")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Clinical Practice and Effectiveness Analysis of the Management of Corona Virus Disease 2019 Infected at Shanghai Fangcang Shelter Hospital: A Descriptive Study
Authors Zhu J , Zhu GP, Weng YM, Zhang Y, Li BX
Received 2 January 2023
Accepted for publication 23 February 2023
Published 1 March 2023 Volume 2023:16 Pages 337—346
DOI https://doi.org/10.2147/RMHP.S403414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Jian Zhu,1,* Guang-Ping Zhu,2,* Yan-Ming Weng,3,* Yong Zhang,4 Bi-Xi Li5
1Department of Thoracic Cardiovascular Surgery, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 2Department of Endocrinology, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 3Department of Stomatology, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 4Department of Integrative Medicine, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, People’s Republic of China; 5Department of Anesthesiology, General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, Hubei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Zhang; Bi-Xi Li, Tel +86-13986107360 ; +86-13397192089, Email [email protected]; [email protected]
Background: The Fangcang shelter hospital has gradually become the primary management mode in China’s fight against this Corona Virus Disease 2019 (COVID-19) in 2020. In early 2022, the Fangcang shelter hospital management model was successfully applied to the new outbreak of COVID-19 in Shanghai also. Although Fangcang shelter hospitals are no longer the prevailing mode of prevention of COVID-19, the management experience of Shanghai makeshift hospitals is worthy of reference for public health.
Methods: The authors conducted a descriptive statistical analysis of Hall 6-2 of the Shanghai National Convention and Exhibition Center Fangcang shelter hospital. The whole hall of the Fangcang shelter hospital was managed by the one hospital, and the inclusion of third-party management personnel alleviated the shortage of medical personnel human resources. Through practice, a new procedure for treating batch infected people was introduced.
Results: By optimizing ward management, 72 on-duty doctors, 360 on-duty nurses, 3 sense-control administrators, and 15 administrators cured 18,574 infected people in 40 days, and created a record of a doctor managing 700 infected people without compromising the quality of treatment. There have been no deaths and no complaints from the infected people located in Hall 6-2 of the Shanghai National Convention and Exhibition Center Fangcang shelter hospital.
Conclusion: Compared with previous data, the new management mode of Fangcang shelter hospitals provides a reference for the management of the new infectious diseases for public health.
Keywords: COVID-19, Omicron variant, Fangcang shelter hospital, management, Shanghai’s experience
Introduction
The Omicron variant of SARS-COV-2 is highly transmissible but has a significantly lower infection fatality rate than that of the previous variant, such as Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2).1–3 For this social reason, a wave of SARS-CoV-2 infection rapidly appeared in Shanghai, China, in late February 2022.4,5 Although the Omicron variant shows evidence of evolution toward being less virulent, a higher rate of severe outcomes and a considerable mortality rate have been reported in unvaccinated people, especially older adults. In Shanghai, with a population of 25 million, if no strict public health measures are taken, the number of severe to critical cases and the resultant death toll could be high among unvaccinated older people.4 Fangcang shelter hospitals were built in a limited time to accommodate approximately ten thousand mild patients or asymptomatic carriers. The building of such hospitals has been indicated to be an efficient and safe strategy, with most of the infected people completely recovering and no infection being transmitted to the medical staff.6 However, Fangcang shelter hospitals are simple temporary institutions without a standard medical management system. Previous experience showed that one doctor was only responsible for 10 to 15 beds in Fangcang shelter hospitals.6–8 In this article, we report our recent experience with the efficient and practical combination of multiple forces engaging in treatment under the conditions of the Shanghai Fangcang shelter hospital.
The Structure of Hall 6-2 of the Shanghai National Convention and Exhibition Center Fangcang Shelter Hospital
Fangcang shelter hospitals are mostly built in large spaces with adequate ventilation and in locations that can be easily sealed with regard to free access. The Shanghai National Convention and Exhibition Center Fangcang shelter hospital was renovated from the former convention and exhibition center in approximately 10 days. Hall 6-2 has 3538 beds and is divided into Areas D1 to D4, E1 to E8, and F1 to F8. The entrance for infected people, staff and waste exit are all relatively separate. The floor plan with three zones and two passages of total hall is shown in Figure 1a, the floor plan of Hall 6-2 is shown in Figure 1b, and an indoor physical picture is shown in Figure 1c. The doctors’ office and nurses’ office are located on opposite sides. At each access point, there are staff members who are responsible for infection control and who regulate entrances or exits and help the medical staff wear and take off their personal protective equipment (Figure 2a and b). Each nurses’ station has its own pharmacy, where the nurses dispense medicines based on a doctor’s prescription. Each nurse station also has an emergency room, which includes ventilators, surgical incision and suture kits, electrocardiograph monitoring instruments, defibrillators and other complete medical equipment and first-aid drugs. In addition, there are two police office rooms, one psychological consultation room, two study and reading rooms, and three dance venues in Hall 6-2.
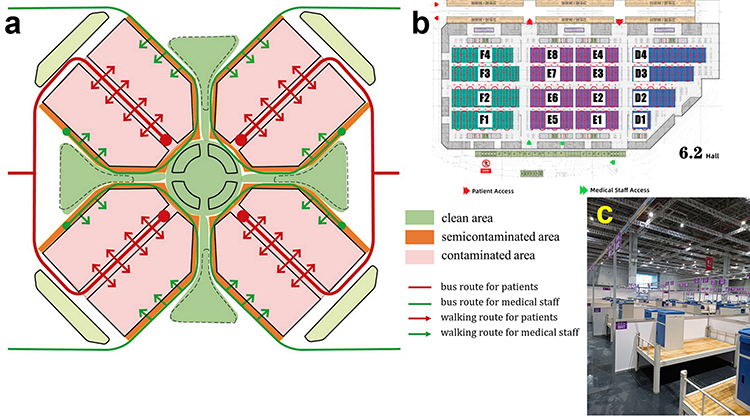 |
Figure 1 The Shanghai National Convention and Exhibition Center Fangcang shelter hospital (a) plane diagram of passages for monolithic architecture; (b) plane diagram of zones and passages for Hall 6-2; (c) realistic photograph. |
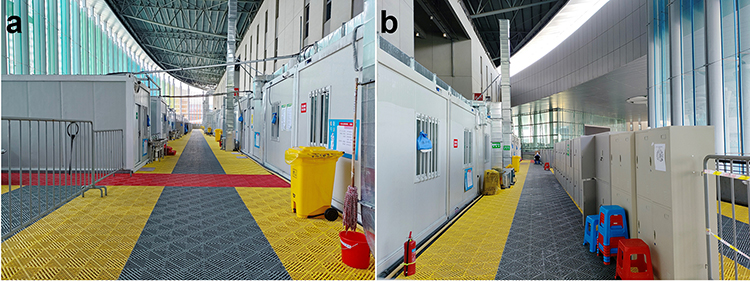 |
Figure 2 Access to the locker room (a) medical staff; (b) third-party personnel. |
Medical Staff Management
Seventy on-duty doctors, 360 on-duty nurses, and 10 administrators were divided into ten groups. Two doctors are responsible for coordination and medical exchanges with local affiliated hospitals. Each group worked 4 hours in a cycle. Inside the wardroom, the doctors are assigned as follows: two doctors are in charge of receiving and transferring infected people, and the remaining five doctors are in charge of judging the condition of infected people. Therefore, one doctors should cover more than 700 beds. These five doctors are guaranteed to include one respiratory doctor, one circulatory doctor, and one neurological doctor. Later, experience showed that a surgeon was also necessary. This is because some surgical procedures are more difficult for physicians to perform while wearing protective clothing. These include changing the dressing of fistula tube, catheterization and cystostomy in patients with benign prostatic hyperplasia. With surgeons, the medical care in the Fangcang Shelter Hospital is a completely complex. With the exception of respiratory symptoms, all other conditions required handover and the Shanghai Fangcang shelter hospital app discussion. This greatly reduces handover time and improves the efficiency of dealing with specific symptoms and diseases. In terms of nursing, one nurse can cover 150 to 200 beds, and three to six nurses assist in infection control, such as being responsible for infection control by regulating the entrances or exits and helping the medical staff in wearing and taking off their personal protective equipment, and the supervision and correction of infection control inside the wardroom. PCR tests and antigen tests for SARS‐CoV-2 are carried out daily by medical staff.
Patients or Infected People Admission Criteria
The admission and standards of infected people are jointly decided on by the government’s epidemic prevention department and the main doctors in the Fangcang shelter hospitals. The government’s principle is that people with mild patients or asymptomatic carriers are sent to Fangcang shelter hospitals. Doctors would turn away high-risk patients to Fangcang shelter hospitals, such as acute exacerbations of chronic diseases or severe symptoms of COVID-19. Doctors, patients or infected people, and government officials all have veto power, but they must give proper reasons for their decisions, including who violates temporary quarantine regulations and who will take legal responsibility. Generally, only confirmed cases of asymptomatic carriers or patients with mild severity should be accommodated. Because infected people are transported in batches by bus, the process of receiving and triaging infected people is very important. The procedures for receiving batch patients or infected people include screening, asking, checking, and guiding them. Please see the flow chart for the specific process (Figure 3). A few matters that need attention other than admission include avoiding bus congestion and guiding buses in driving away on time as soon as possible. After monitoring their symptoms’, infected people are generally considered for several hours before being accepted to the Fangcang shelter hospital. A reasonable explanation for not being accepted by Fangcang shelter hospital can calm the mood of those who are rejected by the Fangcang shelter hospital. Giving the infected people who had been turned away from the Fangcang shelter hospital a free bus ride back would have warmed their hearts. Some infected people arrive wearing protective clothing and isolation clothing, which should be removed at the entrance of the Fangcang shelter hospital. The Shanghai Fangcang shelter hospital app should be scanned when entering to ensure that infected information is identified and managed by doctors, nurses, and government officials. After the abovementioned procedures are completed, the infected people are officially admitted to the Fangcang shelter hospital. Upon admission, each infected individual receives a free care package, including toiletries, towels, disinfectants, protective gloves, cutlery, short-term snacks, lamps and more.
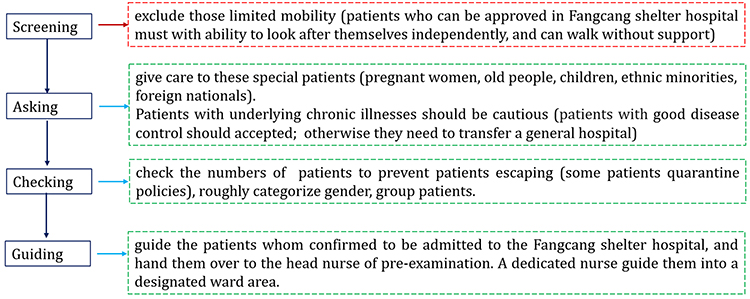 |
Figure 3 The process of procedures for receiving batches of patients. |
Patients or Infected People Management
Infected information, such as medical history and symptoms, is reported by patients or infected people through the Shanghai Fangcang shelter hospital app. Some special infected people, volunteers and nurses assisted in filling in the information provided by the Shanghai Fangcang shelter hospital app; these volunteers were previously infected people in the Fangcang shelter hospital (they are changed with admission and discharge). Medical staff can quickly receive infected individuals information through relevant instructions provided via the medical manager identity of this app. This greatly reduces the workload and ensures the accuracy of relevant data. Medical records, doctor orders, and nursing documents can all be generated in batches according to these data. Having a fixed time period of admission and discharge arrangements has greatly optimized the management procedures of infected people in the Fangcang shelter hospital. Generally, the infected who meet the discharge criteria of the Fangcang shelter hospital will be sent to one of the isolation centers that are located in each community by bus the following morning. This same bus will take the newly found patients or infected people within these communities back to the shelter hospital in the afternoon. All daily necessities (including tissues, toothpaste, and sanitary napkins for women), meals, and disease treatment are provided free by the government. Compared to the members of the general population who are not infected, patients or infected people are provided with better free meals (including afternoon tea and late-night snacks). In addition, government policies advocate that infected people receive normal labor wages, medical compensation and other legitimate rights and interests.
Most of the country’s anti-epidemic policies and doctors’ general treatment plans are taught to infected people by volunteers in the Fangcang shelter hospital. Infected peoples’ concerns and appeals are often conveyed to doctors by volunteers. In addition, volunteers are responsible for distributing food, drink, and daily consumption to all infected people.
Treatment Process Management
Infected individuals without special symptoms should not be given as much as medicine possible. Symptom relief for infected peoples’ symptoms is necessary. Therefore, there are some types of treatment willingness available for confirmed infected people. Most infected people are responsive to the government’s quarantine policy and trust doctors’ customized treatment plans. Some infected people are afraid of this disease and complain of various uncomfortable symptoms every day in the hope of receiving more drug treatment or even defrauding the offer of antibiotic treatment. Based on this phenomenon, only one doctor is allowed to prescribe drugs at a fixed time for each group on duty, and antibiotics are strictly controlled. Of course, medicines are readily available in an emergency. An even smaller number of infected people refuse to take any medication at all. Their living conditions in the Fangcang shelter hospital are more comfortable than if they were isolated at home. These last two types of patients require psychotherapy by a neurological doctor. In addition, approximately 15.68% of those confirmed patients or infected people in Hall 6-2 have a chronic disease that requires them to take medication. Aggressive treatment, including blood glucose testing, electrocardiogram testing, and blood pressure monitoring, is needed. Especially for expensive cancer drugs, the government can guarantee normal outcomes for free.
PCR tests for SARS‐CoV-2 were performed daily on each infected. There were no routine blood, liver or kidney function tests or other blood test conditions. For people at high risk of thrombosis, antiplatelet aggregation or anticoagulant drugs can be given, but coagulation function is not detected. Chest CT scans are repeated every week until the related issues are resolved or referral criteria are met; doctors can also arrange chest CT scan examinations in special conditions. If the PCR test for SARS-CoV-2 was negative two consecutive times with an interval of more than 24 hours between the tests, the body temperature was normal for more than 3 days, and the infected had no clinical symptoms, then he or she was discharged. Then, they must engage in up to fourteen days of home isolation.
Generally, no special disease progresses while an infected individual is in the shelter hospital, and transfers are thus rarely attempted. Except for two infected individual who were transferred due to persistent high fever, no infected individual was transferred due to the exacerbation of pneumonia symptoms. Other reasons for transfer include the acute exacerbation of chronic diseases, strong referral requests, and drug abstinence. The hospital transfer procedure is similar to the discharge of the infected people, which summarizes the diagnosis and treatment process of the infected people in detail, the current state of the disease, and the special matters that need to be explained.
Third-Party Personnel Management
Third-party personnel mainly include police, fire personnel, water and electricity maintenance personnel, and cleaning personnel. They are responsible for the maintenance of order in the Fangcang shelter hospital, the repair of water and electricity faults, and the cleaning of domestic garbage and other daily life maintenance and services. These individuals receive a rigorous course regarding wearing and taking off protective clothing before entering the workplace. PCR tests and antigen tests for SARS-CoV-2 are carried out daily for these third-party personnel. There are staff members responsible for infection control who regulate the entrances and exits and who help the third-party personnel wear and take off their personal protective equipment. Each shift has thirty cleaning personnel, two water and electricity maintenance personnel; in addition, three police and fire personnel are located outside the Fangcang shelter hospital.
Daily and Living Support for Infected People in Fangcang Shelter Hospital
In addition to mobile phones, infected people can enter Fangcang shelter hospitals without carrying any other daily necessities. The Chinese government provides everything that infected people need for free. Daily necessities include disposable underwear, towels, toothpaste, toothbrush, shampoo, washing bucket, disposable razors, nail clippers, pads or tampons, douches, wipes, feminine sprays and so on. In terms of food, in addition to three meals, there are also late-night snacks here. Breakfast includes eggs, milk, bread, ham sausage, and Chinese pasta. There are two meat dishes and three vegetarian dishes for lunch and dinner (the meals of ethnic minorities will be specially prepared according to their customs). Meals vary from day to day and are guaranteed to be hot. All food is free in Fangcang shelter hospital. In terms of water, mineral water and warm water are free in 7×24 hours. There is no line to wash your hands. The shower room is divided into men and women, and the line time is within 5 minutes. These are also free. The indoor temperature is comfortable (a little hot for medical staff who wear protective clothing). Chargers, lamps, and electrical sockets are provided free of charge at each bed, and the electricity is continuously supplied 7×24 hours. The equipment, which is provided free in hall, will be repaired or replaced within 10 minutes by the hall’s maintenance personnel. Due to the concentration of personnel in the hall, the communication department added mobile phone signal enhancement equipment, the communication inside the hall was barrier-free, and the network speed was good 5G network. In terms of drug safety, some expensive targeted anti-cancer drugs, special vision protection devices and needles for insulin injection can be provided free of charge in a timely manner.
Results
The data were obtained from the Shanghai Fangcang shelter hospital app. From 10 April 2022 to 20 May 2022, 18,574 infected people were cured in Hall 6-2 of the Shanghai National Convention and Exhibition Center Fangcang shelter hospital. There were 10,843 males and 7731 females. The youngest was 1 year old, and the oldest was 89 years. There were 1246 infected people over the age of 65 years. The most common chronic diseases among infected people in Hall 6-2 were hypertension and diabetes, for details were Figure 4. A total of 107,398 PCR tests for SARS‐CoV-2 were performed in Hall 6-2. The average number of days between SARS-CoV-2 PCR test results from positive to negative in each area (D1-F4) was 3.1–3.8 days. The number of infected people hospitalized for more than 10 days was 1467. A total of 117 infected people were referred to specialized hospitals for further treatment due to worsening conditions or additional patient requirements. A PCR test for SARS-CoV-2 reactivation occurred in 444 infected people within one week of discharge. The places where these infected people are suspected to have contracted COVID-19 are shown Figure 5. There were 300 infected people who had not been vaccinated against SARS-CoV-2 among these cured infected people, and Figure 6 shows the details of vaccination against SARS-CoV-2. From 10 April 2022 to 20 May 2022, there were no medical accidents or deaths in Hall 6-2 of the Shanghai National Convention and Exhibition Center Fangcang shelter hospital.
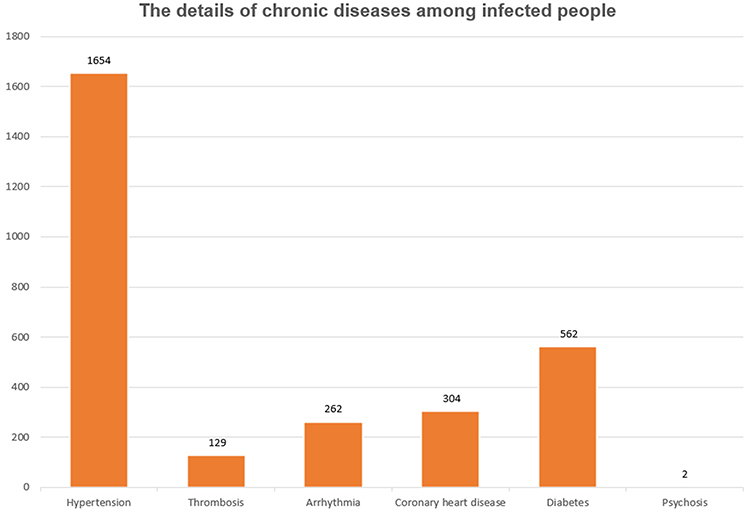 |
Figure 4 The details of chronic diseases among infected people. |
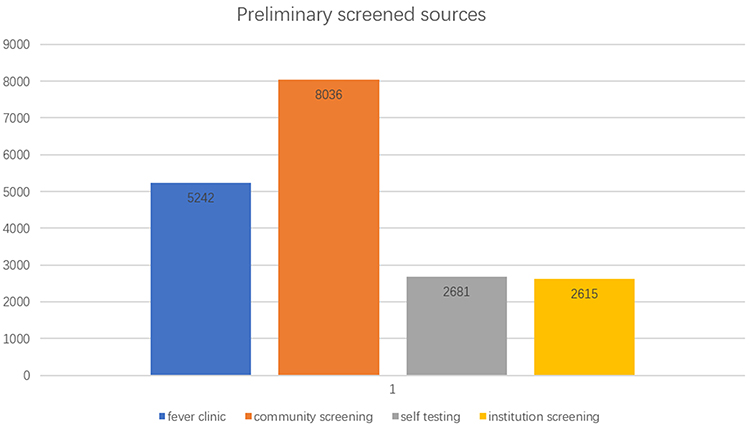 |
Figure 5 Sources of suspected COVID-19 patients determined in preliminary screening. |
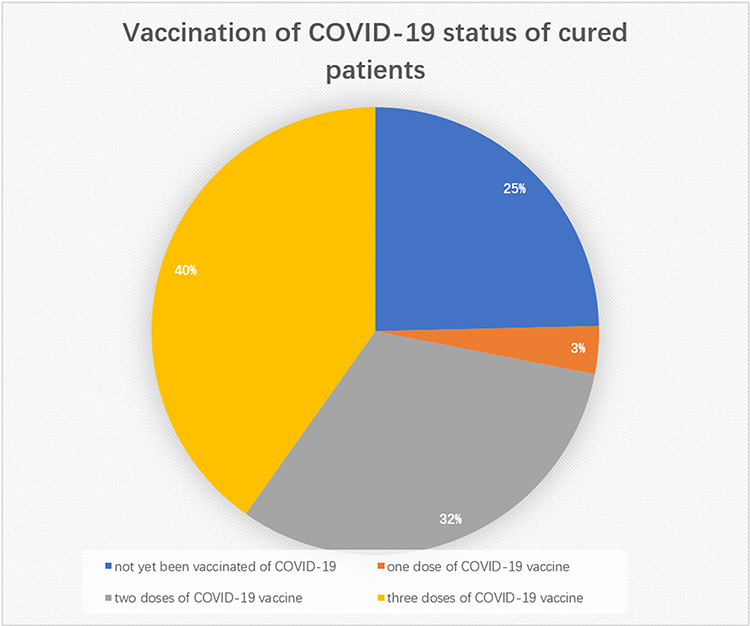 |
Figure 6 Vaccination status confirmed by COVID-19 patients. |
Discussion
Since COVID-19 was first reported in Wuhan, the Fangcang shelter hospital model has gradually become the primary management mode in China’s fight against this respiratory infectious disease.9–15 Such facilities can provide a large volume of comprehensive placement for medical treatment, refuge, daily life, and study in a short time.7,8 This approach eliminates confirmed asymptomatic carriers or patients with mild cases of COVID-19 as a source of transmission.8,13,16 Experiments from some regions have shown that Fangcang shelter hospitals are feasible and do not require a large amount of investment, although further improvements and complete systems are needed in terms of form, regulation, and treatment procedures.14,15,17,18 The management mode of Shanghai Fangcang shelter hospital has been further optimized and upgraded in the following aspects.
First, there are more mature models for managing medical staff, with fewer medical staff curing for more infected people in a short time. We created a record of a doctor managing 700 infected people without compromising the quality of treatment. Two years ago, each doctor was responsible for the management of 10 to 15 patients or infected people.15 The reasons may be the follows: the distribution model of the personnel in Fangcang shelter hospitals was based on medical staff coming from different hospitals and departments in 2020.17–20 The medical workers in Hall 6-2 of the Shanghai National Convention and Exhibition Center Fangcang shelter hospital come from the same hospital (General Hospital of Central Theater Command of the People’s Liberation Army); they all know each other and have a unified medical management style. Thus, they are more able to demonstrate good executive ability and have a higher desire to perform, to present, and to contribute. It is also easier for organizers to adjust positions and make emergency decisions according to the needs of the working.21–23 More importantly, this characteristic helps centralize the management of infection control.21,24,25 When assigning specialties to each medical duty group, consideration should be given to integrity.24–26 Respiratory doctors, circulatory doctors, digestive doctors, metabolic system doctors, nervous system doctors, and surgeons all need to be considered. At the same time, attention should be given to the distribution of professional titles. Doctors with more first-aid experience should be considered the group leader on duty.21,22,24
Second, third-party personnel and volunteers have been brought in, which has reduced the nonmedical work of medical staff. Police, fire personnel, water and electricity maintenance personnel, cleaning personnel, and third-party personnel provide good logistical support. In such a large public space, the infected people’s safety can be guaranteed, lives can be lived freely, and the demand for food can be satisfied. Individuals have enough energy to study, exercise and present themselves.15,17–19 Small square dances, singing parties and wall paintings are all allowed. Interestingly, some of individuals have fallen in love in the Fangcang shelter hospital. The volunteers were all previously hospitalized infected people with confirmed SARS-CoV-2 infection. Thus, they are more aware of and able to better express the needs of infected people to the government and doctors and can publicize the government’s anti-epidemic policies and medical treatment plans with doctors and nurses.27–29 Therefore, journalists, lawyers, and teachers have priority in applying for volunteer positions. Of course, the government will issue a certificate of honor to volunteers who participate in the advanced selection of his or her work institution.
Third, the daily livelihood of the infected people in the Fangcang shelter hospital is guaranteed, which increases patient or infected people cooperation. Food, drink, medical care, and daily consumption needs are all freely provided to all infected people. In contrast, ordinary residents who are confined to the community need to make more effort to obtain food. Even at elevated costs, some of the higher priced vegetables and fruits are bought.30 Therefore, some infected people are not willing to leave the Fangcang shelter hospital even when they are cured. Even so, some confirmed SARS-CoV-2 patients or infected people are very resistant to being admitted to Fangcang shelter hospitals. At this time, government departments are organizing specialized personnel for door-to-door counseling or 7×24 hours of surveillance to prevent these individuals from becoming sources of infection.
Fourth, the health of medical staff is guaranteed, and their work efficiency and enthusiasm are improved. Changing shifts around the clock cause sleep disturbances. Eating cuisine from different provinces can make them uncomfortable. Infection-control policies require treating every colleague as if they are an infected people, and each medical staff member is thus firmly confined to his or her own room.15–18 Daily supplies are delivered to the door by special personnel. Consequently, the hearts of medical staff members are extremely fragile. Therefore, hospital management organizes many online heart-to-heart talks, skill learning sessions, and entertainment activities for them. Cokes, specialty snacks, and yoga mats are supplied via a special aisle. At the same time, the work institution also works to solve family difficulties for medical staff members fighting the epidemic. The media also plays up the accolades of medical staff members. Therefore, they remain at ease and actively engaged in their work.31,32
Fifth, efficient software and information maintenance capabilities make medical paperwork easy to handle. Patients or infected people information, such as medical history and symptoms, is reported by patients or infected people through the Shanghai Fangcang shelter hospital app.33–35 From passively asking patients or infected people questions to actively filling out the questionnaire, cooperation has significantly improved. Medical staff can also quickly receive patients or infected people information through relevant instructions obtained from the medical manager identity of this app, thereby reducing the occurrence of fear related to making mistakes in this frantic work environment when wearing airtight protective clothing.36–42
In summary, the Fangcang shelter hospital is run successfully based on efficient and practical combinations from multiple forces who are engaged in working under the conditions of Shanghai Fangcang shelter hospital with limited facilities and medical staff. It is an effective and safe method of isolating infected people, providing basic medical care and identifying potential severe cases very early on. Persistence in using this dynamic approach has led to zero COVID-19 community transmissions in Shanghai. Compared with previous data, the new management mode of Fangcang shelter hospitals provides a reference for the management of the new infectious diseases for public health.
Data Sharing Statement
Data are available in a public, open access repository.
Ethics Statement
This study complies with the guidelines for human studies and is in accordance with the Declaration of Helsinki. Written informed consent for participation was not required for this study in accordance with the hospital legislation and the institutional requirements. This is a public health management experience report; thus, no medical ethics statement is needed according to the Ethics Review Committee of General Hospital of Central Theater Command of the Chinese People’s Liberation Army.
Patient and Public Involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, agreed to the submitted journal, and agreed to be accountable for all aspects of the work. These authors contributed equally to this work and should be considered as co-first authors: Jian Zhu, Guang-Ping Zhu and Yan-Ming Weng.
Funding
The authors do not declare a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu Y, Yu Y, Zhao Y, He D. Reduction in the infection fatality rate of Omicron variant compared with previous variants in South Africa. Int J Infect Dis. 2022;120:146–149. doi:10.1016/j.ijid.2022.04.029
2. Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. doi:10.1136/postgradmedj-2020-138234
3. Umakanthan S, Patil S, Subramaniam N, Sharma R. COVID-19 vaccine hesitancy and resistance in India explored through a population-based longitudinal survey. Vaccines. 2021;9(10):1064. doi:10.3390/vaccines9101064
4. Zhang X, Zhang W, Chen S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet. 2022;399(10340):2011–2012. doi:10.1016/S0140-6736(22)00838-8
5. Liu Y, Xu L, Piao X, et al. Epidemiological, clinical, and household transmission characteristics of children and adolescents infected with SARS-CoV-2 Omicron variant in Shanghai, China: a retrospective, multicenter observational study. Int J Infect Dis. 2023;129:1–9. doi:10.1016/j.ijid.2023.01.030
6. Chen S, Zhang Z, Yang J, et al. Fangcang shelter hospitals: a novel concept for responding to public health emergencies. Lancet. 2020;395(10232):1305–1314. doi:10.1016/S0140-6736(20)30744-3
7. Shi F, Li H, Liu R, et al. Emergency preparedness and management of mobile cabin hospitals in China during the COVID-19 pandemic. Front Public Health. 2022;9:763723. doi:10.3389/fpubh.2021.763723
8. Liu P, Zhang H, Long X, et al. Management of COVID-19 patients in Fangcang shelter hospital: clinical practice and effectiveness analysis. Clin Respir J. 2021;15(3):280–286. doi:10.1111/crj.13293
9. Contini C, Di Nuzzo M, Barp N, et al. The novel zoonotic COVID-19 pandemic: an expected global health concern. J Infect Dev Ctries. 2020;14(3):254–264. doi:10.3855/jidc.12671
10. Liu M, Shi L, Chen H, et al. Comparison between China and Brazil in the two waves of COVID-19 prevention and control. J Epidemiol Glob Health. 2022;12:1–14. doi:10.1007/s44197-022-00036-6
11. Feng S, Zhang J, Li J, et al. The impact of quarantine and medical resources on the control of COVID-19 in Wuhan based on a household model. Bull Math Biol. 2022;84(4):47. doi:10.1007/s11538-021-00989-y
12. Cai Y, Chen Y, Xiao L, et al. The health and economic impact of constructing temporary field hospitals to meet the COVID-19 pandemic surge: Wuhan Leishenshan Hospital in China as a case study. J Glob Health. 2021;11:05023. doi:10.7189/jogh.11.05023
13. Lim KX, Chen YT, Chiu KM, Hung FM. Rush hour: transforma modern hotel into cloud-based virtual ward care center within 80 hours under COVID-19 pandemic. Far eastern MemorialHospital’s experience. J Formos Med Assoc. 2022;121(4):868–869. doi:10.1016/j.jfma.2021.10.023
14. Lu J, Zhao M, Wu Q, et al. Mental health needs of the COVID-19 patients and staff in the Fangcang shelter hospital: a qualitative research in Wuhan, China. Glob Ment Health. 2021;8:e33. doi:10.1017/gmh.2021.23
15. Chen S, Zhang P, Zhang Y, et al. Coordinated management of COVID-19 response: lessons from whole-of-society and whole-of-health strategies in Wuhan, China. Front Public Health. 2021;9:664214. doi:10.3389/fpubh.2021.664214
16. Butkiewicz S, Zaczyński A, Hampel M, Pańkowski I, Gałązkowski R, Rzońca P. Analysis of risk factors for in-hospital death due to COVID-19 in patients hospitalised at the temporary hospital located at the national stadium in Warsaw: a Retrospective Analysis. Int J Environ Res Public Health. 2022;19(7):3932. doi:10.3390/ijerph19073932
17. Fang D, Pan S, Li Z, et al. Large-scale public venues as medical emergency sites in disasters: lessons from COVID-19 and the use of Fangcang shelter hospitals in Wuhan, China. BMJ Glob Health. 2020;5(6):e002815. doi:10.1136/bmjgh-2020-002815
18. Li J, Yuan P, Heffernan J, et al. Fangcang shelter hospitals during the COVID-19 epidemic, Wuhan, China. Bull World Health Organ. 2020;98(12):830–841D. doi:10.2471/BLT.20.258152
19. Gu Y, Zhu Y, Xu F, Xi J, Xu G. Factors associated with mental health outcomes among patients with COVID-19 treated in the Fangcang shelter hospital in China. Asia Pac Psychiatry. 2021;13(2):e12443. doi:10.1111/appy.12443
20. Zhou L, Rong X, Fan M, et al. Modeling and evaluation of the joint prevention and control mechanism for curbing COVID-19 in Wuhan. Bull Math Biol. 2022;84(2):28. doi:10.1007/s11538-021-00983-4
21. Cao Y, Li Q, Chen J, et al. Hospital emergency management plan during the COVID-19 epidemic. Acad Emerg Med. 2020;27(4):309–311. doi:10.1111/acem.13951
22. Ma X, Li S, Yu S, et al. Emergency management of the prevention and control of novel coronavirus pneumonia in specialized branches of hospital. Acad Emerg Med. 2020;27(4):312–316. doi:10.1111/acem.13958
23. Umakanthan S, Senthil S, John S, et al. The effect of statins on clinical outcome among hospitalized patients with COVID-19: a multi-centric cohort study. Front Pharmacol. 2022;13:742273. doi:10.3389/fphar.2022.742273
24. Arredondo A, Ogedegbe C, Hoffman JR, Goldfrank LR, Wall SP, Smith TY. Emergency medicine’s role in the crossroads of social revolution and the COVID-19 pandemic. Acad Emerg Med. 2020;27(12):1350–1352. doi:10.1111/acem.14155
25. Ragazzoni L, Barco A, Echeverri L, et al. Just-in-time training in a tertiary referral hospital during the COVID-19 pandemic in Italy. Acad Med. 2021;96(3):336–339. doi:10.1097/ACM.0000000000003575
26. Zakaria A. Connections lead to trainee courage during the COVID-19 pandemic in a community hospital setting. Acad Med. 2021;96(7):943. doi:10.1097/ACM.0000000000004024
27. Parravicini S, Provenzi L, Barello S, et al. The experience of child neuropsychiatry residents who volunteered in Italian COVID-19-designated hospitals. Acad Psychiatry. 2021;45(5):587–592. doi:10.1007/s40596-021-01442-x
28. Lyon ZM, Yang R, Savoie MB, et al. Rapid implementation of a volunteer-run service to combat social isolation in hospitalized patients during the COVID-19 pandemic. Am J Med Qual. 2021;36(1):63. doi:10.1097/01.JMQ.0000733452.79287.c2
29. Niccolai L, Shelby T, Weeks B, et al. Community trace: rapid establishment of a volunteer contact tracing program for COVID-19. Am J Public Health. 2021;111(1):54–57. doi:10.2105/AJPH.2020.305959
30. Sayyed A, Baker ML, Peesay T, Rooney A, Syed Z. An auxiliary medical education: the evolution of a medical student-founded organization in response to the COVID-19 era personal protective equipment shortage. Acad Med. 2021;96(12):1663–1670. doi:10.1097/ACM.0000000000004185
31. Arghittu A, Deiana G, Dettori M, et al. Web-based analysis on the role of Digital Media in Health Communication: the experience of VaccinarSinSardegna Website. Acta Biomed. 2021;92(S6):e2021456. doi:10.23750/abm.v92iS6.12072
32. Farrell CM, Hayward BJ. Ethical dilemmas, moral distress, and the risk of moral injury: experiences of residents and fellows during the COVID-19 pandemic in the United States. Acad Med. 2022;97(3S):S55–S60. doi:10.1097/ACM.0000000000004536
33. Jiang H, Song P, Wang S, et al. Quantitative assessment of the effectiveness of joint measures led by Fangcang shelter hospitals in response to COVID-19 epidemic in Wuhan, China. BMC Infect Dis. 2021;21(1):626. doi:10.1186/s12879-021-06165-w
34. Lu C, Wang HY, Chen X, et al. Clinical characteristics of 1327 patients with coronavirus disease 2019 (COVID-19) in the largest Fangcang shelter hospital in Wuhan. Chin Med J. 2020;134(2):241–242. doi:10.1097/CM9.0000000000001194
35. Shang L, Xu J, Cao B. Fangcang shelter hospitals in COVID-19 pandemic: the practice and its significance. Clin Microbiol Infect. 2020;26(8):976–978. doi:10.1016/j.cmi.2020.04.038
36. Kassaeian S, Gohari A, Masoumi G, Ghomian Z, Dehghani A. Post-hospital discharge strategy for COVID-19 treatment and control: focus on fangcang hospitals. Disaster Med Public Health Prep. 2021;1–3. doi:10.1017/dmp.2021.83
37. Wang X, Wang J, Shen J, et al. Facilities for centralized isolation and quarantine for the observation and treatment of patients with COVID-19. Engineering. 2021;7(7):908–913. doi:10.1016/j.eng.2021.03.010
38. Feng Q, Zhou H, Wang L, Kang C. A study on the effect of the pre-go-live training in anxiety and depression of medical staff based on the data of Wuhan Fangcang shelter hospital during COVID-19 in the era of big data. Front Public Health. 2022;10:909241. doi:10.3389/fpubh.2022.909241
39. Zhou W, Wang A, Wang X, Cheke RA, Xiao Y, Tang S. Impact of hospital bed shortages on the containment of COVID-19 in Wuhan. Int J Environ Res Public Health. 2020;17(22):8560. doi:10.3390/ijerph17228560
40. Guo T, Liu X, Xu C, et al. Fangcang Shelter Hospital in Wuhan: a radiographic report on a cohort of 98 COVID-19 patients. Int J Med Sci. 2020;17(14):2125–2132. doi:10.7150/ijms.48074
41. Umakanthan S, Bukelo MM, Gajula SS. The Commonwealth Caribbean COVID-19: regions resilient pathway during pandemic. Front Public Health. 2022;10:844333. doi:10.3389/fpubh.2022.844333
42. Lei N, Li BX, Zhang KF, Bao H, Ding J, Wang Y. Analysis of the protective effect of infection controllers supervising third-party personnel entering and leaving Shanghai Fangcang Shelter Hospital. Infect Drug Resist. 2022;15:7519–7527. doi:10.2147/IDR.S388707
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.