Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Clinical Features of Suspected Malignant Hyperthermia in China from 2015 to 2020: A Retrospective Study from China Malignant Hyperthermia Emergency Assistance Group
Authors Tan L, Teng Y, Yu H, Liu C, Xiao K, Yin J, Zuo Y, Zhu T, Deng X ![]()
Received 23 August 2022
Accepted for publication 25 November 2022
Published 29 December 2022 Volume 2022:15 Pages 3005—3013
DOI https://doi.org/10.2147/JMDH.S387208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lingcan Tan,1,* Yi Teng,1,* Hong Yu,1 Chunyuan Liu,2 Kun Xiao,3 Jin Yin,4 Yunxia Zuo,1 Tao Zhu,1 Xiaoqian Deng1
1Department of Anesthesiology, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 2Department of Anesthesiology, Chongqing Liangping District People’s Hospital, Chongqing, 405200, People’s Republic of China; 3School of Information and Software Engineering, University of Electronic Science and Technology of China, Chengdu, 610054, People’s Republic of China; 4West China Biomedical Big Data Center, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoqian Deng, Department of Anesthesiology, West China Hospital, Sichuan University, No. 37 Guoxue Alley, Chengdu, 610041, People’s Republic of China, Tel +86 885423592, Email [email protected]
Purpose: Malignant hyperthermia (MH) is a rare but fatal pharmacogenetic disorder, triggered by inhalational anesthetics or succinylcholine. Since the first nonprofit academic organization China Malignant Hyperthermia Emergency Assistance WeChat-based Group (CMHEA Group) was established in 2015, they have actively participated in the diagnosis and treatment of MH patients. Based on the CMHEA Group, the aim of the study was to retrospectively analyze the characteristics of suspected MH in China from 2015 to 2020.
Methods: We conducted a retrospective analysis of the suspected MH patients from 2015 to 2020, for analyzing the current clinical diagnosis, treatment and prognosis of MH in China.
Results: A total of 58 suspected MH cases occurred from 2015 to 2020, of these, 36 cases were collected with detailed data. The MH clinical grading score of 36 patients ranged from 33 to 73, with a median of 55. Abnormal hyperthermia and hypercarbia were the most common early signs of MH. Four patients were confirmed carrying six different potential MH-causative mutations. Of the total 58 cases, 14 patients (24.1%) received dantrolene and the whole mortality rate was 53.4%. Compared to the patients not receiving dantrolene treatment, the survival rate of patients receiving dantrolene treatment was significantly higher than that of patients not receiving dantrolene (78.6% vs 36.4%, p = 0.007).
Conclusion: The current main diagnostic methods of suspected MH in China are still clinical diagnosis. Hence, it is critical to keep dantrolene for immediate accessibility with the introduction of domestic dantrolene to China. The WeChat group model has played an important but limited role in quick diagnosis and treatment of MH.
Keywords: malignant hyperthermia, dantrolene, mortality, China
Introduction
Malignant hyperthermia (MH) is a rare pharmacogenetic disorder of skeletal muscle linked to mutations in RYR1 and CACNA1S genes, commonly triggered by volatile anesthetics or depolarizing muscle relaxants.1–5 Hence, MH is considered as one of the most severe anesthesia-related rare diseases associating with rapid progress and high mortality rate.6,7 Reported incidence of clinical MH episodes ranges from 1:35,000 to 1:68,000 in surgical patients.8,9 In recent years, about 200 million cases of general anesthesia are performed worldwide, and 15% of these are annually done in China.10 According to the reported incidence, there are hundreds of potential MH patients annually in China. It should be noted that the genetic prevalence of MH diagnostic mutations is considerably greater, and some possible explanations for the discrepancy might be the fact that many mutation carriers may never be exposed to anesthetic triggers in the whole life, and even when exposed to a triggering agent, not all carriers will develop an MH crisis.8,11,12
Previous studies indicated the mortality rate of MH in China could be as high as 73.5%.10,13,14 The striking high mortality may be due to the fact that few hospitals in China stored dantrolene.10 On the other hand, there is a major shortage of MH-related resources and most anesthesiologists have never received MH simulation training. Hence, anesthesiologists lack certain stock of MH relevant theoretical knowledge and are inexperienced in face of MH crisis.14 Moreover, owing to lack of professional MH organization or MH hotline in China, like the European Malignant Hyperthermia Group (EMHG) or the Malignant Hyperthermia Association of the United States (MHAUS), the great difficulties to obtain expert guidance from professionals in MH emergency worsen the situations.
Even so, Chinese anesthesiologists never give up their efforts. With the increasing popularities of smartphone, Chinese anesthesiologists are also exploring new ways for MH. WeChat app is one of the important Chinese communication tools for health education in the current “non-contact”, which has over 1 billion users in China and has the advantages of immediacy, interactivity, and convenience.15,16 WeChat group can be understood as Chinese version of online Facebook chatting groups. Therefore, the first nonprofit academic organization China Malignant Hyperthermia Emergency Assistance WeChat-based Group (CMHEA Group) was established in 2015, dedicated to providing emergent professional consultation and assisting dantrolene mobilization for Chinese anesthesiologists in case of suspicious MH emergencies. Currently, there are nearly 500 group members, covering more than 300 hospitals across the whole country. Over the past 5 years, members of CMHEA Group have actively participated in the diagnosis and treatment of 58 suspectable MH patients and managed to save patients’ lives.
Thus, we conducted a survey among the members of CMHEA Group, to retrospectively analyze the clinical diagnosis and treatment of Chinese MH patients from 2015 to 2020 and provide further information for the construction of National Remote Emergency System for MH.
Materials and Methods
Data Collection
This is a retrospective survey among the members of CMHEA Group, as all the cases have been reported previously to CMHEA Group. After obtaining approval from the Ethics Committee of West China Hospital, Sichuan University (protocol number 2021-1387), this online survey had been conducted among the medical staff from October to November 2021. This online questionnaire was designed in the form of a WeChat Mini Program that medical staff could use through the smart mobile phone to read the QR code and authorize a WeChat application to fill in and submit the questionnaire. The online questionnaire should be completed by anesthesiologist responsible for the rescue of MH patients. The main demographic variable was patients’ gender, age and personal and/or family history of MH. The other variables were types of surgery, anesthesia methods, choice of anesthetic drugs, clinical manifestation of MH, treatment of MH including use of dantrolene, patients’ prognosis and genetic analysis. Validity of suspected MH reactions is demonstrated with MH clinical grading score (CGS),17 which is considered as an aid to the objective definition of MH. However, CGS only represents a clinical diagnosis, and to confirm the MH susceptibility, the patient should receive a contracture test or a genetic test. The detailed questionnaire can be reached in the Supplementary Data.
Outcomes
The primary outcome of the retrospective study was the all-cause mortality rate of MH patients. The second outcomes included MH clinical grading scale, utilization of dantrolene and the impacts of dantrolene on patients’ prognosis.
Statistical Analysis
We use the statistical package program for social sciences version 25.0 (SPSS, IBM, Armonk, NK, USA) to perform all statistics. Pearson’s chi-square test was used to compare the categorical variables. Continuous variables were tested for normality of distribution. If normality was violated, the Mann–Whitney U-test was used (presented as median with interquartile range), and Un-paired Student’s t-test (presented as mean ± standard deviation) was used for normally distributed continuous variables. Statistical significance was defined as P < 0.05.
Results
Overall View and Characteristics of Suspected MH Cases
Finally, data pertaining to 58 MH cases gathered were exported from the program computer server. However, not all data were collected and reported for these 58 cases, 37 responses provided detailed information of 36 cases, and the rest 22 were incompletely filled owing to incomplete memories of respondents. Thus, we had a response rate of 62.1% (36/58), whereas the incomplete responses were not excluded as they still could offer adequate useful information. Therefore, some variables included less than 58 cases and some patients’ CGS points were underestimated or not estimated.
A total of 58 cases in this study involved 13 departments (Figure 1) and 23 different provinces or states in China. According to the 36 detailed responses, tertiary class-A hospital accounted for 83.3% (n = 30) MH patients. Thirty-six patients included 32 (88.9%) males and 4 (11.1%) female, 4 (11.1%) were aged 3 years or younger, 9 (25%) were children between 3 and 17 years, 21 (58.3%) were adults between 18 and 65 years, and 2 (5.6%) were seniors over 65 years, which indicated that MH was more common in males and young than in females and seniors, respectively (Table 1). Only one patient had family history of MH, and the rest had no family history.
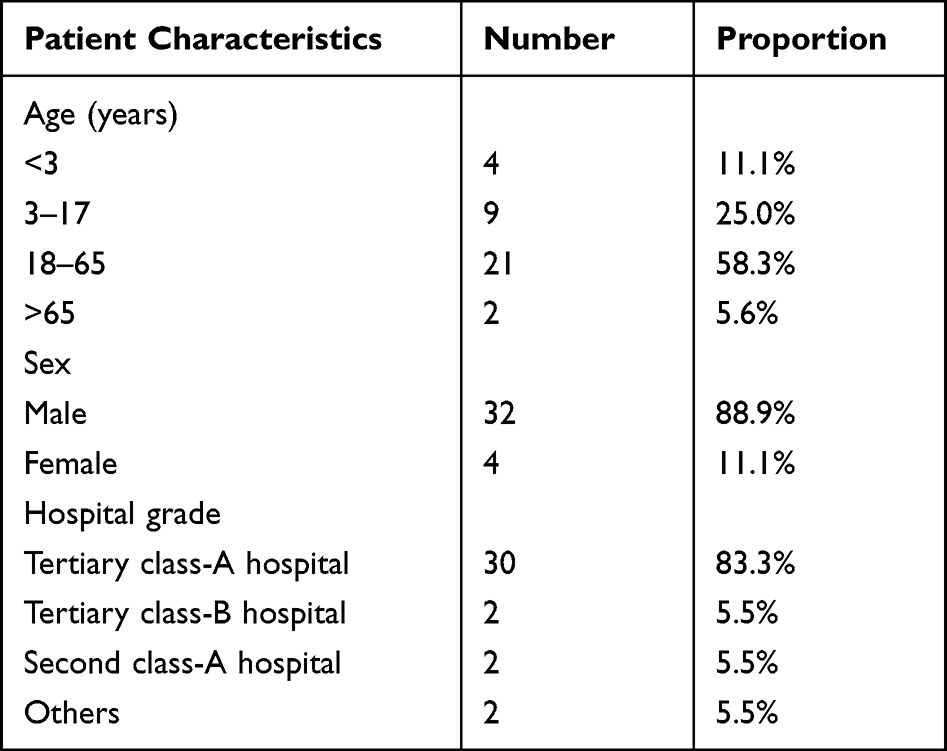 |
Table 1 Characteristics of Suspected MH Patients in China (n = 36) |
 |
Figure 1 Occurrence year of 58 suspected MH cases. |
Operative Associated Findings in Suspected MH Patients
Figure 2 shows the 13 types of surgery in 36 suspected MH patients. It was worth noting that ophthalmic and orthopedic procedures appeared to be the most common surgeries in children’s cases. Table 2 shows the onset stage and anesthetic choices of these patients. All underwent a surgical procedure with general anesthesia, of which, 34 patients accepted intravenous-inhalation combined anesthesia and 2 patients accepted simple inhalation anesthesia. Notably, succinylcholine was used in none of these 36 cases.
 |
Table 2 Onset Stage and Anesthetics of 36 Suspected MH Cases |
 |
Figure 2 Surgery types of 36 suspected MH cases. |
Clinical Signs of Suspected MH Cases
The MH clinical grading score of 36 patients ranged from 33 to 73, with a median of 55.21 (58.3%) cases were MH rank 6 representing the MH probability is almost certain. Ten (27.8%) cases were MH rank 5 representing the MH probability is very likely. Five (13.9%) cases were MH rank 4 representing the MH probability somewhat greater than likely. Table 3 shows the clinical signs of 36 patients. Abnormal hyperthermia and hypercarbia were the most common first signs in the early stage of MH. The maximum temperature of 36 patients ranged from 37.4° to 44°C with a median of 42°C. Significantly, 19 (52.8%) patients had hyperthermia of over 40°C for more than 2 hours. Muscular rigidity was specific signs of MH but not so sensitive. With the progress of condition, severe acidosis (PH <7.2) or hyperkalemia (K+ >6mmol/L) could be found in most cases (n = 24 and n = 31, respectively) owing to the development of rhabdomyolysis (n = 23).
 |
Table 3 Clinical Signs of Suspected MH Cases (n = 36) |
Diagnostic Test of Suspected MH Cases
Of the total cases, 4 patients took genetic testing and were confirmed carrying six different potential MH-causative mutations (Table 4). It is worth noting that two RYR1 variants (p.Pro1773Ser and p.Ile4196Thr) and one CACNA1S variant (Leu1800Ser) were founded in the same patient. Among them, there were two RYR1 variants (p.Ile4196Thr and Glu1732Lys) identified in two patients. These two rare variants are of unknown significance and have not been reported in association with MH. In other patients, the gene involved is still unknown. None of the patients underwent a muscle biopsy for caffeine-halothane contracture test immediately at the onset of MH, although it is the golden criteria of MH diagnosis.18
 |
Table 4 Analyses of RYR1 and CACNA1S Variants Reported in 4 Patients |
Association Between Dantrolene Treatment and Outcomes
Among the total 58 cases of suspected MH, dantrolene was administered in 14 patients. However, since most hospitals lacked quick access to dantrolene and only a few hospitals that stored dantrolene had abilities to offer a helping hand to those in urgent need of the specific drugs. Eventually, 31 patients unfortunately died of the MH episode and 27 patients were rescued successfully and survived, the whole mortality rate was 53.4%. Eleven patients survived in the 14 patients receiving dantrolene treatment, while 16 patients survived in the 44 patients not receiving dantrolene treatment, the survival rate of patients receiving dantrolene treatment was significantly higher than that of patients not receiving dantrolene (78.6% vs 36.4%, p = 0.007). In the subgroup analysis of 36 cases, these statistics could display a definite trend that with the extension of the time interval between MH episode and dantrolene administration, the survival rate of the patients decreased, although there was no statistical difference (p = 0.071, Figure 3). We also noted that, for the 3 patients who quickly received dantrolene, their temperature rapidly dropped to normal within one hour. By contrast, for the rest 11 patients who received delayed dantrolene, the hyperthermia remained for several hours.
 |
Figure 3 The association between administration time of dantrolene and outcomes. The increased time interval between the first signs of MH and dantrolene administration is associated with increased mortality (p = 0.071). |
Discussion
To our knowledge, this is the first retrospective study investigating the current diagnosis and treatment of MH in China, based on the Chinese Malignant Hyperthermia Emergency Help WeChat group. The whole mortality rate of MH patients was 53.4% in our research, which was lower than previous study in Chinese population (approximately up to 73.5%),13 however, obviously higher than that of Europe and the United States (approximately 11%).9 For one thing, the reduction in mortality was attributed to the positive rescue effect of the CMHEA Group. To a certain extent, expert advice from the WeChat group assisted the quick diagnosis of MH, and improved the standard treatment of MH. Furthermore, increasing utilization of dantrolene in China further improved prognosis of MH patients. In our study, 24.1% (14 of 58) patients received dantrolene, which increased obviously than previous reports (only 4 of 98).19 In addition, the survival rate of patients receiving dantrolene treatment was significantly higher than that of patients not receiving dantrolene (78.6% vs 36.4%, p = 0.007). It is undeniable that the WeChat group could optimize the mobilization of dantrolene and promote its utilization.
Our findings showed that MH trait was significantly higher in males compared with females (88.9% vs 11.1%), which are consistent with prior studies.8,9,20 On the whole, the pathomechanism leading to gender differences in the penetrance of MH is still unknown, it may be attributable that epigenetic RYR1 allele silencing has been ruled out as a cause of reduced penetrance of MH susceptibility in females.8,21 Different from earlier findings showing that children aged 12 or younger comprised more than 50% of all MH reactions,22 our results described that children aged 17 or younger accounted for 36.1% of all MH cases. Even so, it still implies that younger people might be most affected.
The results of this study suggest that the diagnosis of MH in China mainly depends on clinical diagnosis, and the median of MH clinical grading score of 36 patients was up to 55. Our results showed that abnormal hyperthermia and hypercarbia were the most common initial symptoms of MH, emphasizing the importance of body temperature monitoring and end-tidal dioxide monitoring. Whereas, in many Chinese hospitals, intraoperative body temperature monitoring and end-tidal carbon dioxide monitoring are still not routine, which was in urgent need of change. Only 4 patients who underwent genetic testing showed positive results associated with mutations in RYR1 and CACNA1S genes. At present, 48 RYR1 and 2 CACNA1S variants are recognized as MH-causative mutations.8 Besides, variants in SH3 and cysteine-rich domain 3 (STAC3) genes are also associated with MH.23,24 Our current genetic testing kit did not contain all known MH-diagnostic mutation sites, and the limitation of genetic detection method might underestimate the prevalence of MH susceptibility. Although over one hundred potentially pathogenic RYR1 variants were found in at least one independent MH family, a significant proportion of RYR1 sequence variants in the human gene mutation database classified as “disease-causing mutations” was found to be probably benign, or as being of unknown pathogenicity.11,12 The sensitivity of commonly used bioinformatics prediction tools for RYR1 and CACNA1S has been estimated 46 at 84–100% with specificity of 25%–83%.12 The good news is that the development of next-generation sequencing technologies provides another powerful method for MH diagnosis.25 Furthermore, a recent study identified that transient receptor potential vanilloid 1 (TRPV1) variants contribute to the sarcoplasmic reticulum Ca2+-release/Ca2+-leak mechanism and highlight a potential actionable therapeutic target of MH.26 While muscle biopsy and caffeine-halothane contracture testing are the gold standard of MH diagnosis, the extremely low incidence of MH limits its application and owing to this, the diagnosis of MH in China highly relies on clinical diagnosis. Consequently, we need to strengthen the training of MH clinical diagnosis.
The outcome determining factors is the time interval from the onset of MH reaction to establishment of correct treatment, including terminating the trigger agent exposure and administering dantrolene.3 Nevertheless, our results suggest that only 3 patients quickly received dantrolene after MH episode. Furthermore, with the delay of dantrolene administration, the survival rate of the patients decreased although not statistically different. The fact is far away from the recommendation of the MHAUS that dantrolene should be immediately available (for administration within 10min) in operating room areas.27,28 Indeed, as the only disease-specific drug available for MH, lack of IV dantrolene in most Chinese hospitals is the major problem in MH treatment.14,29 Only few hospitals in China stored IV dantrolene because of the high cost and low utilization. In addition, the imported IV dantrolene was not on the list of government-approved drugs in China in the past years. Fortunately, domestic IV dantrolene was produced by a Chinese pharmaceutical company (Livzon Pharmaceutical Group Co., Ltd, Zhuhai, China) and approved by the Chinese Food and Drug Administration (CFDA) in October 2020. With the introduction of domestic dantrolene to China, it is critical to keep dantrolene for immediately accessible in anesthesia sites, and we are hopeful that the mortality of MH could dramatically reduce. An alternative to make dantrolene more available in more hospitals may be that the manufacturers can produce and offer smaller containers of dantrolene. This may reduce costs and limit the waste of unused product.
The prognosis of an MH crisis depends on how soon MH is suspected and how fast treatment is initiated. The WeChat group has improved the treatment efficiency of MH. However, this model may be insufficient to promote in clinic in face of increasing MH crisis. First, this group can only accommodate 500 members from 300 hospitals, and the limited capacity limits the inclusion of more grass-roots hospital. Meanwhile, Chinese grass-roots hospitals are exactly in more need of help, owing to poor infrastructure and facilities, and little experience. Secondly, the critical messages for help could likely be ignored by other irrelevant messages. Similarly, the help seekers also need to extract effective suggestion from a large number of messages, which seems time-consuming. Last but not least, sometimes no one responds to the emergencies in the group, due to the incapability of automatic alerts. Therefore, a more real-time and effective emergency system for MH is urgently needed in China.
Telephone hotlines for MH counselling and management guidelines have been established in many countries. A smartphone application issued by the EMHG in cooperation with the MHAUS can also provide direction to MH management.25 In China, we plan to develop a system national remote emergency system for MH based on an applet of the WeChat app. Unlike WeChat group, which was characterized by communication convenience, WeChat app focuses on tool-based services, which means it can implement more functionality than WeChat group.30–32 Moreover, medical staff could find this system quickly through searching this applet in WeChat without taking time to download a new app, especially in the rescue, race against time. We are confident that if well designed, the applet can achieve the key functions including quick auto-diagnosis, rapid initiation of MH treatment and dantrolene mobilization, and ultimately improve the management of MH in China.
There are limitations inherent to our study design. Data collection was retrospective and based on questionnaire, carrying the risk of recall bias. Second, some patients’ data were missing, and the features of small sample limits this study. Still and all, as the first retrospective study based on CMHEA WeChat Group we analyzed the current diagnosis and treatment of MH in China, discussed the strength and flaws of WeChat group model, and explored the future possible model for MH management in China.
Conclusions
From 2015 to 2020, the current diagnostic methods of MH in China are mainly clinical diagnosis. Early use of dantrolene can decrease the mortality of MH, but few hospitals in China stored dantrolene. Nowadays, it is critical to keep dantrolene for immediate accessibility with the introduction of domestic dantrolene to China. The WeChat group model has played an important but limited role in diagnosis and treatment of MH, and future possible models for quick and comprehensive MH management are worthy of exploration.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to individual privacy of the patients included but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of West China Hospital, Sichuan University (protocol number 2021-1387). Due to the retrospective nature of the study, which did not involve patient privacy, did not harm patients’ health and did not pose any risk to anesthesiologists participating in the survey, the board waived the need for patient written consent. The study was conducted in compliance with the Declaration of Helsinki principles, and all personal information would be kept confidential.
Consent for Publication
All the authors included signed the consent for publication.
Acknowledgments
We would like to acknowledge the membership of China Malignant Hyperthermia Emergency Assistance WeChat-based Group for their assistance in completing the questionnaires. Lingcan Tan and Yi Teng are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The project is supported by the National Natural Science Foundation of China (No.72074162) and the 1.3.5. Project for Disciplines of Excellence, West China Hospital, Sichuan University (No. 2018HXFH006).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rosenberg H, Pollock N, Schiemann A, Bulger T, Stowell K. Malignant hyperthermia: a review. Orphanet J Rare Dis. 2015;10:1–19. doi:10.1186/s13023-015-0310-1
2. de Correia AC, Silva PCB, da Silva BA. Malignant hyperthermia: clinical and molecular aspects. Rev Bras Anestesiol. 2012;62:820–837. doi:10.1016/S0034-7094(12)70182-4
3. Broman M, Islander G, Müller CR. Malignant hyperthermia, a Scandinavian update. Acta Anaesthesiol Scand. 2015;59:951–961. doi:10.1111/aas.12541
4. Julien Marsollier F, Roux-Buisson N, Dalmas AF, Bruneau B, Dahmani S. Management of malignant hyperthermia in France: current organisation. Anaesthes Crit Care Pain Med. 2019;38:535. doi:10.1016/j.accpm.2019.02.008
5. Litman RS, Smith VI, Larach MG, et al. Consensus statement of the malignant hyperthermia association of the United States on unresolved clinical questions concerning the management of patients with malignant hyperthermia. Anesth Analg. 2019;128:652–659. doi:10.1213/ANE.0000000000004039
6. Rüffert H, Bastian B, Bendixen D, et al. Consensus guidelines on perioperative management of malignant hyperthermia suspected or susceptible patients from the European Malignant Hyperthermia Group. Br J Anaesth. 2021;126:120–130. doi:10.1016/j.bja.2020.09.029
7. Jones PM, Allen BN, Cherry RA, et al. Association between known or strongly suspected malignant hyperthermia susceptibility and postoperative outcomes: an observational population-based study. Can J Anesth. 2019;66:161–181. doi:10.1007/s12630-018-1250-8
8. Ibarra Moreno CA, Hu S, Kraeva N, et al. An assessment of penetrance and clinical expression of malignant hyperthermia in individuals carrying diagnostic ryanodine receptor 1 gene mutations. Anesthesiology. 2019;131:983–991. doi:10.1097/ALN.0000000000002813
9. Lu Z, Rosenberg H, Li G. Prevalence of malignant hyperthermia diagnosis in hospital discharge records in California, Florida, New York, and Wisconsin. J Clin Anesth. 2017;39:10–14. doi:10.1016/j.jclinane.2017.03.016
10. Li Z, Liu K, Guo X. Dantrolene available in china for malignant hyperthermia treatment. Anesthesiology. 2022;136:515–516. doi:10.1097/ALN.0000000000003998
11. Riazi S, Kraeva N, Hopkins PM. Malignant hyperthermia in the post-genomics era: new perspectives on an old concept. Anesthesiology. 2018;128:168–180. doi:10.1097/ALN.0000000000001878
12. Miller DM, Daly C, Aboelsaod EM, et al. Genetic epidemiology of malignant hyperthermia in the UK. Br J Anaesth. 2018;121:944–952. doi:10.1016/j.bja.2018.06.028
13. Wang YL, Luo AL, Tan G, Cui XL, Guo XY. Clinical features and diagnosis for Chinese cases with malignant hyperthermia: a case cluster from 2005 to 2007. Chin Med J. 2010;123:1241–1245.
14. Belani KG, Cao C, Daugherty D, et al. Malignant hyperthermia status in China. Anesth Analg. 2016;122:574–577. doi:10.1213/ANE.0000000000001043
15. Hu X, Li X, Lü Y, Tang J, Li HR, Tang M. Effect of WeChat consultation group on residents staying at home in Sichuan and Chongqing regions during the Coronavirus Disease 2019 (COVID-19) outbreak in China: a cross-sectional study. BMC Public Health. 2020;20:1–9. doi:10.1186/s12889-020-09951-4
16. Montag C, Becker B, Gan C. The multipurpose application WeChat: a review on recent research. Front Psychol. 2018;9:1–8. doi:10.3389/fpsyg.2018.02247
17. Larach MG, Localio AR, Allen GC, et al. A clinical grading scale to predict malignant hyperthermia susceptibility. Anesthesiology. 1994;80:771–779. doi:10.1097/00000542-199404000-00008
18. Bendahan D, Guis NM, Kozak-Ribbens G, et al. Comparative analysis of in vitro contracture tests with ryanodine and a combination of ryanodine with either halothane or caffeine: a comparative investigation in malignant hyperthermia. Acta Anaesthesiol Scand. 2004;44:1019–1027. doi:10.1111/j.0001-5172.2004.00461.x
19. Fang Y, Wu JB, Ding ZN. Clinical analysis of malignant hyperthermia reported cases from 1970 to 2017 in China. Jiangsu Med. 2018;44:843–846.
20. Pinyavat T, Henry Rosenberg BH, Lang CAW, Sheila Riazi JE, Brady LS, Sun GL. Accuracy of malignant hyperthermia diagnoses in hospital discharge records. Anesthesiology. 2015;122:55–63. doi:10.1097/ALN.0000000000000467
21. Rutkowsky JM, Knotts TA, Allen PD, Pessah IN, Ramsey JJ. Sex-specific alterations in whole body energetics and voluntary activity in heterozygous R163C malignant hyperthermia-susceptible mice. FASEB J. 2020;34:8721–8733. doi:10.1096/fj.202000403
22. Klingler W, Heiderich S, Girard T, et al. Functional and genetic characterization of clinical malignant hyperthermia crises: a multi-centre study. Orphanet J Rare Dis. 2014;9. doi:10.1186/1750-1172-9-8.
23. Horstick EJ, Linsley JW, Dowling JJ, et al. Stac3 is a component of the excitation-contraction coupling machinery and mutated in Native American myopathy. Nat Commun. 2013;4. doi:10.1038/ncomms2952
24. Polster A, Nelson BR, Olson EN, Beam KG. Stac3 has a direct role in skeletal muscle-type excitation-contraction coupling that is disrupted by a myopathy-causing mutation. Proc Natl Acad Sci U S A. 2016;113:10986–10991. doi:10.1073/pnas.1612441113
25. Yang L, Tautz T, Zhang S, Fomina A, Liu H. The current status of malignant hyperthermia. J Biomed Res. 2020;34:75–85. doi:10.7555/JBR.33.20180089
26. Vanden AF, Lotteau S, Ducreux S, et al. TRPV1 variants impair intracellular Ca 2+ signaling and may confer susceptibility to malignant hyperthermia. Genet Med. 2019;21:441–450. doi:10.1038/s41436-018-0066-9
27. Ho PT, Carvalho B, Sun EC, Macario A, Riley ET. Cost-benefit analysis of maintaining a fully stocked malignant hyperthermia cart versus an initial dantrolene treatment dose for maternity units. Anesthesiology. 2018;129:249–259. doi:10.1097/ALN.0000000000002231
28. Guglielminotti J, Rosenberg H, Li G. Prevalence of malignant hyperthermia diagnosis in obstetric patients in the United States, 2003 to 2014. BMC Anesthesiol. 2020;20. doi:10.1186/s12871-020-0934-0
29. Changsheng H, Ahn Wonsik GQ, Guo Q. Current state of malignant hyperthermia in China mainland: a less optimistic reality. Paediatr Anaesth. 2012;22:503–504. doi:10.1111/j.1460-9592.2011.03774.x
30. Wang X, Tao J, Zhu Q, et al. Depression and anxiety symptoms to COVID-19 outbreak among the public, medical staff and patients during the initial phase of the pandemic: an online questionnaire survey by a WeChat Mini Program. BMJ Open. 2021;11:115.
31. Ding Y, Lu X, Xie Z, Jiang T, Song C, Wang Z. Evaluation of a novel wechat applet for image-based dietary assessment among pregnant women in China. Nutrients. 2021;13:3158. doi:10.3390/nu13093158
32. Li Q, Deng X, Yan J, et al. Neonatal severe hyperbilirubinemia online registry in Jiangsu Province: protocol for a multicentre, prospective, open, observational cohort study. BMJ Open. 2021;11:1–7.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.