Back to Journals » Infection and Drug Resistance » Volume 13
Clinical Performance of BD Kiestra InoqulA Automated System in a Chinese Tertiary Hospital
Authors Yue P ![]() , Zhou M
, Zhou M ![]() , Zhang L, Yang Q, Song H, Xu Z, Zhang G
, Zhang L, Yang Q, Song H, Xu Z, Zhang G ![]() , Xie X, Xu Y
, Xie X, Xu Y ![]()
Received 8 January 2020
Accepted for publication 10 March 2020
Published 1 April 2020 Volume 2020:13 Pages 941—947
DOI https://doi.org/10.2147/IDR.S245173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Pinli Yue,1,* Menglan Zhou,1– 3,* Lintao Zhang,1,* Qiwen Yang,1 Hongmei Song,1 Zhipeng Xu,1 Ge Zhang,1 Xiuli Xie,1 Yingchun Xu1
1Department of Clinical Laboratory, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing 100730, People’s Republic of China; 2Graduate School, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing 100730, People’s Republic of China; 3Beijing Key Laboratory for Mechanisms Research and Precision Diagnosis of Invasive Fungal Diseases, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiwen Yang; Yingchun Xu Email [email protected]; [email protected]
Background: The aim of this study was to evaluate the clinical performance of the BD Kiestra InoqulA automated specimen processing system with commonly encountered clinical microbiology specimens.
Materials and Methods: Four types of clinical specimens (sputum, urine, normally sterile body fluids, and feces) were inoculated onto relevant agar plates using a manual method and the BD Kiestra automated system. The number of isolated pathogen species, number of isolated single colonies and uniformity of plate streaking were calculated and compared between two methods.
Results: Significantly more isolated colonies were observed on plates inoculated by InoqulA for all specimen types and media with the exception of sputum specimens inoculated onto chocolate agar with vancomycin (P =0.076) and urine onto China blue agar (P =0.856). The quality of plate streaking was also better with InoqulA for all specimen types and media with the exception of urine specimens (P =1.000) and sterile body fluids (P =0.56) inoculated onto China blue agar.
Conclusion: This is the first evaluation study of InoqulA with 4 types of clinical specimens in China. It focused on the effect of streaking plates automatically with the magnetic bead. Inoculation of clinical specimens with the BD Kiestra InoqulA system is superior to the manual method for recovery of single colonies and the overall quality of semi-quantitative plate streaking.
Keywords: BD Kiestra, InoqulA, microbiology automation
Introduction
Automation of specimen processing has historically been adopted slowly in clinical microbiology laboratories due to the complexity of processing different types of specimens received in a variety of transport containers.1 However, inoculation and streaking of culture plates to obtain isolated colonies is a fundamental process in the clinical microbiology laboratory and one that should be amenable to automation.2 Furthermore, with the global consolidation of diagnostic testing into core facilities, many laboratories are confronted with increasing numbers of clinical specimens that need to be processed more efficiently than was done with traditional manual methods. To better meet these needs, automated inoculation systems have been introduced in markets including BD Kiestra InoqulA (BD Integrated Diagnostic Solutions, Sparks, MD) and Copan WASP (Brescia, Italy).3
In China, laboratory automation was introduced many years ago in several clinical diagnostic disciplines such as hematology and molecular biology.4 To improve work efficiency and provide high-quality services at the lowest possible price, most Chinese clinical microbiology laboratories have automated various tasks, such as blood culture monitoring, Gram staining, and pathogen identification. With the increase of clinical sample volume, it is necessary to introduce automated inoculation systems, which can help improve clinical microbiology laboratory workflow, save labors, decrease repetitive tasks, and reduce overtime payments.
Although the BD Kiestra InoqulA system was originally introduced in 2006 and has been evaluated in the United States and Europe,5–7 the system was only recently approved for use in China and this is the first evaluation of the system performance. Additionally, previous studies primarily focused on processing urine specimens and not more challenging specimens where a heavy growth of multiple organisms may be encountered. In this study, we compared processing with an automated method and a manual method with four common clinical specimens: sputum, urine, normally sterile body fluids, and feces.
Materials and Methods
Clinical Specimens
A total of 200 samples were randomly selected from inpatient specimens received in Peking Union Medical College hospital from December 2015 to March 2016. Fifty samples each of sputum, urine, sterile body fluids, and feces were evaluated.
Reagents
The media (Oxoid, England) used in this study were: Columbia agar with 5% sheep blood (blood agar), vancomycin-containing chocolate agar (V-Choc agar), China blue agar (a strong selective medium which is similar to MacConkey agar plate; CB agar), and xylose-lactose-desoxycholate agar (XLD agar). Sputasol (Oxoid, England) was used to digest the sputum specimens.
Automated Microbiology Inoculation System
In this study, we evaluated the BD Kiestra InoqulA automated microbiology inoculation system. To better adapt to the diversity of microbiology specimens, it consists of two modules, one for fully automated processing of liquid specimens and a semi-automatic manual module for processing tissue specimens. A specimen can be inoculated onto up to 5 plates simultaneously with both modules and in our experience 200–300 plates can be processed per hour. Proper dispensing is monitored in the fully automated module with an imaging system that records the plate inoculation. All plates are streaked with magnetic beads in customized predetermined patterns (eg, 4-quadrant pattern, zig-zag pattern, uniform lawn pattern). The inoculation and streaking are performed in a closed, HEPA-filtered system, that can effectively avoid contamination of adjacent specimens and the environment.
Pretreatment and Inoculation
Each specimen was processed both manually and automatically. Although specimens are traditionally inoculated onto agar plates manually using an inoculation loop, a 10 μl pipette was used in this study so the same volume of specimen was inoculated onto each plate.
Manual Specimen Pretreatment and Inoculation
(i) Sputum. Specimens were treated with equal volume of sputasol, vortex 1 min, and then held for 30 mins at room temperature; 10 μL of digested samples was dispensed onto each of three different plates (blood agar, V-Choc agar, and CB agar) and streaked in a 4-quadrant pattern with an inoculation loop.
(ii) Urine. A volume of 10 μL was dispensed onto blood agar plates and then the entire plate surface was streaked with an inoculation loop in a continuous streaking pattern with 60-degree rotation twice. This plate was used for quantification of growth. CB agar plates were inoculated with 10 μL samples and 4-quadrant streaking was performed with the inoculation loop. This plate was used to obtain isolated colonies.
(iii) Sterile body fluids. A volume of 10 μL samples was dispensed onto blood agar and CB agar plates and then 4-quadrant streaking was performed with an inoculation loop.
(iv) Feces. A disposable sterile swab was used to pick up feces, applied it to the XLD agar and CB agar plates, and then 4-quadrant streaking was performed with an inoculation loop.
Automated Specimen Pretreatment and Inoculation
(i) Sputum. A minimum of 0.5 mL of the sputasol-treated sputum specimens prepared for manual processing was dispensed into sterile capped vacuum tubes. The tubes were labeled and placed on the specimen rack of the instrument. A volume of 10 μl was automatically dispensed on the three agar plates and streaked with magnetic beads in a 4-quadrant pattern.
(ii) Urine and sterile body fluids. A minimum of 0.5 mL samples was added to sterile vacuum tubes with disposal sterile tips and the tubes were capped tightly. The tubes were labeled and placed on the specimen rack of the instrument and the inoculation was performed automatically. Confluent streaking was applied to blood agar plates with urine specimen and 4-quadrant streaking was applied to other plates with the same volume of 10 μL.
(iii) Feces. A disposable sterile swab was used to pick up feces from the suspected lesion and manually applied it to the light-marked position on the plates. Plate streaking was performed automatically in a 4-quadrant pattern with magnetic beads.
All plates inoculated with the manual and automated methods were placed into a 5% CO2, 35°C incubator. The BD Kiestra ReadA Compact was not used for this study so the incubation conditions were identical for all plates. The plates were examined after 24 hrs and 48 hrs and the results recorded.
Evaluation of the Effectiveness of Specimen Isolation
Examination of plates processed by the manual method and automated method was done independently. The number of potential pathogens isolated, the number of isolated single colonies per plate, and the quantity of bacterial growth were recorded and compared between the two methods for each sample. The number of potential pathogens isolated was defined by the number of unique colonies that were selected for further work up (ie, identification, antibiotic susceptibility tests). Semi-quantification of growth was estimated by the following criteria: growth only in one quadrant, 1+; growth in two quadrants, 2+; growth in three quadrants, 3+; growth in all of four quadrants, 4+. The semi-quantitative results were compared for sputum, urine (CB agar only), normally sterile body fluids, and feces specimens. Quantitative growth of urine specimens on blood agar was determined by counting colonies.
Statistical Analysis
Statistical analyses were performed with SPSS22.0 paired t test (normal distribution data) or Mann–Whitney U-test (non-normal distribution data); P value <0.05 was regarded as statistically significant.
Results
Comparison of Isolated Species
The recovery of suspected pathogens with the automated method and manual method is summarized in Table 1. The number of pathogen species worked up with the automated and manual methods is not statistically different for all specimens except sputum inoculated onto blood agar where significantly more pathogen species were isolated with the automated method (113 vs 104; P =0.019).
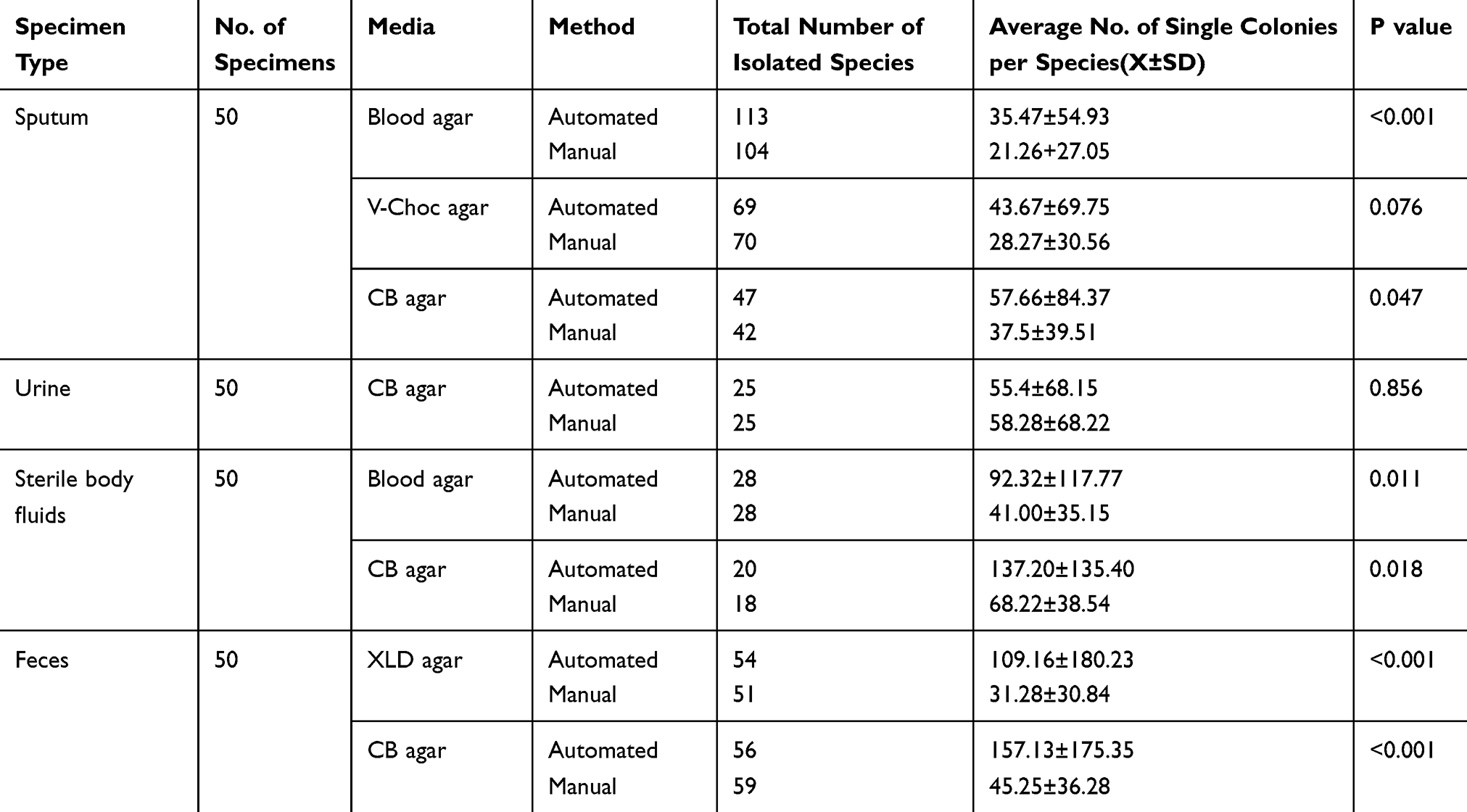 |
Table 1 Comparison of BD Kiestra InoqulA Automated Method and Manual Method for the Recovery of Pathogens and Isolated Colonies |
Comparison of Isolated Single Colonies
The recovery of isolated single colonies on plates inoculated with the automated and manual methods is summarized in Table 1 and a representative culture is depicted in Figure 1. Significantly more isolated colonies were observed on the plates processed in the automated method for all specimens and agar plates except for sputum inoculated onto vancomycin-containing chocolate agar (P =0.076) and urine inoculated onto China blue agar (P =0.856).
 |
Figure 1 The isolated single colonies on plates inoculated with the automated and manual methods. Feces specimen inoculated onto xylose-lactose-desoxycholate agar with BD Kiestra lnoqulA automated method (a1) and manual method (a2);urine specimen inoculated onto Columbia blood agar with BD Kiestra lnoqulA automated method (b1) and manual method (b2); sputum specimen inoculated onto vancomycin-containing chocolate agar with BD Kiestra lnoqulA automated method (c1) and manual method (c2); sputum specimen inoculated onto Columbia blood agar with BD Kiestra lnoqulA automated method (d1) and manual method (d2); sterile body fluids specimen inoculated onto Columbia blood agar with BD Kiestra lnoqulA automated method (e1) and manual method (e2). |
We furtherly analyzed the distribution of number of species with more single isolated colonies in different specimen types (Table 2). Significantly more species with more single colonies were found in the automatic processed specimens for sputum, sterile body fluids, and feces. For urine, 9 species showed more single colonies with the automatic method and 13 species exhibited more single colonies with the manual method.
 |
Table 2 Analysis of Specimen Processing Method Resulting in Most Isolated Colonies |
Comparison of Bacterial Growth Quantity
Another method for evaluating the quality of streaking culture plates is to determine the number of colonies observed in each quadrant of the plate. Cultures with light growth (ie, few colonies) would be expected to be restricted to the first quadrant (1+) while cultures with heavy growth would have colonies observed in the third (3+) and fourth (4+) quadrants. Because the same volume of specimen was processed for each specimen by the manual and automated methods, higher semi-quantitative values would reflect better streaking effects. The results of this experiment are summarized in Table 3. All plates streaked with the automated method had significantly higher semi-quantitative values compared to the manual method except for sterile body fluids streaked onto China blue agar (P =0.56). The urine specimens inoculated onto Columbia blood agar were streaked in a manner to provide quantification of growth. The values for urine streaked with the manual method and automated method were not significantly different as would be expected since all plates were inoculated with the same volume delivered with a calibrated pipette (P =1.000).
 |
Table 3 The Comparative Results Between BD Kiestra InoqulA Automated Method and Manual Method on Semi-Quantitative Bacterial Growth |
Discussion
Recent studies suggest fully automated microbiology specimen inoculation systems have many advantages, such as improved workflow efficiency and reduced labor costs, operational errors and environmental contamination.5–9 Previously, Croxatto et al5 demonstrated that urine specimens processed with the benchtop InoqulA model resulted in better isolated colonies and fewer subcultures. This confirmed the observations made previously by Froment et al6 with the Kiestra InoqulA and Quiblier et al10 with urine specimens processed with the Copan WASP system. Croxatto et al5 and Iversen et al8 compared the performance of BD Kiestra InoqulA and Copan WASP with urine specimens and reported more isolated colonies from the InoqulA system. This is the first study that has systematically examined the performance of BD Kiestra InoqulA with multiple specimen types and has demonstrated that improved isolated colonies and more uniform plate streaking were observed compared to manual streaking.
Because both manual and automated processed specimens were inoculated with a calibrated pipette, the complication of variations in specimen volume between a manual loop and automated pipette in the InoqulA system has been eliminated. Thus, we have focused on the efficiency of streaking different specimens’ types with an automated magnetic bead compared with manual loop. Earlier studies have demonstrated the inaccuracy of specimen inoculation with bacteriologic loops;11 thus, it would be anticipated that greater variation in recovery of isolated colonies and reproducible plate streaking would be observed in traditional manual microbiology laboratories than in this study.
In our study, we observed that more isolated colonies were incubated on the plates processed in the automated system, which is consistent with the results of Croxatto et al.5 With more isolated colonies, the steps following incubation, such as plate sorting according to positivity, colony picking for MALDI-TOF MS identification, and antimicrobial susceptibility testing can be conducted without subcultures, which contributed to reduced time to results. When clinicians get results earlier, patients can get better treatment and decrease time and cost of hospitalization.3,12 In our experience 200–300 plates can be processed per hour by InoqulA system, which can meet the demand in our laboratory and is faster than manual streaking. In this study, all the samples inoculated by a skilled laboratory technician took a total of 3.97 hrs (sputum, 1.2 hrs; urine, 0.95 hr; sterile body fluids, 0.9 hr; and feces, 0.92 hr). It took 2.2 hrs to complete the inoculation of all the samples (sputum, 0.7 hr; urine, 0.5 hr; sterile body fluids, 0.5 hr; and feces, 0.5 hr) by automated system. A reduction of 45% working hours in inoculation was observed by automated system in this study, which means a shorter time to result. But the data shown here may be different for laboratories with different equipment.
In the last decades, some instrumentation and services for total laboratory automation (TLA) have been introduced. The advantages of TLA include improvement of laboratory workflow and efficiency, labor, and cost saving, increased yield of isolated colonies and bacterial growth, reduced time to results and so on. Moreover, TLA system can decrease errors like sample and media plates by providing a traceable barcode. Croxatto showed that staff activities can be reduced 100% for plate sorting, labelling, and incubation; 30–60% for inoculation, plate reading, identification, and antibiotic susceptibility testing by laboratory automated systems.3 However, TLA also has some limitations. On the one hand, only using eyes we may miss the characteristic bacteria with odor like anaerobic pathogens. On the other hand, incubators cannot provide an anaerobic atmosphere which is the main problem of anaerobes cultivation. Compared to the automated inoculation systems, anaerobes, unusual or new species can be found more easily by manual inoculation.13 TLA cannot replace the current manual labor completely in a short time.
In summary, the BD Kiestra InoqulA system is superior to the manual method for processing common clinical specimens. More uniform plate streaking and colony isolation was achieved, which reduce the need for subcultures before further processing of cultures can be performed.
Ethics and Consent Statement
This study was carried out in accordance with the recommendations of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Medical College Hospital ethics committee with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Medical College Hospital ethics committee (Approval no. S-K588).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by The National Key Research and Development Program of China (2018YFE0101800, 2018YFC1200100 and 2018YFC1200105), CAMS Initiative for Innovative Medicine (grant no. 2016-I2M-3-014). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Greub G, Prod’hom G. Automation in clinical bacteriology: what system to choose? Clin Microbiol Infect. 2011;17:655–660. doi:10.1111/j.1469-0691.2011.03513.x
2. Bourbeau P, Ledeboer N. Automation in clinical microbiology. J Clin Microbiol. 2013;51:1658–1665. doi:10.1128/JCM.00301-13
3. Croxatto A, Prod’Hom G, Faverjon F, Rochais Y, Greub G. Laboratory automation in clinical bacteriology: which system to choose? Clin Microbiol Infect. 2016;22:217–235. doi:10.1016/j.cmi.2015.09.030
4. Burckhardt I. Laboratory automation in clinical microbiology. Bioengineering (Basel). 2018;5:e102. doi:10.3390/bioengineering5040102
5. Croxatto A, Dijkstra K, Prod’Hom G, Greub G. Comparison of inoculation with the InoqulA and WASP automated systems with manual inoculation. J Clin Microbiol. 2015;53:2298–2307. doi:10.1128/JCM.03076-14
6. Froment P, Marchandin H, Vande P, Lamy B. Automated versus manual sample inoculations in routine clinical microbiology: a performance evaluation of the fully automated InoqulA instrument. J Clin Microbiol. 2014;52:796–802. doi:10.1128/JCM.02341-13
7. Graham M, Tilson L, Streitberg R, Hamblin J, Korman T. Improved standardization and potential for shortened time to results with BD Kiestra total laboratory automation of early urine cultures: a prospective comparison with manual processing. Diag Microbiol Infect Dis. 2016;86:1–4. doi:10.1016/j.diagmicrobio.2016.06.020
8. Iversen J, Stendal G, Gerdes C, Meyer C, Andersen C, Frimodt-Møller N. Comparative evaluation of inoculation of urine samples with the Copan WASP and BD Kiestra InoqulA instruments. J Clin Microbiol. 2016;54:328–332. doi:10.1128/JCM.01718-15
9. Thesparee T, Das S, Thomson RB. Total Laboratory automation and MALDI-TOF improve turnaround times in the clinical microbiology laboratory: a retrospective analysis. J Clin Microbiol. 2018;56:e01242–17. doi:10.1128/JCM.01242-17
10. Quiblier C, Jetter M, Rominski M, Mouttet F, Bottger E, Keller P. Performance of Copan WASP for routine urine microbiology. J Clin Microbiol. 2016;54:585–592. doi:10.1128/JCM.02577-15
11. Frimodt-Møller N, Espersen F. Evaluation of calibrated 1 and 10 µL loops and dipslide as compared to pipettes for detection of low count bacteriuria in vitro. APMIS. 2000;108:525–530. doi:10.1034/j.1600-0463.2000.d01-92.x
12. Fournier PE, Drancourt M, Colson P, Rolain JM, La Scola B, Raoult D. Modern clinical microbiology: new challenges and solutions. Nat Rev Microbiol. 2013;11:574–585. doi:10.1038/nrmicro3068
13. Gajdács M. Anaerobes and laboratory automation: like oil and water? Anaerobe. 2019;59:112–114. doi:10.1016/j.anaerobe.2019.06.009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.