Back to Journals » Medical Devices: Evidence and Research » Volume 18
Clinical Outcomes Among Patients Undergoing Open Abdominal or Orthopedic Surgery with Wound Closure Incorporating Triclosan-Coated Barbed Sutures: A Multi-Institutional, Retrospective Database Study
Authors Fortin SP, Spychaj K, Tomaszewski J ![]() , Grebeck H, Yalla R, Coplan PM
, Grebeck H, Yalla R, Coplan PM ![]() , Zhang S
, Zhang S ![]()
Received 23 November 2024
Accepted for publication 15 February 2025
Published 6 March 2025 Volume 2025:18 Pages 161—176
DOI https://doi.org/10.2147/MDER.S508169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Stephen P Fortin,1 Kerstin Spychaj,2 Jörg Tomaszewski,3 Holly Grebeck,3 Rithwik Yalla,4 Paul M Coplan,1,5 Shumin Zhang1
1MedTech Epidemiology and Real-World Data Science, Office of the Chief Medical Officer, Johnson & Johnson, New Brunswick, New Jersey, USA; 2Clinical Research, Johnson & Johnson MedTech, Raritan, New Jersey, USA; 3Medical Affairs, Johnson & Johnson MedTech, Raritan, New Jersey, USA; 4Mu Sigma, Bangalore, India; 5University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, USA
Correspondence: Stephen P Fortin, MedTech Epidemiology and Real-World Data Science, Office of the Chief Medical Officer, Johnson & Johnson, New Brunswick, NJ, USA, Tel +1 908 927 4844, Email [email protected]
Purpose: Determining the best suture for wound closure in high-tension areas by anatomical site and procedure type remains a challenge. This study assessed the cumulative incidence of clinical outcomes among patients undergoing procedures incorporating the STRATAFIX Symmetric PDS™ Plus Knotless Tissue Control Device (STRATAFIX Symmetric) for closure of high-tension areas, such as the abdominal fascia and hip and knee joint capsule, in the course of routine clinical practice.
Patients and Methods: Patients undergoing open abdominal or orthopedic surgery between October 1, 2016, and October 31, 2023, using size 0 or 1 STRATAFIX Symmetric were identified from the Premier Healthcare Database. The cumulative incidences of 30-day internal wound dehiscence and 30-day surgical site infection (SSI) were measured. To contextualize the results, a targeted literature search of articles published between October 2016 and April 2024 describing the use of STRATAFIX Symmetric for wound closure in the abdominal fascia or joint capsule was performed.
Results: A total of 8156 patients undergoing open abdominal surgery and 25,807 patients undergoing open orthopedic surgery met the study criteria. In the abdominal surgery cohort, the cumulative incidences of 30-day internal wound dehiscence and SSI were 0.65% (95% CI: 0.49%, 0.85%) and 3.54% (95% CI: 3.15%, 3.97%), respectively. The overall cumulative incidences of 30-day internal wound dehiscence and SSI in the orthopedic surgery cohort were 0.07% (95% CI: 0.04%, 0.11%) and 0.58% (95% CI: 0.49%, 0.68%), respectively. These findings were within the range of clinical outcomes reported in 12 articles identified during the targeted literature search.
Conclusion: The cumulative incidence of 30-day internal wound dehiscence and SSI among patients undergoing abdominal and orthopedic procedures incorporating STRATAFIX Symmetric for wound closure of high-tension areas was low and comparable to prior literature.
Keywords: barbed suture, STRATAFIX Symmetric, fascia, joint capsule, abdominal surgery, orthopedic surgery
Introduction
Wound closure technique in abdominal wall closure and orthopedic procedures is a key factor influencing wound complications.1–3 Barbed sutures, as compared to conventional sutures applied in an interrupted fashion, allow for a running closure of wounds and avoid the need to tie knots. These knotless sutures have been associated with reduced closure time and total hospital costs as well as higher cyclical tension thereby providing better waterproofing.3–6 This has led to increased adoption of barbed sutures in a variety of procedures, including arthroplasty,2,5 and spinal,7,8 general,3,9 gynecologic,10–12 urologic13,14 and cosmetic surgery.15,16
Other physical properties of sutures may also influence wound complications. For instance, meta-analyses have shown barbed sutures with polydioxanone as a material can sustain greater maximum load and larger gap-formation force as compared to conventional sutures, a finding that was not observed among barbed sutures composed of other materials.17 Indeed, polydioxanone has favorable tensile strength retention compared to other polymers, such as polyglycolic acid (PGA) and poly-glycolide-co-lactide (PGLA), exhibiting minimal absorption until 90 days and slowly absorbed through hydrolysis between 180 and 210 days.18–20 These characteristics have contributed to the widespread utilization of polydioxanone sutures in procedures with longer healing periods such as fascial closure and orthopedic surgery, with the recent guideline for closure of abdominal wall incisions from the European and American Hernia Societies recommending slowly absorbable sutures for the closure of midline incisions.20,21 Furthermore, sutures coated with the antimicrobial agent triclosan, widely used in suture coating due to its in vivo and in vitro antibacterial efficacy, have been associated with lower risk of postoperative infection in several surgical scenarios.22,23 This has led to the recommendation of utilizing antimicrobial/triclosan coated sutures in various guidelines, such as the World Health Organization, the American College of Surgeons or the National Institute for Health and Care Excellence in the United Kingdom.24–27
These physical properties are reflected in the design of the STRATAFIX™ Symmetric PDS™ Plus Knotless Tissue Control Device, henceforth referred to as STRATAFIX Symmetric, an absorbable polydioxanone, triclosan-coated barbed suture.28 In addition, the innovative barb design of STRATAFIX Symmetric facilitates high strength soft tissue approximation and has been demonstrated to provide appropriate strength for closing high-tension areas, such as fascia, in benchtop testing.29 The anchors are designed with optimized size and spacing to provide maximum holding in soft tissue and, furthermore, provide tactile feedback during passage through tissue, assisting surgeons to apply the desired tension. A fixation tab, at the distal end of the device, anchors the suture at the first pass into tissue, eliminating the need for tying a knot.29 Prior studies have demonstrated in vitro antibacterial efficacy of triclosan-coated polydioxanone sutures, formulated similar to STRATAFIX Symmetric, lasting 17 days against Escherichia coli and 23 days for Staphylococcus aureus.23
The choice of wound closure technique in high-tension areas remains a topic of debate. Selection of the best suture for abdominal fascia or joint capsule closure represents a challenge to surgeons requiring careful consideration of both their physical properties as well as prior research findings. Additional consideration must be given to potential differences in the reliability of sutures across different procedure types and anatomical sites.17 While a growing body of evidence exists supporting the use of STRATAFIX Symmetric for wound closure in high-tension areas, more data are needed to understand clinical outcomes associated with the use of the device in routine clinical practice across a broad range of procedure types.
This retrospective, single-arm study assessed the cumulative incidence of clinical outcomes among patients undergoing procedures of high-tension areas, including abdominal and orthopedic surgery, using size 0 or 1 STRATAFIX Symmetric contained in a large, multi-institutional database. Size 0 or 1 STRATAFIX Symmetric, representing thicker sutures typically used in circumstances requiring more tensile strength, was included to increase the likelihood that STRATAFIX Symmetric was used in the fascia or joint capsule.
Material and Methods
Study Design and Data Source
We conducted a retrospective, single-arm, multi-institution cohort study in the Premier Healthcare Database (PHD). The PHD contains hospital administrative and billing discharge data from approximately 1400 hospitals, including 1 in 4 annual inpatient hospital stays, in the United States. Discharge-level information on all International Classification of Diseases, Tenth Revision, Clinical Modification and Procedure Code System (ICD-10-CM and ICD-10-PCS, respectively) diagnoses and procedures recorded during each admission, and patient, hospital, and provider information is contained in the PHD. Detailed service-level information for each hospital day is recorded, including details on devices received. Although the PHD excludes federally funded hospitals (eg, Veterans Affairs), the hospitals included are nationally representative based on bed size, geographic region, location (urban/rural), and teaching hospital status.30
Study Population
We identified patients aged 18 years or older with an inpatient admission between October 1, 2016, and October 31, 2023, with a principal ICD-10-PCS procedure code for open abdominal or orthopedic surgery where size 0 or 1 STRATAFIX Symmetric (see Figure 1) was used. For each patient, the index event was defined as the first inpatient admission meeting these criteria. Patients receiving surgery at a hospital contributing data for at least 30 days from the index procedure date were included. A complete list of codes used to query the database is available in Supplemental Appendix A.
 |
Figure 1 STRATAFIX™ Symmetric PDS™ Knotless Tissue Control Device. Source: Ethicon website: Available from: https://www.jnjmedtech.com/en-US/product/stratafix-symmetric-pds-plus-knotless-tissue-control-device. Accessed: January 16, 2025. |
Study Variables
We measured patient demographics, patient clinical characteristics, procedural characteristics, and hospital as well as provider characteristics at index. Patient demographics included age, sex, race, marital status, and payor type. Patient clinical characteristics were measured using the Elixhauser comorbidity system, a risk-adjustment score comprised 31 comorbid conditions derived from ICD-10-CM diagnosis codes.31 Procedural characteristics included the year of surgery, procedure subtype and anatomical site, and admission type. Procedure subtype and anatomical site were defined based on the principal ICD-10-PCS procedure code recorded at index (see Supplemental Appendix A, Table 1,). Hospital and provider characteristics included hospital bed size, geographic location, urban vs rural setting, teaching status, and procedural physician specialty.
Study Outcomes
Outcomes of interest, including internal wound dehiscence and surgical site infection (SSI), were identified based on ICD-10-CM diagnosis codes (see Supplemental Appendix A, Table 2) recorded at index or within 30 days post-index procedure. Internal wound dehiscence, comprised of a subset of ICD-10-CM diagnosis codes for wound dehiscence, was captured to increase the likelihood the outcome occurred at the fascia or joint capsule. To identify incident outcomes, diagnosis codes present on admission at index were not used to measure study outcomes.
Subgroup and Stratification Variables
All analyses were stratified by procedure type (ie, abdominal or orthopedic surgery). In the abdominal surgery cohort, subgroup analyses were performed for the following procedure subtypes: general surgery, gynecologic surgery, urologic surgery, and colorectal surgery. Colorectal surgery is defined as a general surgery procedure of the colon, intestine, or appendix. Among patients undergoing orthopedic surgery, subgroup analyses were performed for the following procedure subtypes: spinal fusion surgery, hip arthroplasty, and knee arthroplasty.
Statistical Analyses
Descriptive analyses of all study variables in both the abdominal surgery and orthopedic surgery cohorts were conducted. For each study cohort, the cumulative incidence of 30-day internal wound dehiscence and SSI were measured as a proportion. Two-sided 95% confidence intervals (CI) were calculated for each outcome of interest using a Clopper-Pearson exact confidence interval.
Comparison with Prior Literature
To contextualize the study findings, a literature review was performed to compare the incidence of outcomes of interest in the current study to prior literature. A targeted literature search was conducted in PubMed to identify articles published between October 2016 and April 2024 using the keywords “barbed suture”, “triclosan-coated suture”, “STRATAFIX”, “wound dehiscence”, “wound complications”, “surgical site infection”, “abdominal”, “colorectal”, “knee”, “hip”, or “closure”. Articles were first screened based on their title and abstract, where articles containing information on wound complication rates and the use of STRATAFIX Symmetric in high-tension areas including abdominal wall closure or orthopedic procedures were selected. Key findings from 12 articles identified during the targeted literature search were summarized.
Results
Descriptive Analyses of Abdominal Surgery Cohort
A total of 8156 patients undergoing open abdominal surgery using STRATAFIX Symmetric met the study criteria. Patient characteristics of the abdominal surgery cohort are summarized in Table 1. Overall, the mean age was 56.0 (standard deviation [SD] = 17.5) years and just over two-thirds (67.9%) of patients were female. General, gynecologic, and urologic surgery accounted for 52.7%, 33.5%, and 13.7% of procedures, respectively, with colorectal surgery representing 38.4% of procedures.
 |
Table 1 Characteristics of Patients Undergoing Abdominal Surgery |
Supplemental Appendix B, Table 1 contains information on the patient characteristics of each abdominal surgery subgroup. The gynecologic surgery subgroup (N = 2735) contained females with a lower average age (44.2 [SD = 16.4] years) and, as indicated by an Elixhauser comorbidity score between 0 and 1, a higher proportion had few comorbidities (56.0%). A higher proportion of the urologic surgery subgroup (N = 1120) was male (65.1%) and had an Elixhauser comorbidity score >1 (94.6%). Patients in the general surgery (N = 4301) and colorectal surgery (N = 3134) subgroups had the highest average age (62.8 [SD = 14.7] years and 63.0 [SD = 14.9] years, respectively). The proportion of patients with an Elixhauser comorbidity score >1 was 79.44% in the general surgery subgroup and 78.05% in the colorectal surgery subgroup.
Descriptive Analyses of Orthopedic Surgery Cohort
Table 2 shows the patient characteristics of 25,807 patients meeting the study criteria included in the orthopedic surgery cohort. Among these patients, the average age was 69.0 [SD = 11.5] years with 67.7% of patients being 65 years of age or older and 59.6% of patients being female.
 |
Table 2 Characteristics of Patients Undergoing Orthopedic Surgery |
Patient characteristics of each orthopedic surgery subgroup are summarized in Supplemental Appendix B, Table 2. The spinal fusion surgery, hip arthroplasty, and knee arthroplasty subgroups were comprised of a total of 2877 (11.2%), 12,442 (48.2%), and 10,488 (40.6%) of patients, respectively. In the hip and knee arthroplasty subgroups, a similar proportion of patients were aged 65 years or older (72.2% and 67.1%, respectively) and female (60.8% and 60.9%, respectively). A lower proportion of patients in the spinal fusion surgery subgroup were aged 65 years or older (50.0%) and female (49.2%). As indicated by an Elixhauser comorbidity score ≥5, the proportion of patients with high comorbidity was greatest in the hip arthroplasty subgroup (20.4%) followed by the spinal fusion surgery (17.6%) and knee arthroplasty (16.0%) subgroups.
Outcome Analyses of the Abdominal Surgery Cohort
The cumulative incidences of 30-day outcomes of interest for the abdominal surgery cohort and abdominal surgery subgroups are shown in Table 3. In the abdominal surgery cohort, the cumulative incidences of internal wound dehiscence and SSI were 0.65% (95% CI: 0.49%, 0.85%) and 3.54% (95% CI: 3.15%, 3.97%), respectively. The range in the cumulative incidences of outcomes of interest across abdominal surgery subgroups were as follows: internal wound dehiscence, 0.15% to 1.07%; and SSI, 1.46% to 4.72%. A lower cumulative incidence of internal wound dehiscence (0.15% [95% CI: 0.04%, 0.37%]) and SSI (1.46% [95% CI: 1.05%, 1.99%]) was observed in the gynecologic surgery subgroup; and the general surgery subgroup had a modestly higher cumulative incidence of SSI (4.72% [95% CI: 4.11%, 5.40%]).
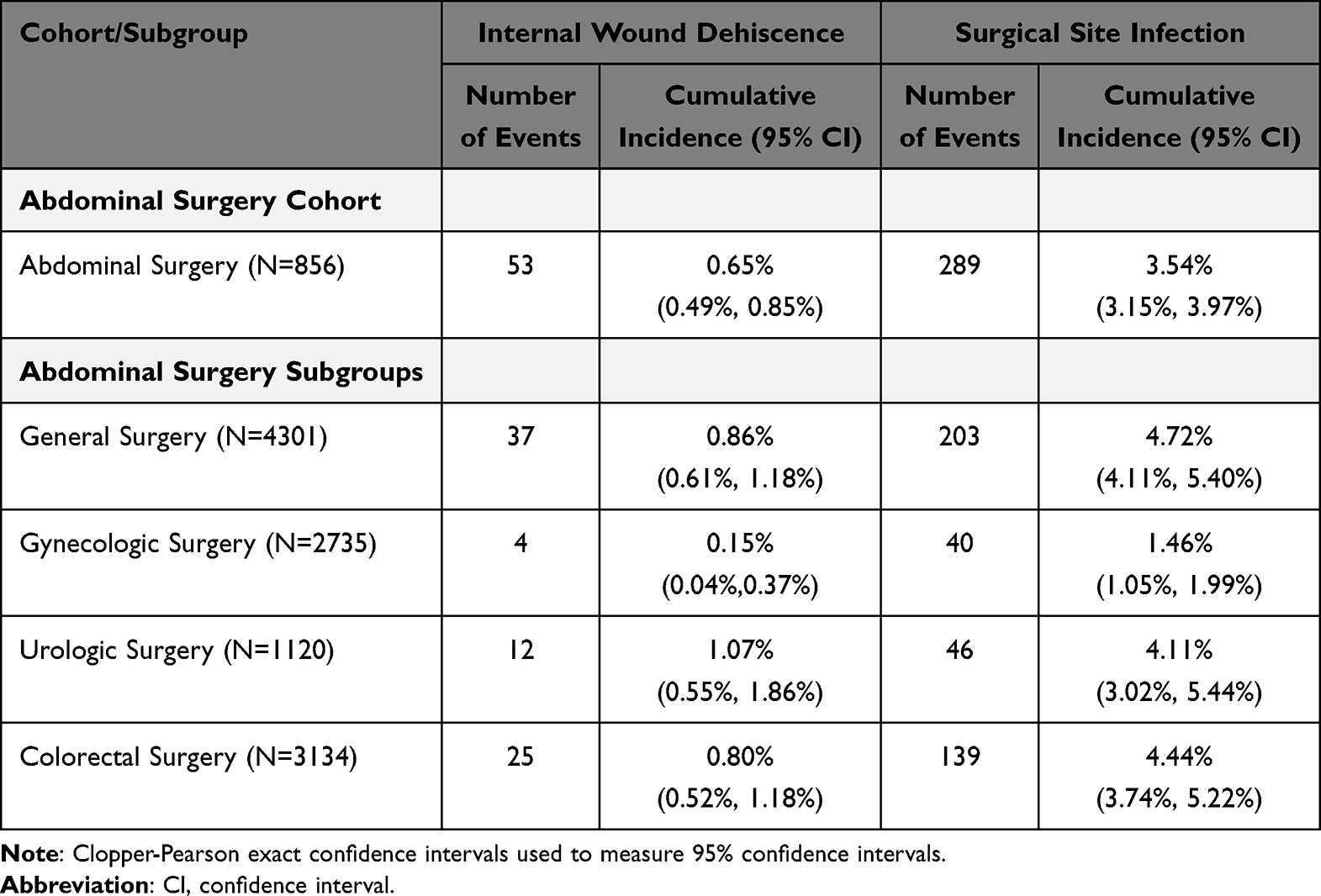 |
Table 3 Summary of Outcome Analyses Among Patients Undergoing Abdominal Surgery Using STRATAFIX Symmetric |
Outcome Analyses of the Orthopedic Surgery Cohort
Table 4 contains a summary of the cumulative incidences of 30-day outcomes of interest in the orthopedic surgery cohort and orthopedic surgery subgroups. The overall cumulative incidences of internal wound dehiscence and SSI in the orthopedic surgery cohort were 0.07% (95% CI: 0.04%, 0.11%) and 0.58% (95% CI: 0.49%, 0.68%), respectively. Among the orthopedic surgery subgroups, outcomes of interest ranged between 0.04% and 0.25% for internal wound dehiscence and 0.34% to 1.74% for SSI. Similar cumulative incidences of outcomes of interest were observed in the hip and knee arthroplasty subgroups. In the spinal fusion surgery subgroup, the cumulative incidence of SSI (1.74% [95% CI: 1.29%, 2.28%]) was slightly higher.
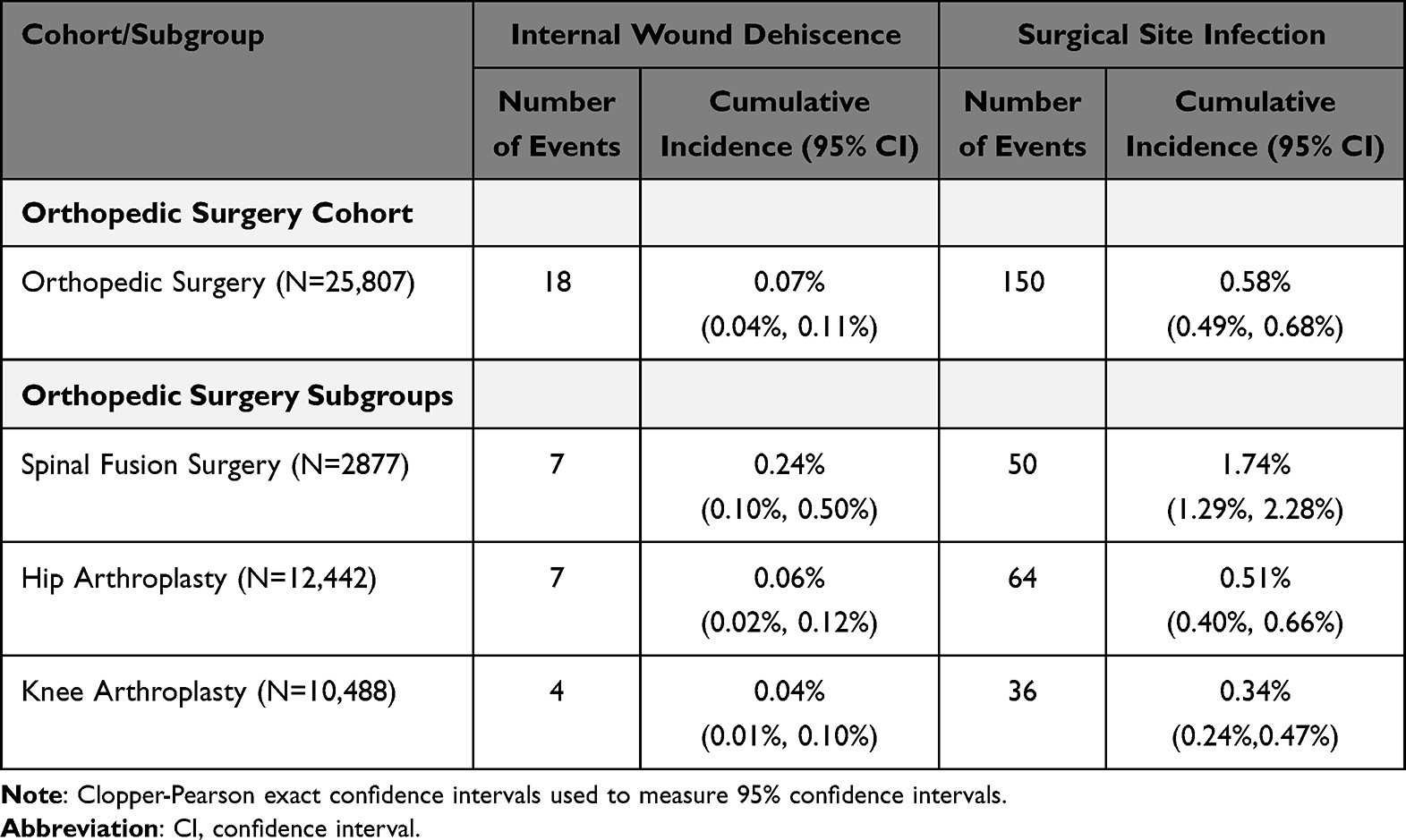 |
Table 4 Summary of Outcomes Analyses Among Patients Undergoing Orthopedic Surgery Using STRATAFIX Symmetric |
Comparison with Prior Literature
Key findings from the 12 publications identified during the targeted literature search are summarized in Table 5. These articles include data from randomized controlled trials, retrospective cohort studies and case series depicting the utilization of STRATAFIX Symmetric for fascial and joint capsule closure or tendon repair in abdominal (5 of 12 articles) and orthopedic surgery (7 of 12 articles).
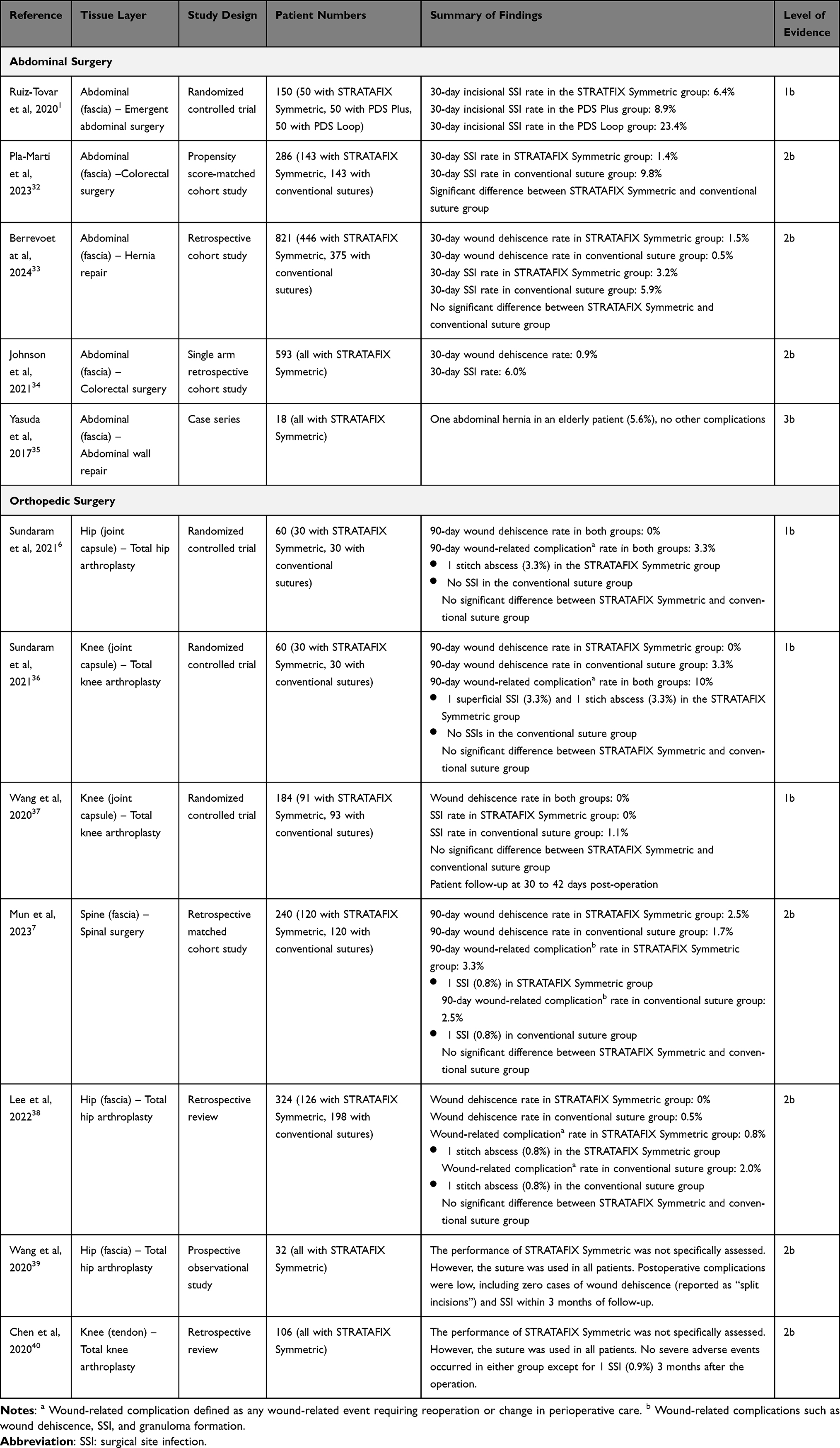 |
Table 5 Prior Literature of Clinical Outcomes Among Patients Undergoing Abdominal or Orthopedic Surgery Using STRATAFIX Symmetric for Wound Closure |
Prior publications in which STRATAFIX Symmetric was used for abdominal fascial closure found a wound dehiscence rate ranging between 0% to 1.5% and SSI rate ranging between 0% and 6.4%, which is similar to the range of 30-day outcomes reported across abdominal surgery subgroups in the current study (internal wound dehiscence: 0.15% to 1.07%; and SSI, 1.46% to 4.72%).
In publications where STRATAFIX Symmetric was used for hip joint capsule (1 article), knee joint capsule (2 articles) or hip fascial (2 articles) closure, or knee tendon repair (1 article) in arthroplasty procedures, no cases of wound dehiscence were observed, and the SSI rate ranged between 0% and 0.9%. These findings were consistent with the current study, which found the hip and knee arthroplasty subgroups to have a low rate of internal wound dehiscence (0.04% and 0.06%, respectively) and SSI (0.34% and 0.51%, respectively). It is important to note that rare outcomes, such as wound dehiscence, may not have been detected in prior literature due to the limited sample size of the STRATAFIX Symmetric group (maximum sample size = 126 patients) contained in these studies. A single article was identified describing the use of STRATAFIX Symmetric in the spine fascia, which reported a 90-day wound dehiscence rate of 2.5% (95% CI: 0.52%, 7.13%) and SSI rate of 0.8% (95% CI: 0.02%, 4.56%). The cumulative incidence of 30-day internal wound dehiscence (0.24% [95% CI: 0.10%, 0.50%) was slightly lower in the current study, albeit these findings may be attributable to differences in the length of the follow-up period (ie, 30 days versus 90 days).
A total of 8 publications compared STRATAFIX Symmetric to conventional sutures, including Vicryl sutures,6,7,36 Vicryl Plus sutures,37,38 PDS sutures,1,33 and conventional non-coated sutures,32 in terms of wound dehiscence and/or SSI for abdominal surgery (3 articles) and orthopedic surgery (5 articles). Among patients undergoing abdominal surgery using conventional sutures, the 30-day wound dehiscence rate was 0.5% (1 article) and SSI rate ranged between 5.9% and 23.4% (3 articles). No significant difference was observed between STRATAFIX Symmetric and conventional sutures in the rate of wound dehiscence (1 article); however, STRATAFIX Symmetric was associated with a significantly lower rate of 30-day SSI (2 of 3 articles) as compared to PDS Loop and conventional non-coated sutures.1,32 Among patients undergoing orthopedic surgery using conventional sutures, no significant differences were found in the rate of wound dehiscence (range: 0% to 3.3%; 5 articles) or SSI (1.1%; 1 article) as compared to STRATAFIX Symmetric.
Discussion
The present study assessed clinical outcomes among patients undergoing a wide spectrum of abdominal and orthopedic procedures with tissue closure incorporating STRATAFIX Symmetric in high-tension areas. Overall, the cumulative incidence of 30-day internal wound dehiscence and SSI were low in both the abdominal surgery and orthopedic surgery cohorts. Similarly, there was a low cumulative incidence of adverse clinical outcomes in subgroup analyses of patients undergoing general, gynecologic, urologic, colorectal, and spinal fusion surgery, and hip and knee arthroplasty. These findings were comparable to those of previously published randomized controlled trials, retrospective cohort studies and case series where STRATAFIX Symmetric was used for wound closure in the fascia or joint capsule.
Based on a meta-analysis of pre-clinical animal studies, it has been proposed the reliability of sutures may differ across different procedure types and anatomical sites.17 The current study found the cumulative incidence of postoperative internal wound dehiscence and SSI to be low when STRATAFIX Symmetric was used in high-tension areas during both abdominal and orthopedic surgery. Adverse clinical outcomes were lowest in the orthopedic surgery cohort and, as expected, modestly higher among patients undergoing clean-contaminated procedures in the abdominal surgery cohort. Moreover, STRATAFIX Symmetric has been demonstrated to possess either similar or improved wound dehiscence and SSI rates in such procedures as compared to conventional sutures in prior literature.1,32–34 While there was a lower cumulative incidence of adverse clinical outcomes among a subgroup of patients undergoing gynecologic surgery in the current study, it is important to note that over a third of the subgroup contained women undergoing obstetric procedures who tended to be younger and healthier.
Guidelines from the European and American Hernia Societies, published in November 2022, provide no recommendation on the use of barbed sutures for wound closure in the abdominal fascia.21 The absence of recommendations on the use of barbed sutures may reflect a paucity in clinical evidence contained in the literature, which, as noted by Theodorou et al, had only shown promising first results in high-risk situations such as emergency laparotomies.41 That being said, there has been mounting evidence supporting the use of barbed sutures in abdominal and arthroplasty procedures in recent years.
Meta-analyses have found barbed sutures to be cost-effective, have shorter wound closure time, and similar complication rates as compared to conventional sutures in both knee and hip arthroplasty.2,42,43 Furthermore, a recent international Delphi panel on wound closure in total hip and knee replacement acknowledged the savings in time and financial resources when using barbed sutures in hip and knee arthroplasty as well as a lower risk of wound complications in total knee replacement.44,45 From an engineering perspective, the physical properties of STRATAFIX Symmetric, a triclosan-coated monofilament prepared from durable polyester polydioxanone with an innovative barb design facilitating high strength soft tissue approximation, are well suited for procedures in high-tension areas. Indeed, similar findings have previously been published from randomized controlled trials and retrospective cohort studies comparing STRATAFIX Symmetric to conventional sutures in abdominal surgery1,32,34 and orthopedic surgery.6,7,36–38 Specifically, these studies found comparable or improved1,32 rates of wound-related complications between STRATAFIX Symmetric and conventional sutures applied in an interrupted manner, including Vicryl sutures,6,7,36 Vicryl Plus sutures,37,38 PDS sutures,1,33 and conventional non-coated sutures.32 The current study further supports the safety and effectiveness of STRATAFIX Symmetric in abdominal and orthopedic procedures in high-tension areas including arthroplasty, and general, gynecologic, urologic, colorectal, and spinal fusion surgery.
Since April 2024, two additional studies have been published comparing the cumulative incidence of wound-related complications among patients undergoing orthopedic procedures using STRATAFIX Symmetric vs conventional sutures. Song et al conducted a randomized controlled trial comparing STRATAFIX Symmetric to conventional interrupted knotted suture technique for deep tissue closure in orthopedic surgery. Glener et al performed a pilot study comparing STRATAFIX Symmetric vs interrupted braided absorbable stitches for fascial closure in spinal surgery. No events of wound dehiscence or SSI were observed in either study.46,47 In Dilday et al, emergency laparotomy fascial closure with triclosan-coated barbed sutures (STRATAFIX Symmetric) showed significantly decreased rates of fascial dehiscence compared with closure with conventional polydioxanone sutures (4% vs 14%; p < 0.05) and a strong trend toward lower SSI events (11% vs 21%; p = 0.07).48 These findings from recent publications further highlight the safety and effectiveness of STRATFIX Symmetric in abdominal and orthopedic surgery.
The current study summarizes the findings of prior literature and adds to the body of evidence demonstrating the safety and effectiveness of STRATAFIX Symmetric for wound closure in high-tension areas. This was the largest study to assess the cumulative incidence of internal wound dehiscence and SSI with 8156 patients in the abdominal surgery cohort and 25,807 patients in the orthopedic surgery cohort. Furthermore, patients were identified from the nationally representative sample of hospitals contained in the Premier Healthcare Database, which captures 1 in 4 annual inpatient admissions. Finally, the study provided real-world evidence on clinical outcomes of STRATAFIX Symmetric in the course of routine clinical practice, thereby increasing the generalizability of the study findings.
Conclusion
The choice of wound closure technique, especially in high-tension areas, remains a challenge. There is mounting literature that knotless sutures, associated with reduced closure time and total hospital costs, such as STRATAFIX Symmetric have comparable or improved wound-related complications rate to conventional sutures applied in an interrupted fashion in procedures of high-tension areas. In this study of 8156 and 25,807 patients undergoing abdominal and orthopedic surgery, respectively, with closure of the fascia or joint capsule incorporating STRATAFIX Symmetric, the cumulative incidence of internal wound dehiscence and SSI was low. The cumulative incidence of clinical outcomes observed in the current study falls within the range reported in prior literature, thereby indicating the safety and effectiveness of STRATAFIX Symmetric in abdominal and orthopedic procedures of high-tension areas. It is hoped the findings of the current study will support clinician decision-making for the benefit of patients.
Abbreviations
PGA, polyglycolic acid; PGLA, poly-glycolide-co-lactide; PHD, Premier Healthcare Database; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification; ICD-10-PCS, International Classification of Diseases, Tenth Revision, Procedure Coding System; CI, confidence interval; SD, standard deviation; SSI, surgical site infection.
Data Sharing Statement
The data that support the findings of this study are available from Premier Applied Sciences® but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Ethics Approval and Informed Consent
Pursuant to Title 45 Code of Federal Regulations, Part 46 of the United States, specifically 45 CFR 46.104 (d)(4), retrospective analyses conducted in the DOD and MDCD are considered exempt from informed consent and institutional review board (IRB) approval in the United States. All methods were carried out in accordance with relevant guidelines and regulations.
Acknowledgments
There are no further acknowledgements to disclose.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by Johnson & Johnson.
Disclosure
Stephen P Fortin, Kerstin Spychaj, Jörg Tomaszewski, Holly Grebeck, Paul M Coplan, and Shumin Zhang are employees of Johnson & Johnson or subsidiary companies of Johnson & Johnson and own stock of Johnson & Johnson. Rithwik Yalla is a paid consultant for Johnson & Johnson. The authors report no other conflicts of interest in this work.
References
1. Ruiz-Tovar J, Llavero C, Jimenez-Fuertes M, Duran M, Perez-Lopez M, Garcia-Marin A. Incisional surgical site infection after abdominal fascial closure with triclosan-coated barbed suture vs triclosan-coated polydioxanone loop suture vs polydioxanone loop suture in emergent abdominal surgery: a randomized clinical trial. J Am Coll Surg. 2020;230(5):766–774. doi:10.1016/j.jamcollsurg.2020.02.031
2. Raja BS, Gowda AKS, Choudhury AK, Paul S, Kalia RB. Barbed sutures for total hip and knee arthroplasty have shorter wound closure time and are cost-effective in comparison to traditional sutures: a systematic review and meta-analysis of 16 randomized controlled trials. Indian J Orthop. 2022;56(7):1156–1173. PMID: 35813548; PMCID: PMC9232689.doi:10.1007/s43465-022-00638-z
3. Wiggins T, Majid MS, Markar SR, Loy J, Agrawal S, Koak Y. Benefits of barbed suture utilisation in gastrointestinal anastomosis: a systematic review and meta-analysis. Ann R Coll Surg Engl. 2020;102(2):153–159. doi:10.1308/rcsann.2019.0106
4. Elmallah RK, Khlopas A, Faour M, et al. Economic evaluation of different suture closure methods: barbed versus traditional interrupted sutures. Ann Transl Med. 2017;5(Suppl. 3):S26. doi:10.21037/atm.2017.08.21
5. Li P, Zhang W, Wang Y, et al. Barbed suture versus traditional suture in primary total knee arthroplasty: a systematic review and meta-analysis of randomized controlled studies. Medicine. 2020;99(21):e19945–e19945. doi:10.1097/MD.0000000000019945
6. Sundaram K, Piuzzi NS, Klika AK, et al. Barbed sutures reduce arthrotomy closure duration and suture utilisation compared to interrupted conventional sutures for primary total Hip arthroplasty: a randomised controlled trial. HIP Int. 2020:1120700020911891. doi:10.1177/1120700020911891.
7. Mun J, Hyun SJ, Lee JK, An S, Kim KJ. Surgical and clinical outcomes associated with the use of barbed sutures and self-adhering mesh system and polymeric glue for wound closure in multilevel or revision spinal surgery: a matched cohort comparative study with conventional wound closure procedure. Neurospine. 2023;20(3):981–988. doi:10.14245/ns.2346534.267
8. Johnston SS, Chen BP, Tommaselli GA, Jain S, Pracyk JB. Barbed and conventional sutures in spinal surgery patients: an economic and clinical outcomes comparison. J Wound Care. 2020;29(Sup5a):S9–S20. PMID: 32412893.doi:10.12968/jowc.2020.29.Sup5a.S9
9. Velotti N, Manigrasso M, Di Lauro K, et al. Barbed suture in gastro-intestinal surgery: a review with a meta-analysis. Surgeon. 2022;20(2):115–122. Epub 2021 Apr 2. PMID: 33820730.doi:10.1016/j.surge.2021.02.011
10. Agarwal S, D’Souza R, Ryu M, Maxwell C. Barbed vs conventional suture at cesarean delivery: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2021;100(6):1010–1018. Epub 2021 Feb 5. PMID: 33404082.doi:10.1111/aogs.14080
11. Khanuja K, Burd J, Ozcan P, Peleg D, Saccone G, Berghella V. Suture type for hysterotomy closure: a systematic review and meta-analysis of randomized controlled trials. Am J Obstet Gynecol MFM. 2022;4(6):100726. Epub 2022 Aug 19. PMID: 35995367.doi:10.1016/j.ajogmf.2022.100726
12. Gardella B, Dominoni M, Iacobone AD, et al. What is the role of barbed suture in laparoscopic myomectomy? A meta-analysis and pregnancy outcome evaluation. Gynecol Obstet Invest. 2018;83(6):521–532. Epub 2018 Apr 12. PMID: 29649814.doi:10.1159/000488241
13. Lin Y, Liao B, Lai S, et al. The application of barbed suture during the partial nephrectomy may modify perioperative results: a systematic review and meta-analysis. BMC Urol. 2019;19(1):5. PMID: 30630449; PMCID: PMC6329109.doi:10.1186/s12894-018-0435-3
14. Bertolo R, Campi R, Klatte T, et al. Suture techniques during laparoscopic and robot-assisted partial nephrectomy: a systematic review and quantitative synthesis of peri-operative outcomes. BJU Int. 2019;123(6):923–946. doi:10.1111/bju.14537
15. Rubin JP, Hunstad JP, Polynice A, et al. A multicenter randomized controlled trial comparing absorbable barbed sutures versus conventional absorbable sutures for dermal closure in open surgical procedures. Aesthet Surg J. 2014;34(2):272–283. Epub 2014 Jan 13. PMID: 24421408.doi:10.1177/1090820X13519264
16. Su X, Lin Y, Wu Y, et al. Effectiveness and safety of knotless barbed sutures in cosmetic surgery: a systematic review and meta-analysis. J Plast Reconstr Aesthet Surg. 2023;87:416–429.> Epub 2023 Oct 13. PMID: 37939647. doi:<doi
17. Xiang N, Lin Y, Su X, et al. Assessing the application of barbed sutures in comparison to conventional sutures for surgical applications: a global systematic review and meta-analysis of preclinical animal studies. Int J Surg. 2024;110(5):3060–3071. PMID: 38445518; PMCID: PMC11093437.doi:10.1097/JS9.0000000000001230
18. Li Y, Meng Q, Chen S, et al. Advances, challenges, and prospects for surgical suture materials. Acta Biomater. 2023;168:78–112.> Epub 2023 Jul 28. PMID: 37516417. doi:<doi
19. Hochberg J, Meyer KM, Marion MD. Suture choice and other methods of skin closure. Surg Clin North Am. 2009;89(3):627–641. PMID: 19465201.doi:10.1016/j.suc.2009.03.001
20. San Valentin EMD, Barcena AJR, Klusman C, Martin B, Melancon MP. Nano-embedded medical devices and delivery systems in interventional radiology. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2023;15(1):e1841. Epub 2022 Aug 10. PMID: 35946543; PMCID: PMC9840652.doi:10.1002/wnan.1841
21. Deerenberg EB, Henriksen NA, Antoniou GA, et al. Updated guideline for closure of abdominal wall incisions from the European and American Hernia Societies. Br J Surg. 2022;109(12):1239–1250. Erratum in: Br J Surg. 2023 Jan 10;110(2):287. doi: 10.1093/bjs/znac412. PMID: 36026550; PMCID: PMC10364727.doi:10.1093/bjs/znac302
22. Otto-Lambertz C, Decker L, Adams A, Yagdiran A, Eysel P. Can triclosan-coated sutures reduce the postoperative rate of wound infection? Data from a systematic review and meta-analysis. Surgery. 2023;174(3):638–646. Epub 2023 Jun 14. PMID: 37328397.doi:10.1016/j.surg.2023.04.015
23. Ming X, Rothenburger S, Nichols MM. In vivo and in vitro antibacterial efficacy of PDS plus (polidioxanone with triclosan) suture. Surg Infect (Larchmt). 2008;9(4):451–457. PMID: 18687027.doi:10.1089/sur.2007.061
24. World Health Organization. (2018). Global guidelines for the prevention of surgical site infection, 2nd ed. World Health Organization. License: CC BY-NC-SA 3.0 IGO. Available from: https://iris.who.int/handle/10665/277399.
25. Ban KA, Minei JP, Laronga C, et al. American college of surgeons and surgical infection society: surgical site infection guidelines, 2016 update. J Am Coll Surg. 2017;224(1):59–74. Epub 2016 Nov 30. PMID: 27915053.doi:10.1016/j.jamcollsurg.2016.10.029
26. Calderwood MS, Anderson DJ, Bratzler DW, et al. Strategies to prevent surgical site infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2023;44(5):695–720. Epub 2023 May 4. PMID: 37137483; PMCID: PMC10867741.doi:10.1017/ice.2023.67
27. National Institute for Health and Care Excellence (NICE). Plus Sutures for preventing surgical site infection. Medical technologies guidance [MTG59]. Cited January 2025 [Webpage]. London & Manchester: NICE; 2021. Available from: https://www.nice.org.uk/guidance/mtg59.
28. U.S. Food and Drug Administration. Center for Devices and Radiologic Health, K182873 510(k) Letter and Summary. [Online]. 2019. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf18/K182873.pdf.
29. Nawrocki JG, Nonnenmann H, Mooney M, Sutton N, Schmitz ND.A high-strength, absorbable, antibacterial knotless tissue control device for fascial closure. Curr Obstet Gynecol Rep. 2017;6(2):175–181. Epub 2017 May 6. PMID: 28603661; PMCID: PMC5442192.doi:10.1007/s13669-017-0208-0
30. PINC. AITM Healthcare Data: data that informs and perform, Dec 2023. PINC AITM Applied Sciences, Premier Inc. Available from: https://offers.premierinc.com/rs/381-NBB-525/images/PINC_AI_Healthcare_Data_White_Paper.pdf.
31. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. doi:10.1097/00005650-199801000-00004
32. Pla-Marti V, Martin-Arévalo J, Moro-Valdezate D, et al. Triclosan-coated barbed sutures in elective laparoscopic colorectal cancer surgery: a propensity score matched cohort study. Surg Endosc. 2023;37(1):209–218. doi:10.1007/s00464-022-09418-0
33. Berrevoet F, van Cauteren L, Gunja N, et al. Clinical outcomes of triclosan-coated barbed suture in open hernia repair: a retrospective cohort study. Hernia. 2024;28(4):1239–1247. Epub ahead of print. PMID: 38609582.doi:10.1007/s10029-024-03012-0
34. Johnson BH, Rai P, Jang SR, Johnston SS, Chen BP. Real-world outcomes of patients undergoing open colorectal surgery with wound closure incorporating triclosan-coated barbed sutures: a multi-institution, retrospective database study. Med Devices. 2021;14:65–75. doi:10.2147/MDER.S297671
35. Yasuda S, Tomita K, Kiya K, Hosokawa K. STRATAFIX for abdominal wall repair following abdominal flap harvest. Plast Reconstr Surg Glob Open. 2017;5(11):e1572. doi:10.1097/GOX.0000000000001572
36. Sundaram K, Warren JA, Klika A, Piuzzi NS, Mont MA, Krebs V. Barbed sutures reduce arthrotomy closure duration compared to interrupted conventional sutures for total knee arthroplasty: a randomized controlled trial. Musculoskelet Surg. 2021;105(3):275–281. doi:10.1007/s12306-020-00654-y
37. Wang W, Yan S, Liu F, et al. A Symmetric anchor designed barbed suture versus conventional interrupted sutures in total knee arthroplasty: a multicenter, randomized controlled trial. J Orthop Surg. 2020;28(3):2309499020965681. doi:10.1177/2309499020965681
38. Lee S, Kee T, Jung MY, Yoon PW. A comparison of barbed continuous suture versus conventional interrupted suture for fascial closure in total Hip arthroplasty. Sci Rep. 2022;12(1):3942. doi:10.1038/s41598-022-07862-5
39. Wang LS, Wang XY, Tu HT, Huang YF, Qi X, Gao YH. Octyl-2-cyanoacrylate tissue adhesive without subcuticular suture for wound closure after total Hip arthroplasty: a prospective observational study on thirty-two cases with controls for 3 months follow-up. J Orthop Surg Res. 2020;15(1):467. doi:10.1186/s13018-020-01997-9
40. Chen L, Yang J, Xie J, Hu Y, Zeng M. Clinical outcome of different skin closure in total-knee arthroplasty: running subcuticular closure vs intermittent closure: a retrospective study. Medicine. 2020;99(34):e21947. doi:10.1097/MD.0000000000021947
41. Theodorou A, Banysch M, Gök H, Deerenberg EB, Kalff JC, von Websky MW. Don’t fear the (small) bite: a narrative review of the rationale and misconceptions surrounding closure of abdominal wall incisions. Front Surg. 2022;9:1002558.> PMID: 36504582; PMCID: PMC9727106. doi:<doi
42. Sun C, Chen L, Du R, Wu S, Ma Q, Cai X. Barbed sutures in total knee arthroplasty: a meta-analysis of randomized-controlled trials. J Knee Surg. 2021;34(14):1516–1526. Epub 2020 May 27. PMID: 32462647.doi:10.1055/s-0040-1710373
43. Li E, Niu W, Lu T, et al. A comparison between barbed suture and conventional suture in total knee arthroplasty: a systematic review and meta-analysis. Arthroplasty. 2020;2(1):8. PMID: 35236431; PMCID: PMC8796359.doi:10.1186/s42836-020-00028-6
44. Ainslie-Garcia M, Anderson LA, Bloch BV, et al. International delphi study on wound closure and dressing management in joint arthroplasty: part 1: total knee arthroplasty. J Arthroplasty. 2024;39(4):878–883. Epub 2024 Jan 18. PMID: 38244638.doi:10.1016/j.arth.2023.12.032
45. Ainslie-Garcia M, Anderson LA, Bloch BV, et al. International delphi study on wound closure and incision management in joint arthroplasty part 2: total hip arthroplasty. J Arthroplasty. 2024;39(6):1524–1529. Epub 2024 Feb 5. PMID: 38325531.doi:10.1016/j.arth.2024.01.047
46. Song M, Cho Y. A prospective randomized controlled study of stratafix versus standard-of-care for deep tissue closure in orthopedic surgery. Clin Orthop Surg. 2024;16(5):820–826. Epub 2024 Sep 13. PMID: 39364101; PMCID: PMC11444938.doi:10.4055/cios22017
47. Glener SR, Patel PD, Serva SN, Self DM, Heller JE. Prospective analysis of STRATAFIX™ symmetric PDS plus suture for fascial closure in spinal surgery: a pilot study. Neurosurg Rev. 2024;47(1):438. PMID: 39152260; PMCID: PMC11329535.doi:10.1007/s10143-024-02671-y
48. Dilday J, McGillen P, Park S, et al. Is barbed better? Evaluation of triclosan-coated barbed suture on wound complications following emergency laparotomy. J Trauma Acute Care Surg. 2024;97(1):149–157. Epub 2024 Apr 10. PMID: 38595220.doi:10.1097/TA.0000000000004341
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.