Back to Journals » Cancer Management and Research » Volume 12
Clinical Features and Prognostic Factor of Thoracic Postoperative Oligo-Recurrence of Non-Small-Cell Lung Cancer
Authors Yuan Q, Wang W, Zhang Q, Wang Y, Chi C, Xu C
Received 10 September 2019
Accepted for publication 17 February 2020
Published 25 February 2020 Volume 2020:12 Pages 1397—1403
DOI https://doi.org/10.2147/CMAR.S230579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sanjeev K. Srivastava
Qi Yuan, 1–3 Wei Wang, 1–3 Qian Zhang, 1–3 Yuchao Wang, 1–3 Chuanzhen Chi, 1–3 Chunhua Xu 1–3
1Endoscopic Center of the Affiliated Brain Hospital of Nanjing Medical University, Nanjing, Jiangsu 210029, People’s Republic of China; 2Clinical Center of Nanjing Respiratory Diseases and Imaging, Nanjing, Jiangsu 210029, People’s Republic of China; 3Department of Respiratory Medicine, The Affiliated Brain Hospital of Nanjing Medical University, Nanjing, Jiangsu 210029, People’s Republic of China
Correspondence: Chunhua Xu
Department of Respiratory Medicine, The Affiliated Brain Hospital of Nanjing Medical University, 215 Guangzhou Road, Nanjing 210029, People’s Republic of China
Email [email protected]
Objective: The study aimed to clarify clinical features and prognostic factors of thoracic oligo-postoperative recurrences that underwent local therapy of non-small-cell lung cancer (NSCLC).
Methods: From 2332 patients of resected pathological stage I–IIIA NSCLC between 2008 and 2015, a total of 542 patients in follow developed recurrence. Thoracic oligo-recurrence was defined as 1– 3 loco-regional confined to lung lobe, hilar/mediastinal lymph nodes, bronchial stump, or chest wall. This study included 56 thoracic oligo-recurrences. Local therapy included secondary surgery, stereotactic radiotherapy, radiotherapy with a 45 Gy or higher dose, and proton radiation therapy, performed with radical intent. We retrospectively reviewed the postoperative data and performed the univariate and multivariate analysis by Kaplan-Meier methods and Cox regression models, respectively.
Results: Thoracic Oligo-recurrence was identified in 56(542,10.3%) patients, mainly in lung lobe(n=22,39%) and regional lymph nodes(n=19,34%). Compared with distant oligo-recurrences, more of the thoracic oligo-recurrences were II–III in pathological stage at initial surgery(p=0.002) and less were adenocarcinoma(p=0.005). The 5-year postoperative survival rate and postoperative progression-free survival rate of thoracic oligo-recurrence were 10.8% and 6.7%, respectively. Median post-recurrence survival (PRS) was 31 months, and the median postoperative progression-free survival (PR-PFS) was 17 months. Multivariate analyses revealed that time to recurrence ≥ 12 months was associated with improved PRS [odds ratio (OR) 0.74, confidence interval (CI) 0.65– 0.85], and regional lymph node oligo-recurrence was associated with poor PRS [OR 1.48, CI 1.38– 1.60]. All the five long-term (≥ 5-year) progression-free survivors were with a solitary pulmonary recurrence.
Conclusion: Thoracic postoperative oligo-recurrence of non-small-cell lung cancer is a limited but highly heterogeneous population, with different prognosis at different recurrence sites. Local therapy for thoracic oligo-recurrence of NSCLC achieved favourable PRS in a selected population. Pulmonary solitary oligo-recurrence may achieve a long survival time.
Keywords: oligo-recurrence, NSCLC, postoperative recurrence, local therapy
Introduction
In general, the standard and recommended treatment for early non-small cell lung cancer (NSCLC) is radical surgical resection;1 however, postoperative recurrence limited the overall survival after radical resection, and the overall 5-year survival is less than 50%.2 80% of recurrences occurred within two years after surgery, and the median survival after recurrence was approximately 11.5 months.3 Postoperative follow-up revealed that some of the recurrences presented as the limited number of local lesions termed oligo-recurrence.4 The definition was initially proposed by Niibe and colleagues in 2006 as an intermediate state of cancer spread between localized and widespread situation after the primary lesion has been controlled.5–7 Patients with oligo-recurrence show a better prognosis than those with extensive metastasis, and about 25% of them can achieve long-term survival after clearing all metastatic lesions.7
For oligo-recurrence lesions in distant organs such as the brain, liver, and adrenal gland, secondary surgical resection, or local radical radiotherapy, has been generally accepted.8,9 Thoracic oligo-recurrence lesions often come with anatomical structure change, high incidence of complications, and the low willingness of patients to undergo surgery again, making secondary surgery difficult. Meanwhile, the sites of oligo-recurrences in the chest may be complicated, and the recurrent lesions may be in the lung lobes, chest wall, bronchial stump, or hilar/mediastinal lymph nodes. For these patients, there is currently no clear consensus on the most appropriate treatment, but local radiotherapy with or without chemotherapy may be a more common treatment option. In this study, we summarized the local treatment mode of patients with thoracic oligo-recurrence after radical resection of non-small cell lung cancer, their survival data, compared the efficacy of treatment with that of distant recurrence, and analyzed the characteristics of the patients that benefited the most.
Patients and Methods
Patient Inclusion and Treatment
Retrospectively, a total of 2039 patients underwent lobectomy and mediastinal lymph node dissection in Nanjing Chest Hospital of histologically proven NSCLC stage I–IIIA (according to the 7th American Joint Committee on Cancer 7th edition Tumor Node Metastasis [TNM] staging system) between 2009 and 2014. The ethics committee of Nanjing Brain Hospital Affiliated to Nanjing Medical University approved this study. We provided the written informed consent to all enrolled patients. Examinations performed on patients suspected of recurrence included chest enhanced computed tomography(CT), whole-body bone scanning, head enhanced magnetic resonance imaging(MRI), abdominal plain CT, or positron emission tomography/computed tomography (PET/CT). We performed CT guided percutaneous needle lung biopsy (PNLB), bronchoscopy, or endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) for definite pathological diagnosis when possible. Considering that PET/CT cannot differentiate tuberculosis and sarcoidosis from a tumour, we also performed a tuberculin(PPD) test, tuberculosis antibody, and angiotensin converting enzyme(ACE) examination. Sometimes it is challenging to distinguish sarcoidosis and mediastinal lymph node recurrence. To these patients, we may follow up to observe the dynamic changes of the lesion rather than immediately start treatment, and we considered the lesions which did not change or shrink benign during radiologic surveillance.
Inclusion criteria: in this study, we defined oligo-recurrence as 1–3 localized recurrent lesions in a single organ. The thoracic oligo-recurrence confined in the pulmonary lobe, bronchial stump, regional lymph node, and chest wall. At the same time, distant oligo-recurrence was recurrence in the brain, adrenal gland, liver, skin, and other extra-thoracic organs, also including simultaneous recurrences in both lungs. A regional lymph node zone was classified as a single organ. We excluded patients if they: (i) were diagnosed as second primary lung cancers (SPLCs) by experienced pathologists based on the criteria by Martini and Melamad,10 and metachronous intrapulmonary nodules with ground-glass attenuation on chest CT suspected as SPLC but histologically unproved; (ii) underwent sub-lobar resection; (iii) were poly-recurrences(n=423). This retrospective study finally included 56 thoracic oligo-recurrences and 63 distant oligo-recurrences.
Radical local therapy for thoracic oligo-recurrence patients mainly included secondary surgical resection, stereotactic radiotherapy (SBRT), conventional radiotherapy with total therapeutic dose ≥45Gy, and proton beam radiotherapy (PBT). The mode of chemotherapy included adjuvant chemotherapy and neoadjuvant chemotherapy, both with a platinum-based combination chemotherapy regimen. The remaining patients who did not receive radical local therapy were access to other treatments, including systemic chemotherapy, molecular targeted therapy, local palliative radiotherapy, and best support curative therapy (BSC). The reasons for not receiving local therapy include: (i) the location of the lesions not suitable for radiotherapy or surgery; (ii) deficient Eastern Cooperative Oncology Group performance status or lung function; (iii) patient refused for financial or personal reasons.
Follow-Up After Initial Surgery and Recurrence
The patients were followed up every six months in the first two years after surgery and every one year 3 to 5 years after surgery. Auxiliary examinations mainly included blood tumour markers, chest and abdominal CT scan, head enhanced MRI or B-ultrasound. Patients with suspected recurrence took the above examinations to confirm the diagnosis. Cases with oligo-recurrences in the chest were evaluated every 2–3 months after surgery to evaluate the efficacy; the evaluation criteria based on the Response Evaluation Criteria In Solid Tumors (RECIST), version 1.1.
Statistical Analysis
The count data were expressed as n (%), t-test was used for comparison between two sets of normal-distribution continuous variables, and Mann–Whitney U two-sample rank-sum test was used for comparison of non-parametric data. Categorical data were compared using Pearson’s χ2 test. Survival curves, including PRS and PR-PFS, were constructed using the Kaplan-Meir method, and differences in groups were compared using the Log rank test. Prognostic factors for PRS were evaluated using univariate and multivariate Cox regression analysis, with age, gender, histology, initial pathological stage, regional lymph node recurrence, time to recurrence, as the candidate factors. P < 0.05 was considered statistically significant. We used SPSS for Windows version 17 (SPSS, Chicago, IL) for statistical analyses.
Result
Clinical Features of Thoracic and Distant Oligo-Recurrence
Table 1 shows the clinical features of thoracic oligo-recurrences and distant oligo-recurrences. Compared with distant oligo-recurrence, the thoracic recurrences showed a significantly higher proportion of non-adenocarcinoma (p=0.044), a higher rate of stage II–IIIA (p=0.046), and a higher rate of postoperative adjuvant chemotherapy (p=0.016). There were no differences in age and gender between the two groups. A total of 81 patients accepted EGFR gene detection of surgical specimens, no significant difference was detected between the thoracic recurrences (43%) and distant ones (51%). No significant difference in survival was detected between the two groups after recurrence (p=0.785, Figure 1A). Median 5-year survival time and 5-year survival rate after recurrence were 36 months and 10.8% in the thoracic oligo-recurrence group, and 37 months and 19.5% in distant oligo-recurrence group.
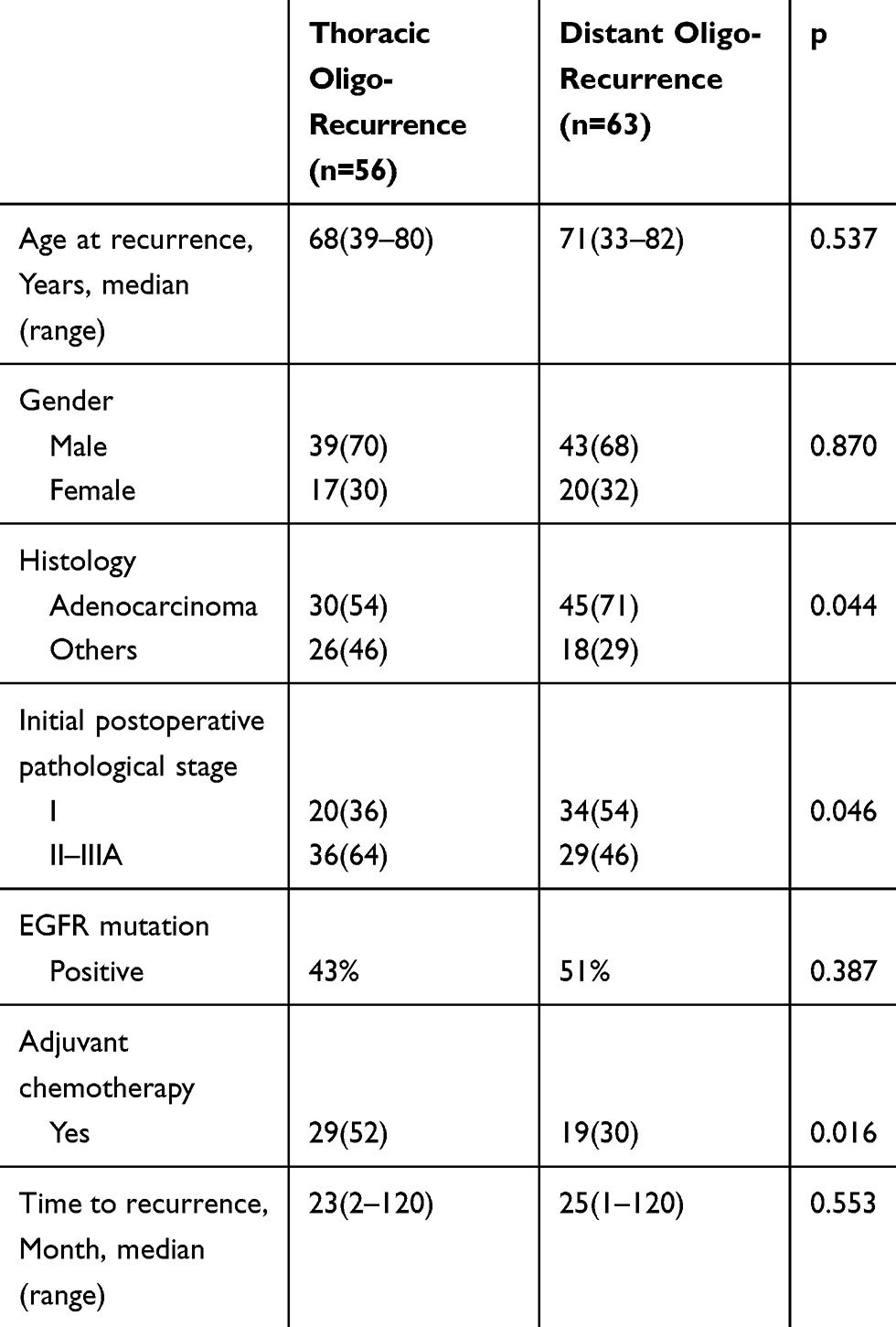 |
Table 1 Characteristics of Patients with Thoracic and Distant Postoperative Oligo-Recurrence |
 |
Figure 1 (A) PRS and (B) PR-PFS curves of the patients with thoracic and distant postoperative oligo-recurrence. (A) PRS curves curves are not statistically different between thoracic and distant postoperative oligo-recurrence. (B) PR-PFS curves of the patients with thoracic and distant postoperative oligo-recurrence. The patients with distant oligo-recurrence show significantly better PR-PFS than those with thoracic oligo-recurrence. Abbreviations: PRS, post-recurrence survival; PR-PFS, postoperative progression-free survival. |
Clinical and Treatment Profiles of the Patients with Thoracic Oligo-Recurrence
Among the 56 cases with thoracic oligo-recurrence, the most common sites of recurrence was the ipsilateral or contralateral lobes (n=22, 39%), followed by the hilar or hilar/mediastinal lymph nodes (n=19, 34%), the bronchial stump (n=13, 23%), and chest wall where drainage tube located in 2 patients. Table 2 shows the treatment modes for different recurrence sites. Among the patients, 46(82%) received local therapy alone or in combination with adjuvant or neoadjuvant chemotherapy. Local treatments were different according to recurrence sites. All recurrence in local lymph nodes received local radiotherapy (n=19), most intra-pulmonary oligo-recurrences received secondary surgery and stereotactic radiotherapy (n=17, 77%), 2 cases of recurrence in the lobes received proton radiation therapy.
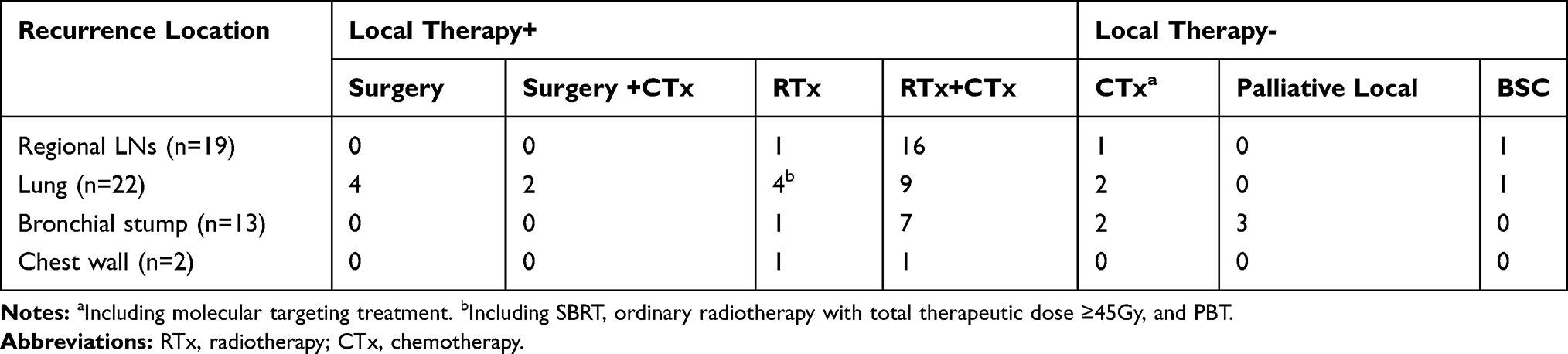 |
Table 2 Treatment for Thoracic Oligo-Recurrences According to Recurrence Location |
Survival and Prognostic Factors for Thoracic Oligo-Recurrence
The 3-year and 5-year survival rates after recurrence were 50.9% and 10.8% in the thoracic oligo-recurrence group and 48.7% and 19.5% in the distant oligo-recurrence group, respectively, with no significant differences between the two groups (p=0.785, Figure 1A). All post-recurrence progression occurred in 99 of the cases during the follow-up, most commonly in the primary recurrence site (n=64, 65%). The 3-year and 5-year progression-free survival rates and median progression-free time were 18.8%, 6.7%, 16 months in the thoracic oligo-recurrence group and 33.5%, 14.2%, and 27 months in the distant oligo-recurrence group, respectively. The progression-free time of the thoracic group was significantly shorter than the distant group (p=0.029, Figure 1B). The five patients in the thoracic recurrence group who survived for more than five years all had a solitary recurrent lesion in the lung lobe.
The prognostic factors for total survival time after recurrence were analyzed by univariate and multivariate regression analysis, with age, gender, histological type, initial surgical stage, time to recurrence and regional lymph node recurrence, as candidate risk factors. The results, as shown in Table 3, suggest that regional lymph nodes recurrence and time to recurrence ≥12 months were significant risk factors. Time to recurrence ≥12 months was associated with improved PRS [odds ratio(OR) 0.74, confidence interval(CI) 0.65–0.85], and regional lymph node oligo-recurrence was associated with poor PRS [OR 1.48, CI 1.38–1.60]. Although younger patients showed longer post-recurrence survival than the elder ones, the differences were not significant. None of the other factors had apparent effects on total survival time.
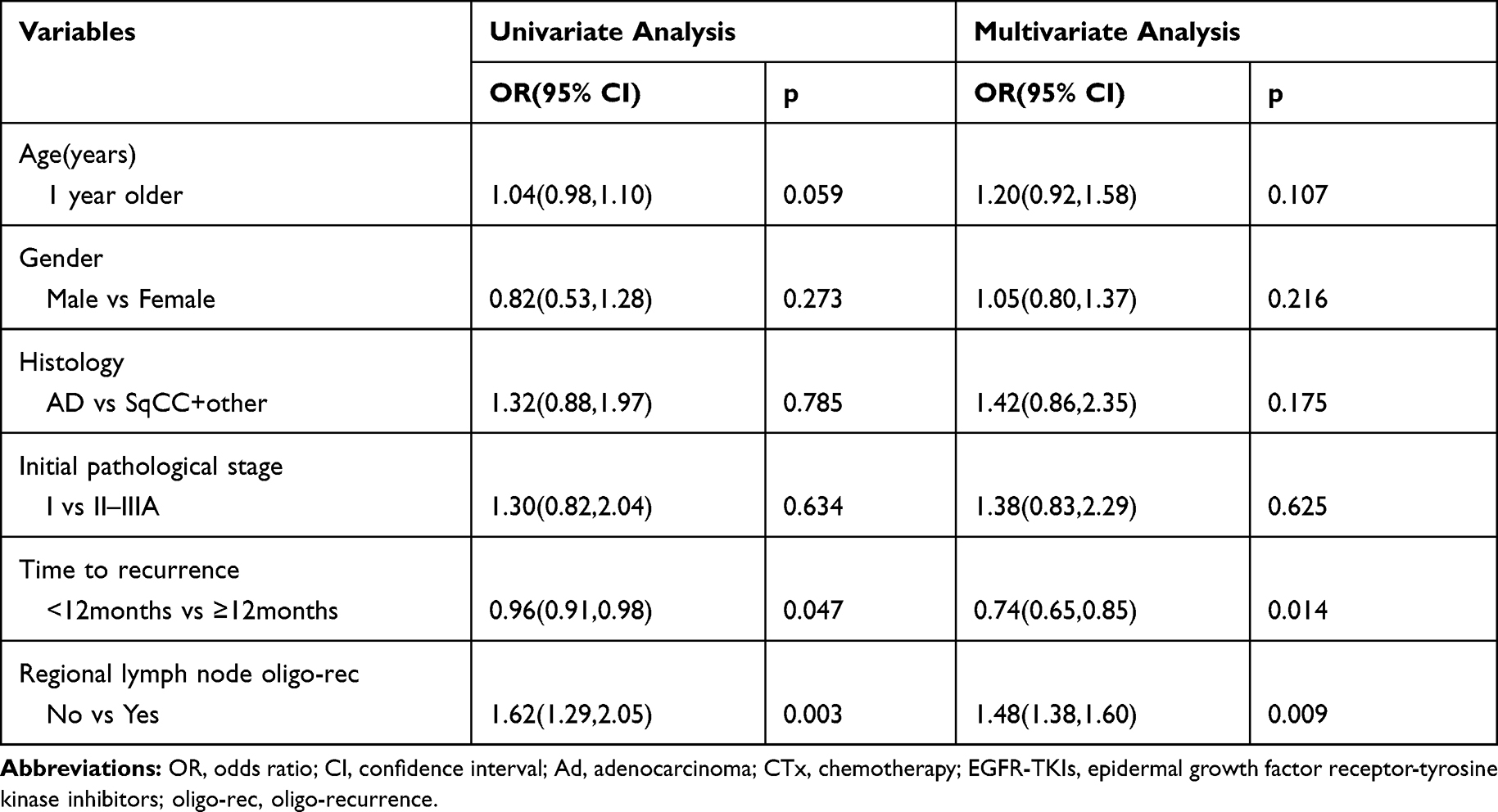 |
Table 3 Prognostic Factors Associated with Post-Recurrence Survival After Thoracic Oligo-Recurrence (Univariate and Multivariate Analysis) |
Discussion
With the popularization of lung cancer screening and the development of imaging technology, more patients with lung cancer have been discovered early and have the opportunity to undergo radical surgery. A small number of patients have oligo-recurrence after surgery, and these patients may achieve long-term survival after radical treatment of the recurrent lesion. The longest recorded survival time after relapse was 9.8 years,11 and for oligo-recurrence lesions in the brain, liver and adrenal glands, surgical resection, or local radical radiotherapy have been well recognized. Re-excision of the thoracic recurrence has been difficult due to pleural adhesion and dense scar after primary surgery and post-surgery radiotherapy and chemotherapy, so the technical requirements are high. Besides, a considerable number of patients were not willing to undergo chest surgery again, and local radiotherapy alone or in combination chemotherapy represents a more common choice for these patients.
This study retrospectively reviewed 543 cases of recurrence of lung cancer after radical resection in our hospital, including 119 cases (21.9%) of oligo-recurrences, most commonly in the brain, regional lymph nodes, lungs, adrenal glands, which were generally in line with previous researches.12,13 Among the patients with oligo-recurrence, 56 cases had thoracic oligo-recurrences mainly located in the lung lobe, regional lymph nodes, bronchial stump, and chest wall. Only five patients with isolated lung recurrence underwent radical surgery, and 40 patients underwent local radiotherapy alone or in combination with systemic chemotherapy.
Compared with patients with distant oligo-recurrence, patients with thoracic oligo-recurrence had a higher proportion of non-adenocarcinoma, and postoperative staging was relatively advanced, and more often received postoperative adjuvant chemotherapy, possibly reflecting the more advanced postoperative staging of the thoracic oligo-recurrence group. Radical surgery could not remove tumour cells in circulating blood, lymphatic tissue fluid, or surrounding tissues that had not formed detectable lesions, and these cells are responsible for recurrences near or distant from the resected primary tumour. More advanced TNM staging is an independent factor for local recurrence,14 so it was suspected that some of the thoracic recurrences were due to incomplete resection of the primary tumour, and in a manner different in the mechanism from that of the distant recurrences as spatiotemporal heterogeneous synchronous metastasis.
3-year PR-PFS rate and 5-year PR-PFS rate were 18.8% and 6.7% in the thoracic group, and 33.5% and 14.2% in the distant group, respectively, and two groups of data were all statistically different. The overall survival time of oligo-recurrences was shorter than that reported in foreign literature,9,11,15 possibly because of a lower rate of local radiotherapy treatment in this group of patients, which was due to unwillingness of the patients and lung function status failing to achieve the standard for radiotherapy. In the current study, no significant difference has been observed in survival time between the thoracic recurrence cases and the distant ones. The difference in PR-PFS after recurrence in this study may be mainly due to the difference in pathological type and staging.
Multivariate regression analysis showed that recurrence-free interval and regional lymph node recurrence were the prognostic factors affecting thoracic oligo-recurrence cases, which was consistent with previous results.9 This study did not find the benefits of local treatment combined with chemotherapy for patients with oligo-recurrence, and available studies have not concluded as to whether chemotherapy is needed after topical treatment, further stratified analysis based on the characteristics of the group of patients who benefited from the therapy would be required.
There are some limitations to the current study. First, the number of registered patients is limited to 56 subjects. At present, there are few clinical studies on oligo-recurrence after lung cancer surgery, and most of them are small sample studies, mostly due to the proportion of patients with oligo-recurrence after surgery is low in all surgical patients. Second, this study is a single-center retrospective analysis of a small sample, which may affect the accuracy of the multi-factor analysis. Third, a definite diagnosis of recurrence by clinically without pathology is not always possible. Therefore, the number of disease recurrences is not absolute accuracy. This inaccuracy is the crucial weak point for this study. Besides, the two sets of data were unbalanced distributed in three clinical features, including histology, initial postoperative pathological stage, and adjuvant chemotherapy. The sample size of thoracic group and distant group in the study were too small to do propensity score matching to pick more suitable samples. The thoracic group showed a higher proportion of non-adenocarcinoma, stage II–IIIA, and the rate of postoperative adjuvant chemotherapy. The three variables above are related to a worse prognosis. Our study found no difference in overall survival between the two groups. Due to the existence of three unbalanced clinical variables related to worse prognosis between the two groups, we speculated that the survival of the thoracic group would be better than that of the distant group.
Conclusion
Thoracic postoperative oligo-recurrence of non-small-cell lung cancer is a limited but highly heterogeneous population, with different prognosis at different recurrence sites. Local therapy for thoracic oligo-recurrence of NSCLC achieved favourable PRS in a selected population. Pulmonary solitary oligo-recurrence may achieve a long survival time.
Data Sharing Statement
The data described in this article are openly available in the Open Science Framework at DOI:10.17605/OSF.IO/TPA6U.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Howington JA, Blum MG, Chang AC, et al. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e278S–e313S. doi:10.1378/chest.12-2359
2. Goldstraw P, Chansky K, Crowley J, et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (Eighth) Edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11(1):39–51. doi:10.1016/j.jtho.2015.09.009
3. Ichinose Y, Yano T, Yokoyama H, et al. Postrecurrent survival of patients with non-small-cell lung cancer undergoing a complete resection. J Thorac Cardiovasc Surg. 1994;108(1):158–161. doi:10.1016/S0022-5223(94)70233-0
4. Yano T, Okamoto T, Haro A, et al. Local treatment of oligometastatic recurrence in patients with resected non-small cell lung cancer. Lung Cancer. 2013;82(3):431–435. doi:10.1016/j.lungcan.2013.08.006
5. Niibe Y, Kenjo M, Kazumoto T, et al. Multi-institutional study of radiation therapy for isolated para-aortic lymph node recurrence in uterine cervical carcinoma: 84 subjects of a population of more than 5000. Int J Radiat Oncol Biol Phys. 2006;66(5):1366–1369. doi:10.1016/j.ijrobp.2006.07.1384
6. Niibe Y, Kazumoto T, Toita T, et al. Frequency and characteristics of isolated para-aortic lymph node recurrence in patients with uterine cervical carcinoma in Japan: a multi-institutional study. Gynecol Oncol. 2006;103(2):435–438. doi:10.1016/j.ygyno.2006.03.034
7. Niibe Y, Hayakawa K. Oligometastases and oligo-recurrence: the new era of cancer therapy. Jpn J Clin Oncol. 2010;40(2):107–111. doi:10.1093/jjco/hyp167
8. Niibe Y, Nishimura T, Inoue T, et al. Oligo-recurrence predicts favorable prognosis of brain-only oligometastases in patients with non-small cell lung cancer treated with stereotactic radiosurgery or stereotactic radiotherapy: a multi-institutional study of 61 subjects. BMC Cancer. 2016;16(1):659. doi:10.1186/s12885-016-2680-8
9. Hishida T, Yoshida J, Aokage K, et al. Postoperative oligo-recurrence of non-small-cell lung cancer: clinical features and survivaldagger. Eur J Cardiothorac Surg. 2016;49(3):847–853. doi:10.1093/ejcts/ezv249
10. Martini N, Melamed MR. Multiple primary lung cancers. J Thorac Cardiovasc Surg. 1975;70(4):606–612. doi:10.1016/S0022-5223(19)40289-4
11. Niibe Y, Jingu K, Onishi H. Long-term outcome of surgery or stereotactic radiotherapy for lung oligo-recurrence. J Thorac Oncol. 2017;12(11):e191. doi:10.1016/j.jtho.2017.07.035
12. Corbin KS, Hellman S, Weichselbaum RR. Extracranial oligometastases: a subset of metastases curable with stereotactic radiotherapy. J Clin Oncol. 2013;31(11):1384–1390. doi:10.1200/JCO.2012.45.9651
13. Sonobe M, Yamada T, Sato M, et al. Identification of subsets of patients with favorable prognosis after recurrence in completely resected non-small cell lung cancer. Ann Surg Oncol. 2014;21(8):2546–2554. doi:10.1245/s10434-014-3630-9
14. Pfannschmidt J, Muley T, Bülzebruck H, et al. Prognostic assessment after surgical resection for non-small cell lung cancer: experiences in 2083 patients. Lung Cancer. 2007;55(3):371–377. doi:10.1016/j.lungcan.2006.10.017
15. Lodeweges JE, Klinkenberg TJ, Ubbels JF, et al. Long-term outcome of surgery or stereotactic radiotherapy for lung oligometastases. J Thorac Oncol. 2017;12(9):1442–1445. doi:10.1016/j.jtho.2017.05.015
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.