Back to Journals » Infection and Drug Resistance » Volume 15
Clinical Laboratory Features of Microbes That Cause Neonatal Sepsis: An 8-Year Retrospective Study
Authors Jin Z ![]() , Wang Z, Li J, Yi L, Liu N, Luo L
, Wang Z, Li J, Yi L, Liu N, Luo L
Received 19 March 2022
Accepted for publication 3 June 2022
Published 9 June 2022 Volume 2022:15 Pages 2983—2993
DOI https://doi.org/10.2147/IDR.S367068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Zhengjiang Jin,1,* Zhenhui Wang,1,* Jinchun Li,2 Lu Yi,1 Nian Liu,1 Lan Luo3
1Department of Clinical Laboratory, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China; 2Department of Neonatology, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China; 3Department of Child Health, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lan Luo, Department of Child Health, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China, Email [email protected]
Purpose: To determine the distribution and antibiotic resistance patterns among pathogens that cause neonatal sepsis (NS) and to assess trends in antibiotic resistance.
Patients and methods: A total of 864 patients with sepsis admitted to a neonatal intensive care unit (NICU) between 2014 and 2021 were enrolled. Data on neonate age and sex, pathogenic microbes, and antimicrobial susceptibility were collected. Univariate and linear regression analyses were performed to determine the differences and trends in antibiotic resistance rates.
Results: The overall incidence rate of NS was 4.59 cases per 1000 live births. Of these cases, 255 (29.5%) were early-onset neonatal sepsis (EONS) and 609 (70.5%) were late-onset neonatal sepsis (LONS). A total of 670 (70.5%) gram-positive cocci and 171 (19.8%) gram-negative bacilli were identified. Among the 552 coagulase-negative Staphylococcus (CoNS) strains, the rate of oxacillin resistance was 70.6%, but no strains were resistant to linezolid, vancomycin or tigecycline. Among the antibiotic resistance patterns of the top three gram-negative pathogens, K. pneumoniae showed the highest rates of resistance, with resistance rates of 37.9% and 39.4% to ertapenem and imipenem, respectively, while E. coli and Enterobacter cloacae showed high levels of susceptibility to both. With regard to the trends in resistance among important pathogens, the rates of resistance to rifampicin, ciprofloxacin, levofloxacin, moxifloxacin and clindamycin by Staphylococcus epidermidis significantly decreased (p< 0.05) during the study period. E. coli strains exhibited a significant increase in ceftriaxone resistance during the study period (p< 0.05).
Conclusion: CoNS was the main microbe that caused NS, followed by E. coli. The bacterial isolates showed varying levels of resistance to the antimicrobial drugs tested. Thus, periodic surveillance in hospital settings to monitor changes in pathogens and antibiotic resistance is important.
Keywords: neonatal sepsis, NICU, microorganisms, antibiotic resistance
Introduction
Neonatal sepsis (NS) generally refers to infectious diseases caused by bacterial, fungal, or viral infections that occur in infants within 28 days of birth.1,2 In the early stage of the disease, typical clinical manifestations are often absent, but progression is rapid, and the outcomes are unfavorable. Therefore, NS is considered a leading cause of neonatal mortality, resulting in 15% of neonatal deaths worldwide and is a matter of great concern, especially in developing countries, where it accounts for approximately 30% to 50% of neonatal mortality.3,4
NS is divided into early-onset sepsis and late-onset sepsis according to the age of onset and time of sepsis onset. Early-onset neonatal sepsis (EONS) is defined as signs and symptoms of sepsis within the first 72 h after birth, whereas late-onset neonatal sepsis (LONS) occurs after this period but before 90 days after birth.1,5 EONS is mainly caused by bacterial pathogens transmitted vertically from mother to child before or during delivery, while LONS may be caused by pathogens acquired vertically or horizontally. EONS is a common and serious problem in neonates, especially preterm infants. However, the incidence rate and spectrum of pathogens that cause NS vary from country to country. In developed countries,6–9 group B Streptococcus (GBS) remains the leading cause of NS, but efforts regarding the administration of intrapartum antimicrobial prophylaxis have significantly reduced the incidence of NS, especially EONS, due to GBS. In the United States, intrapartum antibiotic prophylaxis (IPAP) involving ampicillin administration has been carried out since 1996 to prevent the vertical transmission of GBS, a risk factor for EONS. However,6 in recent years, many studies have reported an increase in EONS caused by E. coli, which is associated with high fatality rates, especially in preterm infants and those with very low birth weights. Developing countries exhibit significant differences in NS from developed countries,10,11 although the data supporting those differences are limited data. The differences, including bacterial pathogen and antibiotic resistance profiles, may vary temporally and geographically, which can influence local prevention policies and clinical management.
China is the largest developing country worldwide, covering a vast area in which the prevalence and distribution of pathogens vary widely. Therefore, it is very important to identify the common pathogens and related antibiotic resistance in individual hospitals.12–14 Furthermore, dynamic monitoring of the local epidemiology of NS is critical to detect any changes in infection patterns and drug susceptibility.
In this retrospective study, we collected clinical laboratory data from neonates with bacterial sepsis confirmed by blood culture in the Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, which is the main healthcare center for women and children in Central China and is located in Wuhan City. We analyzed the pathogenic microbe distribution and the antibiotic resistance patterns of major NS-inducing isolates in this clinical setting, with the aim of providing better guidance for the empirical antimicrobial treatment of NS in the future.
Methods
Study Design and Period
This study was carried out in our clinical setting (the Maternal and Child Health Hospital), which has a 200-bed neonatal intensive care unit (NICU) and, on average, cares for 6000 critically ill neonates each year. The medical records of neonates admitted to the NICU with clinical features of sepsis and who had a positive blood culture during an 8-year period (January 2014 to December 2021) were retrospectively reviewed. This study was approved by the Ethics Committee of the Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, and was conducted in accordance with the Declaration of Helsinki. The need to obtain individual informed consent was waived because this study used existing data collected during the course of routine diagnostic procedures for sepsis and did not pose any additional risks to the patients. The patient records and information were anonymized and deidentified prior to analysis.
Study Participants
In this study, NS was defined as one or more blood cultures obtained during 0–28 days after birth that grew recognized pathogenic bacteria or fungi as well as a clinical diagnosis of sepsis. Data from NS patients with positive blood culture results who were diagnosed during the study period and who had undergone antibiotic susceptibility tests were included in this study. The microorganisms that caused NS isolated from blood cultures were defined as pathogenic microbes. However, samples with only one blood culture positive for CoNS, micrococci, diphtheroids, Corynebacterium or Bacillus as well as those with low C-reactive protein (CRP) concentrations (< 10 mg/L), for which repeated cultures showed no growth, were considered to have been contaminated and were excluded. The isolation of multiple organisms from the same culture led to the exclusion of that sample due to suspected contamination. The date of sepsis onset was defined as the date of collection of the first blood sample containing a pathogenic strain. EONS was defined as an infection occurring less than 72 h after birth, whereas cases thereafter (3–28 days after birth) were classified as LONS.7,9 For all included cases, the following data were collected: age and sex of the neonate, pathogenic bacteria identified, and drug susceptibility of the isolate that caused NS (only the first strain was analyzed).
Culture and Identification
Microbial identification and culture were conducted according to routine diagnostic standard operating procedures used in the clinical laboratory of this study hospital: 1–3 mL of blood was collected from neonates with suspected cases of sepsis, and this sample was cultured using an automated BacT/ALERT 3D system or BD BACTEC™ system. Incubation was continued until positive results were observed or for up to 5 days. Positive cultures were subcultured and identified to the species level by Bruker matrix-assisted laser desorption ionization time of flight (MALDI-TOF) mass spectrometry (Bruker Daltonik GmbH, Leipzig, Germany).
Antimicrobial Susceptibility Testing
Positive cultures were subcultured. Bacterial isolates were tested for susceptibility to antibiotics using the VITEK 2 Compact (BioMérieux) or manual Kirby-Bauer disc diffusion method, and yeast-like fungi were tested with ATB FUNGUS3 for susceptibility to antibiotics according to the interpretive criteria established by the Clinical Laboratory Standards Institute (CLSI, USA).
Statistical Analyses
Data were first entered into Excel and then imported into and analyzed with SPSS 21.0. Univariate analyses of dichotomous data were performed with the χ2 test or Fisher’s exact test.15,16 The changes in trends in antimicrobial resistance were evaluated by linear regression. A P value < 0.05 was considered statistically significant. WHONET 5.6 was used to analyze the antimicrobial resistance rates and resistance patterns. The incidence of NS per 1000 live births (LBs) was calculated as the total number of cases diagnosed with culture-proven sepsis (according to the definition in this study) divided by the total number of infants born in the study hospital during the study period, multiplied by 1000.17
Results
Study Participants
A total of 188,070 children were born in this hospital from January 2014 to December 2021, with an average of 23,500 children born each year; thus, this hospital ranked first among all clinical settings in Hubei Province. Of these neonates, 49,094 were hospitalized for various reasons within 28 days of birth, and 46,603 had blood cultures after admission, of which 1312 had a positive blood culture. Among the neonates with a positive blood culture, 62 were excluded due to incomplete clinical data, and 379 with cases of CoNS infections as well as 8 with cases of Micrococcus and Bacillus infections with CRP levels <10 mg/L were also excluded. The remaining 864 neonates with cases of true infections with complete data, including 255 with EONS and 609 with LONS, were included. Only the first blood culture-positive true infection pathogen data were analyzed for each NS case, producing a total of 864 isolates (Figure 1). The overall incidence rate of NS was 4.59 cases per 1000 LBs (864/188,070). The incidence of EONS was 1.36 cases per 1000 LBs (255/188,070) and that of LONS was 3.24 cases per 1000 LBs (609/118,070).
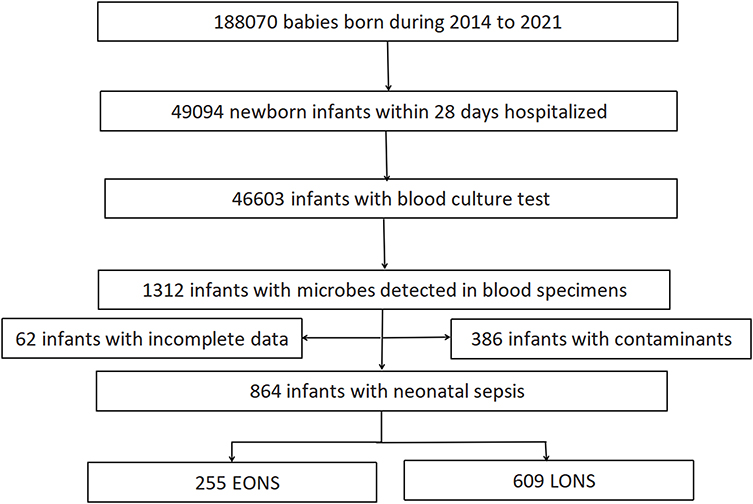 |
Figure 1 The inclusion and exclusion of cases in this study. |
Distribution of Microorganisms
The characteristics of the study participants and the microorganism distribution in this study are listed in Table 1. Among the 864 cases included in this study, the mean (± standard deviation; SD) age of newborns was 9.24 (7.65%) days; of these neonates, 516 were boys (59.7%) and 348 (40.3%) were girls. There were 255 EONS cases (29.5%) and 609 LONS cases (70.5%).
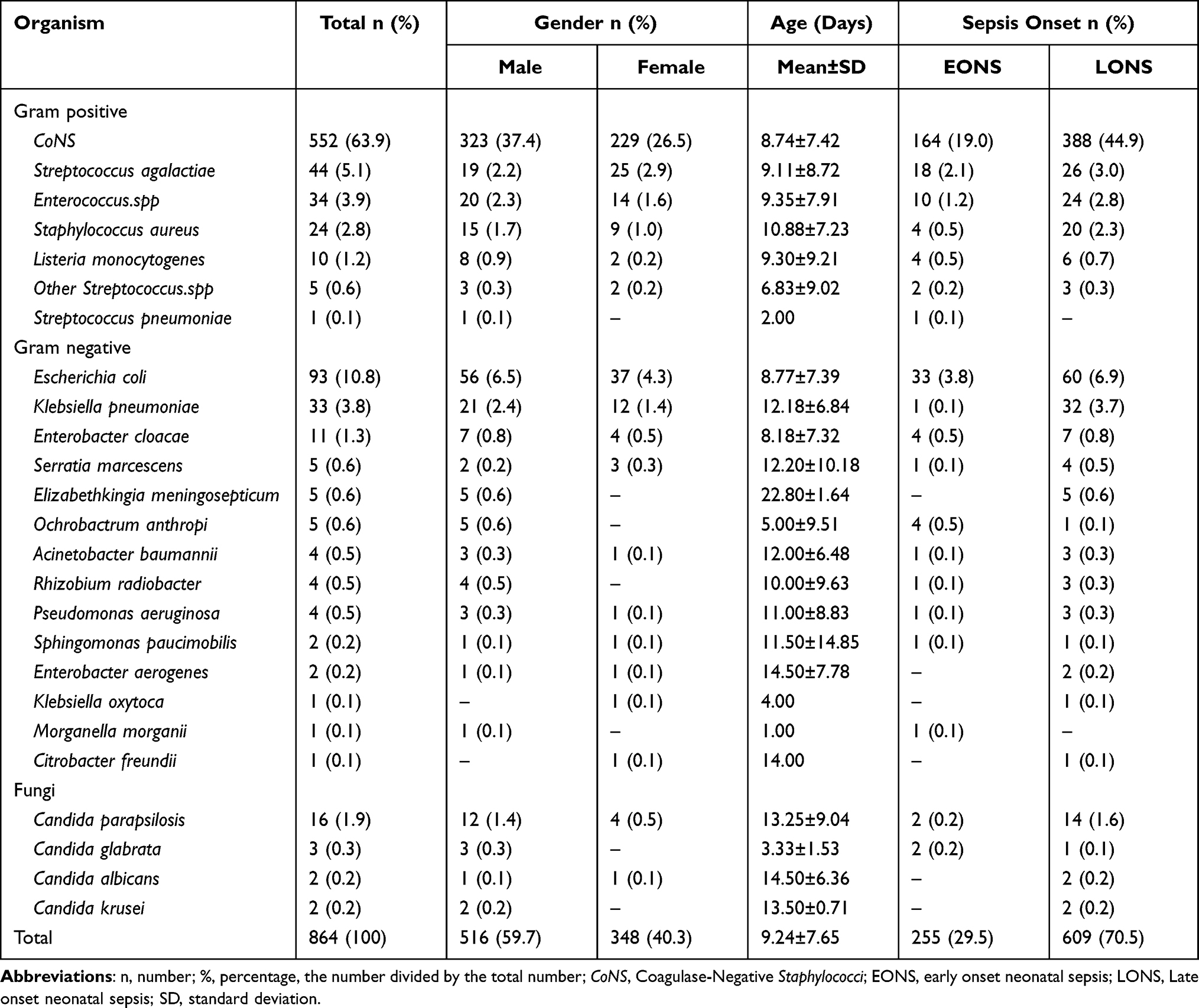 |
Table 1 Distribution of Organisms Isolated from Neonatal Sepsis Patients According to Sepsis Onset, Gender, and Age of the Newborns |
Of the 864 strains isolated from newborns with sepsis, there were 670 (70.5%) strains of gram-positive cocci, including 552 (63.9%) strains of CoNS (400 Staphylococcus epidermidis strains, 54S. haemolyticus strains, 43S. hominis stains, 29S. warneri strains, and 26 other CoNS strains), 44 (5.1%) strains of Streptococcus agalactiae, 34 strains (3.9%) of Enterococcus spp., 24 (2.8%) strains of Staphylococcus aureus, 10 (1.2%) strains of Listeria monocytogenes, 5 (0.6%) strains of other β-hemolytic Streptococcus, and 1 (0.1%) strain of Streptococcus pneumoniae. Among the gram-positive coccus infection cases, there were no significant differences based on sex or age of sepsis onset (p>0.05).
There were 171 (19.8%) gram-negative bacilli; the top three pathogens were E. coli (93, 10.8%), K. pneumoniae (33, 3.8%), and Enterobacter cloacae (11, 1.3%), all of which are Enterobacterales. There were 4 strains each of Acinetobacter baumannii and Pseudomonas aeruginosa (0.5%), and there were 5 strains (0.6%) that were rare opportunistic pathogens, such as Elizabethkingia meningosepticum and Ochrobactrum anthropi. Among the cases of infection with gram-positive cocci, there were no significant differences based on sex or age of sepsis onset (p>0.05).
The isolates from neonates with cases of sepsis induced by infection with fungus were dominated by Candida, of which Candida parapsilosis was the most abundant, accounting for 16 cases (1.9%). The cases of neonatal fungal sepsis affected significantly more boys (2.1%) than girls (0.6%) (p<0.05), but there was no significant difference in age of sepsis onset (p>0.05).
Antibiotic Resistance Patterns and Trends in Gram-Positive Bacteria
To examine antibiotic susceptibility, we analyzed the antibiotic susceptibility patterns of the predominant pathogens that caused NS, including the top four gram-positive pathogens, top three gram-negative bacilli and Candida. The trends in the antibiotic resistance rates were analyzed for Staphylococcus epidermidis and E. coli from 2014 to 2021.
The antibiotic resistance patterns of the predominant gram-positive bacteria between 2014 and 2021 are presented in Figure 2. Among the CoNS strains, the rate of antibiotic resistance to oxacillin was 70.6%, and those to ciprofloxacin and levofloxacin were 31.1% and 33.3%, respectively, while that to moxifloxacin was only 9.8%. The rates of antibiotic resistance to clindamycin and erythromycin were greater than 50%. No CoNS strains resistant to linezolid, vancomycin or tigecycline were found in this study (Figure 2A). Streptococcus agalactiae was highly sensitive to penicillin G, and no resistant strains were found in this study, nor was any resistance to linezolid, vancomycin or tigecycline observed (Figure 2B). Among the Enterococcus spp., the rates of resistance to penicillin G and ampicillin were 65.5% and 73.1%, respectively, which both exceeded 60%, and the rates of resistance to quinolones such as ciprofloxacin, levofloxacin, and moxifloxacin were all greater than 50%. Vancomycin-resistant enterococci (VRE) were not detected in this study (Figure 2C). Among the Staphylococcus aureus isolates, methicillin-resistant S. aureus (MRSA) accounted for 29.2%. S. aureus exhibited the lowest rate of resistance to quinolones, and no strains resistant to linezolid or vancomycin were found (Figure 2D).
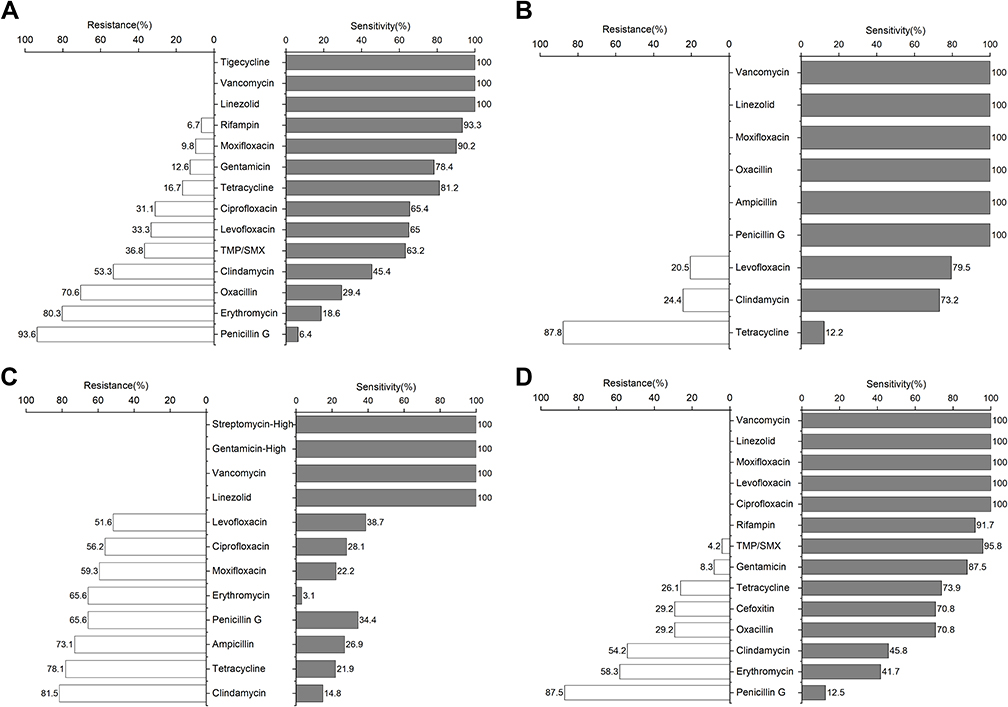 |
Figure 2 Antibiotic resistance patterns of predominant gram-positive bacterial isolates from neonatal sepsis patients. (A) Coagulase-negative Staphylococci (CoNS), (B) Streptococcus agalactiae, (C) Enterococcus spp., (D) Staphylococcus aureus. Abbreviation: TMP/SMX, Trimethoprim/Sulfamethoxazole. |
Over these 8 years, the rates of S. epidermidis resistance to rifampicin, ciprofloxacin, levofloxacin, moxifloxacin and clindamycin showed significant decreases (p<0.05). There was no significant change in the trend in resistance to the other drugs tested (p>0.05) (Figure 3).
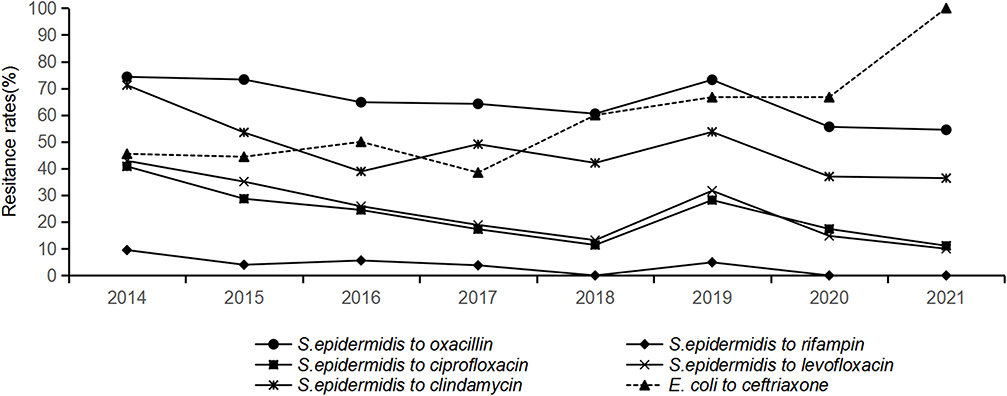 |
Figure 3 Antibiotic resistance trends of Staphylococcus epidermidis and E. coli isolates from neonatal sepsis patients during 2014–2021. |
Antibiotic Resistance Patterns and Trends in Gram-Negative Bacteria
The antibiotic resistance patterns of predominant gram-negative bacteria between 2014 and 2021 are presented in Figure 4. Among the top three pathogens, the rate of resistance to ampicillin was the highest, with that of Enterobacter cloacae at 100%, followed by that of K. pneumoniae at 88.9% and that of E. coli at 88.7% (Figure 4A, and B). The rates of antibiotic resistance to penicillin combination inhibitors showed different patterns. The rates of resistance to ampicillin/sulbactam were higher than 50%, while those to piperacillin/tazobactam were lower; the highest rate in K. pneumoniae was 15.2%, and that in E. coli was only 2.2%. The rates of resistance to third- and fourth-generation cephalosporins differed. In E. coli, the rate of resistance to ceftriaxone was as high as 48.9% and that to cefepime was 14.0%. The drug resistance of K. pneumoniae was more serious, with rates of 67.7% and 62.5% for ceftriaxone and cefepime, respectively. The rate of Enterobacter cloacae resistance to ceftriaxone was 70% but that to cefepime was only 10% (Figure 4C). Among the carbapenem-resistant isolates, K. pneumoniae had the highest rates of resistance. The rates of K. pneumoniae resistance to ertapenem and imipenem were 37.9% and 39.4%, respectively, while E. coli and Enterobacter cloacae both showed high susceptibility. K. pneumoniae and Enterobacter cloacae showed extremely high sensitivity to quinolone antibiotics. No strains resistant to ciprofloxacin or levofloxacin were found in this study, while the rates of E. coli resistance to these antibiotics were 36.9% and 37.4%, respectively. For the other antibiotics tested, the three dominant pathogens showed varying resistance rates.
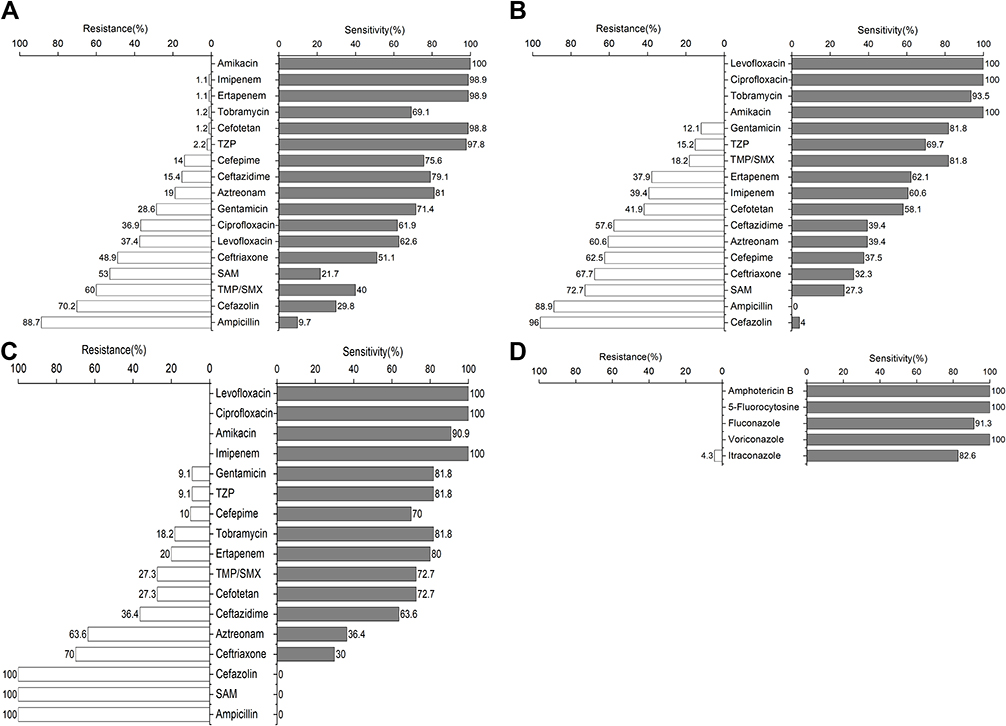 |
Figure 4 Antimicrobial resistance patterns of predominant gram-negative bacterial and Candida isolates from neonatal sepsis patients. (A) E. coli, (B) K. pneumoniae, (C) Enterobacter cloacae, (D) Candida. Abbreviations: TZP, Piperacillin/Tazobactam, SAM, Ampicillin/Sulbactam, TMP/SMX, Trimethoprim/Sulfamethoxazole. |
Based on the trend of E. coli resistance over these 8 years, ceftriaxone merits additional attention, as there was a significant increase in resistance to this drug during the study period (p<0.05). However, on a positive note, there was no significant change in the trend in resistance to the other drugs tested (p>0.05) (Figure 3).
Antibiotic Resistance Patterns in Fungi
The fungi that caused NS were mainly Candida spp. According to the antibiotic resistance patterns, susceptibility to amphotericin B, 5-flucytosine and voriconazole was very low, and no drug-resistant strains were found in this study. The rate of resistance to itraconazole was 4.3%, while the rates of intermediate resistance to fluconazole and itraconazole were 13% and 8.7%, respectively (Figure 4D).
Discussion
NS is one of the main causes of neonatal death due to its insidious onset and rapid progression; thus, it has attracted increasing attention.18 NS is related to various factors,19,20 such as local economic development and the quality of health care. Therefore, the incidence of NS varies worldwide. Our findings differ from those in a hospital in South China, as reported by Kankan Gao et al17 but the difference is not significant. These findings are also contrary to results in a different country, according to Song et al21 whose data showed that the incidence rates of EONS and LONS were 3.8 and 48.8 cases per 1000 LBs, respectively.
We found more LONS cases than EONS cases (although this difference was not statistically significant), similar to the findings in other studies.6,14 This difference may result from the prophylactic use of antimicrobial drugs by mothers before delivery, which can transfer a large amount of antibiotics to the fetus through the placenta and prevent the development of septicemia, reducing the incidence of EONS.18
In terms of the distribution of microbes, CoNS isolates were the most common at 63.9%, which is consistent with the results of another study in China.12 CoNS strains can produce intercellular lipopolysaccharide adhesins and extracellular mucus-like substances that contribute to adhesion and colonization on skin and mucosal surfaces. In addition, these factors prevent antibacterial drugs from penetrating bacterial cells.22 Blood cultures are susceptible to contamination if strict disinfection procedures were not followed; therefore, CoNS is frequently considered a contaminant. However, with the widespread development of various new diagnostic techniques and the increase in trauma operations in recent years, which result in the destruction of the neonatal barrier and impair immune function, this bacterium has become an important pathogenic microorganism detected via blood culture. Moreover, the rate of infection with CoNS is rising, which merits attention from pediatricians as well as nursing and hospital staff.
Among the gram-positive organisms, Streptococcus agalactiae, which represents GBS, was the next most prevalent after CoNS, accounting for 5.1% of the isolates. GBS infection is a major cause of NS in developed countries and has been widely reported.23–25 In developed countries, screening for GBS in late pregnancy and administering antimicrobial prophylaxis to positive cases have yielded good results, leading to a yearly decrease in the GBS detection rate. However, in China, uniform guidelines or norms to guide the antenatal screening for and treatment of GBS are lacking; therefore, its prevalence is increasing, as seen in the present study, in which GBS accounted for the second highest number of gram-positive bacterial isolates.26 The third most common gram-positive bacterial isolate at 3.9% was Enterococcus spp., which consisted mainly of E. faecalis and E. faecium. Enterococcus spp. may easily adhere to the surface of various catheters to form biofilms, which are difficult to remove with routine disinfection; the use of intravenous catheters can lead to septicemia. Staphylococcus aureus was the fourth most prevalent microorganism, at 2.8%. Although the number of isolates was small, S. aureus is extremely pathogenic and often causes serious infections, resulting in a poor prognosis or even death. Notably, Listeria monocytogenes (1.2%) and other β-hemolytic Streptococcus spp. (0.6%) were also detected in NS cases. L. monocytogenes is an intracellular, aerobic and partly anaerobic, gram-positive bacterium that is mainly transmitted to humans orally through food. L. monocytogenes infections may be asymptomatic in pregnant women; however, fetal infection is a serious disease that can lead to preterm delivery, miscarriage, septicemia, central nervous system (CNS) involvement, and even death.27 NS caused by GBS has received attention, but other β-hemolytic Streptococcus spp. can also cause NS and merit more attention.28 Therefore, it is recommended that the pathogen scope in prenatal GBS screening be expanded to include other β-hemolytic Streptococcus spp.
In this study, the main gram-negative bacilli that caused NS were Enterobacterales. The predominance of Enterobacterales isolates in NS cases may due to newborn acquisition of these gram-negative bacteria from the mother’s vaginal and fecal flora as well as the environment in which delivery occurs, making strict asepsis and disinfection of the surrounding environment essential during delivery. Nonfermenting gram-negative bacilli such as Acinetobacter baumannii and Pseudomonas aeruginosa are less frequently isolated in cases of NS but are the major pathogens involved in hospital-acquired infections and should be considered important LONS pathogens.29
The fungi that caused NS were mainly Candida, with C. parapsilosis representing the most frequently isolated strain, accounting for 69.6% of fungal cases. C. parapsilosis is ubiquitous in nature and is a symbiotic microorganism on human skin. It is most commonly isolated from the hands (subxiphoid space) and gastrointestinal tract; human hand parasitism may contribute to the horizontal transmission of this microorganism in the NICU. Infection due to indwelling intravenous catheters and prematurity have received the most attention, as accumulating evidence links these factors to C. parapsilosis bloodstream infections.30
In this study, the antibiotic resistance patterns of the top-ranked gram-positive bacteria and gram-negative bacilli were analyzed, and the antibiotic resistance trends of the top-ranked Staphylococcus epidermidis and E. coli strains were analyzed. The results showed that 93.6% of CoNS isolates were resistant to penicillin and that 70.6% of CoNS isolates were methicillin-resistant CoNS (MRCoNS). Vancomycin-resistant CoNS strains were not found. A decreasing trend of resistance to benzocillin, quinolones and clindamycin was found in Staphylococcus epidermidis (P<0.05). The decrease in the rate of MRCoNS detection may be related to recent national policies on the use of antimicrobial drugs, which have promoted the rational use of antimicrobial drugs through administrative interventions and reduced the rate of CoNS resistance to oxacillin. The decrease in the rate of resistance to quinolones and clindamycin over the study period may be related to the low rates of administration of these drugs, especially because quinolones have toxic side effects when administered to newborns and are less commonly used in clinical practice (statistics on the use of antimicrobial drugs will be available in a future study, which has not yet been published). Notably, 100% of GBS isolates were susceptible to penicillin; therefore, penicillin is the first choice for the prophylaxis and treatment of GBS in late-pregnancy GBS-positive pregnant women and newborns. Clindamycin can be used in penicillin-allergic patients, but the resistance rate in GBS is 24.4%; thus, its use is recommended in accordance with drug sensitivity results. No VRE strains were found among the Enterococcus spp. Similarly, no vancomycin-resistant strains were found among the Staphylococcus aureus isolates; notably, however, the rate of MRSA isolation was 29.2%. Therefore, vancomycin should be used as the first choice for the empirical treatment of NS caused by gram-positive bacteria and then as a step-down treatment once drug sensitivity results are available. However, vancomycin has toxic side effects; thus, monitoring the blood concentration of vancomycin is recommended when used in neonatal patients to ensure drug administration safety.
Among the antibiotic resistance patterns of gram-negative bacilli, the greatest concern is the resistance of Enterobacterales to carbapenem-based antimicrobials. E. coli, K. pneumoniae, and Enterobacter cloacae are the major isolates of carbapenem-resistant Enterobacterales (CRE), which cause high morbidity and mortality rates and exhibit worldwide prevalence.31,32 In K. pneumoniae, the rates of resistance to ertapenem and imipenem were severe, at 37.9% and 39.4%, respectively. However, it is encouraging to note that E. coli and Enterobacter cloacae remained highly susceptible to carbapenems. The most important mechanism of resistance to carbapenems in K. pneumoniae is the acquisition of plasmid-mediated carbapenemases, especially serine carbapenemases and metallo-β-lactamases, of which K. pneumoniae carbapenemase (KPC), Verona integron-encoded metallo-β-lactamase (VIM) and New Delhi metallo-β-lactamase (NDM) have been reported most frequently, but the specific mechanism of resistance in this study needs further investigation.33,34 It has also been suggested that CRE can be cloned, allowing rapid transmission of drug resistance genes between bacterial species, and can be transmitted by contact between shared medical equipment and hands, making it highly amenable to causing hospital-acquired infections, the consequences of which can be fatal in the event of an epidemic in a NICU.35 In addition, K. pneumoniae and E. coli have attracted attention because of their high rates of multidrug resistance. In China, ampicillin/piperacillin and third-generation cephalosporins are the first-line empirical antibiotics used to treat NS.24 However, in this study, K. pneumoniae and E. coli exhibited high resistance to ampicillin, to which K. pneumoniae is intrinsically resistant, and third-generation cephalosporins, which merit more attention.
In the analysis of E. coli antibiotic resistance, we found that E. coli showed no trends in resistance to the antimicrobial drugs tested between 2014 and 2021, except for ceftriaxone, to which E. coli showed an increasing trend in resistance (p<0.05). Due to the limited options of antimicrobial drugs in the neonatal population, the use of third-generation cephalosporins, especially ceftriaxone, is high. Ceftriaxone is often used as the first choice for the experimental treatment of neonatal infections because of its broad antibacterial spectrum, which has led to an increase in the rate of drug resistance.
Candida had a low rate of resistance to all five antifungal drugs in the drug sensitivity tests. NS caused by Candida infection is primarily associated with catheter-associated bloodstream infections, and the most effective measure for treating these conditions is catheter removal, as mentioned earlier.30
The present study has some limitations. First, this retrospective study was based on data collected from laboratory records, which lack data on clinical information, the treatment outcomes, and the final outcomes in the neonates. Therefore, it was not possible to classify the infections as community acquired or hospital acquired, nor was it possible to distinguish between neonates born in our hospital and those who were transferred from outside hospitals. Second, the study was conducted at only one hospital; therefore, the pattern of antibiotic resistance observed in our study may be somewhat biased and not generalizable to other parts of the country. Third, there was some bias in the resistance trends or rates due to the decrease in the number of hospitalized children and the decrease in the number of isolated strains in 2020–2021 as a result of the COVID-19 pandemic.
Conclusion
This study showed that the incidence of NS was 4.59 cases per 1000 LBs. CoNS was the main cause of NS in the study, followed by E. coli. The bacterial isolates showed varying levels of resistance to the antimicrobial drugs tested in our hospital. Fortunately, however, gram-positive isolates did not show resistance to linezolid, vancomycin or tigecycline. Similarly, gram-negative isolates were more sensitive to amikacin, gentamicin, imipenem, piperacillin-tazobactam, and tobramycin. Thus, given the most effective antibiotics observed in this study, it is imperative that clinicians modify their empirical treatment regimens when appropriate. Regular surveillance in the hospital setting is recommended to monitor changes in the pathogens that cause NS as well as their antibiotic resistance patterns; this monitoring will enable the implementation of optimal prevention and treatment strategies. Moreover, systematically rotating antibiotics or antibiotic classes for empirical treatment might also reduce rates of antibiotic resistance.36 Finally, further research is needed on the relationship between antimicrobial drug use and resistance, as well as on the mechanisms of resistance in multidrug-resistant organisms (MDROs), to upgrade and develop more targeted and effective interventions.
Funding
This study was funded by the Hubei Provincial Health Commission Joint Fund Project (No: WJ2019H280).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Shane AL, Sánchez PJ, Stoll BJ. Neonatal sepsis. Lancet. 2017;390(10104):1770–1780. doi:10.1016/s0140-6736(17)31002-4
2. Greer O, Shah NM, Sriskandan S, et al. Sepsis: precision-based medicine for pregnancy and the puerperium. Int J Mol Sci. 2019;20:21. doi:10.3390/ijms20215388
3. Almohammady MN, Eltahlawy EM, Reda NM. Pattern of bacterial profile and antibiotic susceptibility among neonatal sepsis cases at Cairo University Children Hospital. J Taibah Univ Med Sci. 2020;15(1):39–47. doi:10.1016/j.jtumed.2019.12.005
4. Pokhrel B, Koirala T, Shah G, et al. Bacteriological profile and antibiotic susceptibility of neonatal sepsis in neonatal intensive care unit of a tertiary hospital in Nepal. BMC Pediatr. 2018;18(1):208. doi:10.1186/s12887-018-1176-x
5. Simonsen KA, Anderson-Berry AL, Delair SF, et al. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014;27(1):21–47. doi:10.1128/CMR.00031-13
6. Schrag SJ, Farley MM, Petit S, et al. Epidemiology of invasive early-onset neonatal sepsis, 2005 to 2014. Pediatrics. 2016;138(6). doi:10.1542/peds.2016-2013
7. Kim SJ, Kim GE, Park JH, et al. Clinical features and prognostic factors of early-onset sepsis: a 7.5-year experience in one neonatal intensive care unit. Korean J Pediatr. 2019;62(1):36–41. doi:10.3345/kjp.2018.06807
8. Braye K, Foureur M, de Waal K, et al. Epidemiology of neonatal early-onset sepsis in a geographically diverse Australian health district 2006–2016. PLoS One. 2019;14(4):e0214298. doi:10.1371/journal.pone.0214298
9. Tessema B, Lippmann N, Knupfer M, et al. Antibiotic resistance patterns of bacterial isolates from neonatal sepsis patients at university hospital of Leipzig, Germany. Antibiotics. 2021;10(3):323. doi:10.3390/antibiotics10030323
10. Ullah O, Khan A, Ambreen A, et al. Antibiotic sensitivity pattern of bacterial isolates of neonatal septicemia in Peshawar, Pakistan. Arch Iran Med. 2016;19(12):866–869.
11. Softic I, Tahirovic H, Di Ciommo V, et al. Bacterial sepsis in neonates: single centre study in a neonatal intensive care unit in Bosnia and Herzegovina. Acta Med Acad. 2017;46(1):7–15. doi:10.5644/ama2006-124.181
12. Guo J, Luo Y, Wu Y, et al. Clinical characteristic and pathogen spectrum of neonatal sepsis in Guangzhou City from June 2011 to June 2017. Med Sci Monit. 2019;25:2296–2304. doi:10.12659/MSM.912375
13. Li X, Ding X, Shi P, et al. Clinical features and antimicrobial susceptibility profiles of culture-proven neonatal sepsis in a tertiary children’s hospital, 2013 to 2017. Medicine. 2019;98(12):e14686. doi:10.1097/MD.0000000000014686
14. Li QY, An Y, Liu L, et al. Differences in the clinical characteristics of early- and late-onset necrotizing enterocolitis in full-term infants: a retrospective case-control study. Sci Rep. 2017;7:43042. doi:10.1038/srep43042
15. Boskabadi H, Moradi A, Ramazani A, et al. Sensitivity and resistance of the microorganisms responsible for neonatal sepsis to antibiotics. Arch Clin Infect Dis. 2020;15(6). doi:10.5812/archcid.84710
16. Boskabadi H, Heidari E, Bagheri F, et al. Antibiotic susceptibility patterns in the NICU of Ghaem Hospital of Mashhad. Int J Med Lab. 2021;8(1):17–26. doi:10.18502/ijml.v8i1.5669
17. Gao K, Fu J, Guan X, et al. Incidence, bacterial profiles, and antimicrobial resistance of culture-proven neonatal sepsis in South China. Infect Drug Resist. 2019;12:3797–3805. doi:10.2147/IDR.S223597
18. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
19. Micek ST, Hampton N, Kollef M. Risk factors and outcomes for ineffective empiric treatment of sepsis caused by gram-negative pathogens: stratification by onset of infection. Antimicrob Agents Chemother. 2018;62(1). doi:10.1128/AAC.01577-17
20. Gebremedhin D, Berhe H, Gebrekirstos K. Risk factors for neonatal sepsis in public hospitals of Mekelle City, North Ethiopia, 2015: unmatched case control study. PLoS One. 2016;11(5):e0154798. doi:10.1371/journal.pone.0154798
21. Song WS, Park HW, Oh MY, et al. Neonatal sepsis-causing bacterial pathogens and outcome of trends of their antimicrobial susceptibility a 20-year period at a neonatal intensive care unit [published online ahead of print, 2021 Dec 9]. Clin Exp Pediatr. 2021. doi:10.3345/cep.2021.00668
22. Marchant EA, Boyce GK, Sadarangani M, et al. Neonatal sepsis due to coagulase-negative staphylococci. Clin Dev Immunol. 2013;2013:586076. doi:10.1155/2013/586076
23. Berardi A, Rossi C, Lugli L, et al. Group B streptococcus late-onset disease: 2003–2010. Pediatrics. 2013;131(2):e361–8. doi:10.1542/peds.2012-1231
24. Dong Y, Jiang SY, Zhou Q, et al. Group B Streptococcus causes severe sepsis in term neonates: 8 years experience of a major Chinese neonatal unit. World J Pediatr. 2017;13(4):314–320. doi:10.1007/s12519-017-0034-5
25. Bekker V, Bijlsma MW, van de Beek D, et al. Incidence of invasive group B streptococcal disease and pathogen genotype distribution in newborn babies in the Netherlands over 25 years: a nationwide surveillance study. Lancet Infect Dis. 2014;14(11):1083–1089. doi:10.1016/s1473-3099(14)70919-3
26. Ji W, Liu H, Madhi SA, et al. Clinical and molecular epidemiology of invasive group B streptococcus disease among infants, China. Emerg Infect Dis. 2019;25(11):2021–2030. doi:10.3201/eid2511.181647
27. Wang J, Zhang H, Yan J, et al. Literature review on the distribution characteristics and antimicrobial resistance of bacterial pathogens in neonatal sepsis. J Matern Fetal Neonatal Med. 2022;35(5):861–870. doi:10.1080/14767058.2020.1732342
28. Saegeman V, Cossey V, Loens K, et al. Streptococcus gallolyticus subsp. pasteurianus infection in a neonatal intensive care unit. Pediatr Infect Dis J. 2016;35(11):1272–1275. doi:10.1097/INF.0000000000001290
29. Pascale R, Corcione S, Bussini L, et al. Non-fermentative gram-negative bloodstream infection in northern Italy: a multicenter cohort study. BMC Infect Dis. 2021;21(1):806. doi:10.1186/s12879-021-06496-8
30. Pammi M, Holland L, Butler G, et al. Candida parapsilosis is a significant neonatal pathogen: a systematic review and meta-analysis. Pediatr Infect Dis J. 2013;32(5):e206–16. doi:10.1097/INF.0b013e3182863a1c
31. Mzimela BW, Nkwanyana NM, Singh R. Clinical outcome of neonates with carbapenem-resistant enterobacteriaceae infections at the King Edward VIII hospital’s neonatal unit, Durban, South Africa. S Afr J Infect Dis. 2021;36(1):223. doi:10.4102/sajid.v36i1.223
32. Seesahai J, Church PT, Asztalos E, et al. Neonates with maternal colonization of carbapenemase-producing, carbapenem-resistant enterobacteriaceae: a mini-review and a suggested guide for preventing neonatal infection. Children. 2021;8(5):399. doi:10.3390/children8050399
33. Abe R, Oyama F, Akeda Y, et al. Hospital-wide outbreaks of carbapenem-resistant enterobacteriaceae horizontally spread through a clonal plasmid harbouring blaIMP-1 in children’s hospitals in Japan. J Antimicrob Chemother. 2021;76(12):3314–3317. doi:10.1093/jac/dkab303
34. Fatima A, Kamran R, Rashid H, et al. Molecular characterisation of carbapenem-resistant enterobacteriaceae from intensive care units. J Coll Physicians Surg Pak. 2019;29(9):878–881. doi:10.29271/jcpsp.2019.09.878
35. Ding Y, Wang Y, Hsia Y, et al. Systematic review of carbapenem-resistant enterobacteriaceae causing neonatal sepsis in China. Ann Clin Microbiol Antimicrob. 2019;18(1):36. doi:10.1186/s12941-019-0334-9
36. van Duijn PJ, Bonten MJ. Antibiotic rotation strategies to reduce antimicrobial resistance in Gram-negative bacteria in European intensive care units: study protocol for a cluster-randomized crossover controlled trial. Trials. 2014;15:277. doi:10.1186/1745-6215-15-277
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.