Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Clinical Meaningfulness of the Composite Endpoint, COPDCompEx, in Defining Exacerbations and Worsening of COPD: A Post Hoc Analysis of 4 Clinical Interventional Studies of COPD
Authors Tal-Singer R ![]() , Vogelmeier CF, Bolton C, Bengtsson T, Peterson S, Sidaway M, Da Silva CA
, Vogelmeier CF, Bolton C, Bengtsson T, Peterson S, Sidaway M, Da Silva CA ![]()
Received 4 March 2026
Accepted for publication 25 June 2026
Published 9 July 2026 Volume 2026:21 603089
DOI https://doi.org/10.2147/COPD.S603089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Ruth Tal-Singer,1,* Claus F Vogelmeier,2,* Clare Bolton,3 Thomas Bengtsson,4 Stefan Peterson,4 Martin Sidaway,5 Carla A Da Silva6,7
1Global Allergy and Airways Patient Platform, Vienna, Austria; 2Department of Medicine, Pulmonary and Critical Care Medicine, University Medical Centre Giessen and Marburg, Marburg, Germany; 3Early R&D, AstraZeneca, Cambridge, UK; 4StatMind Statistical and Mathematical Modelling, Innovation, and Design AB, Lund, Sweden; 5Late Respiratory and Immunology Clinical Development, AstraZeneca, Gothenburg, Sweden; 6Early Respiratory and Immunology Clinical Development, AstraZeneca, Gothenburg, Sweden; 7Digital Health Strategy & Implementation, Evinova, Gothenburg, Sweden
*These authors contributed equally to this work
Correspondence: Carla A Da Silva, Early Respiratory and Immunology Clinical Development, AstraZeneca, Gothenburg, Sweden, Email [email protected]
Purpose: COPDCompEx is a novel composite end point that includes moderate and severe exacerbation events (requiring oral corticosteroid and/or antibiotic use, or hospitalization), as well as acute worsening events (AWEs), defined as deteriorating chronic obstructive pulmonary disease (COPD) symptoms accompanied by a decline in peak expiratory flow (PEF; morning or evening) or an increase in reliever medication use. AWEs are generally self-managed and rarely reported in clinical trials.
Patients and Methods: In this post hoc analysis, patient data were obtained from 4 COPD clinical intervention studies and were pooled and grouped according to the occurrence of COPDCompEx events (exacerbations only, AWEs only, and mixed events). For each group, outcomes evaluated included: PEF, reliever medication use, COPD symptoms (ie, breathlessness, sputum, cough, and sleep), forced expiratory volume in 1 second (FEV1), and St. George’s Respiratory Questionnaire (SGRQ).
Results: All event types impacted PEF and reliever medication use, with AWEs having a greater effect than exacerbations (event-level data). The COPD symptoms were more pronounced for AWEs and mixed events than exacerbations; the return to baseline was slower for mixed events. Additionally, mixed events had a greater impact on FEV1 and SGRQ scores compared to non-COPDCompEx and other COPDCompEx events (patient-level data), indicating a potential impact on lung function and quality of life.
Conclusion: The COPDCompEx composite outcome includes patient-relevant AWEs that represent a clinically meaningful, patient-centric end point. The data highlight the relevance of COPDCompEx as a drug development tool that could improve clinical development in COPD treatments thereby achieving better outcomes for patients.
Keywords: acute worsening event, composite endpoint, patient-centric, pulmonary disease tool
Introduction
Key goals of treatment for chronic obstructive pulmonary disease (COPD) are to reduce the burden of symptoms and to prevent acute exacerbations, with the ultimate aim of improving or maintaining patients’ health status and quality of life (QoL).1 Severe exacerbations are generally defined as acute worsening of COPD symptoms requiring hospitalization or an emergency department visit lasting ≥24 hours; or resulting in death.2 Moderate exacerbations are generally defined as acute worsening of COPD symptoms requiring treatment with oral corticosteroids and/or antibiotics. Due to the post facto nature of these definitions, differences in resource availability, and local standards for hospital visits, there is significant international variability in reporting of acute exacerbation events of COPD (AECOPD).1
Although instruments such as EXAcerbations of Chronic pulmonary disease Tool (EXACT) and EXACT-Patient-Reported Outcomes (EXACT-PRO) currently exist to measure self-reported symptoms associated with COPD, their ability to detect clinically meaningful changes associated with AECOPD is limited.3 Traditionally, the definition of AECOPD does not encompass all events that are relevant to daily functioning and may impact disease progression. The Rome Proposal emerged as a call to action to redefine AECOPD’s definition and severity, aiming to provide a more comprehensive and objective approach than the existing Global Initiative for Chronic Obstructive Lung Disease (GOLD) report. Although it has not yet been widely adopted,4 the Rome Proposal includes objective measurements such as respiratory and heart rates, and pulse oximetry.5 It emphasizes the acute worsening of symptoms due to increased airway inflammation, offering health care professionals a clearer framework for diagnosing and managing COPD exacerbations.
Clinical trials in COPD typically focus on assessing the impact of treatment on AECOPD, which occur infrequently and subsequently require large, extensive trials run over long durations.6,7 The COPD Composite Endpoint for Exacerbations (COPDCompEx) is a clinical-trial measure designed to capture clinically meaningful worsening of COPD by accounting for moderate-to-severe exacerbations, acute worsening events (AWEs), and, in some cases, study discontinuations.8 COPDCompEx was developed to increase the number of clinically relevant events captured in clinical trials, making it useful in early studies that are underpowered to detect differences between treatment groups in AECOPD.8 An AWE is an episode of COPD worsening that may be self-managed and does not always result in additional treatment. AWEs are identified from daily diary data and require concurrent deterioration in more than one component (eg, worsening symptoms with decline in morning or evening peak expiratory flow (PEF) and/or increased reliever medication use) sustained for ≥2 consecutive days, which helps distinguish AWEs from typical day-to-day symptom variability. In instances where PEF is not considered, AWE is defined by the combination of COPD symptoms and increased reliever medication use. These episodes can occur concurrently or independently of exacerbations.8 When used as a clinical end point, COPDCompEx also includes study drop-outs. COPDCompEx has been used in clinical development as a primary or secondary efficacy outcome in Phase 2 studies, because of its ability to predict 12 months of treatment efficacy on AECOPD in only 3 months.8–10
This post hoc analysis evaluated the correlation between different COPDCompEx event subtypes and the progression of COPD over time. These subtypes include exacerbations, AWEs, and mixed exacerbations/AWEs. Exacerbations in COPD are defined as episodes where there is a sudden and significant worsening of respiratory symptoms, surpassing usual daily fluctuations, and can be moderate (managed with outpatient care) or severe (requiring hospitalization). AWEs are characterized by a rapid decline in respiratory function and are self-managed. Mixed exacerbations/AWEs are complex occurrences where the features of both exacerbations and AWEs are present. It was hypothesized that AWEs are meaningful to individuals with COPD and may contribute to poor health outcomes and disease progression. COPDCompEx could thus represent a valuable composite end point or efficacy assessment tool for future clinical and real-world studies.
Materials and Methods
Data Collection
Data were collected from previously described clinical trials, including Exacerbations 003, SUN, PINNACLE-3, and ACCLAIM I and II.6,7,11,12 The Exacerbations 003 and SUN studies evaluated the efficacy of budesonide plus formoterol metered dose inhaler (MDI; 160/4.5 μg and 80/4.5 μg twice daily [BID]) compared with formoterol MDI (4.5 μg BID) and placebo.6,7 The PINNACLE-3 study assessed the long-term safety and tolerability of glycopyrrolate (18 μg BID) and formoterol fumarate (9.6 μg) combination MDI (GFF; 18/9.6 μg BID), and glycopyrrolate (18 μg BID) and formoterol fumarate (9.6 μg BID) MDIs alone compared with open-label tiotropium bromide inhaler as the active control.11 Lastly, ACCLAIM I and II compared the efficacy of aclidinium bromide (200 μg once daily) to placebo.12
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this post hoc analysis. The study used anonymized data from 4 previously completed interventional COPD trials. As these trials were not co-produced with patient or public representatives, no additional patient engagement was undertaken for the present analysis. All studies have been published previously and were conducted in compliance with the Declaration of Helsinki, International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use, Good Clinical Practice guidelines, and the ethics committee at each participating site. The corresponding publications for each study include their respective ethics approval and informed consent statements. All participants or their legal representatives provided written informed consent.6,7,11,12
The participant inclusion criteria were similar across the included trials (Supplemental Table 1).
Definition of COPDCompEx Events
The definition of a COPDCompEx event is shown in Figure 1A. Moderate exacerbations required treatment with oral corticosteroids and/or antibiotics but did not lead to hospitalization. Severe exacerbations were defined as exacerbations that resulted in hospitalization. The definitions of exacerbation have been aligned with those used in the trials included in this study to ensure consistency and accuracy. Discontinuations or drop-outs were excluded from the COPDCompEx definition as data were generally not collected post-withdrawal. A timeline of events occurring within 3 months was used in line with the original publication. As previously described, AWEs were identified using the COPDCompEx tool based on daily diary entries. Because AWEs only do not fulfill the American Thoracic Society/European Respiratory Society criteria for “moderate or severe exacerbation”,13 they are not formally reported as events in clinical trials. To reduce misclassification due to usual day-to-day symptom variation, an AWE required concurrent deterioration in >1 measure (eg, worsening symptoms with reduced PEF and/or increased reliever medication use) sustained for ≥2 consecutive days Where PEF was not captured (PINNACLE-3), an algorithm based on reliever use and symptoms was used to determine the occurrence of AWE.8 Mixed events were defined when an AWE and a treated exacerbation occurred in proximity within the COPDCompEx framework.
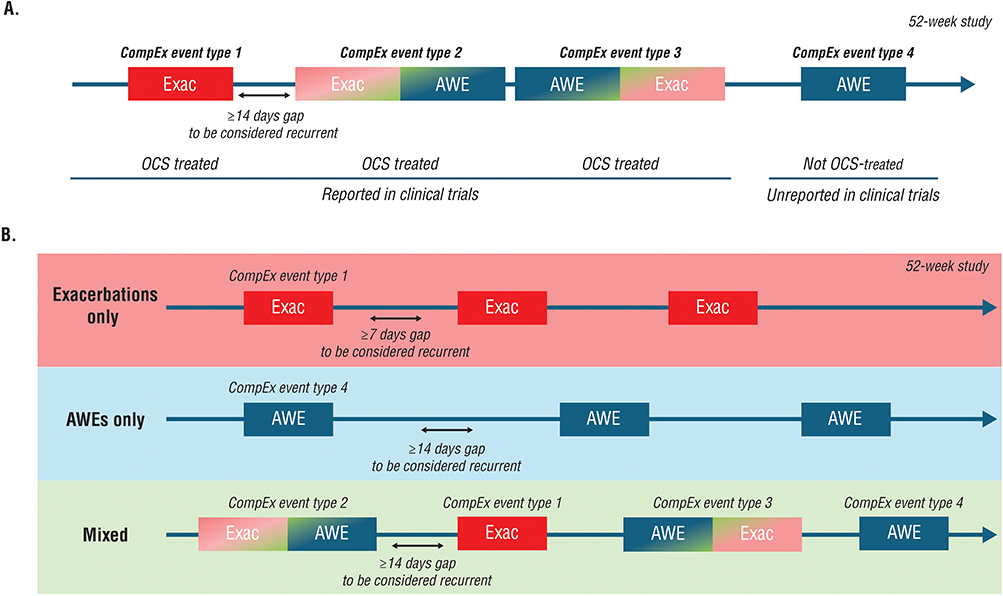 |
Figure 1 (A) Types of COPDCompEx events and (B) categorization of patients based on COPDCompEx events. Abbreviations: AWE, acute worsening event; Exac, exacerbations (moderate or severe); OCS, oral corticosteroid. |
Characterization of the Relationship Between COPDCompEx Event Types and COPD Outcomes (Event-Level Data)
Data from each study for morning and evening PEF, reliever medication use (morning plus evening), and symptoms (breathlessness, cough, sputum, or sleep) were evaluated around the time of occurrence for exacerbations only (treated events), AWEs only (untreated events), or mixed exacerbations/AWEs (treated events) from baseline to 21 days post-event (recovery).
Characterization of the Relationship Between Participants Experiencing Different COPDCompEx Event Types and COPD Outcomes (Patient-Level Data)
Participants were categorized as experiencing a COPDCompEx event and were further subcategorized by COPDCompEx event type including exacerbations, AWEs, or mixed (exacerbations and AWEs in either order; Figure 1B). The relationships between COPDCompEx event types experienced versus forced expiratory volume in 1 second (FEV1) and St. George’s Respiratory Questionnaire (SGRQ) score were evaluated up to 12 months post-randomization. The study assessed comparisons between COPDCompEx and FEV1 or SGRQ score in participants who experienced their first COPDCompEx event within the first 3 months post-randomization. The goal was to determine if the intervention influenced the trajectory of disease progression, as measured by FEV1 or SGRQ.
Statistical Analysis
The frequencies of COPDCompEx subtypes were summarized using descriptive statistics. Profiles of diary card variables surrounding a first COPDCompEx event (exacerbations, AWEs, or mixed events) were described using raw means without imputation. Diary card variables of morning and evening PEF, reliever medication use, breathlessness, sputum, cough, and sleep were compared for each COPDCompEx subtype. Different versions of diary card symptoms were used across the studies; therefore, to assess COPDCompEx, the pooled mean value curves around the events were rescaled to a common score range of 0–4. Changes from baseline in FEV1 and SGRQ score values up to 12 months post-randomization were compared using a mixed model for repeated measures. The model included baseline as covariate, fixed factors for visits, event type, their respective interaction (with the study as a random factor in the pooled analyses), and a Toeplitz covariance matrix. This model also generated the FEV1 and SGRQ score graph data. Due to varying measurement schedules (2 and 3 months across the studies), visit data were moved to the nearest previous visit month. Trajectories of FEV1 and SGRQ score were plotted according to whether a participant experienced a COPDCompEx event during the first 3 months, and by COPDCompEx subtype experienced (exacerbations, AWEs, or mixed).
Sustained recovery was defined as 2 consecutive days within 21 days post-event when diary card variable values met or exceeded the mean value from the second week pre-event. Sustained recovery could also be achieved if the last available value met or exceeded the mean value calculated for the second week pre-event. Participants who did not achieve sustained recovery were censored at Day 21 or at the last day with data, whichever came first. Homogeneity between patient groups of different COPDCompEx event types in sustained recovery up to Day 21 was evaluated by a Cox proportional hazards model and presented using pairwise hazard ratios with 95% confidence intervals.
Results
Participants
The baseline characteristics of the study populations in each clinical trial have been previously published.6,7,11,12 Inclusion criteria are also summarized in Supplemental Table 1.
Relationship Between COPDCompEx Event Types and COPD Outcomes (Event-Level Data)
All categories of events (exacerbations, AWEs, and mixed events) had an impact on the lung function parameters assessed by PEF and reliever medication use. AWEs and mixed events had a greater impact on lung function than treated exacerbations, and the return to baseline post-event was slower for mixed events versus AWEs or exacerbations (Figure 2A and B).
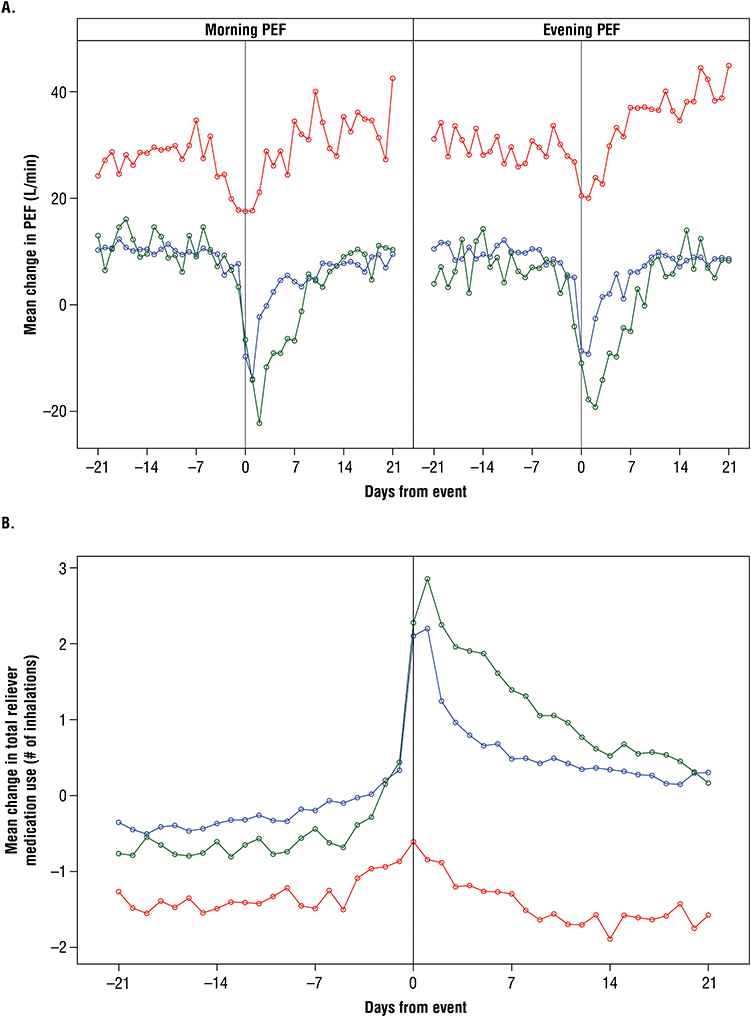 |
Figure 2 Relationship between COPDCompEx events and (A) mean PEF and (B) mean reliever medication use. Abbreviations: AWE, acute worsening event; PEF, peak expiratory flow. Notes: The red line represents participants experiencing exacerbations only; the blue line represents participants experiencing AWE only; and the green line represents participants with mixed events. |
For the analysis of sustained recovery, the cumulative incidence of recovering to mean baseline PEF by 21 days post-event for those with exacerbations was 59% for morning PEF and 59% for evening PEF (Table 1). These proportions were lower for AWEs (40%, P <0.05 for morning PEF and 41%, P <0.05 for evening PEF) and lowest with mixed events (32%, P <0.01 for morning PEF and 35%, P <0.05 for evening PEF). Participants with exacerbations were more likely to achieve sustained recovery at 21 days post-event versus AWEs or mixed events (Figure 3A for morning and evening PEF, respectively). The cumulative incidence of sustained recovery to mean baseline for reliever medication use was highest for exacerbations (88%), followed by AWEs (81%), and mixed events (75%; P <0.001 overall; Table 1). The sustained recovery analysis showed similar results for reliever medication use, with a higher proportion of participants with exacerbations achieving sustained recovery at 21 days post-event versus those with AWEs or mixed events (Figure 3A).
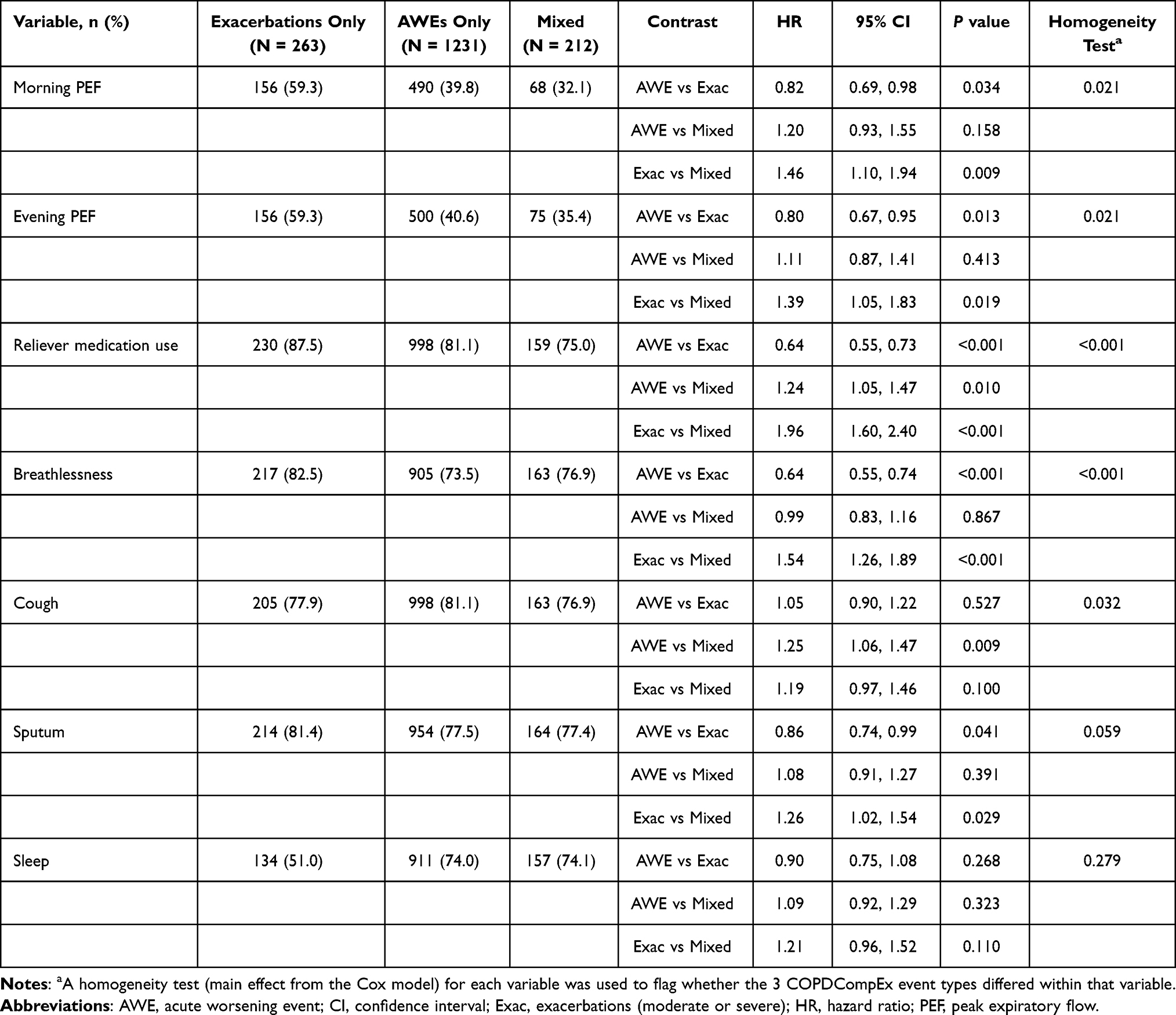 |
Table 1 Rate of Sustained Recovery by 21 Days Post-Event, by COPDCompEx Component Experienced During First 3 Months of Study |
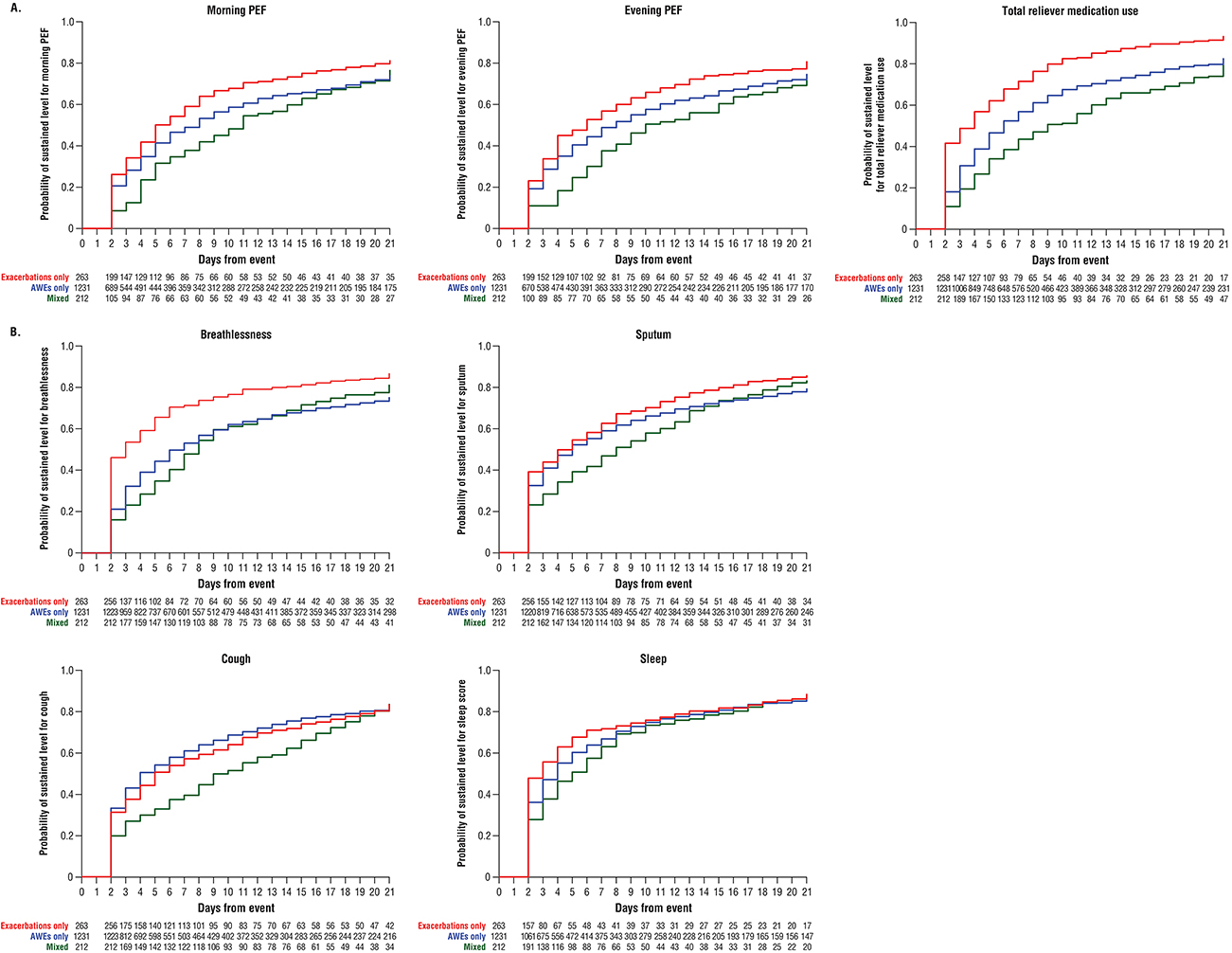 |
Figure 3 Probability of sustained recovery for (A) COPD management metrics and (B) clinical symptoms of COPD. Abbreviations: AWE, acute worsening event; COPD, chronic obstructive pulmonary disease; PEF, peak expiratory flow. Notes: The red line represents participants experiencing exacerbations only; the blue line represents participants experiencing AWE only; and the green line represents participants with mixed events. |
The proportion of participants recovering to mean baseline breathlessness was greater for exacerbations (83%) compared with AWEs (74%, P <0.001), or mixed events (77%, P <0.001; Table 1). The proportion of participants recovering to mean baseline sputum was also greater for exacerbations (81%) compared with AWEs (78%, P <0.05) or mixed events (77%, P <0.05). The sustained recovery analysis indicated that those with exacerbations were more likely to achieve sustained recovery from breathlessness at 21 days post-event versus those with AWEs or mixed events (Figure 3B). Additionally, those with exacerbations were more likely to achieve sustained recovery from sputum at 21 days post-event versus those with AWEs (Figure 3B). However, the proportion of participants recovering to mean baseline cough was not significantly different for exacerbations (78%) compared with AWEs (81%, P = 0.527) or mixed events (77%, P = 0.1; Table 1), and the analysis of participants without sustained recovery of cough did not indicate a difference for those with exacerbations versus AWEs (Figure 3B). Similarly, the proportion of participants recovering to mean baseline sleep was numerically lower, but not significant for exacerbations (51%) compared with AWEs or mixed events (74% each, P = 0.268 and P = 0.110, respectively), and the sustained recovery analysis for sleep did not indicate a difference for those with exacerbations versus AWEs or mixed events (Figure 3B).
The impact of untreated AWEs and of mixed events on COPD symptoms (ie, breathlessness, sputum, cough, or sleep) was greater than the impact of exacerbations on these symptoms (Figures 4A–D).
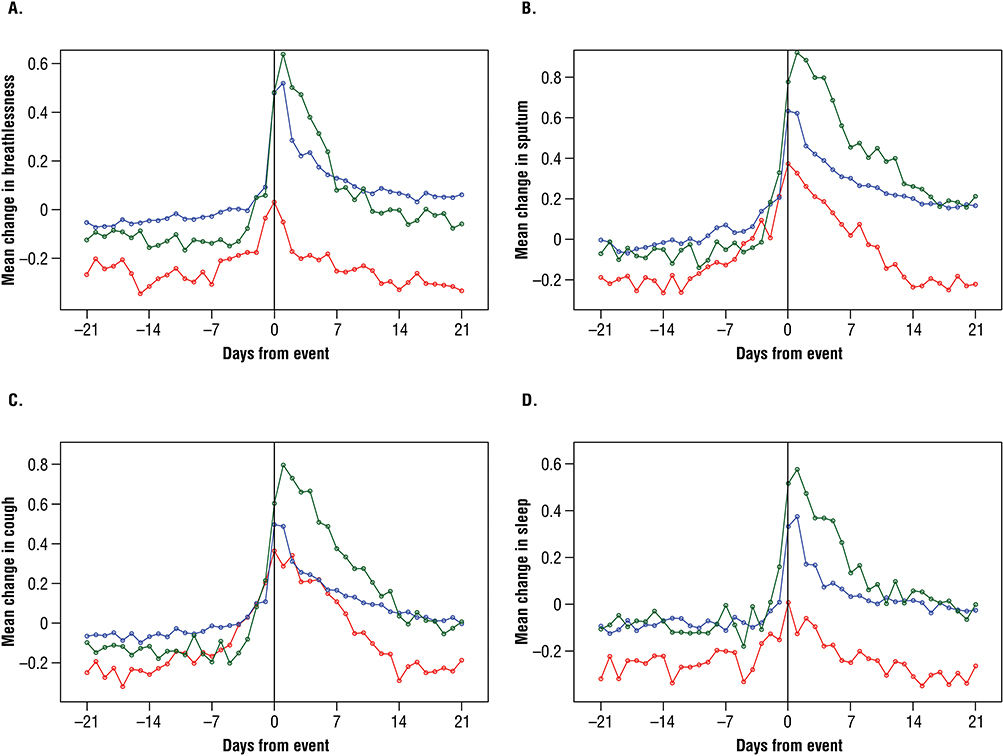 |
Figure 4 Magnitude of change in COPDCompEx component events for COPD symptoms (A) breathlessness, (B) sputum, (C) cough and (D) sleep. Abbreviations: AWE, acute worsening event; COPD, chronic obstructive pulmonary disease. Notes: The red line represents participants experiencing exacerbations only; the blue line represents participants experiencing AWE only; and the green line represents participants with mixed events. |
Relationship Between Participants Experiencing Different COPDCompEx Event Types and COPD Outcomes (Patient-Level Data)
Although participants experiencing AWEs or no COPDCompEx events began with the highest FEV1, their lung function declined over 12 months (Figure 5A). For participants experiencing exacerbations or mixed events, FEV1 started at a lower level compared with other event subtypes and remained relatively stable throughout the 12-month period. Overall, after 12 months, participants experiencing mixed events had the worst FEV1 trajectory outcomes. FEV1 trajectories by COPDCompEx category are shown for each individual trial in Figure 5B.
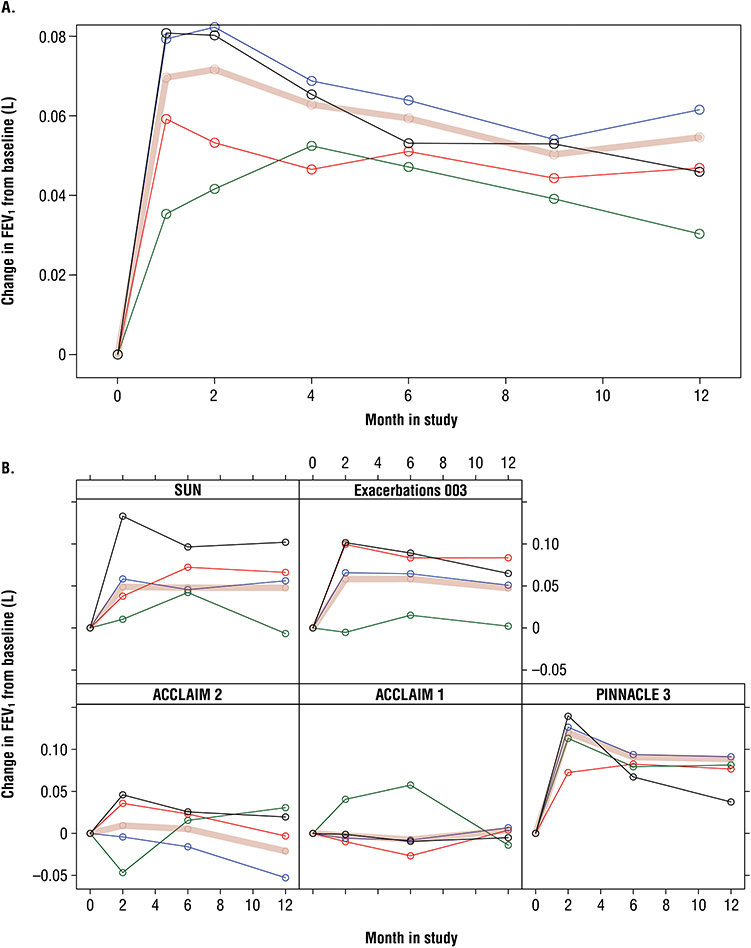 |
Figure 5 Relationship between COPDCompEx events and lung function as measured by FEV1 for (A) overall data and (B) each individual study. Abbreviations: AWE, acute worsening event; FEV1, forced expiratory volume in 1 second. Notes: The red line represents participants experiencing exacerbations only; the blue line represents participants experiencing AWE only; the green line represents participants with mixed events; the pink line represents participants with a CompEx event; and the black line represents participants with no CompEx event. |
Participants experiencing COPDCompEx events during the first 3 months post-randomization had a diminished SGRQ trajectory (higher SGRQ score) indicating a decline in QoL over time (Figure 6A). Participants with mixed events had the poorest SGRQ outcomes compared with participants with no events who had the best SGRQ outcomes. SGRQ trajectory outcomes by COPDCompEx category are shown for each individual trial in Figure 6B.
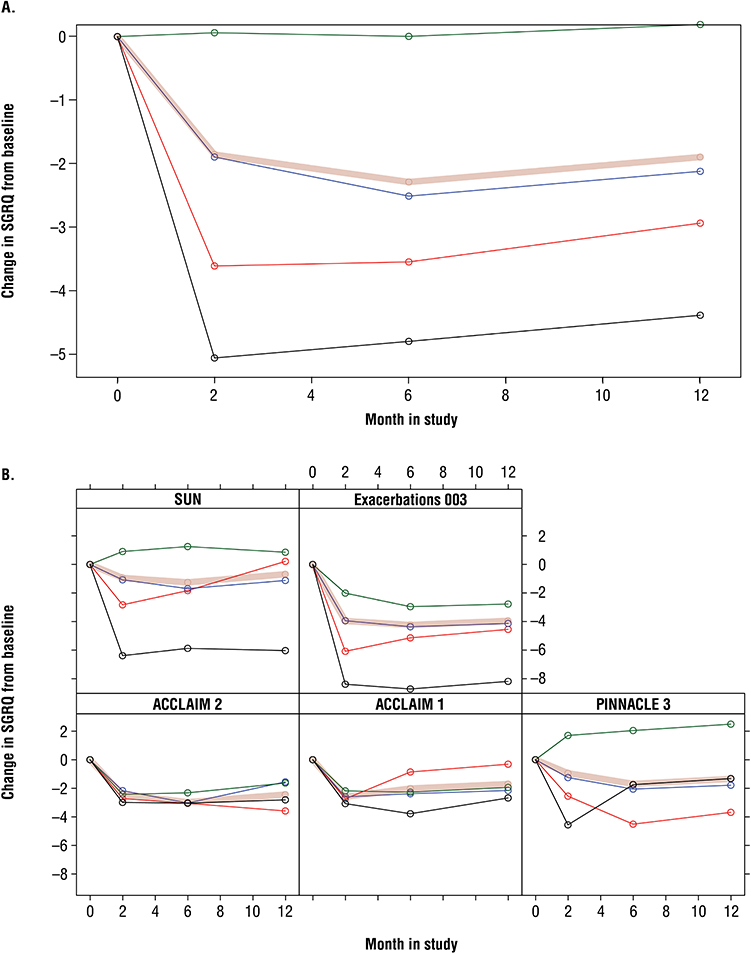 |
Figure 6 Relationship between COPDCompEx events and quality of life as measured by SGRQ scorea for (A) overall data and (B) each individual study. aSGRQ score is based on a scale from 0–100. Abbreviations: AWE, acute worsening event; SGRQ, St. George’s Respiratory Questionnaire. Notes: The red line represents participants experiencing exacerbations only; the blue line represents participants experiencing AWE only; the green line represents participants with mixed events; the pink line represents participants with a CompEx event; and the black line represents participants with no CompEx event. |
Discussion
This post hoc analysis of COPDCompEx events reveals the substantial impact that AWEs (untreated) have on patient outcomes suggesting they may be as clinically meaningful as exacerbations (treated) or mixed events (treated). Unlike exacerbations, which receive medical treatment, AWEs are often self-managed and rarely reported, leading to greater declines in lung function and QoL. Because AWEs are frequently self-managed, they could signal opportunities for earlier clinical intervention and optimization of COPD management. Of note, this analysis was conducted to describe AWEs and their relationship with subsequent outcomes. These findings reinforce the value of COPDCompEx as a tool for capturing patient-relevant worsening events that may be under-represented when trials focus only on treated exacerbations. Future studies are needed to determine whether AWEs are linked to suboptimal maintenance therapy and whether targeted treatment optimization can reduce AWEs or modify longer-term disease trajectories. Consistent with this, AWEs were associated with a deterioration on lung function parameters like PEF and reliever medication use, as well as on COPD symptoms such as breathlessness, sputum production, cough, and sleep disturbances. Notably, lung function following AWEs often fails to return to baseline, indicating the effect of untreated AWEs on COPD progression. The current analysis shows that AWEs contribute to poorer outcomes and disease progression in participants with COPD, particularly in mixed event settings. Mixed events, which involve characteristics of both exacerbations and AWEs, are generally treated with medications and show worse trajectories of FEV1 and QoL compared to other event types. Recovery in lung function and reliever medication use is delayed following mixed events, suggesting they are more sustained than AWEs.
The development of the COPDCompEx composite outcome analyzed diary data from 20 randomized controlled COPD trials.8 COPDCompEx events occurred at a rate 3-fold higher than exacerbations, with consistent treatment effects across PEF, reliever medication use, FEV1, and SGRQ outcomes. The COPDCompEx was designed to predict treatment effects and facilitate smaller and shorter clinical trials, potentially serving as a patient-relevant assessment in clinical practice.
The current definition of exacerbations according to the GOLD report does not consider AWEs,1 despite their impact on disease progression. A large proportion of exacerbations are not reported to health care providers but still have an impact on patients’ health status.14–17 Many patients report taking a “wait and see” approach to symptoms of COPD and only report to a physician if symptoms become unmanageable at home.14,18 This delayed approach, associated with AWEs, may contribute to worse lung function and QoL outcomes. Identification of exacerbations of any severity is important, as prompt treatment can improve outcomes and may delay disease progression.19–21
Patient education can effectively increase recognition and treatment of exacerbations,22–24 and should include AWEs. Resources like the COPD Exacerbation Recognition Tool (CERT), which was developed to support a diverse global patient community, can help educate patients on recognizing AWEs and seeking help when they occur.
This study has several limitations. As with all post hoc analyses, this study did not have prespecified subgroups. Additionally, data collection was dependent on patient use of daily diaries and is thus subject to patient recall bias. Furthermore, participants were classified by COPDCompEx outcomes during the first 3 months post-randomization, meaning that those in the “no CompEx event” group might have experienced exacerbations or AWEs after the 3-month time point. It is important to note that worsening lung function and symptoms around AWE events compared to exacerbations is inherent to their definition. Despite these limitations, this novel analysis provides valuable insights on patient-relevant outcomes based on different event types.
Conclusion
Overall, these findings support the clinical meaningfulness of COPDCompEx as a composite clinical trial end point that captures patient-relevant worsening events, including AWEs that may be under-reported when trials focus only on treated exacerbations. COPDCompEx may therefore be a useful tool for evaluating treatment effects on meaningful worsening events in COPD during drug development. AWEs may also serve as a potential marker of suboptimal COPD control in some patients. Future studies are warranted to determine whether earlier clinical intervention and optimization of COPD management can reduce AWEs and improve longer-term outcomes.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
All studies have been published previously and were conducted in compliance with the Declaration of Helsinki, International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use, Good Clinical Practice guidelines, and the ethics committee at each participating site. The corresponding publications for each study include their respective ethics approval and informed consent statements. All participants or their legal representatives provided written informed consent.
Consent for Publication
As these trials were not co-produced with patient or public representatives, no additional patient engagement was undertaken for the present analysis.
Acknowledgments
Medical writing support was provided by Chan Yoon, PharmD, of Lumanity Communications Inc. under the direction of the authors in accordance with Good Publication Practice guidelines (GPP 2022) and was funded by AstraZeneca (Wilmington, DE, USA). The authors thank Malin Fagerås of BioPharmaceuticals Medical, AstraZeneca (Gothenburg, Sweden) for contributions to the analysis of these data, and Jonathan Marshall of Biopharmaceuticals Medical, AstraZeneca (Cambridge, UK) for contributions to the review of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by AstraZeneca. The researchers retained full independence in the conduct of the analysis, interpretation of the results, and the decision to submit the manuscript for publication. All authors, internal and external, had full access to all data used in the study, including statistical reports and tables, and take responsibility for the integrity of the data and the accuracy of the data analysis.
Disclosure
RTS is a retiree of GSK and reports personal fees from AstraZeneca, Boehringer Ingelheim, COPD Foundation, ENA Respiratory, Global Allergy and Airways Patient Platform, GlobalSkin, GSK, Itay&Beyond, Johnson & Johnson, Renovion, Roche, Samay Health, and Teva. She reports share options from ENA Respiratory. CFV reports financial support from AstraZeneca and reports relationships with A Menarini Pharma GmbH, Aerogen, Boehringer Ingelheim, Chiesi Pharmaceuticals GmbH, CSL Behring, GSK, Grifols Deutschland GmbH Head Office, MedUpdate Europe GmbH, Novartis, Nuvaira, Roche and Sanofi-Aventis Deutschland GmbH that include consulting, advisory and funding grants. TB and SP are employees of StatMind, which received funding from AstraZeneca to complete the statistical analyses. CB, MS, and CDS are employees of, and own stock in, AstraZeneca. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Pocket guide to COPD diagnosis, management and prevention: 2024 report; 2024. Available from: https://goldcopd.org/2024-gold-report/.
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2025. Available from: https://goldcopd.org/wp-content/uploads/2024/11/GOLD-2025-Report-v1.0-12Nov2024_WMV-Draft.pdf.
3. US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Evaluating respiratory symptoms in chronic obstructive pulmonary disease, a patient-reported outcome instrument for the measurement of severity of respiratory symptoms in stable chronic obstructive pulmonary disease: qualification for exploratory use; 2016. Available from: https://www.fda.gov/media/96271/download.
4. Celli BR, Fabbri LM, Aaron SD, et al. An updated definition and severity classification of chronic obstructive pulmonary disease exacerbations: the Rome proposal. Am J Respir Crit Care Med. 2021;204(11):1251–13. doi:10.1164/rccm.202108-1819PP
5. Oh YM. Definition of chronic obstructive pulmonary disease exacerbation: the essentials of the Rome proposal. Tuberc Respir Dis. 2023;86(1):61–62. doi:10.4046/trd.2022.0119
6. Sharafkhaneh A, Southard JG, Goldman M, Uryniak T, Martin UJ. Effect of budesonide/formoterol pMDI on COPD exacerbations: a double-blind, randomized study. Respir Med. 2012;106(2):257–268. doi:10.1016/j.rmed.2011.07.020
7. Rennard SI, Tashkin DP, McElhattan J, et al. Efficacy and tolerability of budesonide/formoterol in one hydrofluoroalkane pressurized metered-dose inhaler in patients with chronic obstructive pulmonary disease: results from a 1-year randomized controlled clinical trial. Drugs. 2009;69(5):549–565. doi:10.2165/00003495-200969050-00004
8. Vogelmeier CF, Fuhlbrigge A, Jauhiainen A, et al. COPDCompEx: a novel composite endpoint for COPD exacerbations to enable faster clinical development. Respir Med. 2020;173:106175. doi:10.1016/j.rmed.2020.106175
9. Singh D, Guller P, Reid F, et al. A phase 2a trial of the IL-33 monoclonal antibody tozorakimab in patients with COPD: FRONTIER-4. Eur Respir J. 2025;66(1):2402231. doi:10.1183/13993003.02231-2024
10. ClinicalTrials.gov. An efficacy and safety study of mitiperstat (AZD4831) (MPO Inhibitor) vs placebo in the treatment of moderate to severe COPD. (CRESCENDO); 2024. Available from: https://clinicaltrials.gov/study/NCT05492877.
11. Hanania NA, Tashkin DP, Kerwin EM, et al. Long-term safety and efficacy of glycopyrrolate/formoterol metered dose inhaler using novel Co-Suspension Delivery Technology in patients with chronic obstructive pulmonary disease. Respir Med. 2017;126:105–115. doi:10.1016/j.rmed.2017.03.015
12. Jones PW, Rennard SI, Agusti A, et al. Efficacy and safety of once-daily aclidinium in chronic obstructive pulmonary disease. Respir Res. 2011;12(1):55. doi:10.1186/1465-9921-12-55
13. Celli BR, MacNee W, ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. doi:10.1183/09031936.04.00014304
14. Barnes N, Calverley PM, Kaplan A, Rabe KF. Chronic obstructive pulmonary disease and exacerbations: patient insights from the global Hidden Depths of COPD survey. BMC Pulm Med. 2013;13:54. doi:10.1186/1471-2466-13-54
15. Jones PW, Lamarca R, Chuecos F, et al. Characterisation and impact of reported and unreported exacerbations: results from ATTAIN. Eur Respir J. 2014;44(5):1156–1165. doi:10.1183/09031936.00038814
16. Xu W, Collet JP, Shapiro S, et al. Negative impacts of unreported COPD exacerbations on health-related quality of life at 1 year. Eur Respir J. 2010;35(5):1022–1030. doi:10.1183/09031936.00079409
17. Langsetmo L, Platt RW, Ernst P, Bourbeau J. Underreporting exacerbation of chronic obstructive pulmonary disease in a longitudinal cohort. Am J Respir Crit Care Med. 2008;177(4):396–401. doi:10.1164/rccm.200708-1290OC
18. Williams V, Hardinge M, Ryan S, Farmer A. Patients’ experience of identifying and managing exacerbations in COPD: a qualitative study. NPJ Prim Care Respir Med. 2014;24:14062. doi:10.1038/npjpcrm.2014.62
19. Wilkinson TMA, Donaldson GC, Hurst JR, Seemungal TA, Wedzicha JA. Early therapy improves outcomes of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;169(12):1298–1303. doi:10.1164/rccm.200310-1443OC
20. Chandra D, Tsai CL, Camargo CA Jr. Acute exacerbations of COPD: delay in presentation and the risk of hospitalization. COPD. 2009;6(2):95–103. doi:10.1080/15412550902751746
21. Singh D, Litewka D, Paramo R, et al. Delaying disease progression in COPD with early initiation of dual bronchodilator or triple inhaled pharmacotherapy (DEPICT): a predictive modelling approach. Adv Ther. 2023;40(10):4282–4297. doi:10.1007/s12325-023-02583-1
22. Song X, Hallensleben C, Shen H, et al. REducing delay through edUcation on eXacerbations for people with chronic lung disease: study protocol of a single-arm pre-post study. J Adv Nurs. 2022;78(8):2656–2663. doi:10.1111/jan.15311
23. Howcroft M, Walters EH, Wood-Baker R, Walters JA. Action plans with brief patient education for exacerbations in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;12(12):CD005074. doi:10.1002/14651858.CD005074.pub4
24. Rice KL, Dewan N, Bloomfield HE, et al. Disease management program for chronic obstructive pulmonary disease: a randomized controlled trial. Am J Respir Crit Care Med. 2010;182(7):890–896. doi:10.1164/rccm.200910-1579OC
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.