Back to Journals » OncoTargets and Therapy » Volume 9
Clinical implication of long noncoding RNA 91H expression profile in osteosarcoma patients
Authors Xia W, Lin Q, Shen D, Liu Z, Su J, Mao W
Received 30 December 2015
Accepted for publication 20 May 2016
Published 26 July 2016 Volume 2016:9 Pages 4645—4652
DOI https://doi.org/10.2147/OTT.S103376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Wen-Kai Xia,1 Qing-Feng Lin,2 Dong Shen,2 Zhi-Li Liu,2 Jun Su,2 Wei-Dong Mao2
1Department of Nephrology, 2Department of Oncology, The Affiliated Jiangyin Hospital, School of Medicine, Southeast University, Jiangyin, Jiangsu, People’s Republic of China
Abstract: Long noncoding RNAs have been documented as having widespread roles in carcinogenesis and cancer progression. However, roles of long noncoding RNAs in osteosarcoma remain unclear. This study is to investigate the clinical relevance and biological functions of long noncoding RNA 91H in osteosarcoma. Herein, we confirmed that 91H expression was notably increased in osteosarcoma patients and cell lines compared to healthy controls and normal human bone cell lines. High expression of 91H was significantly correlated with advanced clinical stage, chemotherapy after surgery, and tumor size >5 cm. Furthermore, 91H was an independent prognostic factor for overall survival in osteosarcoma patients after treatments. Additionally, the knockdown of 91H expression inhibited osteosarcoma cells’ proliferation and promoted their apoptosis in vitro. In summary, these findings indicate that 91H may be a novel biomarker for risk prognostication and also provide a clue to the molecular etiology of osteosarcoma.
Keywords: long noncoding RNA, 91H, osteosarcoma, survival
Introduction
Osteosarcoma is a major primary malignant tumor of bone and accounts for ~20% of all bone malignancies.1,2 It is a leading cause of cancer mortality in young adults and adolescents,3 particularly among adolescents aged 15–19 years.4 Despite the advanced development in therapeutic strategies for osteosarcoma in recent years, the 5-year survival remains unsatisfactory due to local relapse or metastasis after surgery. Lack of a better molecular biomarker to detect osteosarcoma at an early tumor stage is a major cause of the poor outcome of osteosarcoma. Thus, it is essential for us to further decipher the underlying molecular mechanisms and find a beneficial biomarker of osteosarcoma to predict its outcome.
Recently, published evidences have shown that long noncoding RNAs (lncRNAs), longer than 200 nt in length and with a lack of capability for protein coding, play a critical biological role in carcinogenesis and development.2 Despite the lack of understanding of lncRNAs in comparison with microRNAs,5,6 lncRNAs-mediated biological functions have been shown to be implicated in the regulation of diverse cellular processes, such as cell proliferation, cell cycle progression and cell apoptosis, meiotic entry and telomere length, and stem cell pluripotency and differentiation.7,8 Additionally, lncRNAs are highly conserved throughout mammalian evolution and abnormally expressed in tumor tissues, which are considered as oncogenes or tumor suppressors. Intriguingly, lncRNAs are also commonly expressed in serum, plasma, and other bodily fluids.9–11 Changes in lncRNAs expression levels have been increasingly verified in a variety of cancer types, indicating that they are potentially new targets for cancer diagnostics and treatments.12
91H, H19 antisense RNA is also a lncRNA greater than 119 kb in length, located on the position of the H19/insulin-like growth factor 2 (IGF2) locus (accession number NC_000011.9). 91H was originally reported to be overexpressed in breast cancer; IGF2 expression is subject to 91H control in trans.13 Studies have shown that 91H is aberrantly expressed and involved in carcinogenesis and progression of esophageal squamous cell carcinoma and colorectal cancer.14,15 However, to our knowledge, the clinical significance and biological function of 91H lncRNA in osteosarcoma have not been reported.
Here, we evaluated the expression of 91H in plasma samples of osteosarcoma patients and healthy controls, as well as investigated the correlation of circulating 91H expression with clinical characteristics and outcome. Furthermore, a predictive model based on significant variables in multivariate analysis was constructed to forecast the prognosis of osteosarcoma patients. Additionally, we also evaluated the biologic roles of lncRNA 91H in osteosarcoma cell lines.
Materials and methods
Patients and cell lines
The Medical Ethics Committee of The Affiliated Jiangyin Hospital, School of Medicine, Southeast University approved this study. Written informed consent was collected from all enrolled patients in the study. All blood samples were handled and made anonymous following ethical and legal standards.
Sixty-seven blood samples were obtained between 2008 and 2010 from osteosarcoma patients prior to treatment in Jiangyin and Nanjing (Jiangsu, People’s Republic of China) for analysis using quantitative real-time PCR (qPCR). One hundred healthy controls with matched age and sex were enrolled. Plasma samples were immediately isolated from blood samples and then stored at −80°C until RNA extraction. None of the patients had previously undergone surgery, chemotherapy, radiotherapy, or blood transfusion. Clinical characteristics of these patients were collected for diagnosis: sex, age, tumor size, tumor location, clinical stage, chemotherapy after surgery, and initial metastasis (Table 1).
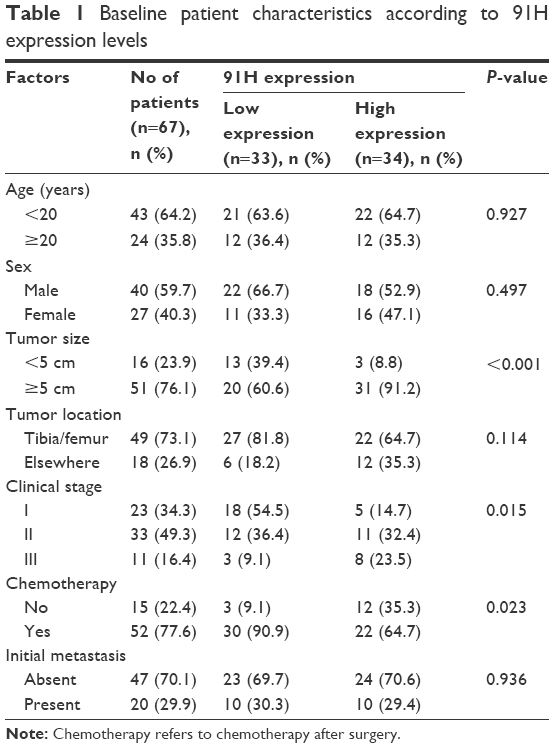 | Table 1 Baseline patient characteristics according to 91H expression levels |
After treatment, each patient was followed up every 3 months for the first 2 years and then every 6 months up to the fifth year, until October 2015, or until death. Physical examination, imageological diagnosis, and laboratory tests were performed at every visit. The follow-up period ranged from 3 months to 60 months, with a median of 60 months. Overall survival (OS) was calculated from diagnosis to death. The date of last follow-up was used for drop-out patients.
Cell lines SAOS-2, U2OS, MG63, HOS (human osteosarcoma cell lines), and hFOB (normal human bone cell line) were purchased from Shanghai Cell Collection, Chinese Academy of Sciences. All cell lines were maintained in Dulbecco’s Modified Eagle’s Medium (DMEM; Thermo Fisher Scientific, Waltham, MA, USA) consisting of 10% fetal bovine serum (Thermo Fisher Scientific) and cultured at 37°C with 5% CO2.
RNA extraction and cDNA synthesis
Total RNA from plasma samples and supernate of cell lines was extracted using the Trizol LS reagent (Thermo Fisher Scientific) according to the manufacturer’s protocol and stored at −80°C. A Nanodrop spectrophotometer (Thermo Fisher Scientific) was used to measure total RNA concentration and purity. The optical density 260/280 for RNA samples varied from 1.8 to 2.0. cDNA was then synthesized using the PrimeScript RT reagent Kit with gDNA Eraser (Takara Bio Inc., Beijing, People’s Republic of China) and stored at −20°C until qPCR.
Quantitative real-time PCR
91H expression was determined by qPCR using the ABI 7500 System (Thermo Fisher Scientific) and SYBR Premix Ex TagTM II (Takara Bio Inc.). The reaction system of qPCR was in a volume of 20 μL, containing 30 ng of cDNA. The qPCR cycling program was set for first hold at 95°C for 10 minutes, followed by 40 amplification cycles of melting at 95°C for 10 seconds, and annealing and extension at 60°C. The sequence of 91H primer was as follows: forward, 5′-GCTTGTCAGTAGAGTGCGCC-3′; reverse, 5′-CATCCAGTTGACCGAGCTTG-3′. Glyceraldehyde 3-phosphate dehydrogenase was used as an internal control. 91H expression was normalized to the internal control to obtain the relative cycle (ΔCt). The relative expression was calculated by the comparative Ct (ΔΔCt) method, and relative expression folds (2−ΔΔCt) were also counted.
Cell transfection
MG63 is selected to perform succeeding experiments as 91H expression levels in MG63 cells were the highest among all cell lines. RNA interference was conducted by using synthetic small interfering RNA (siRNA) duplexes, as described by previous report no 22662250.16 Two synthetic siRNA duplexes (si-91H: si91H1, 5′-GGCGUCAUUCUGAUGGGACTT-3′ and si91H2, 5′-UUCAGGAGCUUAAGAUGCUTT-3′) targeting the 91H RNA sequences and a negative control (si-NC, 5′-CGUGGGUGGAUGCAUGGAUTT-3′) of 400 pmoL were transfected into MG63 cells in a six-well plate using the Lipofectamine 2000 transfection reagent (Thermo Fisher Scientific). After 48 hours of infection, 91H expression levels were determined using qPCR.
Cell proliferation assay
The ability of viable cells was evaluated by the CCK-8 assay using a Cell Counting Kit-8 (CCK-8; Dojindo Laboratories, Rockville, MD, USA) following the manufacturer’s protocol after treatment for 48 hours with siRNA. Treated cells (1,000 cells/well) were seeded in flat bottom 96-well plates with 100 μL DMEM per well. After incubation for 12, 24, 36, 48, and 72 hours, respectively, 10 μL of CCK-8 reagents was added to each well and then the medium was removed after 1 hour of culture. Absorbances were measured on a microplate reader at 450 nm wavelength (Bio-Rad Laboratories Inc., Hercules, CA, USA). Each subgroup was repeated for five wells, and the experiments were repeated three times.
Apoptosis analysis by flow cytometry
Flow cytometry was used to evaluate cell apoptosis after staining with annexin V conjugated with fluorescein isothiocyanate and propidium iodide (BD Biosciences, San Jose, CA, USA). MG63 cells were transfected with si-91H or si-NC in a six-well plate. Cell apoptosis rates were analyzed after 48 hours transfection. All apoptosis assays were performed in triplicate.
Statistical analysis
Statistical analyses were performed using the SPSS version 20.0 software (IBM Corporation, Armonk, NY, USA). A chi-square test or Fisher’s exact test was conducted to analyze categorical data, and an independent t-test or Mann–Whitney U-test was used to explore continuous data. Continuous data were expressed as mean ± standard deviation. Survival curves were depicted by the Kaplan–Meier method, and the statistical significance was assessed by the log-rank test. The predictors of OS determined in univariate analyses were further assessed by multivariate analysis using Cox’s proportional hazards model. A predictive model for OS was constructed by the R 3.0.3 software (Institute for Statistics and Mathematics, Vienna, Austria), and the predictive accuracy was measured by Harrell’s concordance index (c-index). P-value less than 0.05 was considered statistically significant.
Results
Circulating 91H expression profile in osteosarcoma
qPCR was performed to determine the expression of lncRNA 91H in plasma samples from 67 osteosarcoma patients and 100 healthy controls as well as cell lines. The relative expression levels of 91H were markedly increased in the osteosarcoma group compared to the healthy control group (Figure 1A). Furthermore, 91H expression was obviously elevated in osteosarcoma cell lines (SAOS-2, U2OS, MG63, and HOS) than in hFOB cells (Figure 1B). Intriguingly, MG63 cells exhibited the highest expression levels of 91H and were therefore selected for succeeding experiments in vitro.
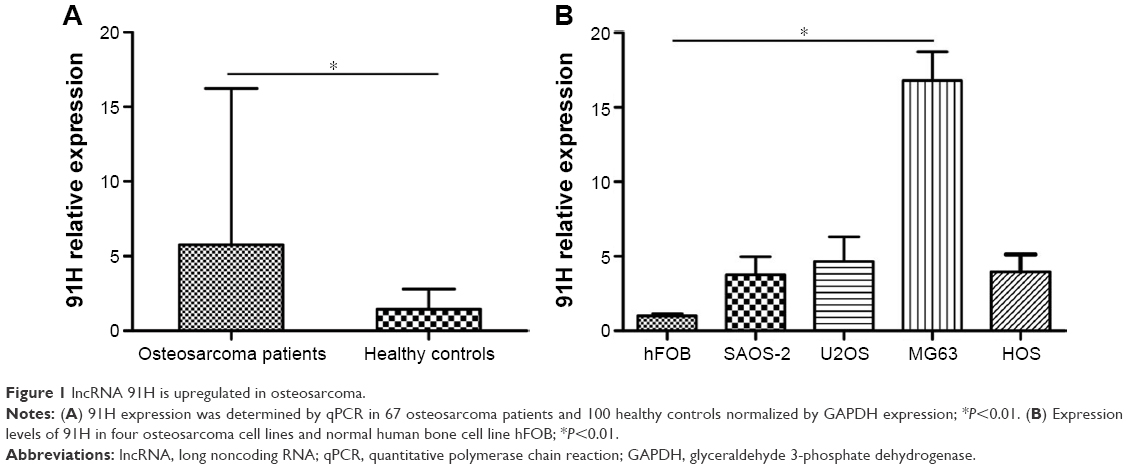 | Figure 1 lncRNA 91H is upregulated in osteosarcoma. |
Correlation of circulating 91H with clinical characteristics in osteosarcoma patients
To determine whether circulating 91H expression was associated with clinical characteristics of osteosarcoma, 67 patients with osteosarcoma were classified into two subgroups (low group <2.05-fold and high group ≥2.05-fold) according to a median of 91H expression levels. Our results indicate that 91H overexpression was notably correlated with advanced clinical stage, chemotherapy after surgery, and tumor size greater than 5 cm, but not with other clinical parameters summarized in Table 1.
Association of circulating 91H and clinical outcome in patients with osteosarcoma
To investigate the prognostic performance of circulating 91H expression in osteosarcoma patients, survival curves were depicted in 67 patients according to prognostic information. Twenty-six deaths were reported and five patients have censored during the follow-up (3–60 months). Kaplan–Meier curves showed that a high expression of 91H (Figure 2A), initial metastasis, and no postoperative chemotherapy were significantly related with a shorter OS (Table 2). However, patients’ age, sex, tumor size, tumor location, and clinical stage (Figure 2B) were not associated with a worsening OS.
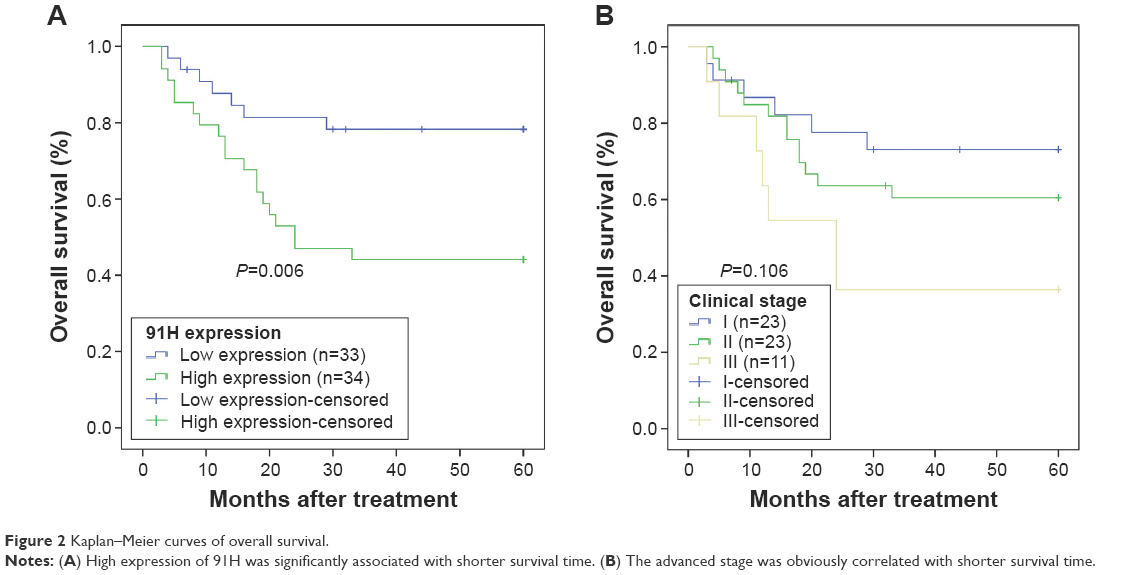 | Figure 2 Kaplan–Meier curves of overall survival. |
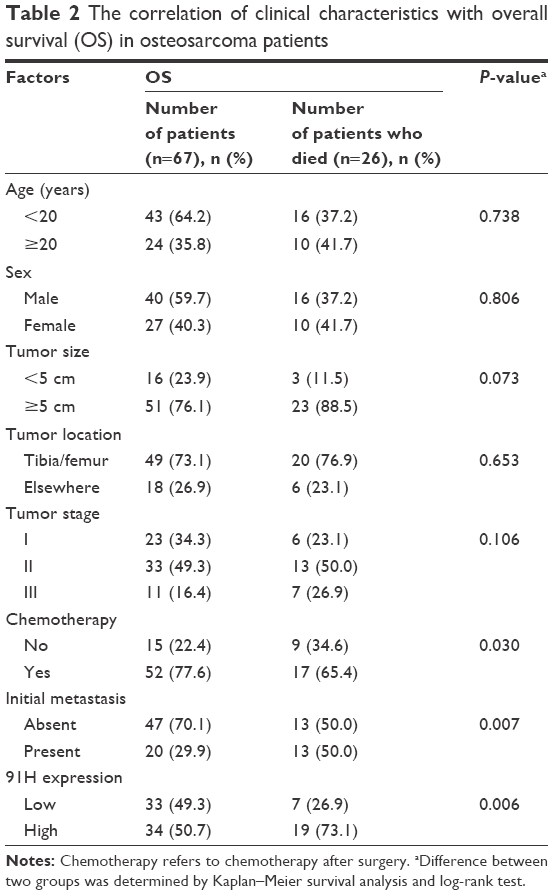 | Table 2 The correlation of clinical characteristics with overall survival (OS) in osteosarcoma patients |
Additionally, Cox regression model was used to further investigate the potential significance of circulating 91H as a prognostic indicator. Clinical stage, postoperative chemotherapy, initial metastasis, and 91H expression were notably correlated with the OS of osteosarcoma patients in univariate analyses, whereas other variables such as age, sex, tumor size, and tumor location were not related with the outcome of osteosarcoma patients (Table 3). Multivariate analyses revealed that 91H expression and initial metastasis were strongly associated with the OS of patients with osteosarcoma (P=0.010 and 0.010, respectively; Table 3). Therefore, 91H expression might be an independent prognostic factor for osteosarcoma patients. Furthermore, a predictive model based on significant parameters in multivariate analyses was established to predict the probability of 3- or 5-year survival in osteosarcoma patients after treatment (c-index: 0.69; Figure 3). The constructed nomogram was employed by summing the points identified on the top scale for each independent indicator. This total point score was further identified on the total points scale to determine the probability of 3- and 5-year survival.
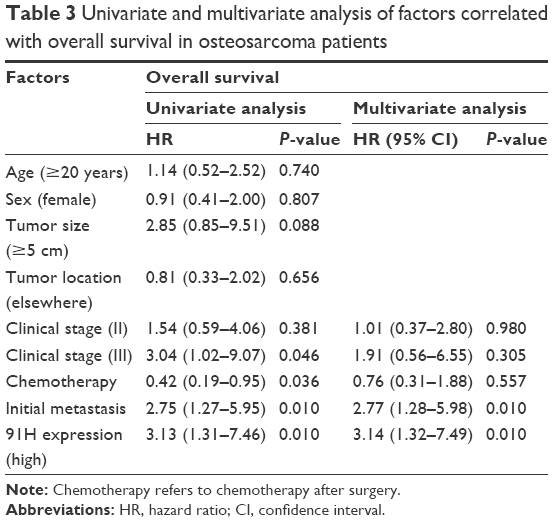 | Table 3 Univariate and multivariate analysis of factors correlated with overall survival in osteosarcoma patients |
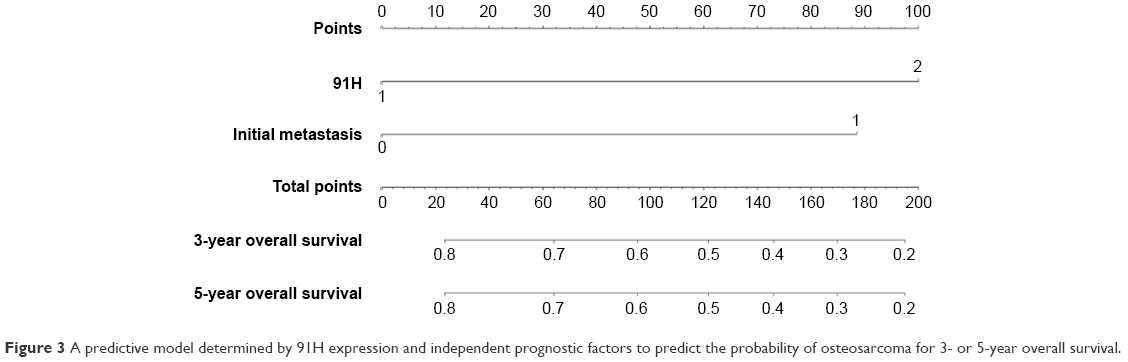 | Figure 3 A predictive model determined by 91H expression and independent prognostic factors to predict the probability of osteosarcoma for 3- or 5-year overall survival. |
Knockdown of 91H expression decreased proliferation and promoted apoptosis of osteosarcoma cells in vitro
To explore the role of 91H in the development of osteosarcoma, MG63 cells were infected with si-NC or si-91H with a high interference efficiency (Figure 4A), suggesting that we successfully silenced the expression of 91H in MG63 cells. In CCK-8 assay, we observed that the knockdown of 91H markedly suppressed the cellular growth of MG63 cells (Figure 4B). These findings suggest a critical role of 91H in manipulating the growth of osteosarcoma. Furthermore, the effect of lncRNA 91H on the apoptosis of osteosarcoma cells was determined by flow cytometry. Apoptosis ability of MG63 cells (Figure 4C) was obviously promoted after the knockdown of 91H expression (Figure 4D).
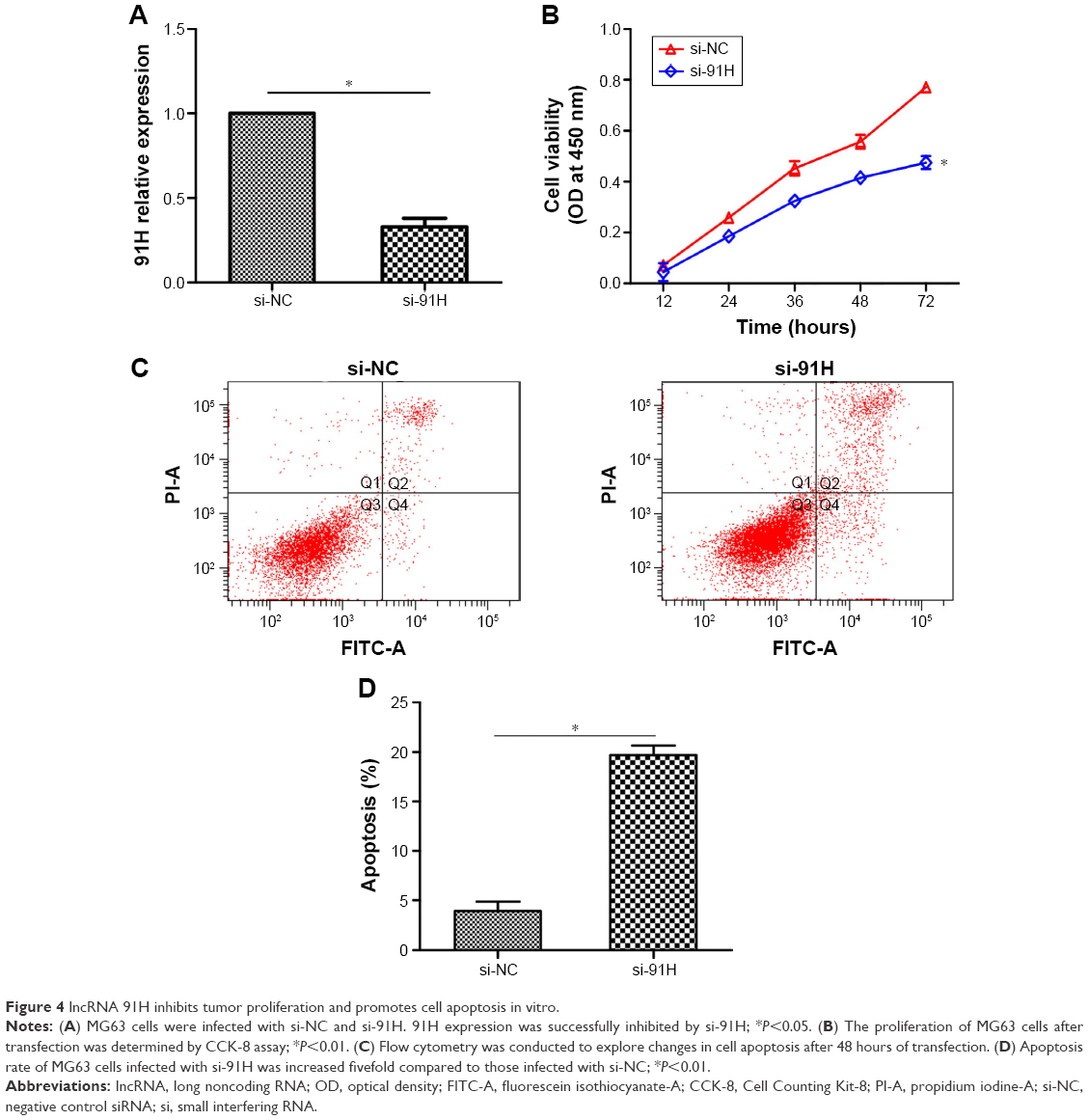 | Figure 4 lncRNA 91H inhibits tumor proliferation and promotes cell apoptosis in vitro. |
Discussion
During recent years, the role of lncRNAs in carcinogenesis has attracted more and more investigators to focus on their biologic functions, such as lncRNA associated with microvascular invasion in hepatocellular carcinoma (MVIH), metastasis-associated with lung adenocarcinoma transcript 1 (MALAT1), and HOX antisense intergenic RNA (HOTAIR). lncRNAs are widely defined as RNA molecules >200 bp in length which lack an open reading frame.17 It has been well established that dysregulation of lncRNAs alters epigenetic information resulting in progressive and persistent tumor growth,18 and lncRNAs have been documented as markers for diagnosis and prognosis, as well as potential therapeutic targets.19,20 For example, microvascular invasion in hepatocellular carcinoma has been associated with a poor recurrence-free survival after hepatectomy as well as tumor intrahepatic metastasis due to activating angiogenesis.21 Metastasis-associated with lung adenocarcinoma transcript 1 is dysregulated in multiple cancers, such as renal cell carcinoma,22 colorectal cancer,23 and prostate cancer.24 HOX antisense intergenic RNA is dysregulated in breast cancer progression by recruitment of polycomb repressive complex 2 to specific targets leading to cancer invasiveness and metastasis.8
Berteaux et al first reported 91H overexpression in human breast cancer in 2008 and demonstrated that the upregulation of 91H promotes the expression of IGF2 expression in trans.13 However, clinical significance and biologic function of 91H in osteosarcoma remain unclear. In this study, we explored the prognostic value of lncRNA 91H in osteosarcoma. Our results suggested that 91H was overexpressed in osteosarcoma patients and cell lines. We also demonstrated that the high expression of 91H was associated with advanced stage, no postoperative chemotherapy, and tumor size. Furthermore, the high expression of 91H shortened OS and served as an independent prognostic factor in patients with osteosarcoma. A previous study showed a high expression of 91H in colorectal cancer that serves as a valuable independent prognostic factor for patients.15 These results suggested that 91H may be involved in carcinogenesis and cancer progression.
Next, to understand its biological role in osteosarcoma cell lines, we transfected si-NC or si-91H into MG63 cells. We observed that the suppression of 91H markedly promoted cell apoptosis and blocked the proliferation of MG63 cells. The previous experiments revealed that 91H regulates the expression levels of H19 in cis and controls IGF2 transcription in trans in mouse myoblasts.25 Gao et al suggested that lncRNA 91H was subjected to H19 imprinting control regions and inhibited IGF2 expression of esophageal squamous cell carcinoma.14 These findings suggest a promising new insight into the potential molecular mechanisms of regulating carcinogenesis and tumor progression.
Additionally, the present study attempted to establish a predictive nomogram to predict the probability of postoperative patients who will die of cancer-related causes within 3 and 5 years based on 91H expression levels and independent factors in multivariate analyses. Therefore, our constructed model could be helpful to predict the 3- or 5-year survival of osteosarcoma. In addition, in our study, we did not find the association between 91H expression and initial metastasis. This result was inconsistent with previous studies.14,15 Sample size, type of the sample, and pathological type of tumor led to the inconsistent results.
Some limitations should be acknowledged. First, we did not evaluate the expression levels of 91H in osteosarcoma tissues to further verify our results. Second, transwell assays were not performed to estimate invasiveness and migration of 91H in osteosarcoma cell lines. Finally, sample size was not adequate and more studies were conducted to prove these findings.
Conclusion
In conclusion, our study showed that 91H expression is associated with clinical stage, as well as being a valuable independent prognostic factor for patients with OS after treatment. Moreover, in vitro experiments revealed that the knockdown of 91H expression contributed to the inhibition of cell proliferation and promotion of cell apoptosis. These results suggest that the downregulated 91H in osteosarcoma promotes tumor progression. 91H may be a therapeutic potential to control tumor progression as well as an indicator for risk prognostication and precise therapy screening of osteosarcoma.
Acknowledgment
This project was supported by grants from The National Natural Science Foundation of China (81402554) to ZLL.
Author contributions
WKX and WDM conceived and designed the experiments; WKX, QFL, DS, ZLL, and JS performed the experiments; WKX and QFL analyzed the data; DS and ZLL contributed reagents/materials/analysis tools; WKX and WDM wrote the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Clark JC, Dass CR, Choong PF. A review of clinical and molecular prognostic factors in osteosarcoma. J Cancer Res Clin Oncol. 2008;134(3):281–297. | ||
Bielack S, Carrle D, Casali PG. Osteosarcoma: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;20(Suppl 4):137–139. | ||
Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004: data from the Surveillance, Epidemiology, and End Results Program. Cancer. 2009;115(7):1531–1543. | ||
Damron TA, Ward WG, Stewart A. Osteosarcoma, chondrosarcoma, and Ewing’s sarcoma: National Cancer Data Base Report. Clin Orthop Relat Res. 2007;459:40–47. | ||
Hammond SM. MicroRNAs as oncogenes. Curr Opin Genet Dev. 2006;16(1):4–9. | ||
Esquela-Kerscher A, Slack FJ. Oncomirs – microRNAs with a role in cancer. Nat Rev Cancer. 2006;6(4):259–269. | ||
Prensner JR, Iyer MK, Sahu A, et al. The long noncoding RNA SChLAP1 promotes aggressive prostate cancer and antagonizes the SWI/SNF complex. Nat Genet. 2013;45(11):1392–1398. | ||
Gupta RA, Shah N, Wang KC, et al. Long non-coding RNA HOTAIR reprograms chromatin state to promote cancer metastasis. Nature. 2010;464(7291):1071–1076. | ||
Panzitt K, Tschernatsch MM, Guelly C, et al. Characterization of HULC, a novel gene with striking up-regulation in hepatocellular carcinoma, as noncoding RNA. Gastroenterology. 2007;132(1):330–342. | ||
Arita T, Ichikawa D, Konishi H, et al. Circulating long non-coding RNAs in plasma of patients with gastric cancer. Anticancer Res. 2013;33(8):3185–3193. | ||
Tinzl M, Marberger M, Horvath S, Chypre C. DD3PCA3 RNA analysis in urine – a new perspective for detecting prostate cancer. Eur Urol. 2004;46(2):182–186; discussion 187. | ||
Qi P, Du X. The long non-coding RNAs, a new cancer diagnostic and therapeutic gold mine. Mod Pathol. 2013;26(2):155–165. | ||
Berteaux N, Aptel N, Cathala G, et al. A novel H19 antisense RNA overexpressed in breast cancer contributes to paternal IGF2 expression. Mol Cell Biol. 2008;28(22):6731–6745. | ||
Gao T, He B, Pan Y, et al. Long non-coding RNA 91H contributes to the occurrence and progression of esophageal squamous cell carcinoma by inhibiting IGF2 expression. Mol Carcinog. 2015;54(5):359–367. | ||
Deng Q, He B, Gao T, et al. Up-regulation of 91H promotes tumor metastasis and predicts poor prognosis for patients with colorectal cancer. PLoS One. 2014;9(7):e103022. | ||
Tran VG, Court F, Duputié A, et al. H19 antisense RNA can up-regulate Igf2 transcription by activation of a novel promoter in mouse myoblasts. PLoS One. 2012;7(5):e37923. | ||
Wilusz JE, Sunwoo H, Spector DL. Long noncoding RNAs: functional surprises from the RNA world. Genes Dev. 2009;23(13):1494–1504. | ||
Hammerle M, Gutschner T, Uckelmann H, et al. Posttranscriptional destabilization of the liver-specific long noncoding RNA HULC by the IGF2 mRNA-binding protein 1 (IGF2BP1). Hepatology. 2013;58(5):1703–1712. | ||
Gibb EA, Brown CJ, Lam WL. The functional role of long non-coding RNA in human carcinomas. Mol Cancer. 2011;10:38. | ||
Prensner JR, Chinnaiyan AM. The emergence of lncRNAs in cancer biology. Cancer Discov. 2011;1(5):391–407. | ||
Yuan SX, Yang F, Yang Y, et al. Long noncoding RNA associated with microvascular invasion in hepatocellular carcinoma promotes angiogenesis and serves as a predictor for hepatocellular carcinoma patients’ poor recurrence-free survival after hepatectomy. Hepatology. 2012;56(6):2231–2241. | ||
Hirata H, Hinoda Y, Shahryari V, et al. Long Noncoding RNA MALAT1 Promotes Aggressive Renal Cell Carcinoma through Ezh2 and Interacts with miR-205. Cancer Res. 2015;75(7):1322–1331. | ||
Ji Q, Zhang L, Liu X, et al. Long non-coding RNA MALAT1 promotes tumour growth and metastasis in colorectal cancer through binding to SFPQ and releasing oncogene PTBP2 from SFPQ/PTBP2 complex. Br J Cancer. 2014;111(4):736–748. | ||
Ren S, Wang F, Shen J, et al. Long non-coding RNA metastasis associated in lung adenocarcinoma transcript 1 derived miniRNA as a novel plasma-based biomarker for diagnosing prostate cancer. Eur J Cancer. 2013;49(13):2949–2959. | ||
Tran VG, Court F, Duputie A, et al. H19 antisense RNA can up-regulate Igf2 transcription by activation of a novel promoter in mouse myoblasts. PLoS One. 2012;7(5):e37923. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.