. Using univariable logistic regression, prediction by each clinical characteristic was reported as an area under the receiver operating characteristic (AuROC) curve. Significant clinical predictors were selected under the multivariable logistic regression, and their regression coefficients were used as item risk scores. Scores for each clinical predictor were added up to obtain a total risk score in each patient. Score prediction of direct CCFs was also reported as an AuROC curve. P value < 0.05 was considered statistical significance.
Results
Sixty patients consisted of 28 patients (46.67%) with direct CCF and 32 patients (53.33%) with dural CCF. Clinical characteristics of the patients are shown in Table 1. In comparison with dural CCFs, patients with direct CCFs were younger (31.32 ± 13.52 vs 61.25 ± 9.94 years, p < 0.001), more history of trauma (92.9% vs 15.6%, p < 0.001), more proptosis (85.7% vs 62.5%, p = 0.042), more bruit (67.9% vs 12.5%, p < 0.001), more conjunctival chemosis (64.3% vs 28.1%, p = 0.005), and poorer visual acuity at presentation (1.04 ± 1.05 vs 0.42 ± 0.55 logMAR, p = 0.005). Patients with dural CCFs were more females (71.9% vs 57.1%, p = 0.023) and more underlying diseases (53.13% vs 10.71%, p = 0.001).
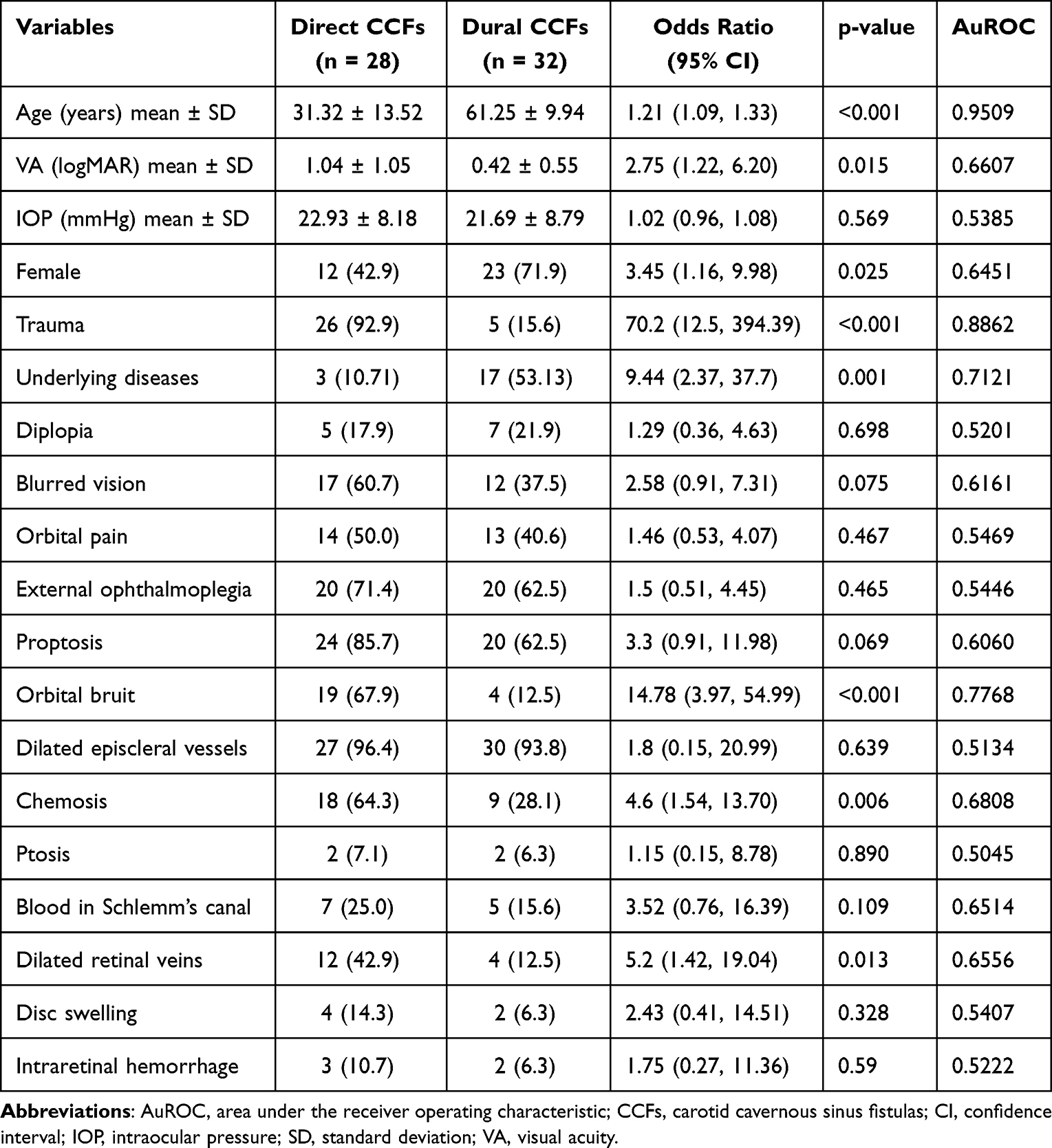 |
Table 1 Logistic Regression Analysis of Clinical Characteristics of CCF Patients |
Using univariable logistic regression, prediction by each clinical characteristic was reported as AuROC curve (Table 1). By multivariable regression analysis, the significant predictors for direct CCFs were age, trauma, orbital bruit, underlying diseases, and logMAR visual acuity. These predictors were selected by the values at which yielded the smallest p values and the highest AuROC curve obtained in logistic regression. These multivariable predictors predicted direct CCFs correctly with AuROC curve of 99.78% (95% CI; 99.24, 100) (Figure 1).
 |
Figure 1 Area under the receiver operating characteristic curve of 5 significant predictors on the prediction of direct carotid cavernous sinus fistulas. |
Regression coefficient for each clinical predictor was rounded to the nearest half (0.5) and used as a risk score (Table 2). Summation of scores from these five predictors for each patient was calculated to be a total risk score, which ranged from 0 to 16.5. Score prediction of direct CCFs was done by using a total risk score as the only one predictor. Figure 2 and Table 3 show that the derived clinical risk score can discriminate between direct and dural CCFs. The total risk score predicted direct CCFs correctly with AuROC curve of 97.77% (95% CI; 93.57, 100) (Figure 3).
 |
Table 2 Significant Clinical Predictors and Assigned Item Score |
 |
Table 3 Distribution of Clinical Risk Score in Patients with Direct and Dural Carotid Cavernous Sinus Fistulas |
 |
Figure 2 Distribution of clinical risk score in patients with direct and dural carotid cavernous sinus fistulas. |
 |
Figure 3 Area under the receiver operating characteristic curve of clinical risk score on the prediction of direct carotid cavernous sinus fistulas. |
The mean total risk score of patients with direct CCFs was significantly higher than that in the dural CCFs (12.66 ± 3.05 vs 2.78 ± 2.15, p < 0.001). The risk scores were divided into three risk groups, low (below 5), moderate (5 to 10), and high (above 10) for interpretation. The positive predictive value for direct CCFs was 3.7% in the low, 33.3% in the moderate and 100% in the high-risk category (Table 4). All patients with dural CCFs had a clinical risk score less than 10, whereas all patients with score 10 and higher were direct CCFs.
 |
Table 4 Sensitivity, Specificity and Positive Predictive Value in Diagnostic Prediction by Clinical Risk Score |
Discussion
Direct CCFs usually have sudden onset, rapid progression and therefore need for urgent treatment. Clinical risk score can help clinician to recognize the urgency of the disease. To find a model that is the best fit for this goal, we first establish a set of variables that will be used to predict an increased risk of direct CCFs. Then, we develop an item risk score for each predictor followed by using this risk scoring system in our patients. Finally, the discriminative ability of the diagnostic prediction for direct CCFs can be achieved.
In this study, the clinical risk score for prediction of direct CCFs has been developed. In a univariable analysis, the clinical characteristics which increased the risk of direct CCFs were age, gender, trauma, underlying diseases, VA at presentation, orbital bruits, chemosis, and dilated retinal vessels. However, in multivariable analysis, the significant predictors were limited to age, trauma, orbital bruits, underlying diseases and logMAR VA. Coefficient of each predictor was used as a clinical risk score because it reflects the slope in the regression model. Clinical characteristics with higher coefficient indicate the higher slope in the model, stronger predictive value, and hence higher risk score. The developed clinical risk score was used in the patients with CCFs in this study, and the prediction ability of this risk score is 97.77%.
Based on the clinical features, ophthalmologist may be the first clinician to treat the patients with CCFs. Patients may have the complaint of red eyes, conjunctival injection, increased IOP or decreased vision.1,13 Ophthalmologist should have CCFs in the differential diagnosis of patients with these symptoms and signs. When patients do not respond to the conventional treatment and there is a high degree of suspicion of CCFs, ophthalmologist should ask for history of trauma, look for bruit or blood in Schlemm’s canal, and consult radiologist for imaging and angiography. Patients typically undergo noninvasive cerebral imaging first. Evidence of cavernous sinus enlargement, proptosis, and superior ophthalmic vein dilation are suggestive of CCFs.2,6,13,14 Then, catheter cerebral angiography is performed to confirm the diagnosis and establish the position of the fistulas. Radiologic imaging and angiography have been emphasized mainly when considering CCFs. Usually, CCFs are not diagnosed before these radiologic investigations.
In remote areas of many developing countries, where radiologic imaging and angiography may not always be available, it is likely that urgency of direct CCFs may not be recognized. In such situation, delay in definite diagnosis may be associated with the risk of serious consequences such as secondary glaucoma and visual loss. We believe that prediction of direct CCFs using only clinical characteristics may be valuable to recognize the urgency. Even though in area where radiologic imaging and angiography are available, there may be a long waiting list so that they are not easily accessible. Clinical risk score may help clinicians and radiologists to recognize the urgency, so that angiography and intervention are performed promptly in these patients.
In our setting, patients who scored below 5 were less likely to be direct CCFs. In those who scored more than 10, the positive predictive value for direct CCFs was 100%. All patients in this category were correctly identified by the derived clinical risk score. In this situation, it may be urgent to refer these patients to the full-equipped hospitals for angiography and radiologic intervention.
The strength of this study is the first, to our knowledge, to develop a clinical risk score for prediction of urgent direct CCFs in patients with clinically suspected CCFs. In addition, the scoring system is simply developed from clinical characteristics which are recorded in routine practice. However, there are some limitations in the study. First, retrospective data collection obtained under routine practice may be incomplete and some data may be missing. Second, our derived score may be specific to our setting. Clinical characteristics used as clinical risk scores in our setting may not be directly applicable to other settings. Further study to validate the prediction ability of our clinical risk score in other different settings should be performed in the future.
Conclusions
The clinical risk score for prediction of urgent direct CCFs has been developed and used in the patients with CCFs. The prediction ability is 97.77%. Simple clinical characteristics may help clinician distinguish between direct and dural CCFs, not only in remote areas where radiographic angiography services are not available but also in available area where these procedures are not easily accessible. Patients with direct CCFs may be informed about their risk or urgency and should be referred to a better equipped hospital for definite diagnosis and treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ellis JA, Goldstein H, Connolly ES, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32(5):E9. doi:10.3171/2012.2.FOCUS1223
2. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62(2):248–256. doi:10.3171/jns.1985.62.2.0248
3. Wang W, Li YD, Li MH, et al. Endovascular treatment of post-traumatic direct carotid-cavernous fistulas: a single-center experience. J Clin Neurosci. 2011;18(1):24–28. doi:10.1016/j.jocn.2010.06.008
4. Lewis AI, Tomsick TA, Tew JM. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995;36(2):239–245. doi:10.1227/00006123-199502000-00001
5. Gupta AK, Purkayastha S, Krishnamoorthy T, et al. Endovascular treatment of direct carotid cavernous fistulae: a pictorial review. Neuroradiology. 2006;48(11):831–839. doi:10.1007/s00234-006-0132-x
6. de Keizer R. Carotid-cavernous and orbital arteriovenous fistulas: ocular features, diagnostic and hemodynamic considerations in relation to visual impairment and morbidity. Orbit. 2003;22(2):121–142. doi:10.1076/orbi.22.2.121.14315
7. Alam MS, Jain M, Mukherjee B, et al. Visual impairment in high flow and low flow carotid cavernous fistula. Sci Rep. 2019;9(1):12872. doi:10.1038/s41598-019-49342-3
8. Meyers PM, Halbach VV, Dowd CF, et al. Dural carotid cavernous fistula: definitive endovascular management and long-term follow-up. Am J Ophthalmol. 2022;134(1):85–92. doi:10.1016/S0002-9394(02)01515-5
9. Preechawat P, Narmkerd P, Jiarakongmun P, Poonyarhalung A, Pongpech SMD. Dural carotid cavernous sinus fistula: ocular characteristics, endovascular management and clinical outcome. J Med Assoc Thai. 2008;91(6):852–858.
10. Theaudin M, Saint-Maurice JP, Chapot R, et al. Diagnosis and treatment of dural carotid-cavernous fistula: a consecutive series of 27 patients. J Neurol Neurosurg Psychiatry. 2007;78(2):174–179. doi:10.1136/jnnp.2006.100776
11. Das JK, Medhi J, Bhattacharya P, et al. Clinical spectrum of spontaneous carotid-cavernous fistula. Indian J Ophthalmol. 2007;55(4):310–312. doi:10.4103/0301-4738.33051
12. Supasai P, Kanjana K, Yospaiboon Y. Direct and dural carotid cavernous sinus fistulas: comparison of clinical characteristics. Clin Ophthalmol. 2023;17:1207–1214. doi:10.2147/OPTH.S410930
13. Chaudhry IA, Eikhamry SM, Al-Rashed W, Bosley TM. Carotid cavernous fistula: ophthalmological implications. Middle East Afr J Ophthalmol. 2009;16(2):57–63. doi:10.4103/0974-9233.53862
14. Rucker JC, Biousse V, Newman NJ. Magnetic resonance angiography source images in carotid cavernous fistulas. Br J Ophthalmol. 2004;88(2):311. doi:10.1136/bjo.2003.026575
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.