Back to Journals » OncoTargets and Therapy » Volume 10
Clinical outcome and toxicity evaluation of simultaneous integrated boost pelvic IMRT/VMAT at different dose levels combined with androgen deprivation therapy in prostate cancer patients
Authors Daoud MA, Aboelnaga EM ![]() , Alashry MS, Fathy S
, Alashry MS, Fathy S ![]() , Aletreby MA
, Aletreby MA
Received 6 May 2017
Accepted for publication 14 July 2017
Published 12 October 2017 Volume 2017:10 Pages 4981—4988
DOI https://doi.org/10.2147/OTT.S141224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ingrid Espinoza
Mohamed A Daoud,1,2 Engy M Aboelnaga,1 Mohamed S Alashry,1 Salwa Fathy,3 Mostafa A Aletreby2,4
1Department of Clinical Oncology and Nuclear Medicine, Mansoura Faculty of Medicine, Mansoura University, Mansoura, 2Department of Oncology, Fakeeh Hospital, Jeddah, Saudi Arabia; 3Department of Radiation, Oncology and Nuclear Medicine, South Egypt Cancer Institute, Assiut University, Assiut, 4Department of Medical Physics, Kasr Alainy Faculty of Medicine, Al Manial, Egypt
Background: The role of dose escalation in patients receiving long-term androgen deprivation therapy (ADT) is still a controversial issue. The aim of the current study was to evaluate whether dose escalation for ≥76–80 Gy had any advantage in terms of biochemical disease-free survival (BDFS), distant metastasis-free survival (DMFS), or overall survival outcomes over the dose levels from 70 to <76 Gy.
Patients and methods: The study included a cohort of 24 patients classified with high- and intermediate-risk localized prostate cancer. All patients received ADT, starting at 4–6 months before radiation therapy and continued for a total period of 12–24 months in high-risk patients. The treatment plan was given in two phases. In the first phase, the nodal planning target volume (PTV) and the prostate PTV received 48.6 and 54 Gy, respectively, over 27 fractions. The treatment was applied through intensity-modulated radiation therapy or volumetric modulated arc therapy with a simultaneous integrated boost technique.
Results: More than half of the patients were in T3–T4 stage, 79.1% of the patients were in the high-risk category, and all patients received ADT. The rate of acute grade II gastrointestinal and genitourinary toxicities in all patients were 41.7% and 62.5%, respectively. The rate of freedom from grade II rectal toxicity at 2 years was 89% and 83% for patients treated with dose levels <76 and ≥76 Gy, respectively. The rate of BDFS at 2 years was 90% and 85% for doses <76 and ≥76 Gy, respectively. The DMFS at 2 years was 100% and 76% for dose levels <76 and ≥76 Gy, respectively.
Conclusion: In the current study, there were no significant differences in the BDFS and DMFS between patients treated with a dose of <76 and ≥76 Gy, including elective pelvic lymph nodes irradiation combined with ADT.
Keywords: androgen deprivation therapy, dose escalation, cancer prostate, combined therapy, radiation dose, intermediate and high risk
Introduction
The role of dose escalation in patients receiving long-term androgen deprivation therapy (ADT) is still a controversial issue. Based on meta-analyses of multiple randomized trials, the combined dose-escalated external beam radiotherapy (DE-EBRT) and ADT have been proved to improve prostate cancer outcomes.1,2 This is applicable to patient populations with either clinically node-negative disease or low volume of nodal involvement.3,4 There are two randomized trials comparing DE-EBRT with 74 Gy versus conventional radiation dose of 64 Gy for patients receiving ADT.5,6 In these two studies, all patients received neoadjuvant ADT. Only one study reported a significant benefit for dose escalation up to 74 Gy in the high-risk group.10 Furthermore, whether pelvic lymph nodes (PLNs) should be treated in intermediate- and high-risk prostate cancer patients with either surgery or radiotherapy is still controversial. Retrospective surgical analysis by Schiavina et al demonstrated a lower biochemical failure (BF) rates as defined by prostate specific antigen (PSA) greater than 0.2 ng/mL in patients undergoing extended PLN dissection.7 The same finding was reported by Morikawa and Roach, and they explained why some studies were negative in demonstrating the benefit of whole pelvic radiotherapy by the fact that predictions of nodal disease based on surgical series may underestimate the true extent of involvement due to missing of some pathologically undetectable micrometastasis.8 Another two randomized Phase III studies addressed this issue, the radiation therapy oncology group (RTOG) 9413 and the genito urinary tumor group 01;9,10 however, they reached conflicting conclusions. The rationale of the PLN irradiation in patients with high risk of subclinical lymph node (LN) involvement by Roach equation (≥15%) either radiologically or pathologically involved nodes is to improve loco-regional control and, possibly, the survival, as the microscopic or gross residual disease could be a critical source of distant metastases.11 Intensity-modulated radiotherapy (IMRT) for PLNs enhances treatment dose conformity and enables dose escalation to the clinical target volume (CTV) while decreasing dose to the surrounding organs at risk (OAR), resulting in increase of the therapeutic ratio.12–14 Volumetric modulated arc therapy (VMAT) is a further evolution of IMRT, which may enable more efficient radiation treatment.15
The aim of the current study was to evaluate whether combined ADT and dose escalation up to 76–80 Gy had any advantage in terms of biochemical disease-free survival (BDFS), distant metastasis-free survival (DMFS), or overall survival (OS) outcomes over combined ADT and dose levels from 70 to <76 Gy in our cohort of high- and intermediate-risk prostate cancer patients.
Materials and methods
Patients
This analysis included a cohort of 24 patients diagnosed with high- and intermediate-risk localized prostate cancer treated by combined ADT and simultaneous integrated boost (SIB) WP-IMRT/VMAT followed by prostate boost to total doses between 70 and 80 Gy. The patients were treated during the period between March 2013 and July 2016. All patients were diagnosed by trans-rectal ultrasound guided core biopsy, and 12 cores were obtained from each patient. The exclusion criteria included those patients with post prostatectomy, National Comprehensive Cancer Network-defined low risk, metastatic, histology other than adenocarcinoma, or did not receive ADT. The local institutional ethics committee of King Abdullah Medical city approved the study, and all patients provided informed consent to be part of the study. Patient characteristics are shown in Table 1. All patients received ADT, starting at 4–6 months before radiation therapy and continued for a total period of 12–24 months in the high-risk group of patients.
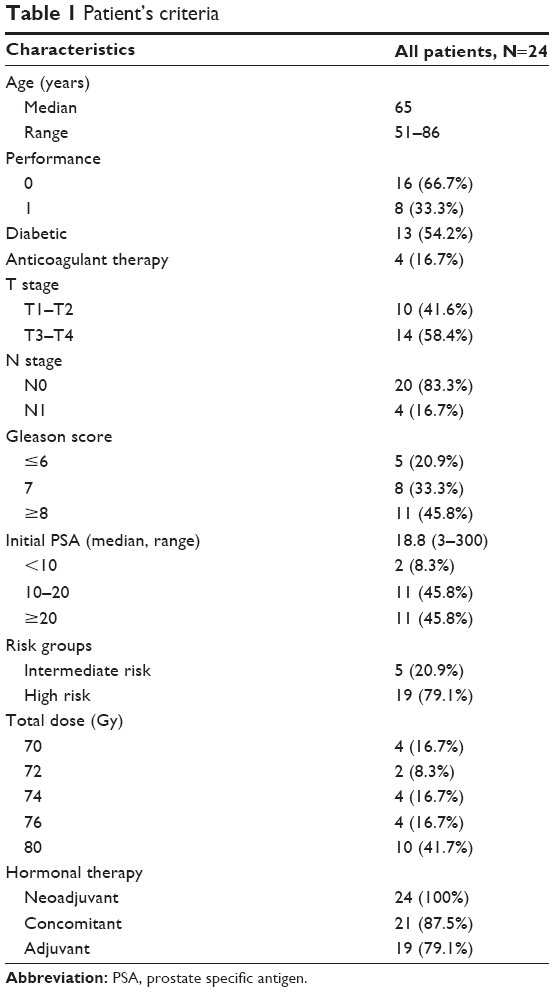 | Table 1 Patient’s criteria |
Simulation, organ contouring, and planning
Computed tomography (CT) was acquired in the supine position, with 2 mm slice thickness from the dome of diaphragm to about 5 cm below the ischial tuberosities. Immobilization was obtained using headrest, kneefix, and feetfix (CIVCO Medical Solutions, Coralville, IA, USA). Before CT simulation, patients were instructed to have a comfortably filled bladder, by drinking 1 L of water, and an empty rectum. The CT data set was transferred to the Eclipse ver. 16.0 treatment planning system (Varian Medical Systems, Palo Alto, CA, USA). The prostate CTV was defined as the entire prostate and the seminal vesicles, and any visible tumor extension. The prostate planning target volume (PTV) was generated by adding a 10 mm margin to the prostate CTV in all dimensions, except posteriorly, where a 6 mm margin was added. Based on the consensus recommendations of the RTOG, the nodal CTV consisted of a 0.7 cm expansion volume on the obturator vessels, the common iliac, external, and internal iliac vessels, while excluding adjacent bone, muscle, bowel, and bladder. The nodal CTV commenced at the level of L5 to S1 interspace, with volumes of the external iliac nodes stopping at the top of the femoral head and the obturator nodal volumes stopping just above the symphysis pubis.16 The presacral nodes were included in the nodal CTV down to S3–S2 interspace. The nodal PTV was defined by adding 0.3 mm expansion to the nodal CTV. For the prostate boost, the CTV included the prostate and proximal 6–8 mm of the seminal vesicles. In case of clinically proved seminal vesicle infiltration, the whole seminal vesicles were included in the CTV boost. The PTV boost was generated by adding 6 mm margin to the CTV boost except 5 mm posteriorly. Contouring of the OAR followed the RTOG pelvic normal tissue contouring guidelines. The rectum was contoured from the level of the ischial tuberosities to the recto-sigmoid flexure, and the whole bladder was contoured from its apex to the dome. Both femoral heads were delineated to the level of the ischial tuberosities. The bowel bag was contoured as the entire volume of peritoneal space from diaphragmatic dome down to the level of S1. The treatment plan was given in two phases. In the first phase, the nodal PTV and the prostate PTV received 48.6 and 54 Gy, respectively, over 27 fractions. Treatment was applied through IMRT or VMAT with SIB technique. In IMRT plans, nine co-planner fields were aligned equal-spaced in 360° around the patient (0, 40, 80, 120, 160, 200, 240, 280, and 320). In VMAT plans, double-arc VMAT clockwise and counterclockwise (CW & CCW) were used. Control points for each arc were adjusted to give at least 1.5 angle step resulting in 178 control points. Variable collimator angle was defined for each arc to minimize the tongue and groove effect. Planning risk volumes were created for rectum and bladder to exclude from the high-dose region. Other helping contours (ring structures with 0.3 cm internal margin and 3 cm external margin) were created around the nodal and prostate PTVs separately for better control of the dose fall off beyond each PTV. A set of dose constrains were defined for the PTVs and the OARs, and no normalization method was selected for any IMRT or VMAT plan. Two lower limits were defined for each PTV as 100% and 97% of the volume and prescribed to 95% and 100% of the dose; also two upper limits, 2% and 0.1% of the volume were defined as 101% and 103% of the prescribed dose, respectively. By using these constrains and through the interactive optimization process, the mean and median dose for each PTV is usually kept equal to the corresponding prescribed dose. Smoothing objectives were also used to have smoother fluence in the x-direction to ensure minimal μ factor. In the second phase, the prostate PTV received 18–26 Gy over 9–13 fractions using double-arc VMAT (CW & CCW). Both phases were optimized using Photon Optimization algorithm newly developed in Eclipse V16.0.03. Treatment plans were considered acceptable when ≥95% of the PTV received ≥95% of the prescribed dose. For the OAR, dose volume constraints were rectal mean dose <50 Gy, minimal dose of 70 Gy (V70 Gy) <15%, and V50 Gy <45%; V70 Gy <25%; and V50 Gy <50% for the bladder. For the femoral heads, the maximal point dose was <55 Gy and minimal dose to 2% (D2%) was <50 Gy. For the bowel bag, V45 Gy was <195 mL. The dose calculation was performed using the Anisotropic Analytic Algorithm (version 16.0.03) and a voxel size of 0.25×0.25×0.25 cm3.
Image guidance
Patients were treated with a Trilogy treatment unit (Varian Medical Systems). Daily kilovoltage (KV) image guidance with on board imaging (OBI) and bi-weekly cone beam CT (CBCT) was performed in all patients. In the initial set up, the patients were immobilized in headrest, kneefix, and feetfix (CIVCO); the skin marks on the patient were used after applying shift. Orthogonal KV radiographs of the patients were then obtained using the OBI and registered to the reference digitally reconstructed radiographs generated from the planning CT. Once the bone registration was well adjusted, CBCT images were also performed and used to obtain the target/soft tissue registration.
Acute and late radiation toxicities
All patients were checked weekly during radiation therapy, once in 2 weeks, and then monthly thereafter. Acute toxicities were reported during radiation therapy and in the first 3 months following treatment. Late toxicities were reported after the initial 3 months of follow-up. Toxicity was assessed using the Common Terminology Criteria for Adverse Events version 4.0 adverse event scoring system.
Statistical analysis
Patients were divided into two groups according to dose levels of <76 Gy and ≥76 Gy. BDFS was defined as survival free from the event of PSA relapse, and DMFS was defined as survival free from the event of metastatic relapse, which were calculated using Kaplan–Meier curves, and the log-rank test was used to compare survival between groups. Univariate and multivariate analyses were done to assess the relationship between potential prognostic factors and BDFS, DMFS, and OS. The variables included were age (≤65 vs >65 years), pretreatment PSA (<10 vs ≥10 ng/mL), Gleason score (6–7 vs 8–10), and radiation dose (<76 and ≥76 Gy). Fisher’s exact test was used to compare the differences in acute toxicity grades between the two dose levels. All statistical analyses were performed using the software SPSS version 22.0 (IBM, Armonk, NY, USA). All reported P-values are two-tailed, and P<0.05 was considered statistically significant. Follow-up time was calculated from the start of ADT.
Results
The study included 24 patients with adenocarcinoma of the prostate treated by combined ADT and SIB IMRT/VMAT for total doses of 70–80 Gy. The demographic data of all patients are summarized in Table 1. The median age at diagnosis was 65 years (range 51–86), more than half of the patients were in (T3–T4) stage, 79.1% of the patients were in the high-risk category, and all patients received ADT. All patients were given radiation therapy in two phases, 15 patients received SIB-IMRT in phase one to the pelvis and prostate followed by prostate boost VMAT. The rest of patients were given SIB-VMAT in both the phases. The prognostic factors including age, stage, GS, and pre-treatment PSA were comparable among both the groups (Table 2). Also, there were no significant differences in the rate of acute gastrointestinal (GI) and genitourinary (GU) toxicities between the two groups (Table 3). The rate of acute grade II GI and GU toxicities in all patients were 41.7% and 62.5%, respectively (Table 4). There were no significant differences in the rate of acute grade II toxicities between the two dose levels with reported GI toxicity 40% and 42.9%, and GU toxicity of 62.5% and 64.3% for doses <76 and ≥76 Gy, respectively. There were no reported late grade III toxicity of GI or GU, and the late GI toxicity was only rectal. The rate of freedom from grade II rectal toxicity at 2 years was 89% and 83% for patients treated with dose levels <76 and ≥76 Gy, respectively (Figure 1). For late grade II GU toxicity, the rate of freedom from toxicity at 2 years was 89% and 92% for dose levels <76 and ≥76 Gy, respectively (Figure 2). The rate of BDFS at 2 years was 90% and 85% for doses <76 and ≥76 Gy, respectively (Figure 3). In univariate and multivariate analyses, there was no significant correlation between the dose level and BDFS. Also, in multivariate analysis, no predicting factors had effect on the BDFS or DMFS, like age group (<65 and >65 years), PSA groups (<10 and >10), Gleason score (≤7 and ≥8), N0 and N1, and T-stage groups. In four patients with N1, one of them developed BF while the other three patients obtained complete response and still under follow-up. Only one patient developed distant metastasis in the bone and extra-regional LNs. The distant metastasis free survival at 2 years was 100% and 76% for doses <76 and ≥76 Gy, respectively (Figure 4). The overall survival at 2 years was 86% and 100% for dose levels <76 and ≥76 Gy, respectively (Figure 5). Only one reported death was related to non-prostate cancer-related death.
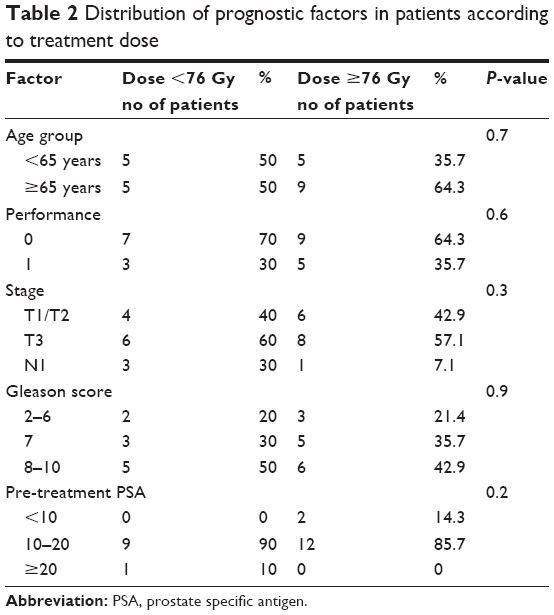 | Table 2 Distribution of prognostic factors in patients according to treatment dose |
 | Table 3 Acute toxicity in relation to dose levels |
 | Table 4 Overall grade II toxicity by treatment dose |
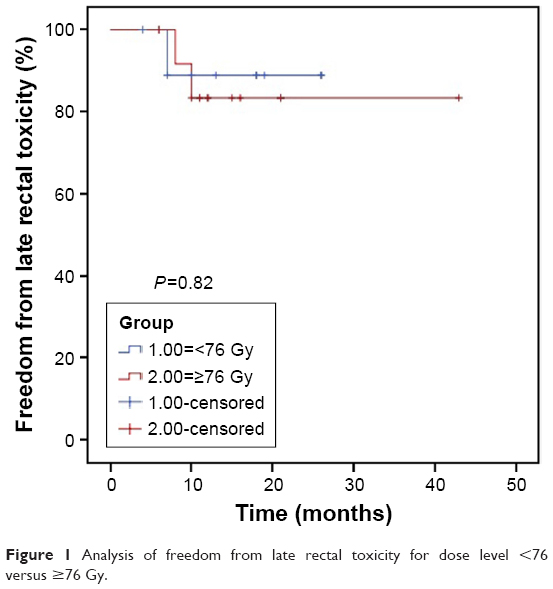 | Figure 1 Analysis of freedom from late rectal toxicity for dose level <76 versus ≥76 Gy. |
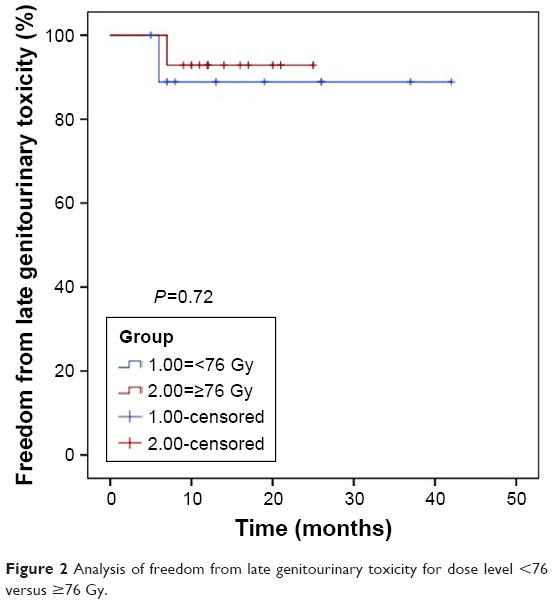 | Figure 2 Analysis of freedom from late genitourinary toxicity for dose level <76 versus ≥76 Gy. |
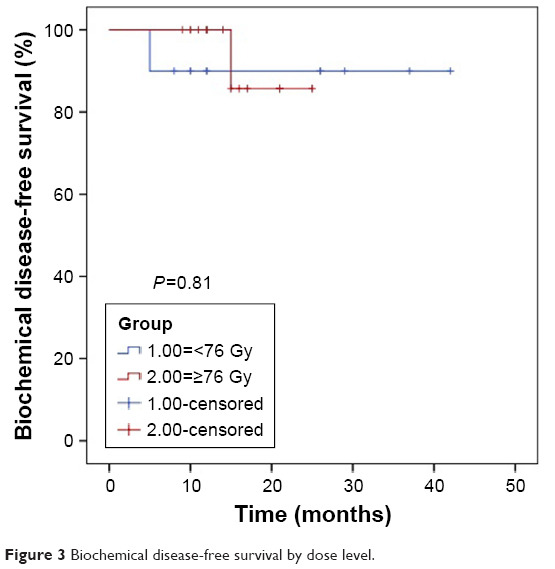 | Figure 3 Biochemical disease-free survival by dose level. |
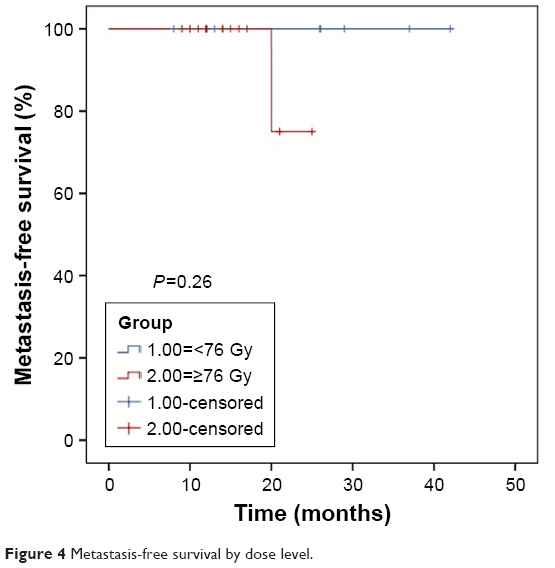 | Figure 4 Metastasis-free survival by dose level. |
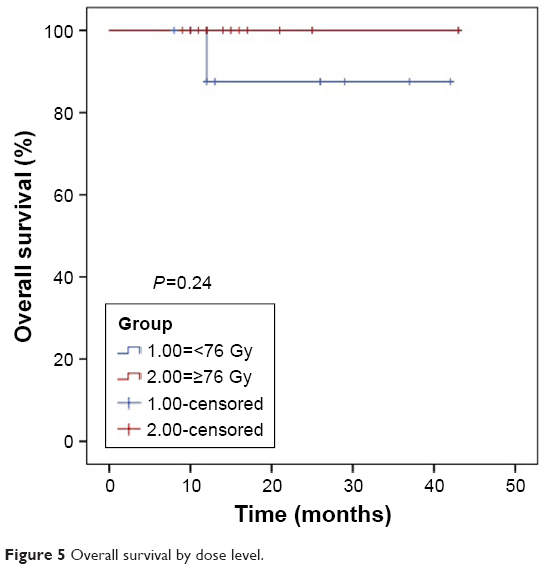 | Figure 5 Overall survival by dose level. |
Discussion
There is evidence that dose escalation improves the BDFS compared with conventional dose in patients with localized prostate cancer.1 Furthermore, the ADT was found to improve both the BDFS and the OS in high-risk prostate cancer patients.2,17 Whether to use dose escalation or standard dose with ADT in high-risk prostate cancer patients had been investigated in multiple randomized studies.5,6 Creak et al demonstrated slight trend for the improvement of BDFS in cancer prostate patients treated by 74 Gy over those treated by 64 Gy.6 However, their study included relatively small number of patients, and they did not analyze the high-risk group of patients. In another Phase III randomized study, Dearnaley et al reported a significant improvement in the progression-free survival (PFS) of dose escalation with 74 Gy compared with 64 Gy.5 Their finding extended to the subgroup of high-risk patients.5 The limitations of their study include the relatively low escalation dose (74 Gy) and all the patients received short course of ADT. In another recent retrospective analysis of combined ADT with dose escalation, Hou et al found improvement of both BDFS and DFS in a cohort of prostate cancer patients treated with dose escalation for total dose of 78 Gy/39 fractions to the prostate and involved seminal vesicles without pelvic irradiation.18 They showed that both short-term and long-term ADT improved the BDFS and PFS in the high-risk group of patients.18 This finding was supported by other studies like the retrospective analysis by Valicenti et al, who reported improved DFS (P=0.050) in high-risk prostate cancer patients with PSA ≥20 ng/mL treated with long-term ADT and cumulative dose of >73.8 Gy.19 Also, Feng et al found a significant improvement in the 5-year cumulative BDFS and DMFS (35% vs 15%, P<0.001) in high-risk prostate cancer patients treated by dose levels 75–79.2 Gy and ADT.20 Similarly, Spanish Phase III randomized study demonstrated the benefit of long-term ADT with dose escalation on BDFS in intermediate- and high-risk prostate cancer patients.21 Stoyanova et al evaluated the relative benefits of ADT with dose escalation and concluded that the benefit of ADT exceeded the benefit from dose escalation up to 80 Gy.22 Also, in a literature review, Roach found that the data that support ADT were more powerful than the data supporting dose escalation.23 In the current study, we tried to evaluate the benefit of dose escalation when combined with ADT versus conventional dose combined with ADT. We considered radiation doses ≥76 Gy as dose escalation and dose levels from 70 to <76 Gy as conventional doses. In most of the previous studies, escalation doses ranged from 74 to 80 Gy.5,18–22 Our study showed no significant differences in the BDFS and DMFS between patients treated with dose <76 and ≥76 Gy including elective pelvic LNs irradiation, combined with ADT. Our results are similar to that reported by Shakespeare in his studies evaluating the potential benefit of dose escalation >74 Gy to prostate and seminal vesicles in combination with ADT for both intermediate- and high-risk prostate cancer patients.24 They did not demonstrate any statistically significant benefit for radiation dose escalation up to 78 Gy.25 Furthermore, Morris et al in a randomized trial reported highly significant (P=0.001) improvement in the BDFS in patients treated by ADT for 12 months with elective pelvic irradiation and boosted by low dose rate brachytherapy to the prostate compared with those boosted by external beam for total radiation dose of 78 Gy to the prostate. Although BF was associated with increased mortality, their results did not show significant difference in the overall survival between the two groups.26
The benefit of dose escalation is limited compared to the benefit from ADT in addition to the increased incidence of late GI and GU toxicity as reported by meta-analysis of randomized trails comparing dose escalation with conventional dose.1 It might be more convenient to combine the long-term ADT with relatively total lower radiation doses like 74–76 Gy in high-risk prostate cancer patients. Especially if the side effects of long-term ADT are reversible and some studies showed protective effect of ADT from the toxicity of radiation therapy, which is partially explained by reducing the size of prostate with subsequently decreasing the dose to both rectum and bladder.27–29 For more clarification about the role of dose escalation in combination with long-term ADT in intermediate- and high-risk prostate cancer patients, further Phase III randomized studies with long-term follow-up are required. The use of dose escalation SIB-IMRT or VMAT with daily CBCT as image guidance will reduce the radiation toxicity to the rectum and bladder.
Our study has many limitations, including the retrospective nature of the study, the relatively small number of patients and the short follow-up period. Also, we did not report the prostate cancer-specific survival which requires long follow-up time.
Conclusion
For intermediate- and high-risk prostate cancer patients receiving long-term ADT, our analysis showed no significant benefit from dose escalation ≥76 up to 80 Gy compared with doses <76 Gy on the BDFS and DMFS. This controversial issue needs to be further investigated in prospective randomized studies with long-term follow-up period to assess the exact role of dose escalation with the long-term ADT in prostate cancer patients.
Disclosure
The authors report no conflicts of interest in this work.
References
Hou Z, Li G, Bai S. High dose versus conventional dose in external beam radiotherapy of prostate cancer: a meta-analysis of long-term follow-up. J Cancer Res Clin Oncol. 2015;141(6):1063–1071. | ||
Schmidt-Hansen M, Hoskin P, Kirkbride P, Hasler E, Bromham N. Hormone and radiotherapy versus hormone or radiotherapy alone for non-metastatic prostate cancer: a systematic review with meta-analyses. Clin Oncol (R Coll Radiol). 2014;26(10):e21–e46. | ||
Widmark A, Klepp O, Solberg A, et al. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open randomised phase III trial. Lancet. 2009;373:301–308. | ||
Daneshmand M, Quek L, Stein J, et al. Prognosis of patients with lymph node positive prostate cancer following radical prostatectomy: long-term results. J Urol. 2004;172(6):2252–2255. | ||
Dearnaley DP, Jovic G, Syndikus I, et al. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: long-term results from the MRC RT01 randomized controlled trial. Lancet Oncol. 2014;15(4):464–473. | ||
Creak A, Hall E, Horwich A, et al. Randomized pilot study of dose escalation using conformal radiotherapy in prostate cancer: long-term follow-up. Br J Cancer. 2013;109(3):651–657. | ||
Schiavina R, Bertaccini A, Franceschelli A, et al. The impact of the extent of lymph-node dissection on biochemical relapse after radical prostatectomy in node-negative patients. Anticancer Res. 2010;30(6):2297–2302. | ||
Morikawa L, Roach M. Pelvic nodal radiotherapy in patients with unfavorable intermediate and high-risk prostate cancer: evidence, rationale, and future directions. Int J Radiat Oncol. 2011;80:6–16. | ||
Roach M, DeSilvio M, Valicenti R, et al. Whole-pelvis, “mini-pelvis,” or prostate-only external beam radiotherapy after neoadjuvant and concurrent hormonal therapy in patients treated in the radiation therapy oncology group 9413 trial. Int J Radiat Oncol Biol Phys. 2006;66(3):647–653. | ||
Pommier P, Chabaud S, Lagrange J, et al. Is there a role for pelvic irradiation in localized prostate adenocarcinoma? Preliminary results of GETUG-01. J Clin Oncol. 2007;25(34):5366–5373. | ||
Roach M. The use of prostate specific antigen, clinical stage and Gleason score to predict pathological stage in men with localized prostate cancer. J Urol. 1993;150:1923–1924. | ||
Muren L, Wasbø E, Helle S, et al. Intensity-modulated radiotherapy of pelvic lymph nodes in locally advanced prostate cancer: planning procedures and early experiences. Int J Radiat Oncol Biol Phys. 2008;71(4):1034–1041. | ||
Goenka A, Magsanoc JM, Pei X, et al. Improved toxicity profile following high-dose post-prostatectomy salvage radiation therapy with intensity-modulated radiation therapy. Eur Urol. 2011;60(6):1142–1148. | ||
Riou O, Fenoglietto P, Laliberté B, et al. Three years of salvage IMRT for prostate cancer: results of the Montpellier Cancer Center. ISRN Urol. 2012;391705. | ||
Fogarty GB, Ng D, Liu G, Haydu LE, Bhandari N. Volumetric modulated arc therapy is superior to conventional intensity-modulated radiotherapy – a comparison among prostate cancer patients treated in an Australian centre. Radiat Oncol. 2011;6(1):108. | ||
Lawton CAF, Michalski J, El-Naqa I, et al. RTOG GU radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2009;74:383–387. | ||
Jones CU, Hunt D, McGowan DG, et al. Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med. 2011;365(2):107–118. | ||
Hou WH, Huang CY, Wang CC, et al. Impact of androgen-deprivation therapy on the outcome of dose-escalation prostate cancer radiotherapy without elective pelvic irradiation. Asian J Androl. 2016;18:1–6. | ||
Valicenti RK, Bae K, Michalski J, et al. Does hormone therapy reduce disease recurrence in prostate cancer patients receiving dose-escalated radiation therapy? An analysis of radiation therapy oncology group 94–06. Int J Radiat Oncol Biol Phys. 2011;79:1323–1329. | ||
Feng FY, Blas K, Olson K, et al. Retrospective evaluation reveals that long-term androgen deprivation therapy improves cause-specific and overall survival in the setting of dose-escalated radiation for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2013;86:64–71. | ||
Zapatero A, Guerrero A, Maldonado X, et al. High-dose radiotherapy with short-term or long-term androgen deprivation in localized prostate cancer (DART01/05 GICOR): a randomized, controlled, phase 3 trial. Lancet Oncol. 2015;16:320–327. | ||
Stoyanova R, Pahlajani NH, Egleston BL, et al. The impact of dose-escalated radiotherapy plus androgen deprivation for prostate cancer using 2 linked nomograms. Cancer. 2013;119(5):1080–1088. | ||
Roach M. Dose escalated external beam radiotherapy versus neoadjuvant androgen deprivation therapy and conventional dose external beam radiotherapy for clinically localized prostate cancer: do we need both? Strahlenther Onkol. 2007;183(2):26–28. | ||
Shakespeare TP. Effect of prostate-specific membrane antigen positron emission tomography on the decision-making of radiation oncologists. Radiat Oncol. 2015;10(1):233–239. | ||
Shakespeare TP, Wilcox S, Aherne N. Can we avoid high levels of dose escalation for high-risk prostate cancer in the setting of androgen deprivation? Onco Targets Ther. 2016;9:2819–2823. | ||
Morris W, Tyldesley S, Rodda S, et al. Androgen suppression combined with elective nodal and dose escalated radiation therapy (the ASCENDE-RT Trial): an analysis of survival endpoints for a randomized trial comparing a low-dose-rate brachytherapy boost to a dose-escalated external beam boost for high-risk and intermediate-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2017;98(2):275–285. | ||
Denham J, Steigler A, Lamb DS, et al. Short-term androgen deprivation and radiotherapy for locally advanced prostate cancer: results from the Trans-Tasman radiation oncology group 96.01 randomized controlled trial. Lancet Oncol. 2005;6(11):841–850. | ||
Zapatero A, García-Vicente F, Sevillano D, et al. Is hormone therapy a protective factor for late hematuria after high-dose radiotherapy in prostate cancer? Urology. 2008;72(5):1130–1134. | ||
Sieber M, Rüffer U, Josting A, Diehl V. Treatment of Hodgkin’s disease: current strategies of the German Hodgkin’s lymphoma study group. Ann Oncol. 1999;10(Suppl 6):23–29. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.