Back to Journals » Clinical Ophthalmology » Volume 15
Clinical Outcomes of Micropulse Laser Trabeculoplasty Compared to Selective Laser Trabeculoplasty at One Year in Open-Angle Glaucoma
Authors Sun CQ ![]() , Chen TA, Deiner MS, Ou Y
, Chen TA, Deiner MS, Ou Y
Received 3 October 2020
Accepted for publication 12 November 2020
Published 22 January 2021 Volume 2021:15 Pages 243—251
DOI https://doi.org/10.2147/OPTH.S285136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Catherine Q Sun, Tiffany A Chen, Michael S Deiner, Yvonne Ou
Department of Ophthalmology, University of California San Francisco, San Francisco, CA, USA
Correspondence: Catherine Q Sun
UCSF F.I. Proctor Foundation, 490 Illinois Street, Floor 2, San Francisco, CA 94143, USA
Email [email protected]
Background: There is limited long-term data comparing selective laser trabeculoplasty (SLT) to the newer micropulse laser trabeculoplasty (MLT) using a laser emitting at 532 nm. In this study, we determine the effectiveness and safety of MLT compared to SLT.
Design: Retrospective comparative cohort study.
Participants: A total of 85 consecutive eyes received SLT and 43 consecutive eyes received MLT.
Methods: Patients with open-angle glaucoma receiving their first treatment of laser trabeculoplasty were included. Exclusion criteria are prior laser trabeculoplasty, laser cyclophotocoagulation or glaucoma surgery, and follow-up of less than 1 year.
Main Outcome Measures: The primary outcome was success at 1 year, defined as a reduction in intraocular eye pressure (IOP) by ≥ 20% from baseline or met prespecified target IOP with no additional glaucoma medication or subsequent glaucoma intervention.
Results: Baseline IOP was 18.0 mmHg (95% CI=16.4– 19.5) in the MLT group on an average of 1.8 (95% CI=1.4– 2.2) glaucoma medications compared to 18.2 mmHg (95% CI=17.2– 19.3) for the SLT group on an average of 2.0 (95% CI=1.6– 2.3) medications. At 1-hour post-laser, the SLT group had more transient IOP spikes (MLT 5% vs SLT 16%, P=0.10). There was a trend toward increased success in the SLT group compared to MLT at 1 year (relative risk=1.4, 95% CI=0.8– 2.5, P=0.30).
Conclusion and Relevance: Eyes had similar success after MLT compared to SLT at 1 year. Laser trabeculoplasty with either method could be offered as treatment with consideration of MLT in those eyes where IOP spikes should be avoided.
Keywords: micropulse laser trabeculoplasty, selective laser trabeculoplasty, open-angle glaucoma
Introduction
Laser trabeculoplasty has been available since the 1970s, and remains an important treatment option for open-angle glaucoma (OAG).1–3 Selective laser trabeculoplasty (SLT) has superseded argon laser trabeculoplasty (ALT) given similar efficacy, improved safety profile, and repeatability.2 SLT selectively applies energy to pigmented cells of the trabecular meshwork (TM) using a 532 nm Q-switched, frequency-doubled Nd:YAG laser. Electron microscopy following SLT showed disruption of the pigmented TM endothelial cells.4 This cellular damage, in addition to biological changes, is thought to cause an increased inflammatory response which increases aqueous outflow through the TM.2,5 The inflammatory response and early pigment dispersion can also cause transient intraocular pressure (IOP) spikes and ocular discomfort.2,5
Micropulse laser trabeculoplasty (MLT) is a form of subthreshold laser that breaks a continuous laser into short pulses to allow for cooling in-between applications. The interpulse period of cooling prevents cellular or morphologic changes to the TM.5 In a study on human corneoscleral rim tissue from cadaver eyes treated with laser trabeculoplasty, SLT and MLT did not leave any morphologic changes to the TM compared to ALT.6 During SLT, the pulse energy can be titrated until occasional bubble formation is visualized. With MLT, there is no visible sign of treatment during the procedure, which makes it difficult to titrate but also reduces post-operative inflammation, discomfort, and IOP spikes compared to SLT.7,8
To our knowledge, there have only been two studies that have compared outcomes of MLT to SLT.7,8 MLT can be performed using a 532 nm, 577 nm, or 810 nm laser. Abramowitz et al8 prospectively compared patients treated with the yellow (577 nm) MLT laser to SLT, including patients with prior laser trabeculoplasty and/or glaucoma filtering surgery, and found similar efficacy between MLT and SLT. We believe comparison studies should be performed using a green MLT laser emitting at 532 nm, equivalent to the wavelength used in SLT and the wavelength that selectively targets melanin in pigmented TM cells.9 The only comparison study using a green (532 nm) MLT laser was a retrospective study with only 6 months of follow-up that demonstrated similar success between MLT and SLT.7
In this retrospective comparative cohort study, we evaluated the 1-year outcomes of MLT using a 532 nm laser compared to SLT in patients with OAG who had not received prior glaucoma laser trabeculoplasty or surgeries. Results of this study will provide insight into the effectiveness and safety of performing primary (first treatment of) MLT compared to SLT with longer follow-up.
Patients and Methods
Inclusion and Exclusion Criteria
Patients with OAG who underwent primary laser trabeculoplasty under the supervisory care of a single provider at the University of California San Francisco (UCSF) between June 1, 2012 and October 1, 2017 were included, though trainees also performed the laser trabeculoplasty. Patients were identified using CPT code 65855 for laser trabeculoplasty. Patients were consecutively assigned to SLT from June 2012 to June 2015 and MLT from June 2015 to October 2017 by the provider to try to decrease selection bias. Several patients received SLT after 2015 when the MLT laser was undergoing repair. Exclusion criteria included prior laser trabeculoplasty, laser cyclophotocoagulation, or glaucoma surgery; patients with mixed-mechanism glaucoma, uveitic glaucoma, neovascular glaucoma, juvenile open-angle glaucoma, congenital glaucoma, or angle-closure glaucoma; and no follow-up at the 1-year window (6–18 months). UCSF Institutional Review Board approval and waiver of informed consent were obtained because the research does not adversely affect the rights and welfare of the individuals, and involves no more than minimal risk to their privacy based on an adequate plan to maintain confidentiality. The research adhered to the tenants of the Declaration of Helsinki.
Procedure and Follow-Up
Patients received topical proparacaine, apraclonidine 0.5%, and pilocarpine 1 or 2% before laser treatment. A Latina SLT lens or MLT lens (Iridex Corporation, Mountain View, CA, USA) was placed on the operative eye with goniosol and laser treatment was applied. All patients received 360 degrees of confluent laser treatment to the pigmented TM. An IQ 532™ laser (Iridex Corporation, Mountain View, CA, USA) was used for MLT with settings of 1,000 mW, 15% duty cycle, 300 millisecond duration, 300 µm spot size for all patients, which is the standard setting that has previously been reported.10 A 532 nm Q-switched, frequency-doubled Nd:YAG Selecta II™ (Lumenis Inc, San Jose, CA, USA) laser was used for SLT with a standard 400 µm spot size and 3 nanosecond duration. The SLT laser energy was titrated between 0.5 to 1.6 mJ per pulse based on the TM pigmentation to see occasional bubble formation. Patients received one drop of apraclonidine 0.5% and one drop of prednisolone acetate 1% immediately post-procedure and had their IOP checked approximately 1 hour post-laser. Patients were not prescribed any anti-inflammatory drops post-laser and were continued on their IOP medications at the discretion of the treating physician. Follow-up was scheduled approximately 4–6 weeks post-procedure and at regular intervals thereafter at the discretion of the physician.
Baseline Variables
Baseline characteristics and exam findings were collected from the medical record. Baseline IOP was the average of the two visits prior to the laser procedure. To determine how to define baseline IOP, a sensitivity analysis was performed to determine differences in baseline IOP when using two prior visits, one prior visit, or the laser day visit, and no significant differences were found. IOP was measured by Goldmann applanation in the majority of patients. Sensitivity analysis was performed to determine if type of IOP measurement affected the primary outcome, and no difference was found when the six eyes without Goldmann applanation tonometry at all visits were excluded. Combination eye drops were counted as two separate medications. Patients were followed in the study until repeat laser trabeculoplasty, cyclophotocoagulation, or glaucoma surgery, then they were considered failures, and the last observation carried forward was performed for any subsequent follow-up visit.
Outcomes
The primary outcome was success at 1 year, defined as 1) reduction in IOP by ≥20% from baseline or met target IOP (pre-specified in the medical record by the treating provider), 2) no additional glaucoma medications compared to baseline, and 3) no subsequent glaucoma interventions, including repeat laser trabeculoplasty, laser cyclophotocoagulation, or glaucoma surgery. Standalone cataract surgery was allowed. Secondary outcomes included mean IOP at 1, 6, 12, and 24-month windows; IOP spike 1 hour post-laser; and number of and time to repeat laser trabeculoplasty or glaucoma surgery.
Statistical Analysis
For the primary outcome, a modified Poisson regression was used to estimate the relative risk of treatment success at 1 year, controlling for baseline IOP, number of glaucoma medications at baseline, and central corneal thickness as covariates. Robust standard errors were clustered on patient to allow for correlation between eyes if both eyes underwent laser trabeculoplasty.11 Secondary outcomes were analyzed using two-tailed unpaired t-test for continuous variables, and chi-square test or Fisher’s exact for dichotomous variables. Based on our sample size, we had 80% power to detect a 1.057 mmHg difference in mean IOP between the MLT and SLT groups assuming a standard deviation (SD) of 2.0 for a 2-sided test with a level of significance of 0.05.
Results
We identified 156 patients who received laser trabeculoplasty at UCSF under the care of a single surgeon from June 1, 2012 to October 1, 2017. Forty-three eyes of 32 patients received MLT treatment and 85 eyes of 59 patients received SLT treatment after inclusion and exclusion criteria were applied. Five patients (10%) were lost to follow-up in the MLT group and four patients (5%) in the SLT group. There was no significant difference in baseline patient characteristics in the patients who were lost to follow-up.
Table 1 shows the baseline characteristics between the MLT and SLT cohorts. The only significant difference between the groups was younger age in the MLT group (68 years old, 95% CI=63–72) compared to the SLT group (74 years old, 95% CI=71–77; P=0.02), and slightly thinner mean central corneal thickness in the SLT group (545 μm, 95% CI=536–554) compared to the MLT group (562 μm, 95% CI=546–578; P=0.046). The majority of eyes had primary open-angle glaucoma (POAG), followed by normal tension glaucoma (NTG) in both groups. Baseline IOP was similar at 18.0 mmHg (95% CI=16.4–19.5) in the MLT group compared to 18.2 mmHg (95% CI=17.2–19.3) in the SLT group (P=0.76). Seven eyes (16%) were on no drops at presentation in the MLT group compared to 20 (24%) in the SLT group (P=0.34).
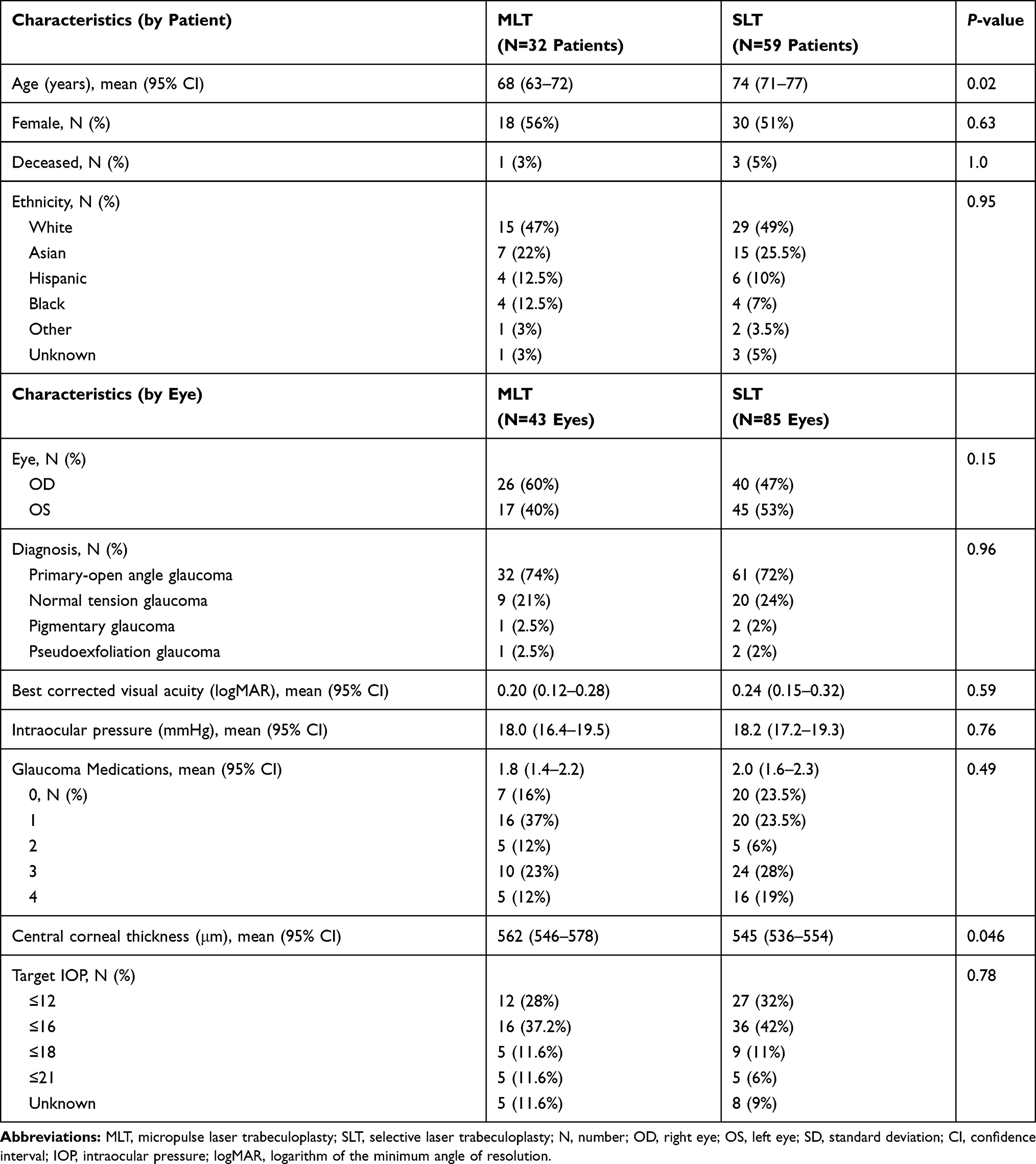 |
Table 1 Baseline Patient and Ocular Characteristics |
The same laser settings were used in all patients undergoing MLT with a mean of 138 laser spots (SD=30). For SLT, the mean laser energy used was 99 mJ (SD=33) with an average of 125 spots (SD=26). The number of laser spots and the mean laser energy did not significantly affect treatment success due to minimal variability between eyes. At 1 hour post-laser, two eyes (5%) treated with MLT had a transient increase in IOP of ≥5 mmHg from pre-laser, compared to 14 eyes (16%) in the SLT group (P=0.10). There were no other post-laser complications.
Figure 1 shows the change in IOP and medication number over 2 years of follow-up. At the 1-month visit, there was a significant improvement in mean IOP after SLT (15.6 mmHg, 95% CI=14.5–16.6) on an average of 1.6 glaucoma drops (95% CI=1.3–2.0) compared to MLT (17.9 mmHg, 95% CI=16.5–19.3) on 1.4 glaucoma drops (95% CI=0.9–1.9) (P=0.008). For the SLT group, this reduction in IOP was maintained until 1 year on a similar number of drops compared to the 1-month visit (Table 2). There was a trend toward greater reduction in IOP at 1 year from baseline with SLT (−11%, 95% CI=−16% to −6%) compared to MLT (−3%, 95% CI=−10% to +4%; P=0.06). There was also a trend toward reduction in number of glaucoma medications from baseline to 1 year for the SLT group (−0.2, 95% CI=−0.5 to −0.1) compared to MLT (+0.1, 95% CI=−0.2 to +0.5; P=0.06). By 2-year follow-up, the mean IOPs were similar in both groups, but there were also fewer eyes in each cohort (P=0.93).
 |
Table 2 Clinical Outcomes at One Year |
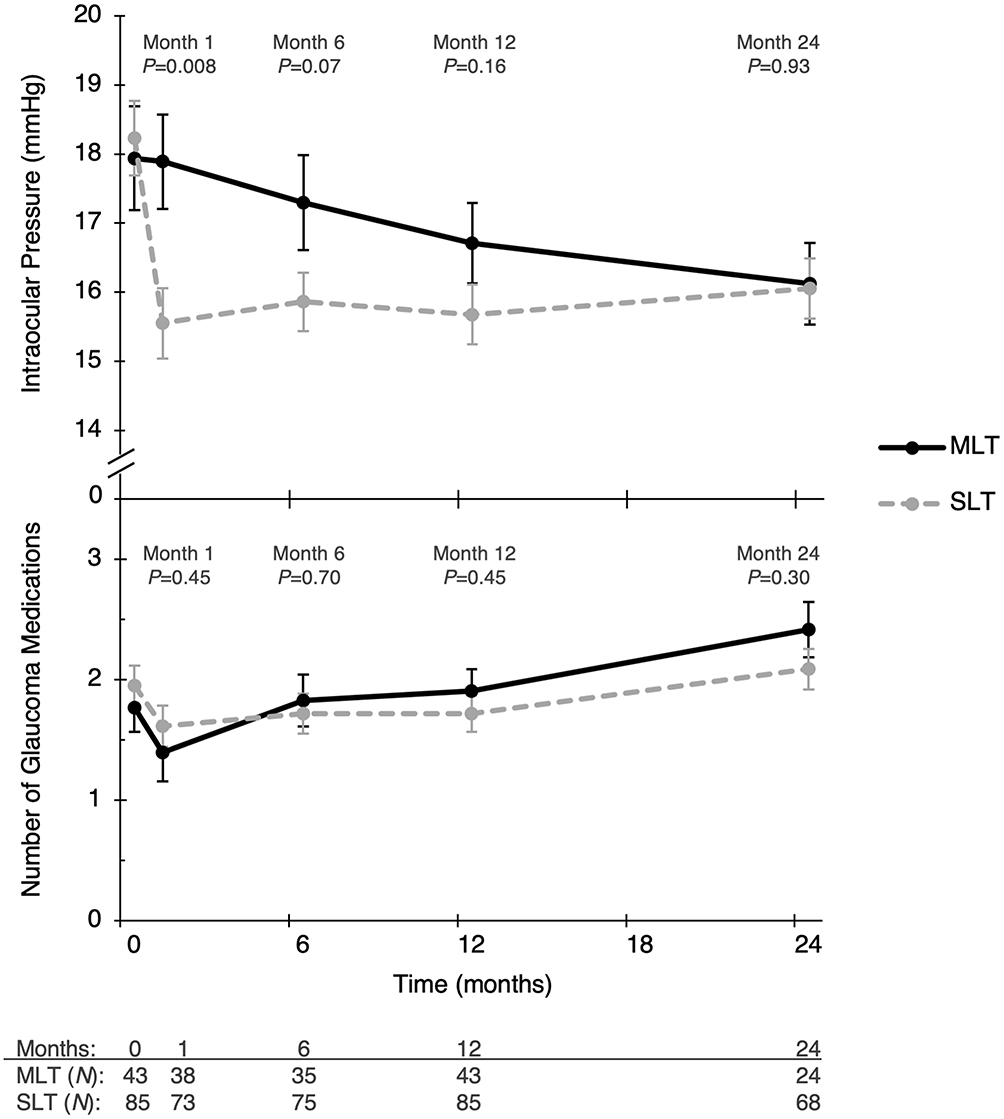 |
Figure 1 Mean intraocular pressure (top graph) and number of glaucoma medications (bottom graph) between the micropulse laser trabeculoplasty (MLT) and selective laser trabeculoplasty (SLT) groups at follow-up intervals up to 2 years. No statistically significant difference was noted between MLT and SLT-treated eyes except for intraocular pressure at 1 month follow-up. Error bars represent standard error of the mean. Abbreviation: N, number of eyes. |
For our primary outcome, the SLT group had a 1.4-times higher probability of treatment success compared to the MLT group at 1 year, though this was not statistically significant (relative risk=1.4, 95% CI=0.8–2.5, P=0.30) (Table 3). Most patients failed due to inadequate IOP reduction and/or need for additional glaucoma medications (Table 2). In our model, there was no association between success and baseline IOP or number of baseline IOP medications. However, when we performed a sensitivity analysis and predicted treatment success using the definition for success from the initial SLT pilot study by Latina et al (reduction in IOP by ≥3 mmHg from baseline without change in medication number), we found higher baseline IOP was significantly associated with treatment success (relative risk=1.07 per mmHg, 95% CI=1.03–1.11, P<0.001).12
 |
Table 3 Multivariable Regression Model Predicting Success at 1 Year |
Discussion
Our retrospective, comparative cohort study demonstrated that eyes treated with MLT and SLT had similar treatment success at 1 year, though there was a trend toward greater success with SLT. In our study, we elected to use a green laser emitting at 532 nm to perform MLT since it is equivalent to the wavelength used in SLT, and selectively targets melanin in pigmented TM cells.9 Our study is unique in that we evaluated primary laser trabeculoplasty, consecutively assigned patients to SLT or MLT in 2 year windows to reduce selection bias, and assessed primary outcome at 1 year. Furthermore, our study provides additional data out to 2 years of follow-up for a subset of the eyes receiving MLT (N=24) or SLT (N=68) treatment.
In their prospective study comparing MLT using a 577 nm yellow laser to SLT, Abramowitz et al8 reported that 30% of MLT patients (N=38) and 36% of SLT patients (N=31) experienced ≥20% IOP reduction from baseline to the 6–13-month follow-up window. However, they included patients with prior laser trabeculoplasty and glaucoma surgery,8 whereas we excluded these patients to determine the effect of primary laser trabeculoplasty. Using their outcome of ≥20% IOP reduction from baseline, we found that in our study fewer MLT eyes (12%) and a similar number of SLT eyes (29%) met criteria at the 1-year window. In our study, the number of eyes with ≥20% IOP reduction at 1 year was likely lower, despite excluding eyes with prior glaucoma laser and surgery, because many of them had severe glaucoma with a target IOP in the low teens (MLT 28% vs SLT 32%).
The only other study comparing MLT to SLT using a 532 nm green laser was also retrospective and evaluated primary laser trabeculoplasty, but provided shorter follow-up at 6 months.7 Their primary outcome was success, defined as a reduction of ≥20% IOP or ≥1 glaucoma medication without requiring additional IOP lowering procedures at 6 months. They similarly did not demonstrate a statistically significant difference in success between MLT and SLT (P=0.98).7 At 6 months, they found a mean IOP reduction of 2.1 mmHg (SD=4.1) or 11.5% with MLT compared to 1.8 mmHg (SD=6.6) or 10.4% with SLT.7 Since our definitions of success were different, we looked at our 6-month percent change in IOP from baseline for comparison. At 6 months, we demonstrated a similar percent reduction in IOP from baseline with SLT (12.5%) but no change with MLT (0.1%) in our study.
In a prospective study of 48 Chinese patients with POAG or NTG who underwent MLT using the 577 nm laser, Lee et al13 reported higher success rates at 1 month after MLT. They reported 73% success, defined as an IOP reduction of ≥20% on the same number of antiglaucoma medications prior to medication titration at 1 month post-MLT.13 They found a 20% mean reduction in IOP from baseline to 6 months with the addition of medications. Their baseline IOP was similar to our study at 18.5 mmHg (SD=3.0), but they had greater reduction in IOP at 1 month. This difference could be due to patient characteristics such as TM pigmentation. All patients in their study had TM pigmentation Spaeth grade 3 or higher. We had gonioscopy data available for approximately 50% of our patients and only 30% who received MLT had TM pigmentation grade 3 or higher, compared to 50% in the SLT group. For MLT, there is limited evidence on the optimal amount of laser energy to use and if it should be titrated during treatment as in SLT.10 Additional investigation is needed to determine the optimal laser parameters, including number of shots and energy per shot.
Our SLT treatment success and percentage of responders were also lower than in prior studies, likely due to the inclusion of patients with lower baseline IOP and more advanced glaucoma. In the original pilot study by Latina et al12 that studied 180 degrees of SLT in laser-naïve patients and those with prior ALT, eyes included had uncontrolled OAG with IOP ≥22 mmHg. Their baseline IOP mean was 24.6 mmHg and improved by a mean of 4.6 mmHg (18.7%) at 6 months.12 They found that 70% of patients were responders (defined as ≥3 mmHg reduction in IOP from baseline to 6 months) in the laser-naïve group and those with prior ALT.12 When we analyzed our primary outcome using their definition of success, we found that baseline IOP was significantly associated with success. In the literature, there is also evidence of a correlation between higher baseline IOP and SLT treatment success.2,–14–16
In a real-world setting, success after SLT may be lower than reported in randomized controlled trials. In a meta-analysis on SLT, the percent reduction in IOP ranged from 6.9–35.9% at ≥1 year.15 In a retrospective observational study of SLT effectiveness from de-identified electronic medical records in the UK, they found that SLT treatment success was 45% at 1 year.14 In our study, we had a similar treatment success of 46% after SLT at 1 year.
We believe the benefits of MLT over SLT are fewer post-laser IOP spikes (≥5 mmHg) and less post-operative inflammation.7,8 Two eyes in the MLT group (5%) and 14 in the SLT group (16%) experienced IOP spikes at 1 hour, though these were all transient. Fifteen of these eyes had POAG and one had pigmentary glaucoma. Higher IOP spikes have been previously reported for SLT compared to MLT.7 In a meta-analysis of SLT studies, the range of transient IOP spikes was 0–62% in 34 studies.15 Abramowitz et al8 also reported that MLT patients experienced significantly less pain than SLT patients in a post-laser survey suggesting less post-laser inflammation with MLT.
The main limitation of this study is its retrospective design, which can increase selection bias. To help reduce selection bias, our patients were consecutively assigned to SLT or MLT by time period (SLT from June 2012 to June 2015 and MLT from June 2015 to October 2017). While there were more patients in the SLT group compared to MLT group, key baseline characteristics such as glaucoma diagnosis, IOP, number of glaucoma medications, and target IOP were not statistically different between the two groups. The only differences were age and central corneal thickness. We controlled for central corneal thickness in our primary outcome analysis. A sensitivity analysis that included age as a covariate did not change the primary outcome. Despite the difference in SLT and MLT group size, we still had 80% power to detect a 1.057 mmHg difference in mean IOP. In this study, we also included patients who had bilateral laser trabeculoplasty, but accounted for this correlation by using robust standard errors clustered on patient.
Generalizability may be reduced since our cohort consisted of more moderate to advanced glaucoma patients with lower baseline IOP. However, our cohort likely better represents how laser trabeculoplasty is currently utilized in real-world practice since medical therapy was noted to be the most common initial intervention based on the American Academy of Ophthalmology Preferred Practice Pattern guidelines in 2016.17 Recent findings from a study looking at real-world SLT outcomes in the UK demonstrated similar success rates at 1 year.14 The results of the Laser in Glaucoma and Ocular Hypertension (LiGHT) trial may also change treatment paradigm in the future.3 The study randomized treatment-naïve patients with OAG and ocular hypertension to SLT versus medications.3 They demonstrated that there was no difference in health-related quality-of-life or clinical outcomes at 3 years, and that SLT as first-line treatment was safe and more cost-effective than medications.3
In conclusion, MLT and SLT had similar efficacy at 1 year, though there was a trend toward increased success with SLT. A sensitivity analysis suggested that higher baseline IOP predicts success. MLT treatment resulted in fewer post-laser IOP spikes than SLT but all were transient. MLT could be considered in patients who are predisposed to IOP spikes, or in advanced glaucoma patients in whom an IOP spike could be detrimental. Our 1-year primary laser trabeculoplasty results provide real-world outcomes of treatment success between MLT and SLT.
Acknowledgments
We thank Benjamin Arnold, PhD (UCSF) for guidance on statistical analysis.
Funding
This research was supported by the following grants: National Eye Institute K12EY031372, University of California San Francisco Vision Core shared resource of the NIH/NEI P30 EY002162, and an unrestricted grant from the Research to Prevent Blindness, New York, NY.
Disclosure
The authors report no potential conflicts of interest for this work.
References
1. Wise JB, Witter SL. Argon laser therapy for open-angle glaucoma. A pilot study. Arch Ophthalmol. 1979;97(2):319–322. doi:10.1001/archopht.1979.01020010165017
2. Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, and future. Eye. 2018;32(5):863–876. doi:10.1038/eye.2017.273
3. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet. 2019;393(10180):1505–1516. doi:10.1016/S0140-6736(18)32213-X
4. Kramer TR, Noecker RJ. Comparison of the morphologic changes after selective laser trabeculoplasty and argon laser trabeculoplasty in human eye bank eyes. Ophthalmology. 2001;108(4):773–779. doi:10.1016/S0161-6420(00)00660-6
5. Ma A, Yu SWY, Wong JKW. Micropulse laser for the treatment of glaucoma: a literature review. Surv Ophthalmol. 2019;64(4):486–497. doi:10.1016/j.survophthal.2019.01.001
6. Fudemberg SJ, Myers JS, Katz LJ. Trabecular meshwork tissue examination with scanning electron microscopy: a comparison of Micropulse Diode Laser (MLT), Selective Laser (SLT), and Argon Laser (ALT) trabeculoplasty in human cadaver tissue. Invest Ophthalmol Vis Sci. 2008;49(13):1236.
7. Hirabayashi MT, Rosenlof TL, An JA. Comparison of successful outcome predictors for MicroPulse((R)) laser trabeculoplasty and selective laser trabeculoplasty at 6 months. Clin Ophthalmol (Auckland, NZ). 2019;13:1001–1009. doi:10.2147/OPTH.S205977
8. Abramowitz B, Chadha N, Kouchouk A, Alhabshan R, Belyea DA, Lamba T. Selective laser trabeculoplasty vs micropulse laser trabeculoplasty in open-angle glaucoma. Clin Ophthalmol (Auckland, NZ). 2018;12:1599–1604. doi:10.2147/OPTH.S167102
9. Latina MA, Park C. Selective targeting of trabecular meshwork cells: in vitro studies of pulsed and CW laser interactions. Exp Eye Res. 1995;60(4):359–371. doi:10.1016/S0014-4835(05)80093-4
10. Ahmed I, Gossage D, Vold S. With years of SLT data, why consider MLT? Glaucoma Today. 2013.
11. Yelland LN, Salter AB, Ryan P. Performance of the modified Poisson regression approach for estimating relative risks from clustered prospective data. Am J Epidemiol. 2011;174(8):984–992. doi:10.1093/aje/kwr183
12. Latina MA, Sibayan SA, Shin DH, Noecker RJ, Marcellino G. Q-switched 532-nm Nd: yAGlaser trabeculoplasty (selective laser trabeculoplasty): a multicenter, pilot, clinical study. Ophthalmology. 1998;105(11):2082–2090. doi:10.1016/S0161-6420(98)91129-0
13. Lee JW, Yau GS, Yick DW, Yuen CY. MicroPulse laser trabeculoplasty for the treatment of open-angle glaucoma. Medicine (Baltimore). 2015;94(49):e2075. doi:10.1097/MD.0000000000002075
14. Khawaja AP, Campbell JH, Kirby N, et al. Real-world outcomes of selective laser trabeculoplasty in the United Kingdom. Ophthalmology. 2019.
15. Wong MO, Lee JW, Choy BN, Chan JC, Lai JS. Systematic review and meta-analysis on the efficacy of selective laser trabeculoplasty in open-angle glaucoma. Surv Ophthalmol. 2015;60(1):36–50. doi:10.1016/j.survophthal.2014.06.006
16. Pillunat KR, Spoerl E, Elfes G, Pillunat LE. Preoperative intraocular pressure as a predictor of selective laser trabeculoplasty efficacy. Acta Ophthalmol. 2016;94(7):692–696. doi:10.1111/aos.13094
17. Prum BE, Rosenberg LF, Gedde SJ, et al. Primary open-angle glaucoma preferred practice pattern((R)) guidelines. Ophthalmology. 2016;123(1):P41–p111. doi:10.1016/j.ophtha.2015.10.053
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.