")
Back to Journals » Clinical Interventions in Aging » Volume 18
Clinical Outcome and Safety of Lumboperitoneal Shunt in the Treatment of Non-Obstructive Hydrocephalus
Authors Foo NP, Tun YC, Chang CC, Lin HL, Cheng CH , Chuang HY
Received 23 December 2022
Accepted for publication 4 March 2023
Published 23 March 2023 Volume 2023:18 Pages 477—483
DOI https://doi.org/10.2147/CIA.S401116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Ning-Ping Foo,1,2 Yang Chien Tun,3 Che Chao Chang,4,5 Hung-Lin Lin,3 Cheng-Hsin Cheng,2,4,* Hao-Yu Chuang4,6,*
1Department of Emergency, An Nan Hospital, China Medical University, Tainan, 70965 Taiwan; 2Graduate Institute of Medical Sciences, Chang Jung Christian University, Tainan, 71101 Taiwan; 3Department of Neurosurgery, China Medical University Hospital, Taichung, 40447 Taiwan; 4Department of Neurosurgery, An Nan Hospital, China Medical University, Tainan, 70965 Taiwan; 5Neurophysiology Laboratory, Department of Surgery, National Cheng Kung University Medical Center and Medical School, Tainan, 70101 Taiwan; 6Department of Neurosurgery, China Medical University Beigang Hospital, Beigang, Yunlin County, 65152 Taiwan
*These authors contributed equally to this work
Correspondence: Cheng-Hsin Cheng; Hao-Yu Chuang, Department of Neurosurgery, An-Nan Hospital, China Medical University, No. 66, Sec. 2, Changhe Road, Annan District, Tainan City, Taiwan, Tel +886-6-3553111, Email [email protected]; [email protected]
Objective: This study aimed to evaluate the functional outcomes of lumboperitoneal (LP) shunt for the treatment of non-obstructive hydrocephalus.
Methods: We retrospectively studied the clinical surgical results of 172 adult patients with hydrocephalus who underwent LP shunt surgery between June 2014 and June 2019. Data regarding the following were collected: pre- and postoperative symptom status, third ventricle width changes, Evans index, and postoperative complications. Additionally, the baseline and follow-up Glasgow Coma Scale (GCS) score, Glasgow Outcome Scale (GOS), and Modified Rankin Scale (mRS) scores were investigated. All patients were followed up for ≥ 12 months using clinical interview and braining imaging using computed tomography (CT) scan or magnetic resonance imaging (MRI).
Results: Majority of patients presented with normal pressure hydrocephalus as the etiology of their disease (48.8%), followed by cardiovascular accident (28.5%), trauma (19.7%), and brain tumor (3%). The mean GCS, GOS, and mRS improved postoperatively. The average period from symptomatic onset to surgery was 402 days. The average width of the third ventricle on CT scan or MRI was 11.43 mm preoperatively and 10.8 mm postoperatively (P< 0.001). The Evans index improved from 0.258 to 0.222 after operation. The symptomatic improvement score was 7.0, with a complication rate of 7%.
Conclusion: Significant improvement was observed in the functional score and brain image after LP shunt placement. Moreover, the satisfaction with symptomatic improvement after surgery remains high. LP shunt operation is a viable alternative in the treatment of non-obstructive hydrocephalus due to the low complication rate, fast recovery, and high satisfaction.
Keywords: clinical outcome, complication, lumboperitoneal shunt, non-obstructive hydrocephalus
Introduction
Ventriculoperitoneal (VP) and lumboperitoneal (LP) shunt operations have no differences in clinical outcomes in the treatment of normal pressure hydrocephalus (NPH).1 Compared to VP shunt operation, performing LP shunt operation is easier with a shorter operative time;2 furthermore, it is minimally invasive, which enhances its efficiency in the treatment of NPH. Jia et al reported asuccess rate of 91.40% with LP shunting; only 5.85% of the cases were complicated by shunt tube malfunction, which mainly occurred in the peritoneal tube.3 Furthermore, agreater lethal risk of nerve tissue is observed during VP shunting than during LP shunting due to the penetration of the brain parenchyma when implanting aVP shunt.4 Therefore, Japanese neurosurgeons suggest LP shunting as the first-line treatment for patients diagnosed with idiopathic NPH to prevent brain injury.5,6 However, aprospective study in Japan found higher risks for shunt revisions when LP shunting was performed than with VP shunting (7% vs 1%) in patients with idiopathic NPH.7 Furthermore, previous reports have found increased surgical complications and revision risk when performing LP shunting compared to VP shunting.5,8 To improve the surgical outcomes, it is necessary to evaluate the patient’s suitability for shunt implantation.9 However, LP shunts remain as aviable alternative for NPH treatment due to their minimally invasive nature and low mortality.6,10
Currently, long-term and large cohort studies have established the application and risks of VP shunts.11–14 However, only afew short term clinical reports have been conducted on LP shunts due to their recent development.1,5,6,10 Only afew studies with large cases have been conducted previously.15 In this study, we aimed to better understand the clinical outcomes and risk of LP shunt operation. However, the long-term outcomes of adouble-blind study on LP shunts in patients with NPH remain to be determined.
Methods
We retrospectively studied the surgical outcomes of 172 patients with non-obstructive hydrocephalus treated with an LP shunt between June2014 and June2019. Before shunt operation, every patient will receive the test of lumbar drainage. Patients with the following characteristics were excluded from the study: age <18 years, obstructive hydrocephalus based on CT and MRI findings, and incomplete follow-up period. Shunt catheters with programmable pressure valve were obtained from astrata programmable valve (“Medtronic” PS Medical Strata NSC Lumboperitoneal Valve and Shunt System 44420, Cremona Drive, Goleta, CA 93117, USA) by asingle doctor.
Demographic data were collected, including age, sex, disease etiology, clinical presentation, interval between onset and operation, and admission days. Additionally, pre- and postoperative functional scores were recorded, including the Glasgow Coma Scale (GCS), Glasgow Outcome Scale (GOS), and Modified Rankin Scale (mRS) scores. Preoperative data were documented on the firstday of admission. Postoperative information and imaging (brain CT or MRI) were obtained after 3 months.
For anatomical evaluation, differences between the pre- and postoperative Evans index and width of the third ventricle were evaluated using brain CT or MRI. We designed the symptomatic improvement score (SIS) to better understand differences in symptomatic improvement. This finding was similar to pain scores. The satisfaction of SIS ranged from 0 to 10 according to the patients’ self-assessment or acaretaker’s assessment (0–2: poor, 3–5: satisfactory, 6–8: good, 9–10: excellent). Postoperative complications were monitored during the surgery. The longest period of postoperative complications related to the LP shunt was 120 days.
Statistical Analysis
All data were analyzed using IBM SPSS Statistics software. Mean ± standard deviation were used to describe normal and non-normal data, while number (percentage) was used to describe categorical variables. An independent sample t-test was used to compare pre- and postoperative differences in the Evans index and width of the third ventricle. Statistical significance was set at P<0.001.
Result
From June2014 to June2019, 172 patients with communicating hydrocephalus and LP shunt operations were recorded in our hospital. Baseline characteristics and presenting symptoms of the patients are shown in Table1. The most common etiology of communicating hydrocephalus is NPH (48.8%), followed by cardiovascular accident (CVA) (28.5%). The high incidence of NPH and CVA may be attributed to the relatively high mean patient age. The etiology of trauma (19.7%) and brain tumors (3%) was relatively low. The average period from onset to operation and operation to follow-up was 402 and 1070 days, respectively. The average admissionday was 4.95 days.
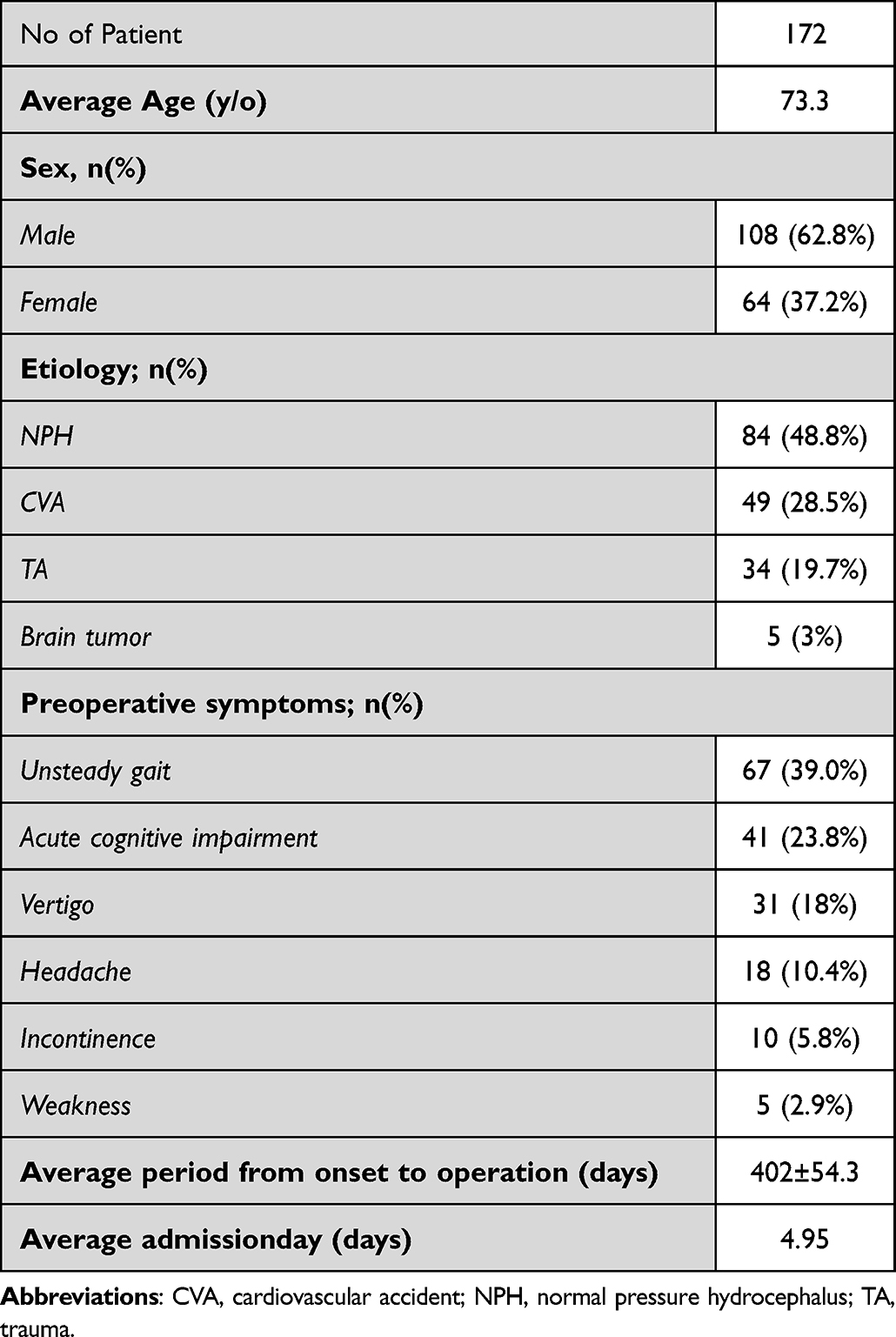 |
Table1 Demographic and Preoperative Characteristics of Patients |
Table2 shows the postoperative data of outcome and complications. Significant difference was found between in the Evans index and width of the third ventricle after LP shunting (P<0.001). Hence, improvement in the width of the third ventricle was noted (from 11.43mm to 10.8mm). The average Evans index was from 0.258 to 0.222 relatively. Additionally, the function outcome of GCS, GOS, and mRS scores were also meaningful compared with preoperative status. The mean SIS was 7. Most patients reported high satisfaction with symptomatic improvement (93%) postoperatively.
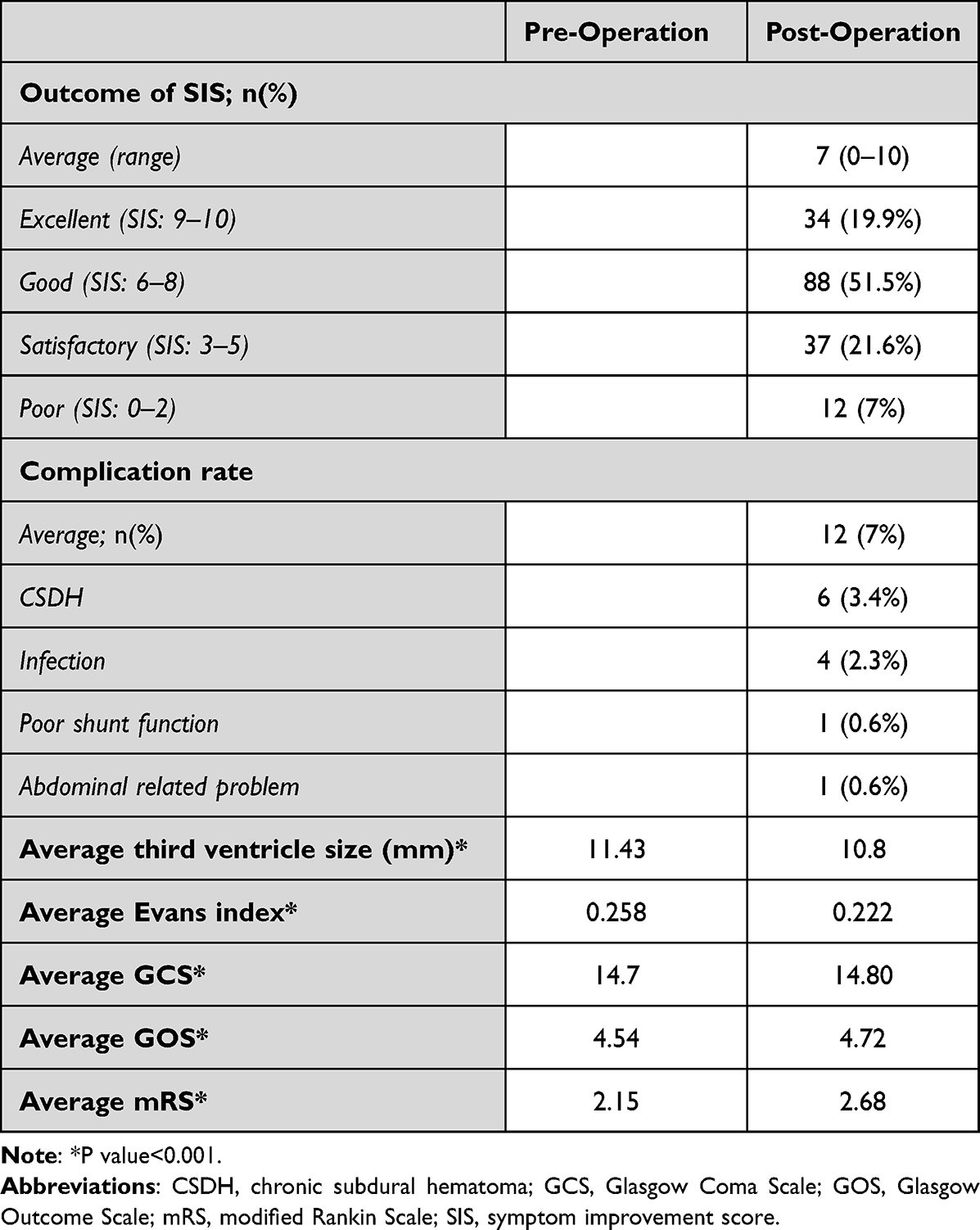 |
Table2 Functional Outcomes |
Twelve (7.0%) complications were observed, which are shown in Table3. Among these 12 patients, six (3.4%) developed chronic subdural hemorrhage (CSDH) due to over-shunting. Among these six who developed CSDH, three patients underwent burr hole drainage, while three underwent operation of the subdural peritoneal shunt. Four patients (2.5%) developed infection of either the wound or the CNS. CNS infection in two patients (1.2%) necessitated shunt removal. One patient with poor wound healing underwent debridement. One patient developed wound infection, which was managed with antibiotic therapy. One patient (0.6%) developed acute hydrocephalus due to poor shunt function 31 days after the shunt operation. Moreover, one LP shunt was removed due to ischemic bowel 120 days after the operation.
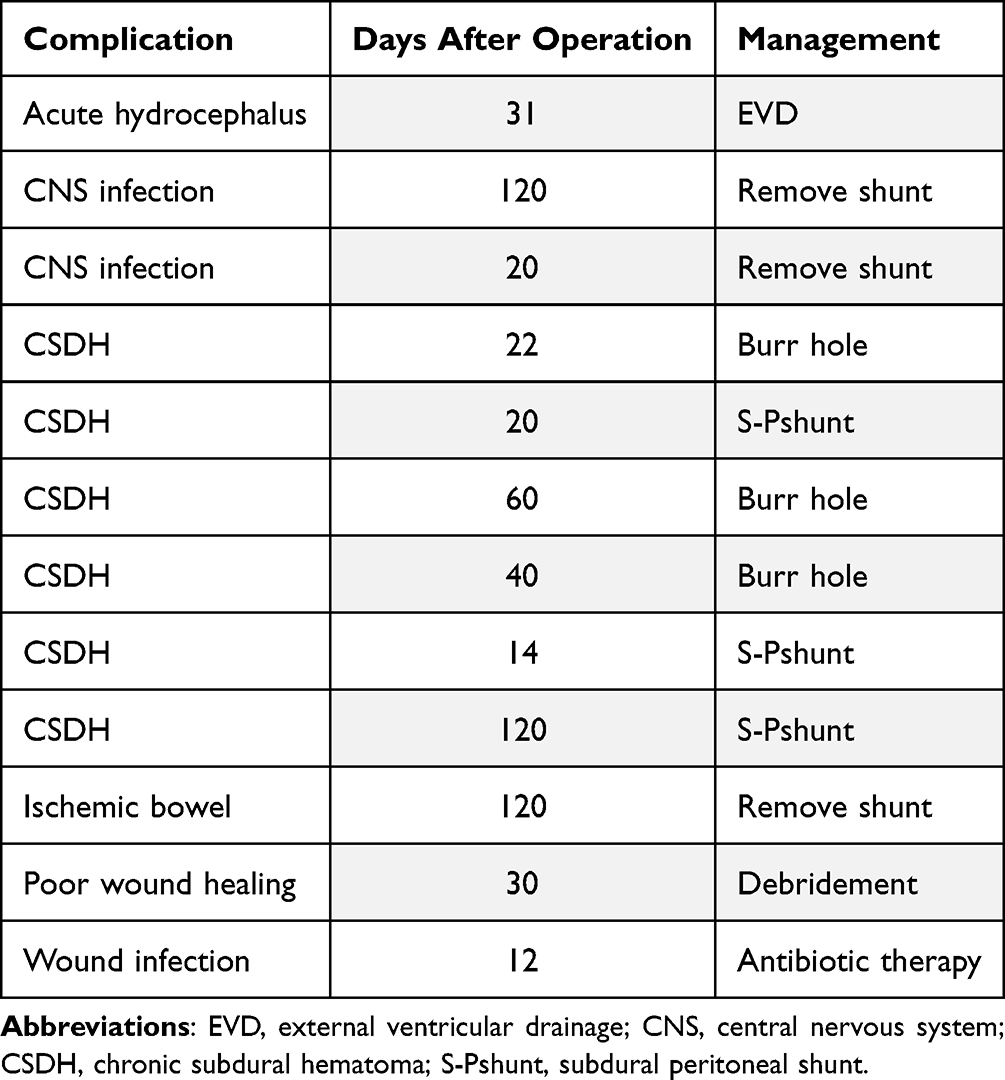 |
Table3 Postoperative Complications |
Discussion
LP and VP shunt operations are the most common surgical procedures in the management of hydrocephalus. Previous studies have found several advantages of LP shunts compared to VP shunts.16,17 However, the lack of aconsensus and standard flow chart have led to controversies regarding the indications and contraindications of LP shunting.17 LP shunts divert the accumulated CSF from the spinal subarachnoid space to the peritoneum; considering this, it is only applicable for non-obstructive hydrocephalus.18 Therefore, patients were diagnosed as obstructive hydrocephalus based on brain CT or MRI were excluded from this trial. In our series, NPH was the most common etiology of hydrocephalus, presenting in 48.8% of patients who received an LP shunt. Brain tumors were the etiology in five patients (3%), confirmed by brain imaging.
The mean SIS was 7, with most patients (93%) showing good satisfaction with symptomatic improvement after LP shunt placement. This is evidence of the effectiveness of LP shunting in the relief of symptoms in the treatment of non-obstructive hydrocephalus. Additionally, functional outcomes of patients were evaluated 3 months postoperatively, using GCS, GOS, and mRS; consequently, significant improvement was observed between these parameters. In our institution, LP shunt was mostly applied in patients with NPH (84%). The average preoperative GCS, GOS, and mRS scores were 14.7, 4.54, and 2.15, respectively, indicating arelatively good preoperative neurologic function. Considering this, the operation of LP shunt was still helpful for initial good cognitive patients under the precise diagnosis. Additionally, pre- and postoperative changes in the Evans index and width of the third ventricle were evaluated. Furthermore, much improvement was observed in the brain images at 3 months postoperatively. The Evans index and width of the third ventricle is aconsiderable parameter for changes of ventricle. Hence, there is alack of study evaluating differences in the ventricle size after LP shunting. Therefore, recommendations regarding the effectiveness of ventricle size change as ameasure of the timing and effectiveness of treatments for hydrocephalus lack evidence.19
The application of the LP shunt is associated with several common complications, including infection, shunt failure, shunt migration, shunt malfunction, tonsillar herniation, overdrainage-induced CSDH, and CSF leakage from the wound.17,20–22 Rare complications include radiculopathy due to catheter irritation, foraminal migration of the shunt, intra-cranial hemorrhage, spinal deformities, subarachnoid hemorrhage, and acute subdural hematoma.22,23 Among these, over-shunting is the major complication following LP shunting, leading to low-pressure conditions.24 In our series, six patients developed CSDH. Among them, three underwent SP shunt conversion and three underwent burr hole drainage. The development of over-shunting in most patients (50%) occurred within 1 month of the operation. There are several ways to address and prevent over-shunting. The use of an anti-siphon device combined with aprogrammable pressure valve has been shown to decrease the risk of over-shunting.25 The anti-siphon design prevents overdrainage while the patient is upright.26 However, over-shunting remained in some surgical reports. In our routine procedure, the highest-pressure setting was used in the programmable valve to decrease CSF drainage. Moreover, the abdominal catheter maintained its original length (84cm). Compared to the 27.5% complication rate reported by Tracy etal,27 we successfully decreased the complication rate of over-shunting to 3.4%. Furthermore, shunt-related deaths were not observed in our study, as opposed to previous studies.16
Shunt failure is another complication observed postoperatively. In our study, only one patient developed shunt failure. Currently, the risk factors for LP shunt failure remain unclear. Ahigh CSF protein level is postulated to play an important role in the development of shunt failure.28 Therefore, some surgeons perform LP shunting only when CSF values are normal. However, astudy on infants revealed no significant relationship between preoperative CSF parameters and shunt failure.29
Previous studies have found a7–85.7% incidence of shunt revision.30 One patient in our study experienced acute headache and dizziness due to acute hydrocephalus approximately 31 days after the LP shunt operation; symptoms were relieved after shunt revision. Because of the design of the LP shunt tube, the diameter of the LP shunt tube is smaller than that of the VP shunt, which may lead to ahigher rate of shunt failure and revision.5
Limitation
Our study has afew limitations. First, bias may occur due to several factors, including the single-center retrospective nature of the study, technique of the operators, devices used, and patient selection. Second, the sample included was relatively small, necessitating alarger cohort study to validate the true value of LP shunts. Third, because SIS is asubjective score, the patient’s baseline consciousness is an important factor for evaluation. Considering that the LP shunt is still not as widely accepted as aVP shunt, alarger study comparing the effectiveness of these two surgical operations is warranted.
Conclusion
In conclusion, LP shunting is aviable alternative in the management of non-obstructive hydrocephalus, regardless of etiology. The minimal invasiveness and prevention of brain penetration is the major idea for LP shunting operation. However, the risk of overshunting and infection should be kept in mind. It still needs more data and studies to prove the true value of LP shunt.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of Tainan Municipal An-Nan Hospital, China Medical University, and informed consent was waived due to the retrospective nature of the study.
Compliance with Ethical Standards
The authors received consent from the patient to participate in the submission.
Acknowledgments
This work was supported by the Tainan Municipal An-Nan Hospital, China Medical University (ANHRF110-40).
Disclosure
The authors report no conflicts of interest. The funders had no role in the organization of the research, in the decision to publish the research data, in the writing of the article content, or interpretation of results, analysis or data collection.
References
1. NakajimaM, MiyajimaM, OginoI, etal. Shunt intervention for possible idiopathic normal pressure hydrocephalus improves patient outcomes: anationwide hospital-based survey in Japan. Front Neurol. 2018;9:421. doi:10.3389/fneur.2018.00421
2. ErU, AkyolC, BavbekM. Delayed intracerebellar hemorrhage secondary to lumboperitoneal shunt insertion. Asian JNeurosurg. 2016;11:447. doi:10.4103/1793-5482.145068
3. JiaL, ZhaoZX, YouC, etal. Minimally-invasive treatment of communicating hydrocephalus using apercutaneous lumboperitoneal shunt. JZhejiang Univ Sci B. 2011;12:293–297. doi:10.1631/jzus.B1000248
4. Barcia-MarinoC, Gonzalez-BonetLG, Salvador-GozalboL, Goig-RevertF, Rodriguez-MenaR. Derivación lumboperitoneal en régimen ambulatorio en el tratamiento de la hidrocefalia crónica del adulto. Estudio y seguimiento de 30 casos [Lumboperitoneal shunt in an outpatient setting for the treatment of chronic hydrocephalus in adults. Astudy and follow-up of 30 cases]. Rev Neurol. 2009;49:300–306. Spanish.
5. MiyajimaM, KazuiH, MoriE, IshikawaM; Sinphoni-Investigators obot. One-year outcome in patients with idiopathic normal-pressure hydrocephalus: comparison of lumboperitoneal shunt to ventriculoperitoneal shunt. JNeurosurg. 2016;125:1483–1492. doi:10.3171/2015.10.JNS151894
6. KazuiH, MiyajimaM, MoriE, IshikawaM, InvestigatorsS. Lumboperitoneal shunt surgery for idiopathic normal pressure hydrocephalus (SINPHONI-2): an open-label randomised trial. Lancet Neurol. 2015;14:585–594. doi:10.1016/S1474-4422(15)00046-0
7. SunT, YouC, MaL, etal. Comparison of ventriculoperitoneal shunt to lumboperitoneal shunt in the treatment of posthemorrhagic hydrocephalus: aprospective, monocentric, non-randomized controlled trial. Medicine. 2020;99:e20528. doi:10.1097/MD.0000000000020528
8. MengerRP, ConnorDE, ThakurJD, etal. Acomparison of lumboperitoneal and ventriculoperitoneal shunting for idiopathic intracranial hypertension: an analysis of economic impact and complications using the Nationwide Inpatient Sample. Neurosurg Focus. 2014;37:E4. doi:10.3171/2014.8.FOCUS14436
9. KarabatsouK, QuigleyG, BuxtonN, FoyP, MallucciC. Lumboperitoneal shunts: are the complications acceptable? Acta Neurochir. 2004;146:1193–1197. doi:10.1007/s00701-004-0392-3
10. NakajimaM, MiyajimaM, OginoI, etal. Use of external lumbar cerebrospinal fluid drainage and lumboperitoneal shunts with Strata NSC valves in idiopathic normal pressure hydrocephalus: a single-center experience. World Neurosurg. 2015;83:387–393. doi:10.1016/j.wneu.2014.08.004
11. GolzL, RuppertFH, MeierU, LemckeJ. Outcome of modern shunt therapy in patients with idiopathic normal pressure hydrocephalus 6 years postoperatively. JNeurosurg. 2014;121:771–775. doi:10.3171/2014.6.JNS131211
12. KoivistoAM, AlafuzoffI, SavolainenS, etal. Poor cognitive outcome in shunt-responsive idiopathic normal pressure hydrocephalus. Neurosurgery. 2013;72:
13. McGirtMJ, WoodworthG, CoonAL, ThomasG, WilliamsMA, RigamontiD. Diagnosis, treatment, and analysis of long-term outcomes in idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57:
14. PujariS, KharkarS, MetellusP, ShuckJ, WilliamsMA, RigamontiD. Normal pressure hydrocephalus: long-term outcome after shunt surgery. JNeurol Neurosurg Psychiatry. 2008;79:1282–1286. doi:10.1136/jnnp.2007.123620
15. LiuJT, SuPH. The efficacy and limitation of lumboperitoneal shunt in normal pressure hydrocephalus. Clin Neurol Neurosurg. 2020;193:105748. doi:10.1016/j.clineuro.2020.105748
16. AokiN. Lumboperitoneal shunt: clinical applications, complications, and comparison with ventriculoperitoneal shunt. Neurosurgery. 1990;26:
17. WangVY, BarbaroNM, LawtonMT, etal. Complications of lumboperitoneal shunts. Neurosurgery. 2007;60:
18. SunT, YuanY, ZhangQ, etal. Establishing apreoperative evaluation system for lumboperitoneal shunt: approach to attenuate the risk of shunt failure. World Neurosurg. 2018;117:e308–e15. doi:10.1016/j.wneu.2018.06.021
19. NikasDC, PostAF, ChoudhriAF, etal. Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. Part10: change in ventricle size as ameasurement of effective treatment of hydrocephalus. JNeurosurg Pediatr. 2014;14(Suppl 1):77–81. doi:10.3171/2014.7.PEDS14330
20. YadavYR, PandeS, RainaVK, SinghM. Lumboperitoneal shunts: review of 409 cases. Neurol India. 2004;52:188–190.
21. YadavYR, PariharV, SinhaM. Lumbar peritoneal shunt. Neurol India. 2010;58:179–184. doi:10.4103/0028-3886.63778
22. ChengCH, LinHL, ChuangHY. Tonsillar herniation as acomplication of lumboperitoneal shunt: case report and literature review. Br JNeurosurg. 2018;1–4. doi:10.1080/02688697.2018.1538481
23. AyvalikF, OzayR, TurkogluE, BalkanMS, SekerciZ. Remote cerebellar hemorrhage following lumboperitoneal shunt insertion: arare case report. Surg J. 2016;2:e139–e42. doi:10.1055/s-0036-1594245
24. SunT, LiX, ZhangQ, ZhouY, GuanJ. Efficacy and safety of lumboperitoneal shunt in the treatment of all-cause communicating hydrocephalus: analysis of risk factors of shunt failure. World Neurosurg. 2019;132:e956–e62. doi:10.1016/j.wneu.2019.06.070
25. NakajimaM, MiyajimaM, AkibaC, etal. Lumboperitoneal shunts for the treatment of idiopathic normal pressure hydrocephalus: acomparison of small-lumen abdominal catheters to gravitational add-on valves in asingle center. Oper Neurosurg. 2018;15:634–642. doi:10.1093/ons/opy044
26. LehmanRM. Complications of lumboperitoneal shunts. Neurosurgery. 2008;63:
27. MaTS, SharmaN, GradyMS. Asimplified pressure adjustment clinical pathway for programmable valves in NPH patients. Clin Neurol Neurosurg. 2017;159:83–86. doi:10.1016/j.clineuro.2017.05.020
28. WhitelawA, EvansD, CarterM, etal. Randomized clinical trial of prevention of hydrocephalus after intraventricular hemorrhage in preterm infants: brain-washing versus tapping fluid. Pediatrics. 2007;119:e1071–8. doi:10.1542/peds.2006-2841
29. FulkersonDH, VachhrajaniS, BohnstedtBN, etal. Analysis of the risk of shunt failure or infection related to cerebrospinal fluid cell count, protein level, and glucose levels in low-birth-weight premature infants with posthemorrhagic hydrocephalus. JNeurosurg Pediatr. 2011;7:147–151. doi:10.3171/2010.11.PEDS10244
30. SunT, YuanY, ZhangQ, etal. One-year outcome of patients with posttraumatic hydrocephalus treated by lumboperitoneal shunt: an observational study from China. Acta Neurochir. 2018;160:2031–2038. doi:10.1007/s00701-018-3654-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.