Back to Journals » Advances in Medical Education and Practice » Volume 14
Clinical Reproducibility and Reliability of Lever Sign (Lelli’s) Test for Acute ACL Tear Performed by Medical Students
Authors Dawod MS ![]() , Alswerki MN
, Alswerki MN ![]() , Darabah AJ
, Darabah AJ ![]() , Darabah YJ, Akel AY, Alisi MS
, Darabah YJ, Akel AY, Alisi MS ![]()
Received 11 January 2023
Accepted for publication 16 March 2023
Published 28 March 2023 Volume 2023:14 Pages 289—295
DOI https://doi.org/10.2147/AMEP.S402496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Moh’d S Dawod,1 Mohammad N Alswerki,2 Asem J Darabah,1 Yazeed J Darabah,1 Alaa Y Akel,1 Mohammed S Alisi2– 4
1Department of Orthopedic Surgery, Mu’tah School of Medicine, Mu’tah University, Al-karak, Jordan; 2Department of Orthopedic Surgery, Jordan University Hospital, Amman, Jordan; 3Faculty of Medicine, Islamic University of Gaza, Gaza, Palestine; 4Ministry of Health, Gaza, Palestine
Correspondence: Mohammad N Alswerki, Department of Orthopedic Surgery, Jordan University Hospital, P.O. Box: 13046, Amman, 11942, Jordan, Tel +962 798576972, Email [email protected]
Background: Injuries to the anterior cruciate ligament (ACL) in sports are frequent in children and young adults participating in sporting activities involving rotational and pivoting movements. Magnetic resonance imaging is the most accurate diagnostic tool to detect an ACL tear. There are, however, a number of specialized tests available to assess ACL competency.
Hypothesis: A novel test was described with extremely high clinical accuracy. The purpose of this study was to assess its clinical accuracy when performed by non-orthopedic providers, such as medical students.
Methods: A cross-sectional study design was adopted, and two patients with an MRI-proven complete ACL tear were selected. One patient was thin, and the other was overweight, and both were examined by 100 medical students for both the injured and uninjured knee. The results for these exams were recorded, and a statistical analysis of the screening test was done to evaluate the new special test.
Results: Our results were different from the ones found in the literature: we found the test to have a significantly lower performance in terms of sensitivity, specificity, and positive and negative likelihood ratios compared to the literature numbers.
Conclusion: The Lever sign (Lelli’s) test loses clinical credibility and significance when performed by non-orthopedic providers or doctors, such as medical students in our study.
Keywords: ACL tear, acute ACL injury, knee instability, Lelli’s test, lever sign test
Plain Language Summary
What is known about the subject: The lever sign has high sensitivity and specificity for detecting knee instability in cases of ACL injury.
What this study adds to existing knowledge: Lelli’s test loses its well-known clinical significance when performed by non-orthopedic providers/doctors.
Level of Evidence: Level 4, Cross sectional Descriptive.
Study Design: Cross-sectional study type.
Introduction
The anterior cruciate ligament (ACL) is a major stabilizing factor of the knee joint and an important biomechanical component of the knee’s rotational and anteroposterior stability.1,2 Injuries to the ACL are common during adolescence and early adulthood during sports activity, especially in sporting exercises that demand pivoting acts and maneuvers.3–5 ACL injuries can be identified by a history of knee trauma followed by knee hemarthrosis, as well as the typical physical examination findings of anterior sliding of the tibia over the femur.6,7 Patients with knee instability due to an ACL injury are treated with physiotherapy first, with a protocol focusing on strengthening the muscle envelop around the knee to improve its stability. Patients who fail to improve with this physical therapy regime will then be referred for surgical ACL reconstruction using either a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST).8 The difficulty of diagnosing an acute ACL injury based on physical exam results comes from the combination of painful hemarthrosis and swelling at the acute phase of the injury,9,10 which can trigger hamstring muscle spasms that can mask the anterior tibial translation.11,12
There are many physical exam tests for detecting ACL deficiency, including the anterior drawer test, Lachman’s test, pivot shift test, and the lever sign (Lelli’s test).13,14 When compared to the other physical examination maneuvers, the lever sign test is the simplest and easiest to perform and thus should have high clinical reproducibility regardless of who performs the test.15,16 When performed by trained orthopedic providers, the lever sign test (reported by Dr Lelli) has a very high reported sensitivity and specificity.17 Aside from studies showing conflicting numbers for the sensitivity and specificity of the test,16,18 no studies were performed to measure the clinical reliability of the test if performed by non-orthopedic doctors. Since the test is simple, it should be performed with high accuracy, even if done by non-orthopedic providers. So, our aim in this study is to measure the accuracy of the test when performed by medical students.
Patients and Methods
The study included 2 male patients who had an acute complete ACL tear confirmed by both physical examination findings (anterior tibial translation evidenced on the anterior drawer, Lachman’s test, and pivot shift test) and a knee magnetic resonance imaging study showing a complete ACL tear with a report documenting the full tear by a consultant radiologist. Adult patients (age > 18 years) with acute ACL injuries (less than 3 weeks) who presented to our hospital’s sports clinic and had no significant knee swelling at the time of examination met the inclusion criteria for patient selection. Exclusion criteria included chronic ACL injury, incomplete ACL injury, injury lasting more than 3 weeks, age under 18 years, and patients with significant persistent swelling. One patient was thin (BMI < 25); the other patient was overweight (BMI > 25).
The Lelli’s test was performed both on the affected and the unaffected knees of the patients as a control. The test was performed by 100 5th-year medical students during their orthopedic rotation in April 2021. The students were instructed about the ideal way to perform the test before doing it by a senior orthopedic consultant. An orthopedic surgery consultant was observing the student while he performed the test. The students were blinded regarding whether the patients had an ACL injury or not. Our research was descriptive in nature, with cross-sectional designs. Ethics approval was obtained from the Mutah University Ethics Committee for this study, IRB number 772022. The Code of Ethics of the World Medical Association (Declaration of Helsinki) was followed while conducting the study. Informed written consent was obtained from the patients, and informed consents were obtained from all the participating students as well.
The Test Technique
The patient is positioned supine on his back, with both knees straightened on the examination table (Figure 1). The examiner put a closed fist beneath the tibial tuberosity of the examined knee. As a result, the knee flexes slightly. With the tester’s second hand, exert moderate downward pressure on the distal femur. With this arrangement, the patient’s leg acts as a lever over a fulcrum—the clinician’s fist. The test was reported as either: Intact ACL: The patient’s foot will rise off the bed with the application of downward pressure to the distal thigh. Ruptured ACL: The patient’s foot will keep in contact with the bed with the addition of downward force to the distal quadriceps.18
 |
Figure 1 The proper technique for performing the lever sign test is shown in picture (A). Picture (B) Depicts the test technique with a negative test result, while Picture (C) Depicts the test technique with a positive result. |
Results
Descriptive statistical analysis was done using the Statistical Package for Social Sciences (SPSS) version 22. The validity of the exam was done using sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Additional to this statistical measurement, we measured the accuracy, which is defined as the summation of true positive and true negative to all test results. P < 0.05 was considered statistically significant.
Assessment and examination were done by 100 medical students. Examination of the first patient revealed that 88 students (88%) failed to identify the ACL tear, and the test was reported negative. Only 12 students (12%) correctly identified the injury as a positive test (Table 1). Examination of the second patient revealed an improved detection rate as per the following, 46 students (46%) correctly identified the injured ACL, while 54 (54%) failed to do so (Table 2). When using the patient’s contralateral normal knee as a control, we obtained the following results: Examination of the first patient revealed that 89 students (89%) successfully identified this knee as having a normally functioning ACL, while 11 (11%) students had positive test results (Table 3). On the overweight patient (patient 2), the numbers were as follows: 70 students correctly identified the normal side as having a normal ACL, and 30 students identified this normal side as abnormal (Table 4).
 |
Table 1 Percent of Students Performed the Test on the Injured ACL on Patient 1 (the Thin Patient BMI = 22) |
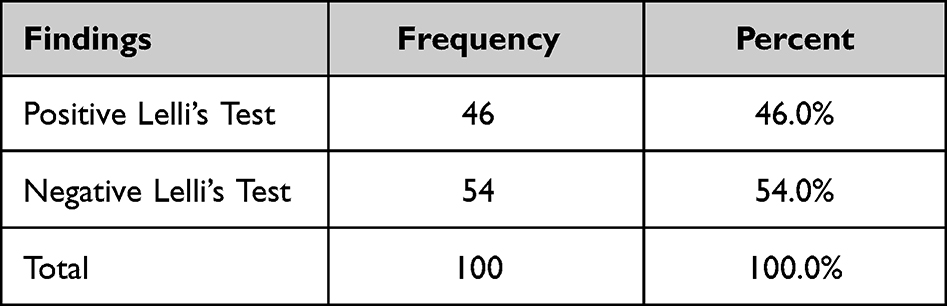 |
Table 2 Percent of Students Performed the Test on the Injured ACL on Patient 2 (the Overweight Patient BMI = 29) |
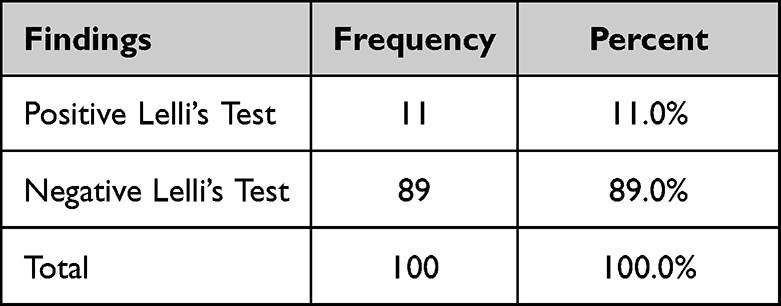 |
Table 3 Percent of Students Performed the Test on Normal ACL on Contralateral Normal Knee on Patient 1 (the Thin Patient BMI = 22) |
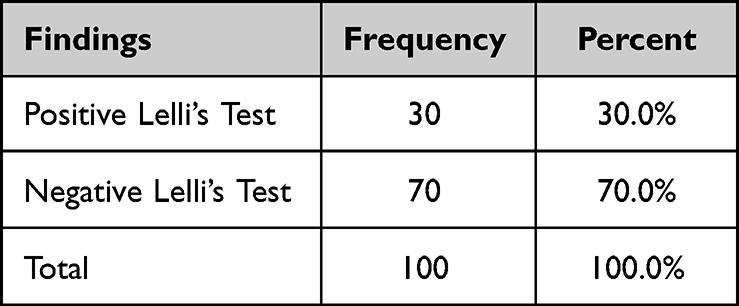 |
Table 4 Percent of Students Performed the Test on Normal ACL on Contralateral Normal Knee on Patient 2 (the Overweight Patient BMI = 28) |
Statistical analysis for the first patient (BMI < 25) by a 4×4 classical statistical table revealed a sensitivity of 12%, a specificity of 89%, a positive predictive value (PPV) of 52%, a negative predictive value (NPV) of 50%, and an accuracy of 50%. The LR+ for the test performed on patient 1 (BMI < 25) was 1.19, and the LR- was 0.98 (Table 5). When 4×4 statistical table analysis is done on patient 2 (BMI > 25), we find a sensitivity of 46%, a specificity of 70%, a positive predictive value (PPV) of 60%, a negative predictive value of 56%, and an accuracy of 58%. The LR+ for the test performed on patient 2 (BMI > 25) was 1.53, and the LR- was 0.77 (Table 6).
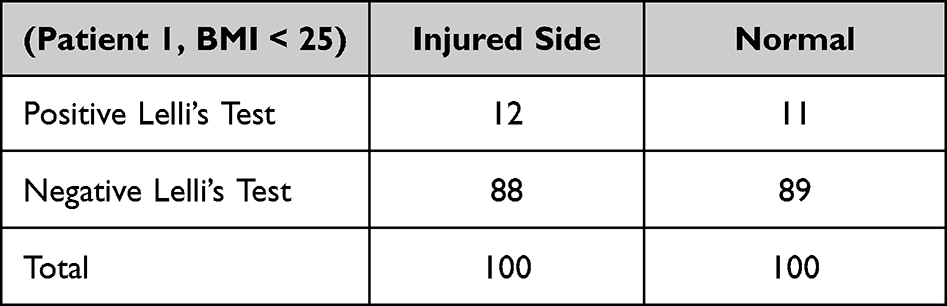 |
Table 5 4×4 Statistical Table to Identify Sensitivity, Specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV) of the Test on the Thin Patient (Patient 1, BMI < 25) |
 |
Table 6 4×4 Statistical Table to Identify Sensitivity, Specificity, Positive Predictive Value (PPV), Negative Predictive Value (NPV) of the Test on the Overweight Patient (Patient 2, BMI > 25) |
Discussion
An anterior cruciate ligament injury is a common sport injury among adolescent and young adult athletes. Knee trauma, particularly when caused by a high-energy mechanism, can result in other capsuloligamentous injuries in addition to the ACL. An injury to the patellofemoral ligaments and retinacula can be associated with such an injury. So, it’s of critical importance to address such injuries during the planning and management of such cases. A study done by Biz et al demonstrated detailed anatomical delineations of such structures.19
The gold standard for the diagnosis of this injury is magnetic resonance imaging (MRI) of the knee joint. However, before reaching a definitive diagnosis, a series of physical examinations and special tests have been described to assess the integrity of the ACL.7 An ideal diagnostic test for a common injury like an ACL tear should be structured, easy to perform, clinically reproducible, and have high sensitivity and specificity. The three most common special tests for an ACL injury are the anterior drawer test, the Lachman’s test, and the pivot shift test. These tests, despite being widely clinically used, have different reported sensitivity and specificity.20
In 2005, a new diagnostic test was proposed by Dr Alessandro Lelli (an Italian orthopedic knee surgeon) with high or nearly perfect (100%) sensitivity and specificity. However, we argue that these results are extremely high even if the test principle is clear and easy to perform. Our theory argues that if this test is so efficient and versatile in detecting ACL injuries regardless of timing, then even non-orthopedic providers should be able to perform it. In our study, those were the 5th medical students during their orthopedics clinical rotation. Lelli et al, in their original work, described this test as being competent in diagnosing both acute and chronic ACL injuries. He also mentioned the test’s ability to detect not only complete ACL tears, but also partial tears.17
Previous literature showed different statistical values for the lever-sign test. One statistical method to assess correlation that was reported in previous work is the use of positive or negative likelihood ratios (LR) as a measure of correlation. In previous literature, Jarbo et al reported a LR + of 6.15 and a LR – of 0.14. 21 Massey et al reported a LR + of 4.5, and a LR – of 0.21.18 Gürpınar et al reported a LR + of 14.7, and a LR – of 0.09.13 Mulligan et al reported a LR+ of 7.5 and a LR- of 0.19.22 In our study, the LR + was 1.1 for the thin patient and 1.53 for the overweight patient. The LR- for the thin patient was 0.98, while the LR- for the overweight patient was 0.77.
In terms of other statistical parameters to assess the competency of the lever sign test, previous literature showed that Jarbo et al, Masset et al, Gürpınar et al and Mulligan et al reported a sensitivity of 64%, 83%, 92%, and 83%, respectively. Their reported specificity was as follows: 90%, 80%, 94%, and 89%, respectively. In our study, the reported sensitivity and specificity for patient 1 (thin patient, BMI < 25) were 12% and 89%, respectively, and the reported sensitivity and specificity for patient 2 (overweight patient, BMI > 25) were 46% and 70%, respectively. A spectrum of differences between the literature and our findings are summarized in Table 7.
 |
Table 7 Summary of Findings in Comparison to Previous Literature |
Evident from the previous summary is that our results showed inferior results for the lever sign (Lelli’s test) in terms of sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio. These changes stem from the fact that most previous studies assessing the accuracy and competency of the Lelli’s test were done by orthopedic providers/doctors. This indirectly reflects against the principle proposed by Lelli, which is that the test is simple, clinically reproducible, and versatile.8 The presented findings show that the lever sign test (Lelli’s test) loses clinical significance when performed by non-orthopedic providers or doctors; hence, it cannot be used as a screening test for an ACL tear. This limitation of the test makes it better performed by orthopedic residents, fellows, and consultants, and its utilization outside these spectrums of those providers in the clinical practice on the ground can be questionable.
A remarkable point noted in the study is the improved sensitivity and specificity of the test in patient 2, the patient with an overweight BMI. It is unclear why Lelli’s test detects ACL injuries better in overweight patients when the opposite would make sense. One plausible theory is that perhaps thin patients have more proprioceptive sensation in their joints and, during the performance of the test, can become more comprehensive with the resultant muscle guarding, which prevents the anterior tibial translation from becoming clinically evident. More studies are needed to better elucidate this issue.
The limitation of our study is that the assessment was done by medical students; other non-orthopedic providers like doctors of other specialties (for example, family physicians) were not included; and a limited number of students were enrolled in the study. A future study to investigate the performance of the test by other non-orthopedic doctors like emergency and family physicians is advised. Furthermore, a comparison study of the Lelli’s and other ACL-specific tests performed by medical students may aid in gaining a better understanding of this lower test accuracy.
Conclusion
The lever sign test is a new special test to detect anterior cruciate ligament (ACL) tears. The original test described by Lelli claimed to have 100% sensitivity and specificity for acute, chronic, partial, and full ACL tears. The literature disagrees about these very high numbers, which still show excellent sensitivity and specificity, hence the clinical credibility of the test. However, to get these clinical results, tests should be done by orthopedic doctors. The test lost its clinical credibility significantly if it was performed by non-orthopedic providers, and it cannot be used as a screening test.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Domnick C, Raschke MJ, Herbort M. Biomechanics of the anterior cruciate ligament: physiology, rupture and reconstruction techniques. World J Orthop. 2016;7(2):82. doi:10.5312/WJO.V7.I2.82
2. Wang L, Wang CJ, Berryman F. Modeling of the knee joint. In: Computational Modelling of Biomechanics and Biotribology in the Musculoskeletal System. Elsevier; 2021:437–472. doi:10.1016/B978-0-12-819531-4.00017-1
3. Friel NA, Chu CR. The role of ACL injury in the development of posttraumatic knee osteoarthritis. Clin Sports Med. 2013;32(1):1. doi:10.1016/J.CSM.2012.08.017
4. Wojtys EM, Brower AM. Anterior cruciate ligament injuries in the prepubescent and adolescent athlete: clinical and research considerations. J Athl Train. 2010;45(5):509. doi:10.4085/1062-6050-45.5.509
5. Arastu MH, Grange S, Twyman R. Prevalence and consequences of delayed diagnosis of anterior cruciate ligament ruptures. Knee Surg Sports Traumatol Arthrosc. 2014;23(4):1201–1205. doi:10.1007/S00167-014-2947-Z
6. Parwaiz H, Teo AQA, Servant C. Anterior cruciate ligament injury: a persistently difficult diagnosis. Knee. 2016;23(1):116–120. doi:10.1016/j.knee.2015.09.016
7. Leblanc MC, Kowalczuk M, Andruszkiewicz N, et al. Diagnostic accuracy of physical examination for anterior knee instability: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):2805–2813. doi:10.1007/S00167-015-3563-2
8. Biz C, Cigolotti A, Zonta F, Belluzzi E, Ruggieri P. ACL reconstruction using a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST): a single-center comparative study. Acta Biomed. 2019;90(Suppl 12):109. doi:10.23750/ABM.V90I12-S.8973
9. Kopkow C, Lange T, Hoyer A, Lützner J, Schmitt J. Physical tests for diagnosing anterior cruciate ligament rupture. Cochrane Database Syst Rev. 2018;2018(12). doi:10.1002/14651858.CD011925.PUB2
10. Hazle C, Duby C. Anterior cruciate ligament injury diagnosis and management in a pediatric patient: a case report. Int J Sports Phys Ther. 2012;7(6):678. /pmc/articles/PMC3537458/.
11. Katz JW, Fingeroth RJ. The diagnostic accuracy of ruptures of the anterior cruciate ligament comparing the Lachman test, the anterior drawer sign, and the pivot shift test in acute and chronic knee injuries. Am J Sports Med. 2016;14(1):88–91. doi:10.1177/036354658601400115
12. Blackburn JT, Norcross MF, Cannon LN, Zinder SM. Hamstrings stiffness and landing biomechanics linked to anterior cruciate ligament loading. J Athl Train. 2013;48(6):764. doi:10.4085/1062-6050-48.4.01
13. Gürpinar T, Polat B, Polat AE, Çarkçi E, Öztürkmen Y. Diagnostic accuracy of lever sign test in acute, chronic, and postreconstructive ACL injuries. Biomed Res Int. 2019;2019. doi:10.1155/2019/3639693
14. Lange T, Freiberg A, Dröge P, Lützner J, Schmitt J, Kopkow C. The reliability of physical examination tests for the diagnosis of anterior cruciate ligament rupture – a systematic review. Man Ther. 2015;20(3):402–411. doi:10.1016/J.MATH.2014.11.003
15. Sobrado MF, Bonadio MB, Ribeiro GF, Giglio PNA, Helito CP, Demange MK. Lever sign test for chronic acl injury: a comparison with Lachman and anterior drawer tests. Acta Ortop Bras. 2021;29(3):132. doi:10.1590/1413-785220212903238345
16. Lichtenberg MC, Koster CH, Teunissen LP, et al. Does the lever sign test have added value for diagnosing anterior cruciate ligament ruptures? Orthop J Sports Med. 2018;6(3). doi:10.1177/2325967118759631/ASSET/IMAGES/LARGE/10.1177_2325967118759631-FIG1.JPEG
17. Lelli A, Di Turi RP, Spenciner DB, Dòmini M. The ‘lever sign’: a new clinical test for the diagnosis of anterior cruciate ligament rupture. Knee Surg Sports Traumatol Arthrosc. 2014;24(9):2794–2797. doi:10.1007/S00167-014-3490-7
18. Massey PA, Harris JD, Winston LA, Lintner DM, Delgado DA, McCulloch PC. Critical analysis of the lever test for diagnosis of anterior cruciate ligament insufficiency. Arthroscopy. 2017;33(8):1560–1566. doi:10.1016/j.arthro.2017.03.007
19. Biz C, Stecco C, Crimì A, et al. Are patellofemoral ligaments and retinacula distinct structures of the knee joint? An anatomic, histological and magnetic resonance imaging study. Int J Environ Res Public Health. 2022;19(3):1110. doi:10.3390/IJERPH19031110
20. Zantop T, Brucker PU, Vidal A, Zelle BA, Fu FH. Intraarticular rupture pattern of the ACL. Clin Orthop Relat Res. 2007;454:48–53. doi:10.1097/BLO.0B013E31802CA45B
21. K. A. Jarbo, D. E. Hartigan, K. L. Scott, K. A. Patel, and A. Chhabra, “Accuracy of the Lever Sign Test in the Diagnosis of Anterior Cruciate Ligament Injuries,” Orthop. J. Sport. Med., vol. 5, no. 10, Jan. 2017, doi: 10.1177/2325967117729809
22. Mulligan EP, Anderson A, Watson S, Dimeff RJ. The diagnostic accuracy of the lever sign for detecting anterior cruciate ligament injury. Int J Sports Phys Ther. 2017;12(7):1057–1067. doi:10.26603/IJSPT20171057
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.