Back to Journals » Clinical Ophthalmology » Volume 17
Clinical Results and Factors Affecting Visual Function in Eyes Implanted with an Enhanced Monofocal Intraocular Lens
Authors Negishi K ![]() , Masui S, Ayaki M
, Masui S, Ayaki M ![]() , Torii H, Yotsukura E, Nishi Y
, Torii H, Yotsukura E, Nishi Y
Received 4 September 2023
Accepted for publication 13 December 2023
Published 21 December 2023 Volume 2023:17 Pages 3965—3973
DOI https://doi.org/10.2147/OPTH.S438599
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kazuno Negishi,1 Sachiko Masui,1 Masahiko Ayaki,1,2 Hidemasa Torii,1 Erisa Yotsukura,1 Yasuyo Nishi1
1Department of Ophthalmology, Keio University School of Medicine, Shinjuku‑Ku, Tokyo, Japan; 2Otake Clinic Moon View Eye Center, Yamato-City, Kanagawa, Japan
Correspondence: Kazuno Negishi, Department of Ophthalmology, Keio University School of Medicine, 35 Shinanomachi, Shinjuku‑Ku, Tokyo, 160‑8582, Japan, Tel +81-3-3353-1211, Fax +81-3-3359-8302, Email [email protected]
Purpose: To compare the clinical results achieved with the enhanced monofocal intraocular lenses (IOLs) with those of the monofocal IOL and investigate factors affecting the distance, intermediate, and near vision.
Patients and Methods: Patients were included who underwent bilateral consecutive cataract surgeries using the same IOLs with follow-up to 1 month postoperatively. Refractions, monocular UDVA and CDVA, and binocular distance-corrected functional visual acuity at 5 meters (BDCFVA), at 66 centimeters (BDCIFVA) and at 40 centimeters (DCNVA) were assessed. Multiple regression analysis was used to assess the factors affecting binocular BDCFVA, BDCIFVA, and BDCNFVA. Subjective symptoms were assessed using the Near Activity Visual Questionnaire (NAVQ) and visual analogue scale (VAS).
Results: Sixty patients (120 eyes) implanted with the Tecnis Eyhance IOL (30 patients, 60 eyes) or the Tecnis monofocal IOL (30 patients, 60 eyes) were included. The Tecnis Eyhance IOL provided significantly better binocular BDCIFVA than the Tecnis monofocal IOL in patients under 70 years of age. Multiple regression analysis showed that age was the only factor affecting distance and intermediate visual function in eyes with the Tecnis Eyhance IOL; gender, pupillary diameter, axial length, and average keratometry were not significant. There were no significant differences in subjective symptoms.
Conclusion: The comprehensive cohort analysis did not confirm the advantage on the intermediate vision of the Tecnis Eyhance IOL. Younger age may be an important factor to benefit from the unique optical characteristics of this IOL.
Keywords: presbyopia correcting intraocular lens, intermediate vision, functional visual acuity, age
Introduction
Intraocular lenses (IOLs) are medical devices that replace the natural crystalline lens during cataract surgery. The monofocal IOL has been used for many years, although replicating the natural accommodative function of the eye remains challenging. Several types of presbyopia-correcting IOLs such as accommodating, multifocal, and extended depth-of-focus IOLs have been used clinically and achieved certain levels of visual performance with a wide range of vision and decreased spectacle dependence after cataract surgery, although decreased contrast sensitivity and photic phenomena remain as trade-offs for range of vision.1,2
Recently, a new type of monofocal IOL, the Tecnis Eyhance (Johnson & Johnson Surgical Vision, Irvine, CA) was introduced that has nondiffractive optics with enhanced intermediate function, potentially reducing the need for glasses postoperatively. The Tecnis Eyhance IOL uses a technology called “continuous extended range of vision” to create a smooth transition between different distances, allowing for improved visual acuity (VA) across a wider range of distances with minimal photic effects.
Overall, the clinical results of the Tecnis Eyhance have been promising, with studies showing improved distance and intermediate VAs, reduced dependence on spectacles, and patient satisfaction.3–13 However, in the real world, the visual results sometimes vary individually, and patient’s pre-existing ocular factors may affect them.
We compared the clinical results achieved with the Tecnis Eyhance IOL with those of the monofocal IOL having the same platform and investigated factors affecting the distance, intermediate, and near vision.
Materials and Methods
Study Design and Patients
This single-site comparative case series involved patients who underwent bilateral consecutive cataract surgeries using the same IOLs for both eyes from February 2022 to January 2023 with follow-up to 1 month postoperatively. All decisions to provide surgical intervention in this study were made as routine clinical care. The inclusion criteria were an age of 20 years and over, no ocular and systemic complications that could affect surgical outcomes, and 0.8 (20/25) and better postoperative corrected distance VA (CDVA). The exclusion criteria were a history of ocular surgery, the presence of intraoperative and/or postoperative ocular compilations, and a greater than 1-month interval between the bilateral surgeries.
The Keio University School of Medicine Ethics Committee approved the study protocol and verbal informed consent (Approval Number 20211047). Each patient provided verbal informed consent before entry into the study, which adhered to the tenets of the Declaration of Helsinki.
IOLs
The conventional monofocal IOL, Tecnis IOL (ZCB00, Johnson & Johnson Surgical Vision, Inc.) is a single-piece 6.0-mm biconvex hydrophobic acrylic monofocal IOL with the aspheric anterior surface that results in a negative spherical aberration of −0.27 micron and has a frosted, continuous 360-degree posterior square edge. The Tecnis Eyhance IOL (ICB00, Johnson & Johnson Surgical Vision, Inc.) is a new monofocal IOL with the same features as the ZCB00 IOL, except for the modified aspheric anterior surface of the optic. This enhanced aspheric optic creates a continuous power profile, ie, the power increases continuously from the periphery to the center of the lens, which is intended to extend the depth of focus, thus improving vision for intermediate tasks compared with the standard monofocal IOL. The IOL is based on the refractive technology without diffractive rings and zones, and it is visually indistinguishable from the ZCB00 IOL. In this study, the preloaded models of these IOLs with/without yellow tint including the toric models were used (DCB00V, DCB00, DIB00V, and DIW150, 225,300, and 375).
Surgery
One experienced surgeon (K.N.) performed all surgeries using a standard technique of sutureless phacoemulsification through a 2.4-mm corneal incision. An anterior capsulorhexis about 5.0 mm in diameter was created and the IOL was implanted into the capsular bag.
Evaluation of Clinical Data
All patients underwent a preoperative ophthalmologic examination that included measurement of the subjective refraction and monocular uncorrected distance visual acuity (UDVA) (5 m) and CDVA under photopic conditions (250 cd/m2) and 100% contrast. Optical biometry (ARGOS®, Alcon, Ft. Worth, TX), corneal topography (OPD-Scan® III, NIDEK, Aichi, Japan). The pupillary diameter was measured under photopic conditions using the ARGOS biometer. The IOL power predicted postoperative refraction was based on biometry data measured using the ARGOS biometry device and calculated using the Barrett Universal II formula with 119.3 of IOL constant. The IOL power was determined according to patient requests. Postoperatively, patients were evaluated at 1 month. Subjective and objective refractions were measured and monocular distance uncorrected and corrected VAs, binocular distance-corrected functional visual acuity (BDCFVA) at 5 meters, binocular distance-corrected functional intermediate VA (DCIVA) at 66 centimeters, and distance-corrected functional near VA (DCNVA) at 40 centimeters were assessed under photopic conditions. The functional visual acuity, FVA, which has been reported to reflect the changes in visual function due to various conditions more sharply than the conventional visual acuity,14–17 was measured using a FVA measurement system (AS-28, Kowa, Aichi, Japan) (Figure 1). This system examined the timewise changes in continuous VA over 60 seconds in photopic condition (background luminance 100cd/m2). The Landolt optotypes are presented in the device. The measurement starts with the best-corrected Landolt VA, which is the baseline VA for each individual. The Landolt optotypes decrease in size automatically with correct answers; when the responses are incorrect, larger optotypes are presented automatically. When there is no response within the set display times, the answer is considered an error and the optotype enlarges automatically. Subjects delineate the orientation of the automatically presented Landolt rings using a joystick. The system can measure VA levels from 30/20 to 20/200. The presentation time of an optotype was adjusted to 2 seconds, and the optotypes changed automatically even if the subjects missed responding within 2 seconds. The VA for 60 seconds was recorded in this study. The testing was performed with the subjects blinking spontaneously, and the continuous VA changes were plotted (Figure 2). The FVA was defined as the average of all VA values measured over time, because this average may reflect the daily vision more accurately than the VA measured at a specific time point. The BDCFVA was measured with the best correction for distance; the BDCIFVA and BDCNFVA were measured with −1.5 diopters (D) and −2.5 D added to the best distance correction respectively, which was equivalent to the mean DCIVA and DCNVA measured continuously for 60 seconds.
 |
Figure 1 Functional visual acuity measurement system (AS-28, Kowa, Aichi, Japan). |
 |
Figure 2 Representative results of the functional visual acuity. The blue line denotes the Landolt corrected visual acuity. The red line shows the time-wise changes in the visual acuity during testing. The green line denotes the mean logarithm of the minimum angle of resolution over 60 seconds, defined as the functional visual acuity. The yellow dots show the number of correct responses; the blue triangles indicate spontaneous blinks. |
Questionnaire
Subjective symptoms were assessed using the Japanese version of the Near Activity Visual Questionnaire (NAVQ) developed by Buckhurst et al.18 The NAVQ is comprised of one question regarding the overall satisfaction with the near vision and 10 questions regarding the near vision such as reading labels, writing notes, and viewing close objects in poor/dim light. The responses regarding the overall satisfaction ranged from 0 (completely satisfied) to 4 (completely unsatisfied). The responses to the other 10 questions ranged from 0 (no difficulty) to 3 (extreme difficulty), and the sum of the 10 can be converted to a linear scale from 0 to 100. We used the converted NAVQ score as the index of the subjective symptoms. In addition, visual disturbances due to photic phenomena (glare, halos, and starbursts) and spectacle independence were assessed using a visual analogue scale (VAS) (0 - +100; 0 = ”I don’t use glasses at all”, ”I don’t feel photic phenomena at all”; 100= “I always use glasses”, ”I feel photic phenomena strongly”). The spectacle dependence for near vision was analyzed for emmetropic patients whose subjective spherical equivalent was within ± 0.5 D (18 patients with the Tecnis Eyhance IOL, the E group, and 17 patients with the Tecnis monofocal IOL, the C group).
Sample Size Determination
According to the previous study comparing the visual outcomes of these IOLs 13, the binocular uncorrected intermediate visual acuity (logMAR) was 0.27 ± 0.06 with the conventional monofocal IOL and 0.16 ± 0.10 with the new monofocal IOL. Based on these results, the required sample size was 14 subjects in each group, totaling 28 subjects, when the effect size was 1.33, α = 0.05 (two-sided), and 1 - β = 0.80. Taking into consideration missing measurements and dropouts, we set a maximum of 30 cases for the new monofocal intraocular lens and 30 cases for the conventional monofocal intraocular lens, for a total of 60 cases.
Statistical Analysis
The values are expressed as the means ± standard deviations unless otherwise specified. The data obtained in this study were analyzed using the SPSS 28 statistical software package (IBM Corp., Armonk, NY). The Shapiro–Wilk test was used to verify the distribution for normality. The Mann–Whitney U-test was used to analyze the age, pre- and postoperative subjective refractions, VAs (UDVA, CDVA, BDCFVA, DCIVA and DCNVA), preoperative biometry, and pupillary diameter. The chi-square test was used to analyze the effect of gender. Multiple regression analysis (forced entry method) was used to assess the factors affecting binocular BDCFVA, BDCIFVA, and BDCNFVA. Age, gender, pupillary diameter, axial length, and average keratometry value served as independent variables. The data from the right eyes were used for regression analysis. In addition, subgroup analyses were conducted for patients under 70 years old. The level of significance was set at P < 0.05.
Results
Clinical Results of All Patients
Sixty patients (120 eyes) who underwent bilateral consecutive cataract surgeries with the Tecnis Eyhance IOL (60 eyes of 30 patients, the E group) or with the Tecnis monofocal IOL (60 eyes of 30 patients, the C group) were included. The implanted IOL models were as follows: DIB00V in 41 eyes, DIW150 in seven eyes, DIW225 in seven eyes, DIW300 in four eyes, and DIW375 in one eye in the E group, and DCB00 in four eyes and DCB00V 56 eyes in the C group. The patient demographic and preoperative data are shown in Table 1. There were no significant differences in age, gender, preoperative monocular UDVA, CDVA, subjective refraction, axial length, keratometry, and pupillary diameter.
 |
Table 1 The Patient Demographic and Preoperative Data |
The postoperative refractions and VAs are shown in Table 2. There were no significant differences in the postoperative subjective refraction, subjective astigmatism, monocular UDVA, CDVA, binocular BDCFVA, BDCIFVA, or BDCNFVA. The NAVQ and VAS scores of the visual disturbances due to photic phenomena (glare, halos, and starbursts) and spectacle independence were 47.42 ± 25.61 (range, 0–80.72), 5.3 ± 15.8 (range, 0–75), 57.2 ± 47.2 (range, 0 - +100) in the E group, and 48.96 ± 19.56 (range, 10.72–75.09), 10.4 ± 24.6 (range,0–90), and 42.2 ± 41.0 (range, 0 - +100) in the C group, respectively. There were no significant differences between the groups.
 |
Table 2 Postoperative Refraction and Visual Acuity |
Multiple Regression Analysis
The results of multiple regression analyses to assess the factors affecting the binocular BDCFVA (5 meters) and BDCIFVA (66 centimeters) showed that only age was a significant factor affecting the BDCFVA and BDCIFVA in the E group (Table 3) (The post-hoc statistical powers= 0.896). In contrast, no significant factors were found in the C group. The scattergrams for age and BDCFVA and BDCIFVA in the E group are shown in Figure 3. No independent variable was adopted for the BDCNFVA in either group.
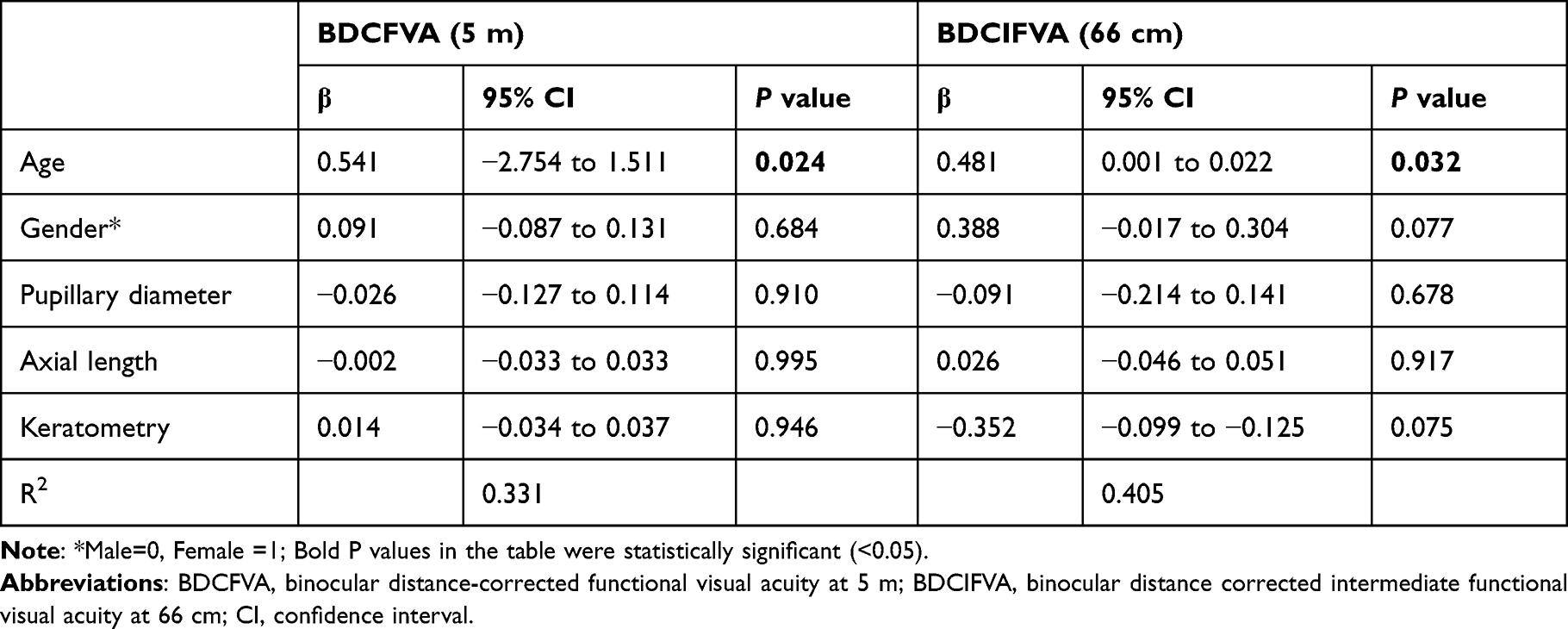 |
Table 3 Multiple Regression Analyses Estimates of Factors Affecting the Binocular Distance-Corrected Functional Visual Acuity and the Binocular Distance-Corrected Intermediate Functional Visual Acuity in the E Group |
 |
Figure 3 Relationships between age and the binocular functional visual acuity in patients in the E group. (A) Binocular distance-corrected functional visual acuity at 5 meters (r=0.592; P=0.001). (B) Binocular distance-corrected intermediate functional visual acuity at 66 centimeters (r=0.526; P=0.003). Abbreviations: BDCFVA, Binocular distance-corrected functional visual acuity; logMAR, logarithm of the minimum angle of resolution; BDCIFVA, Binocular distance-corrected intermediate functional visual acuity at 66 centimeters; logMAR, logarithm of the minimum angle of resolution. |
Subgroup Analyses
Considering the multiple regression analysis that age was a significant factor affecting the BDCFVA and BDCIFVA in the E group, we separately analyzed the patients in younger generation, under 70y/o (23 patients). The postoperative refractions and VAs in the patients under 70 years old are shown in Table 4. The BDCIFVA was significantly better in the E group than in the C group although the post-hoc statistical power was weak (0.549) due to small sample size and the results should be treated with caution. No other significant differences were found in the postoperative subjective refraction, subjective astigmatism, monocular UDVA, CDVA, binocular BDCFVA, or BDCNFVA between the groups.
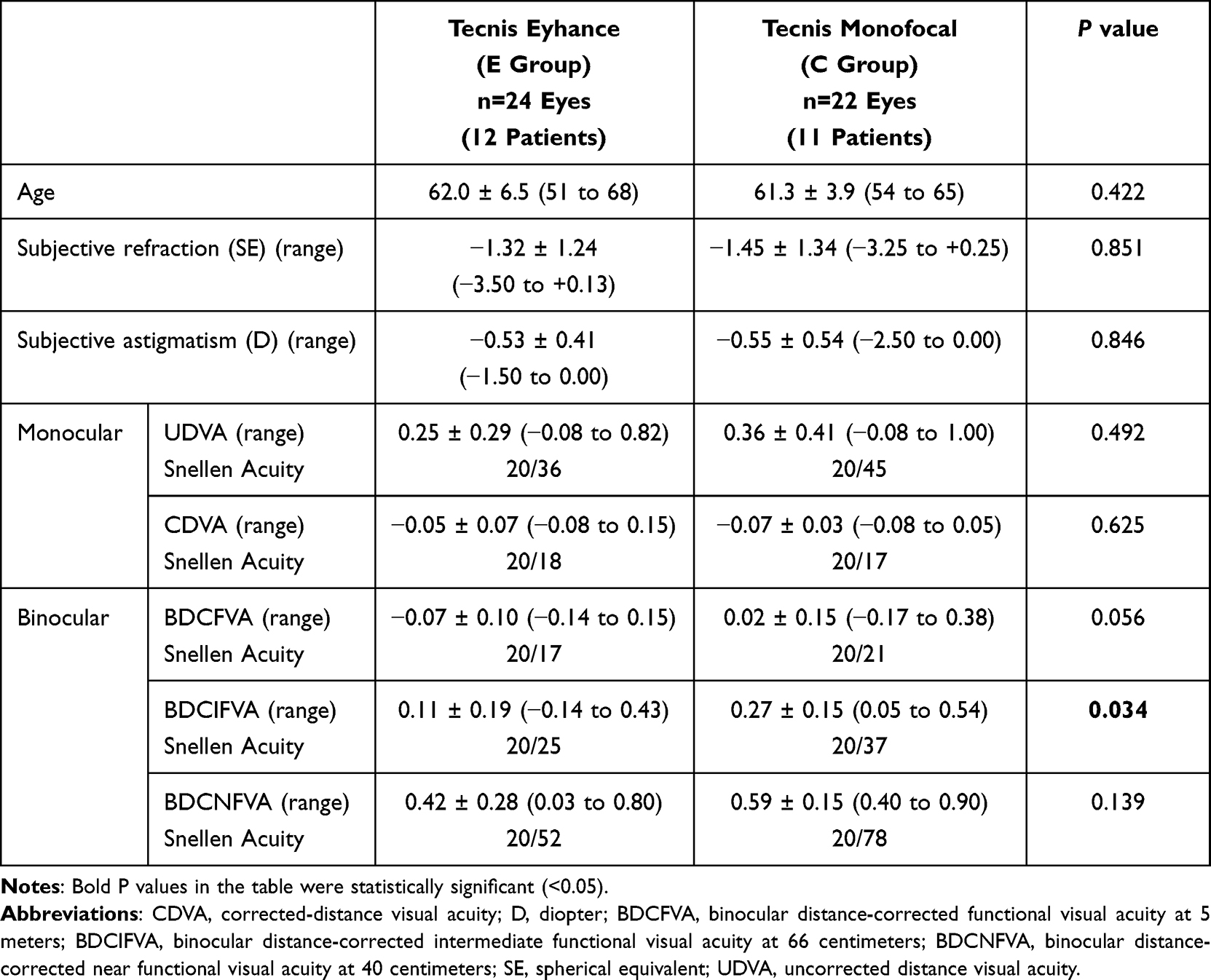 |
Table 4 Postoperative Refraction and Visual Acuity in Patients Under 70 Years Old |
In the patients 70 years and older no significant differences were found in the postoperative refraction and VA at any distance.
Discussion
The results indicated that the Tecnis Eyhance IOL provided significantly better binocular BDCIFVA than the conventional Tecnis monofocal IOL without degradation of distance and near visual function in patients under 70 years of age. Multiple regression analysis showed that age was the only factor affecting distance and intermediate visual function in eyes with the Tecnis Eyhance; gender, pupillary diameter, axial length, and average of keratometry were not significant.
Several previous studies have compared the Tecnis Eyhance and Tecnis monofocal IOLs in both clinical and optical bench settings. Regarding the clinical studies, Wan et al published a meta-analysis of the two IOLs.19 This study included 680 eyes implanted with an enhanced monofocal IOL and 647 eyes with a conventional monofocal IOL from three randomized controlled trials and nine comparative studies and concluded that the enhanced monofocal IOLs effectively improved unaided intermediate vision with excellent distance vision comparable to conventional monofocal IOLs, without compromising the contrast sensitivity or inducing photic phenomena. Redruello-Guerrero et al also published a meta-analysis on the same topic that included five studies that met the inclusion criteria with a total of 604 eyes (309 eyes with Tecnis Eyhance IOLs and 295 eyes with Tecnis ZCB00 IOLs). The authors concluded that preliminary pooled evidence indicated that the intermediate VA improved with the Tecnis Eyhance IOLs.20 Most clinical reports have shown that the Eyhance IOL provides the range of vision without trade-offs in the visual quality including contrast sensitivity and photic phenomena such as glare and halos.3–13
The current results showed a clear correlation between age and distance and intermediate FVAs with distance correction in eyes with the Tecnis Eyhance IOL, although there was no such relationship in eyes with the Tecnis monofocal IOL. To the best of our knowledge, this is the first study to report that age is an important factor affecting the visual performance of the Tecnis Eyhance IOL.
Several reports have been published on the effect of pupillary size on the optical performance of the Tecnis Eyhance IOL. Huh et al reported the results of an optical bench test that showed that the Tecnis Eyhance provided the best optical performance in the intermediate distance at 2 mm of pupillary size.21 Vega et al reported the in vitro optical performance of the Tecnis Eyhance IOL and found that there was a focus extension effect accompanied by myopic shift as the pupillary size decreased, and that this IOL provided an extended range of vision up to −0.50, −0.75, and −1.50 D for 4.5-, 3-, and 2-mm pupillary sizes, respectively. The authors concluded that this IOL had optical behavior comparable to a conventional Tecnis monofocal IOL for distance vision and an extended range of focus up to −1.50 D, considering the pupillary dynamics during distance, intermediate, and near vision under photopic lighting conditions.22 Alarcon et al also reported that the improvement in intermediate simulated VA obtained from the through-focus VA was independent of the pupillary size.23
The current multiple regression analyses of clinical cases showed the pupillary size independence of the distance, intermediate, and near VA in eyes with the Tecnis Eyhance IOL, which agreed with the Alarcon’s report. However, we used the pupil size measured using ARGOS biometer for analysis and did not obtain the detailed data of the pupil size during distance, intermediate, and near vision. Further investigation will be necessary to clarify the influence of pupil size on visual performance in eyes with the Tecnis Eyhance IOL. Age was the only significant independent factor affecting the binocular BDCFVA and BDCIFVA in eyes with the Tecnis Eyhance IOL; the binocular BDCFVA and BDCIFVA were significantly better in eyes with the Tecnis Eyhance IOL than in eyes with the Tecnis monofocal IOL. This implies that younger patients could reap the benefits of this enhanced monofocal IOL more easily, although no adverse effects would occur even if it was implanted in older patients. We speculated that factors related to age such as pupillary dynamics and retinal and brain function might affect the results. Further investigations are needed to determine the factors affecting the range of vision with the Tecnis Eyhance IOL.
In this study, we measured the binocular FVA at distance, intermediate, and near. This was a strength of the study because the FVA can detect minor differences in visual function more sensitively than conventional VA tests, and it is useful for evaluating the daily visual performance under various ocular conditions.14–17 In contrast, the small sample size and mixture of the clear and yellow-tinted and toric models were study limitations; further investigation are needed to confirm the results of this study.
Conclusion
In conclusion, the comprehensive cohort analysis did not confirm significant differences in the intermediate, as well as distance and near visual function, between the patients with the Tecnis Eyhance IOL and those with the conventional Tecnis monofocal IOL. Younger age may be an important factor to benefit from the unique optical characteristics of this IOL.
Acknowledgments
We appreciate Ms. Lynda Enoch Charters for editing our manuscript.
Funding
This study was supported by a grant from Johnson and Johnson Vision (Irvine, CA).
Disclosure
Professor Kazuno Negishi reports grants from Johnson and Johnson Vision, during the conduct of the study; personal fees from Johnson and Johnson Vision, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Megiddo-Barnir E, Alio JL. Latest development in extended depth-of-focus intraocular lenses: an update. Asia-Pac J Ophthalmol. 2023;12(1):58–79. doi:10.1097/APO.0000000000000590
2. Rampat R, Gatinel D. Multifocal and extended depth-of-focus intraocular lenses in 2020. Ophthalmology. 2021;128(11):e164–e185. doi:10.1016/j.ophtha.2020.09.026
3. Auffarth GU, Gerl M, Tsai L, et al., Quantum Study G. Clinical evaluation of a new monofocal IOL with enhanced intermediate function in patients with cataract. J Cataract Refract Surg. 2021;47(2):184–191. doi:10.1097/j.jcrs.0000000000000399
4. Choi WK, Han HJ, Son HS, Khoramnia R, Auffarth GU, Choi CY. Clinical outcomes of bilateral implantation of new generation monofocal IOL enhanced for intermediate distance and conventional monofocal IOL in a Korean population. BMC Ophthalmol. 2023;23(1):157. doi:10.1186/s12886-023-02897-2
5. Cinar E, Bolu H, Erbakan G, et al. Vision outcomes with a new monofocal IOL. Int Ophthalmol. 2021;41(2):491–498. doi:10.1007/s10792-020-01599-8
6. Corbelli E, Iuliano L, Bandello F, Fasce F. Comparative analysis of visual outcome with 3 intraocular lenses: monofocal, enhanced monofocal, and extended depth of focus. J Cataract Refract Surg. 2022;48(1):67–74. doi:10.1097/j.jcrs.0000000000000706
7. Fernandez J, Rocha-de-Lossada C, Zamorano-Martin F, Rodriguez-Calvo-de-Mora M, Rodriguez-Vallejo M. Positioning of enhanced monofocal intraocular lenses between conventional monofocal and extended depth of focus lenses: a scoping review. BMC Ophthalmol. 2023;23(1). doi:10.1186/s12886-023-02844-1
8. Fernandez-Vega-Cueto L, Vega F, Guerra-Velasco R, Millan MS, Madrid-Costa D, Alfonso JF. Optical and clinical outcomes of an enhanced monofocal intraocular lens for high hyperopia. J Refract Surg. 2022;38(9):572–579. doi:10.3928/1081597X-20220802-01
9. Gigon E, Bouthour W, Panos GD, Pajic B, Massa H. Real world outcomes of the new Tecnis Eyhance IOL. Eur J Ophthalmol. 2022. doi:10.1177/11206721221146675
10. Jeon YJ, Yoon Y, Kim TI, Koh K. Comparison between an intraocular lens with extended depth of focus (Tecnis Symfony ZXR00) and a new monofocal intraocular lens with enhanced intermediate vision (Tecnis Eyhance ICB00). Asia-Pac J Ophthalmol (Phila). 2021;10(6):542–547. doi:10.1097/APO.0000000000000439
11. Lee JH, Moon SY, Chung HS, et al. Clinical outcomes of a monofocal intraocular lens with enhanced intermediate function compared with an extended depth-of-focus intraocular lens. J Cataract Refract Surg. 2022;48(1):61–66. doi:10.1097/j.jcrs.0000000000000710
12. Lopes D, Loureiro T, Carreira R, et al. Comparative evaluation of visual outcomes after bilateral implantation of an advanced or conventional monofocal intraocular lens. Eur J Ophthalmol. 2022;32(1):229–234. doi:10.1177/1120672121995343
13. Mencucci R, Cennamo M, Venturi D, Vignapiano R, Favuzza E. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J Cataract Refract Surg. 2020;46(3):378–387. doi:10.1097/j.jcrs.0000000000000061
14. Yamaguchi T, Negishi K, Tsubota K. Functional visual acuity measurement in cataract and intraocular lens implantation. Curr Opin Ophthalmol. 2011;22(1):31–36. doi:10.1097/ICU.0b013e3283414f36
15. Katada Y, Negishi K, Watanabe K, et al. Functional visual acuity of early presbyopia. PLoS One. 2016;11(3):e0151094. doi:10.1371/journal.pone.0151094
16. Watanabe K, Kaido M, Ishida R, Dogru M, Negishi K, Tsubota K. The effect of tinted soft contact lens wear on functional visual acuity and higher-order aberrations. Cont Lens Anterior. 2014;37(3):203–208. doi:10.1016/j.clae.2013.11.009
17. Negishi K, Masui S, Mimura M, Fujita Y, Tsubota K. Relationship between functional visual acuity and useful field of view in elderly drivers. PLoS One. 2016;11(1):e0147516. doi:10.1371/journal.pone.0147516
18. Buckhurst PJ, Wolffsohn JS, Gupta N, Naroo SA, Davies LN, Shah S. Development of a questionnaire to assess the relative subjective benefits of presbyopia correction. J Cataract Refract Surg. 2012;38(1):74–79. doi:10.1016/j.jcrs.2011.07.032
19. Wan KH, Au ACK, Kua WN, et al. Enhanced monofocal versus conventional monofocal intraocular lens in cataract surgery: a meta-analysis. J Refract Surg. 2022;38(8):538–546. doi:10.3928/1081597X-20220707-01
20. Redruello-Guerrero P, Rivera-Izquierdo M, Jimenez-Gutierrez C, Lainez-Ramos-Bossini AJ, Yela R, Lopez-Marin I. Improvement of intermediate vision with new monofocal intraocular lenses: a systematic review and meta-analysis. Eur J Ophthalmol. 2023;33:1308–1319.
21. Huh J, Eom Y, Yang SK, Choi Y, Kim HM, Song JS. A comparison of clinical outcomes and optical performance between monofocal and new monofocal with enhanced intermediate function intraocular lenses: a case-control study. BMC Ophthalmol. 2021;21(1):365. doi:10.1186/s12886-021-02124-w
22. Vega F, Millan MS, Gil MA, Garzon N. Optical performance of a monofocal intraocular lens designed to extend depth of focus. J Refract Surg. 2020;36(9):625–632. doi:10.3928/1081597X-20200710-01
23. Alarcon A, Canovas C, Koopman B, Pande MV, Koch DD, Piers P. Optical bench evaluation of the effect of pupil size in new generation monofocal intraocular lenses. BMC Ophthalmol. 2023;23(1):112. doi:10.1186/s12886-023-02839-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.