Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Clinical Features and Antimicrobial Susceptibility of Pseudomonas aeruginosa and Acinetobacter baumannii Complex Isolates in Intensive Care Patients with Chronic Obstructive Pulmonary Disease and Community-Acquired Pneumonia in Taiwan
Authors Chang KY, Wu PC, Lee CH, Lee YC ![]() , Chen HC, Huang WC
, Chen HC, Huang WC ![]() , Wu MF
, Wu MF
Received 18 March 2021
Accepted for publication 1 June 2021
Published 17 June 2021 Volume 2021:16 Pages 1801—1811
DOI https://doi.org/10.2147/COPD.S311714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ko-Yun Chang,1,* Pi-Chu Wu,2,* Ching-Hsiao Lee,3 Yu-Che Lee,4 Hui-Chen Chen,1 Wei-Chang Huang,1,3,5– 7,* Ming-Feng Wu1,8,*
1Division of Chest Medicine, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, 407, Taiwan; 2Nursing Department, Taichung Veterans General Hospital, Taichung, 407, Taiwan; 3Department of Medical Technology, Jen-Teh Junior College of Medicine, Nursing and Management, Miaoli, 350, Taiwan; 4Department of Medicine, University at Buffalo-Catholic Health, Buffalo, NY, USA; 5School of Medicine, Chung Shan Medical University, Taichung, 402, Taiwan; 6Ph.D. Program in Translational Medicine, National Chung Hsing University, Taichung, 402, Taiwan; 7Master Program for Health Administration, Department of Industrial Engineering and Enterprise Information, Tunghai University, Taichung, 407, Taiwan; 8Department of Medical Laboratory Science and Biotechnology, Central Taiwan University of Science and Technology, Taichung, 406, Taiwan
*These authors contributed equally to this work
Correspondence: Wei-Chang Huang
Division of Chest Medicine, Department of Internal Medicine, Taichung Veterans General Hospital, 1650 Taiwan Boulevard Sect. 4, Taichung, 40705, Taiwan
Tel +886-4-23592525 ext. 4054
Fax +886-4-23741320
Email [email protected]
Purpose: Little is known about the features and implications of Pseudomonas aeruginosa (PA) and Acinetobacter baumannii complex (ABC) isolates discovered in patients with chronic obstructive pulmonary disease (COPD) and community-acquired pneumonia (CAP) requiring invasive mechanical ventilation and admission to an intensive care unit. Thus, our study aimed to investigate the clinical characteristics and antimicrobial susceptibilities of PA and ABC isolates cultured from endotracheal aspirates (EAs) in such population.
Patients and Methods: In this retrospective, cross-sectional study, clinical data from medical records were reviewed and collected for analysis.
Results: Of the 262 participants, 17.2% (45/262), 11.5% (30/262), and 27.1% (71/262) had PA, ABC, and any of the two isolates discovered from EA cultures, respectively. Patients with PA isolates were associated with poorer lung function (the Global Initiative for Chronic Obstructive Lung Disease (GOLD) III+IV versus GOLD I+II, odds ratio (OR)=2.39, p= 0.022) and a lower body mass index (per increase of 1 kg/m2, OR= 0.93, p= 0.106) while the former was an independent predictor. Moreover, both subjects with ABC isolates and those with any of these two microorganisms were independently associated with a lower serum albumin level (per increase of 1 g/dL, OR= 0.44, p=0.009 and OR= 0.59, p=0.023, respectively). Participants with PA isolates were more likely to have failed weaning (62.2% versus 44.7%, p= 0.048) and death (28.9% versus 12.4%, p= 0.010) than those without PA isolates. The majority of the PA and ABC isolates were susceptible and resistant to all the tested antimicrobials, respectively, except that tigecycline had a reliable activity against ABC.
Conclusion: Our findings provide important information to help intensivists make better treatment decisions in critically ill patients with COPD and CAP.
Keywords: Acinetobacter baumannii complex, CAP, COPD, intensive care, Pseudomonas aeruginosa, Taiwan
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms and airflow limitation due to chronic airway inflammation and/or alveolar destruction, which can be caused by substantial exposure to noxious gas or particles.1 COPD has become one of the most common causes of morbidity and mortality throughout the world and patients often die from it or its complications.1 COPD therefore represents an important public health challenge and has a significant global economic burden.1
Community-acquired pneumonia (CAP) commonly occurs in patients with COPD due to their impaired lung defenses.2,3 Once CAP progresses, COPD patients are at increased risk of respiratory failure that requires invasive mechanical ventilation (IMV) and intensive care unit (ICU) admission, which raises their risk of mortality.4,5
Although the most CAP pathogens in patients with COPD are known to be Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis. However, Pseudomonas aeruginosa (PA) and other gram-negative bacilli are more likely to be observed in older hospitalized patients with COPD and CAP, as well as those who have poorer lung function, are receiving oral corticosteroid treatment and require IMV and an ICU admission, and could significantly predict an increased risk of exacerbation that requires hospitalizations or all-cause mortality.5–11 Furthermore, previous studies have reported that Acinetobacter spp. is one of the major bacterial isolates in patients with hospital-acquired pneumonia (HAP) or ventilator-associated pneumonia (VAP) in Asia as well as in Taiwan. Meanwhile, infection with Acinetobacter spp. often leads to a high mortality rate (up to 33–50%) in HAP or VAP cases around the world, including Taiwan,6,12 while significant increases and upward trends in the relative abundance of the Acinetobacter genus and the Acinetobacter baumannii complex (ABC) species were associated with failed weaning in patients with COPD and CAP requiring IMV and admission to an ICU.13 Taken together, these findings indicate that more effort should be made to clarify the features of PA and Acinetobacter spp. in hospitalized COPD patients with either CAP, HAP or VAP, especially in the critical care setting.
We hypothesized that exploring the features of PA and ABC isolates discovered in critically ill patients with COPD and CAP could provide significant information and implications for managing this population. Therefore, the aim of our study was to investigate the characteristics, risk factors and antibiotic susceptibility of PA and ABC isolates identified from endotracheal aspirates (EAs) in patients with COPD and CAP at a respiratory ICU (RICU) in Taiwan.
Patients and Methods
Study Design, Setting and Population
The study setting and population have been described previously.10 Briefly, this retrospective, cross-sectional study included spirometrically confirmed COPD patients complicated with CAP, who required IMV on arrival at the emergency department (ED) as per physician assessment of the patient’s clinical status and an admission to the RICU at Taichung Veterans General Hospital (TCVGH), which is located in central Taiwan from January 2005 to December 2015. Individuals with tracheostomy, receiving endotracheal intubation before arrival of the ED, or a history of bronchiectasis, asthma, lung cancer and other respiratory diseases were excluded from this study. The diagnostic criteria for COPD and CAP have been previously reported in detail.10 Shortly, COPD was diagnosed spirometrically for all patients according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017 recommendations.14 The diagnosis of pneumonia was made based on radiological and clinical criteria while CAP was confirmed if patients were not documented as having healthcare-associated pneumonia, HAP or VAP in the medical records of the ED on admission, and if they had not been hospitalized in the month prior to the development of pneumonia or resided in long-term care facilities.15,16 For each participant, only the first admission to the RICU was included for analysis to eliminate the possibility of bias from multiple admissions towards the isolates cultured from EAs of the same patient. This study was conducted in accordance with the regulations of patient data confidentiality and Declaration of Helsinki. The Institutional Review Board and Ethics Committee of TCVGH approved this study (approval number: CE17160B) and waived the need for informed consent because this study was based on a retrospective medical chart review.
Data Collection
By reviewing and extracting clinical data from electronic medical records, the investigators completed the patient record form for each participant. For the study purpose, the participants were then categorized based on the results of microbiology from EAs into those with or without PA isolates, those with or without ABC isolates, and those with or without PA and/or ABC isolates. Briefly, the patient record form included the demographic characteristics, the most recent spirometry results prior to this study admission which were performed and interpreted based on the American Thoracic Society statement,17 the airflow limitation severity and type of pharmacological maintenance medications for COPD,14 other medications, previous history of hospital admissions and use of antibiotics within the 3 months prior to entry to the study, comorbidities, modified Glasgow Coma Scale with verbal score as one,17 Acute Physiology and Chronic Health Evaluation II score, pneumonia severity index,18 chest X-ray findings, initial laboratory findings upon arrival at the ED, the results of bacteriology for EAs collected upon insertion of an endotracheal tube regardless of whether or not empiric antibiotic therapy, and in-RICU treatment outcomes. Further details on data collection have been previously published.10 Successful weaning was defined as liberation from IMV on RICU discharge. Otherwise, failed weaning was the case. Antimicrobial susceptibility testing was performed on isolates yielded from EAs that were collected following endotracheal intubation in the ED. This was conducted using the disk diffusion method at the central laboratory of the study institute and the results were interpreted based on the recommendations of the National Committee for Clinical Standards; the results were grouped into three categories: susceptible, intermediate, and resistant.19
Statistical Analysis
All data were shown as frequencies (percentages) for categorical variables and as the mean ± standard deviation for continuous variables. Extreme values were considered to be outside the 75/25% boundaries and were excluded from analysis, with 75% of the sample dataset set at +3.0 × the interquartile range and 25% of the sample dataset set at −3.0 × the interquartile range. Differences between the study groups were analyzed using an independent t-test for continuous variables, and a chi-squared test for categorical variables. Multivariate logistic regression models were used to analyze associated factors for the presence of PA or ABC or any of these two isolates from EA cultures, if they were significant in the univariate analysis. In the comparison of independent variables, odds ratios and 95% confidence intervals were obtained. Statistical significance was set at p<0.05. All statistical analyses were performed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
Demographic and Clinical Information
The patient enrollment diagram was shown in our previously published study [10]. A total of 262 patients were enrolled for analysis. The mean age of all the participants was 78.7 ± 8.9 years, and the majority of them were male and ex- or current smokers. Nearly half of the participants had severe-to-very severe airflow limitation according to the GOLD spirometric classifications (Table 1).1 Furthermore, as high as 230 (88.8%) and 169 (64.5%) participants had the use of systemic corticosteroids and a blood eosinophil count of more than 300 cells/uL, respectively (Table 1).
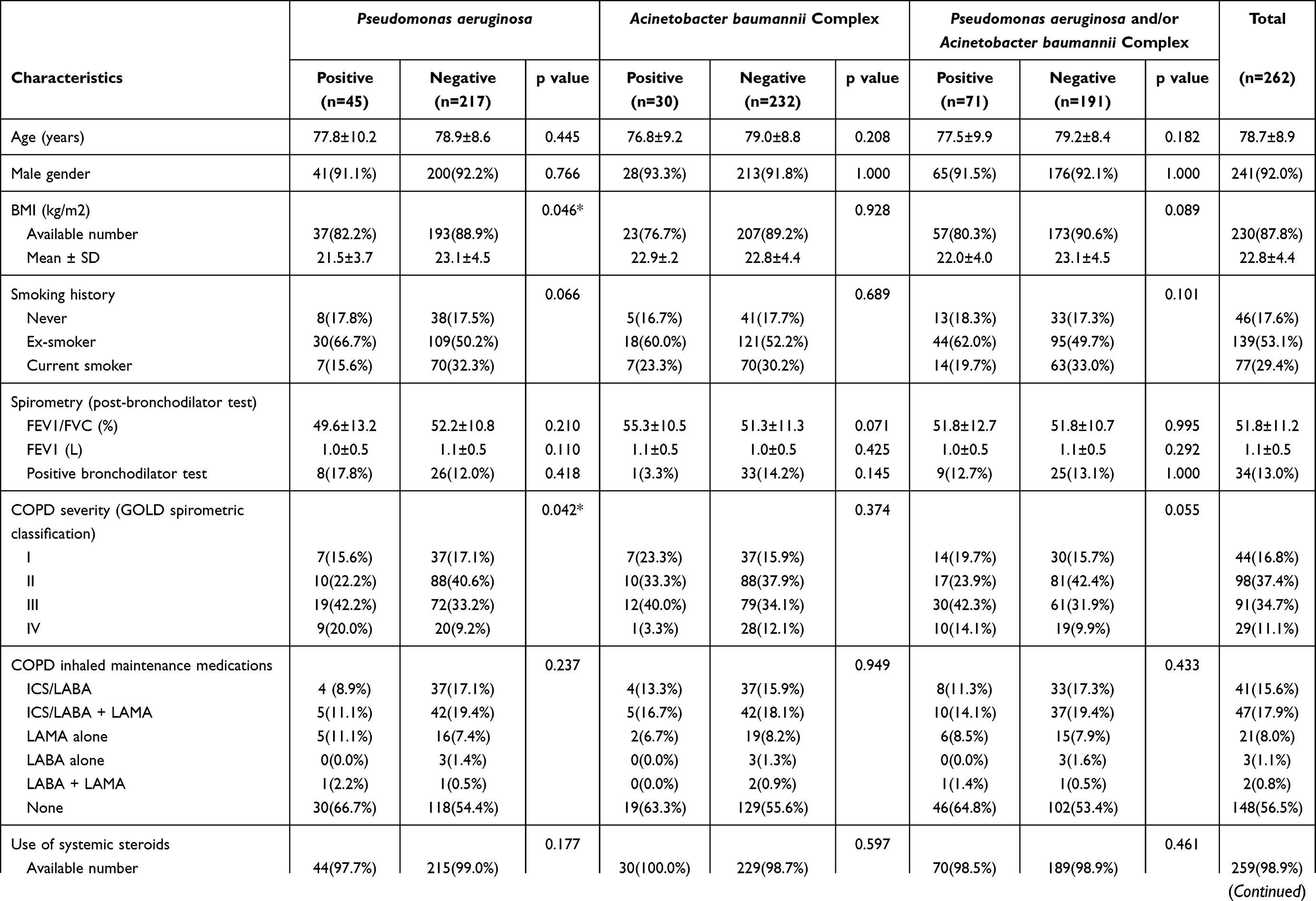 | 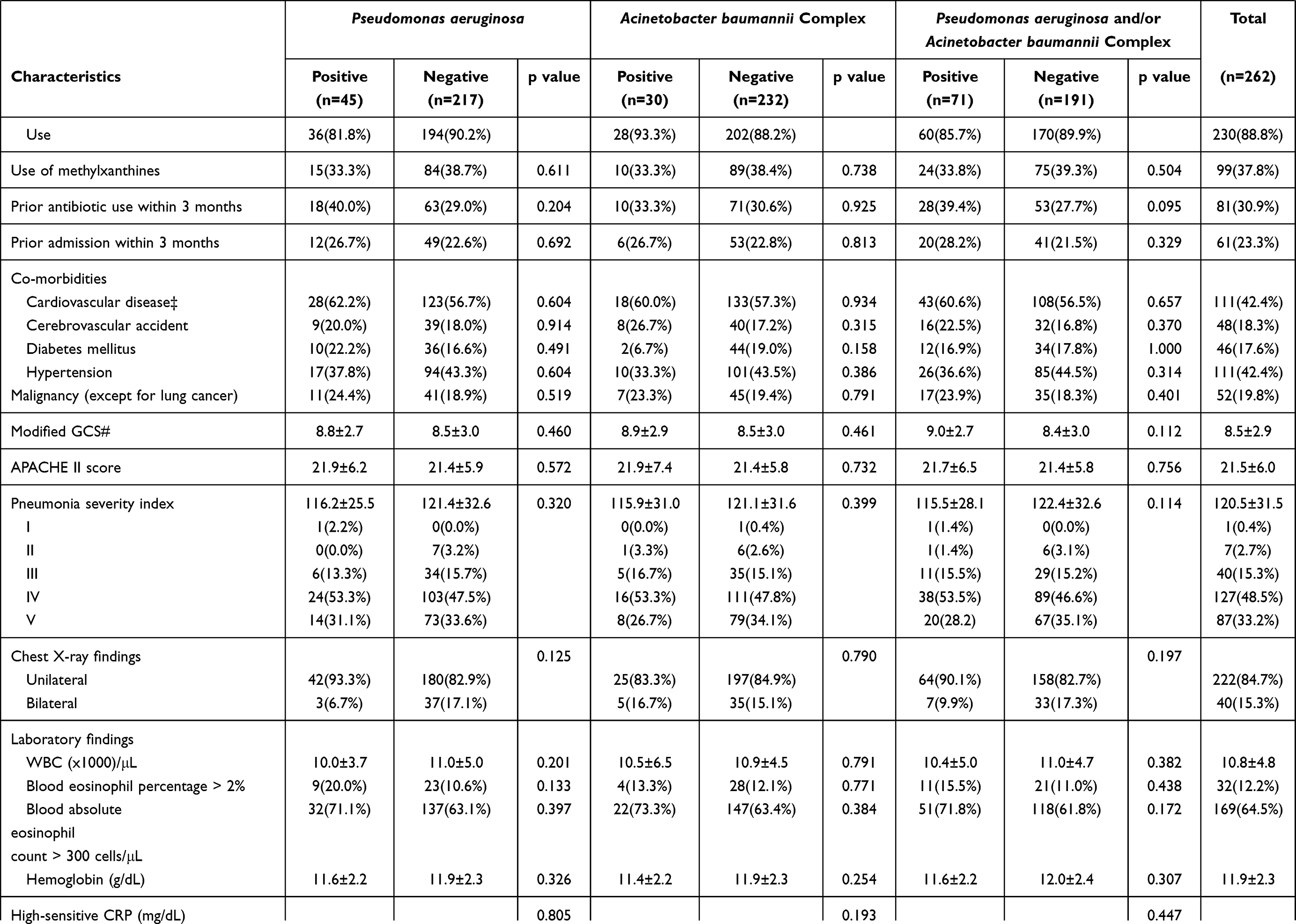 | 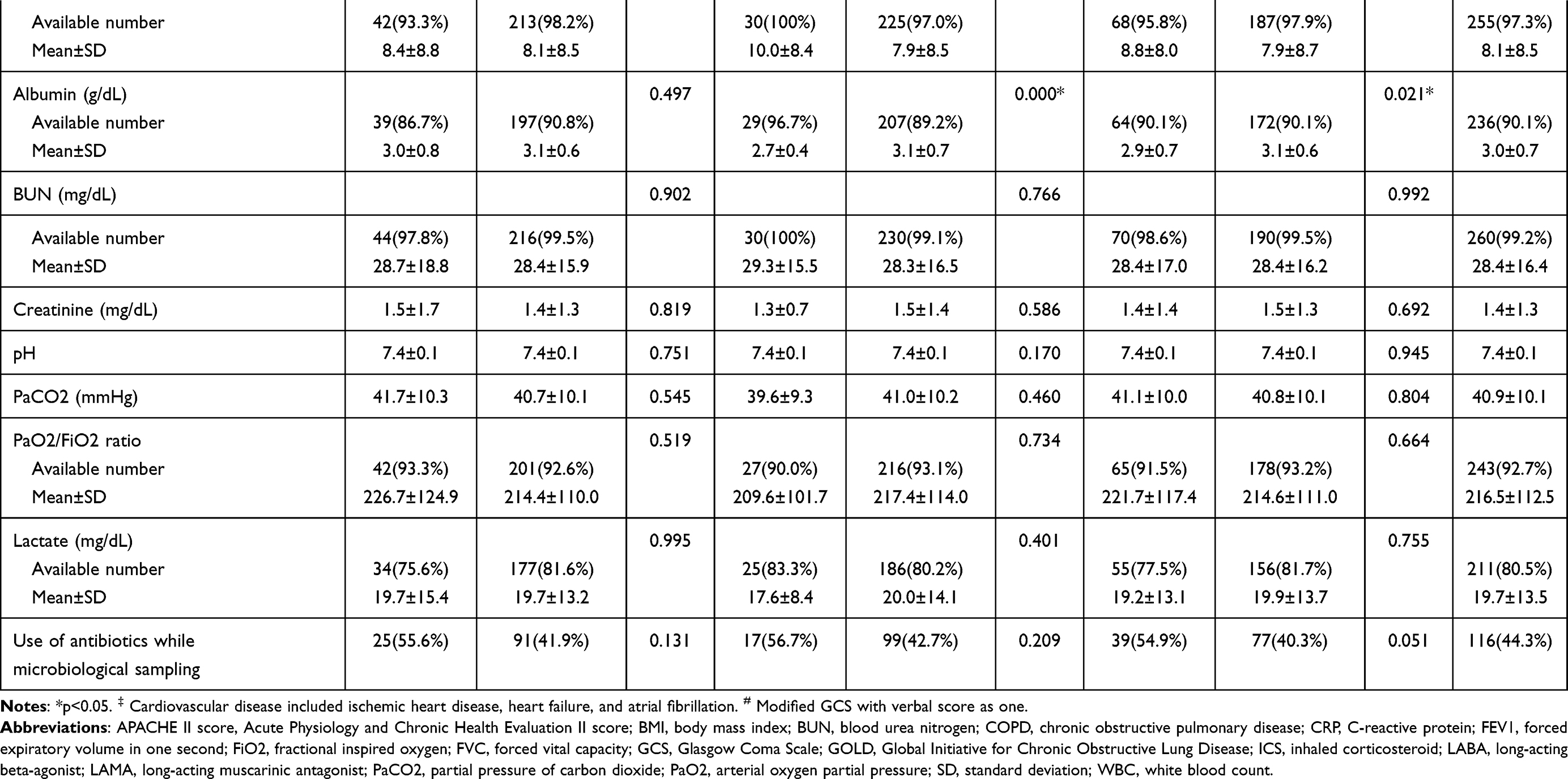 |
Table 1 Demographic and Clinical Characteristics of the Enrolled Participants |
Factors Associated with Pseudomonas aeruginosa and Acinetobacter baumannii Complex Isolates
Among the 262 enrolled patients, 45 (17.2%) had PA isolates (PA-positive group), 30 (11.5%) had ABC isolates (AB complex-positive group), and 71 (27.1%) had any of these two isolates (PA and/or AB complex-positive group), as discovered from their EAs (Table 1). The PA-positive group had a lower body mass index (BMI) and more severe airflow limitation compared with the PA-negative group. Moreover, in contrast to the AB complex-negative and the PA and/or AB complex-negative groups, the AB complex-positive and PA and/or AB complex-positive groups had a lower serum albumin level, respectively (Table 1).
Figure 1 shows the results of the multivariate logistic regression analysis for the discovery of PA and ABC from the EA cultures. We identified that severe-to-very severe airflow limitation (GOLD stage III+IV) was independently associated with the presence of PA isolates, while reduced serum albumin was a significant predictor for the discovery of ABC isolates, and for the presence of PA and/or ABC isolates.
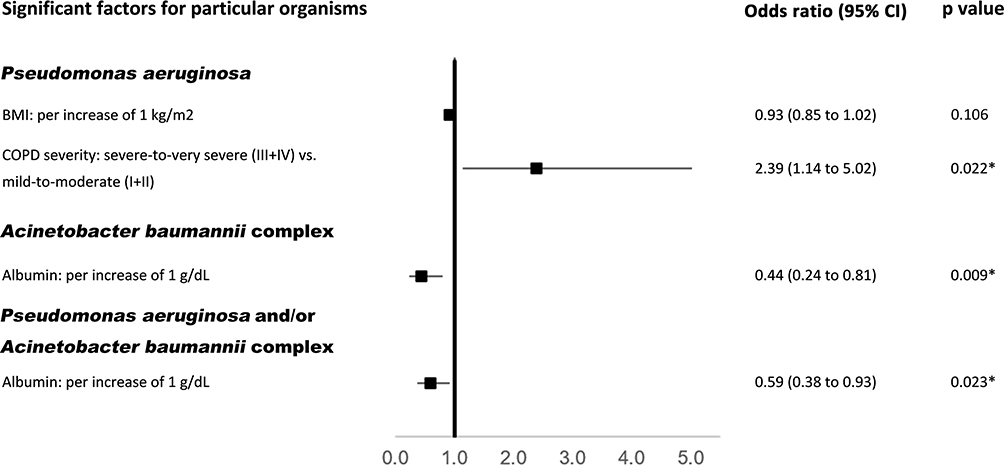 |
Figure 1 Independent factors associated with the presence of Pseudomonas aeruginosa and Acinetobacter baumannii complex discovered from endotracheal aspirate cultures. *p<0.05. Abbreviations: CI, confidence interval; also see Table 1. |
Treatment Outcomes in the RICU
The in-RICU treatment outcomes were shown in Table 2. Particularly, patients with PA isolates were more likely to be associated with failed weaning as well as mortality when compared to those without PA isolates.
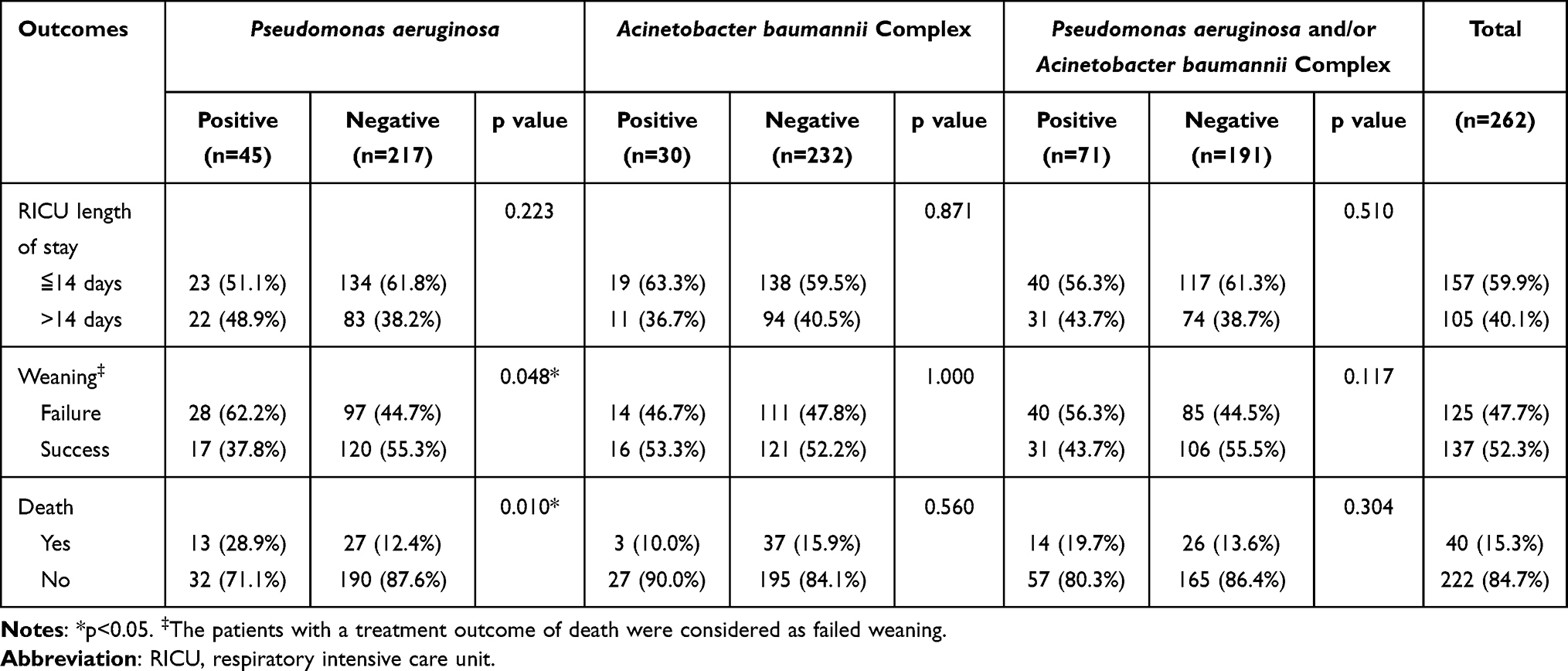 |
Table 2 Clinical Outcomes in the Respiratory Intensive Care Unit for the Enrolled Patients by Study Group |
Antimicrobial susceptibility against Pseudomonas aeruginosa and Acinetobacter baumannii complex isolates
Table 3 shows that most PA isolates were susceptible to all of the tested antimicrobial agents, including β-lactam antibiotics, fluoroquinolones, third- and fourth generation cephalosporins and aminoglycosides. Meanwhile, the majority of ABC isolates were susceptible to tigecycline but resistant to the other tested antimicrobials (Table 4)
 |
Table 3 Antimicrobial Susceptibility of 45 Endotracheal Aspirate Isolates of Pseudomonas aeruginosa |
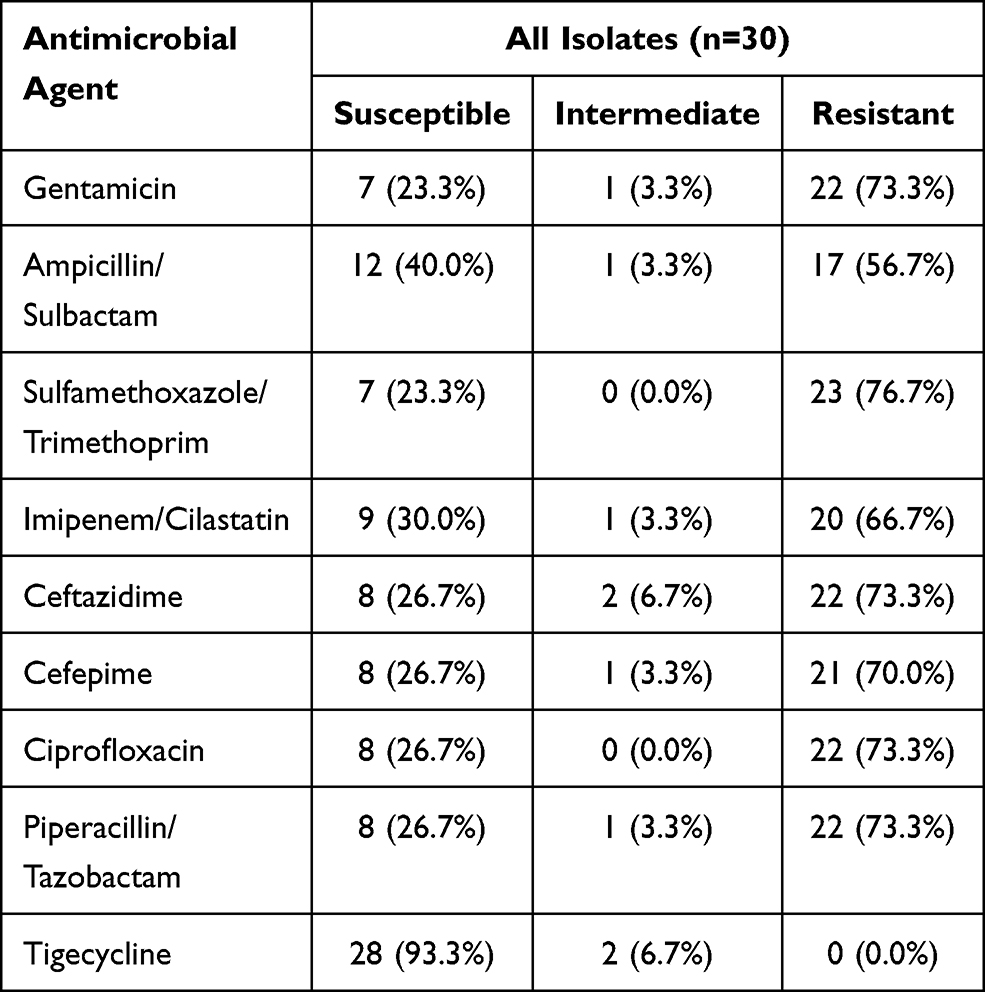 |
Table 4 Antimicrobial Susceptibility of 30 Endotracheal Aspirate Isolates of Acinetobacter baumannii Complex |
Discussion
Main Findings
To the best of our knowledge, this is the first study to evaluate the clinical characteristics and antibiotic susceptibilities of PA and ABC isolates in patients with COPD and CAP, who required IMV and admission to the ICU. Our findings clearly demonstrated that the presence of PA in EA cultures was associated with a lower BMI and poorer lung function, while the latter was a significant predictor for the discovery of PA. The discovery of ABC and the presence of any of PA and ABC in EA cultures were independently associated with a lower serum albumin level. Meanwhile, compared to those without PA isolates, patients with PA isolates were more likely to have failed weaning and death. Moreover, all of the tested antimicrobials had reliable activities against PA, while among the tested antibiotics, only tigecycline had a trustworthy therapeutic response to ABC.
Interpretation of the Findings
In addition to GOLD III–IV spirometric classification, which was independently associated with the discovery of PA from EA cultures in critical care patients with COPD and CAP found in our study and that from sputum cultures in exacerbated patients with COPD found by Eller et al and Miravitlles et al,20,21 we also found that PA was more likely to be discovered from EA cultures in critically ill patients with COPD and CAP who had a reduced BMI. Previous studies have also reported that chronic colonization or previous isolation with PA from the sputum, a history of bronchiectasis, broad-spectrum antibiotic use within the past three months, chronic systemic glucocorticoid use, hospital admission within the past year and a higher BODE (BMI, airflow obstruction, dyspnea, exercise capacity) index, were risk factors for PA isolation in the sputum of patients with exacerbated COPD.22–27 Taken together, it demonstrates that the discovery of PA from respiratory samples has a predictable clinical behavior in patients with COPD in various clinical settings.
Previous studies found that 84.4% of Acinetobacter baumannii (AB) related CAP patients had underlying COPD, while COPD was independently associated with colistin-resistance A. baumannii bacteremia,28,29 indicating that there was a close relationship between ABC and COPD. Furthermore, Li et al and Özgür et al found that higher Acute Physiology and Chronic Health Evaluation II scores and the presence of systemic illness, and higher Simplified Acute Physiology Score II scores, were strongly related to AB pneumonia. While we identified that a lower serum albumin level was independently associated with the presence of ABC and the discovery of any of PA and ABC from EA cultures in patients with COPD and CAP, who required IMV and admission to an ICU.30,31 All these findings suggest that ABC may be particularly pathogenic in patients with pneumonia who are severely ill and have malnutrition.
Our study, conducted between 2005 and 2015 in Taiwan, showed that the majority of PA isolates were susceptible to all of the tested antimicrobial agents, which was consistent with the findings reported by Restrepo et al in 2015.32 They showed a low prevalence (2.0% and 1.0%, respectively) of drug-resistant and multidrug-resistant PA in hospitalized patients with CAP in the United States.32 By contrast, according to the National Healthcare Safety Network, data collected from over 4,500 hospitals in the United States from 2011 to 2014, showed multidrug-resistant rates among PA isolates were as high as 20%, 18%, 18% and 4% in VAP, central line-associated blood stream infections, catheter-associated urinary tract infections, and surgical site infections, respectively.33 Conversely, a favorable trend was observed in a recent study published by Jernigan et al, which reported that the rate of multidrug-resistant PA infections among hospitalized patients decreased by 30% between 2012 and 2017 across 890 hospitals in the United States.34 These data imply that the drug susceptibility pattern of PA changes with time, has geographic differences and should be updated regularly.
Similar to our findings that the majority of ABC isolates were resistant to all tested antimicrobials except for tigecycline, previous studies found that at least 40% of Acinetobacter spp. isolates from various sites of infection, were multidrug-resistant; more than half of the AB isolates were resistant to quinolones (ciprofloxacin and levofloxacin), sulfonamides (baktar), cephalosporins (ceftazidime and cefepime), beta-lactam/beta-lactamase inhibitor combinations (tazobactam/piperacillin), carbapenems (doripenem, imipenem, and meropenem), and aminoglycosides (amikacin and gentamicin).33,35 It has also been reported that the use of tigecycline-based therapy for treating multidrug-resistant A. baumannii (MDRAB) pneumonia might lead to a higher mortality than colistin-based treatment in the ICU.36 Physicians should therefore be aware that their antibiotic choice for the treatment of MDRAB infection should be carefully considered, particularly in the critical care setting.
Previous studies have shown that patients with PA infection exhibited a worse outcome in terms of mortality rate, length of stay, risk of disease exacerbation and period of IMV in varied clinical settings.37–39 Together with our findings that participants with PA isolates discovered in EA cultures were associated with failed weaning and death, this suggests that early suspicion and identification of PA infection may play a crucial role to initiate an appropriate antibiotic therapy even improve disease outcomes in clinical practice.
An interesting result of as high as 64.5% of participants with blood eosinophils > 300 cells/uL was found in our study. Although, the exact mechanism underlying blood eosinophilia remains unknown in such population, a body of evidence has shown that, in COPD, high circulatory eosinophil levels could be used as a biomarker to predict inhaled corticosteroid (ICS) response, or an indicator for ICS usage, whether the patient will be a frequent exacerbator or not, and the in-ICU treatment outcome,1,10,40–42 making blood eosinophil counts could be a useful treatable trait for patients with COPD nowadays.41
Strengths and Limitations
A strength of the current study was that we enrolled a valid study population of COPD patients, which was confirmed by a lung function test. We also collected EA samples for microbiological analysis that were less-upper airway contaminated and more representative of the real bacterial profile of CAP. This compensates for the several limitations of the study, including the fact that this study was conducted in a single medical center located in central Taiwan, meaning that our results may not be generalizable to other regions or countries. It is also possible that there was antibiotic use in some participants prior to the collection of their EAs for microbiological culture, which may have impacted the microbiological profiling because of the study’s retrospective design. Moreover, patients with a history of bronchiectasis were not included in this study; the majority of participants received the treatment with systemic steroids at enrollment; the minimal inhibitory concentration on tested antimicrobial agents for PA and ABC and the history of positive bacterial culture for PA and ABC prior to the enrollment were not recorded, making it less informative for further study.
Implications for Future Research, Policy and Practice
Previously, we found that PA and ABC were the most common potentially pathogenic microorganisms in intensive care patients with COPD and CAP.10 This study further provided information on the predictors and drug susceptibilities of these two potentially pathogenic microorganisms in this population. Taken together, these findings could help intensivists clarify bacterial profiling and patient selection for appropriate antibiotic therapies. Future multicenter, prospective studies should be conducted, not only to validate our results but also to set recommendations regarding treatment decisions in such a population.
Conclusion
Our findings provide useful information for intensivists and have significant implications which could help them make better decisions regarding their choice of antibiotic therapy, when managing intensive care patients with COPD and CAP.
Data Sharing Statement
Data supporting the reported results can be found at Lab. 114 in Taichung Veterans General Hospital, Taichung, Taiwan.
Acknowledgments
The authors would like to thank Dr. Gwan-Han Shen, who supervised Laboratory No. 114 at Taichung Veterans General Hospital and passed away in 2014. We hold you dear in our memory.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Taichung Veterans General Hospital, Taichung, Taiwan (grant numbers TCVGH-1073205B & TCVGH-1093202C).
Disclosure
The authors declare no conflicts of interest.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021.
2. Soriano JB, Visick GT, Muellerova H, Payvandi N, Hansell AL. Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest. 2005;128(4):2099–2107. doi:10.1378/chest.128.4.2099
3. Müllerova H, Chigbo C, Hagan GW, et al. The natural history of community-acquired pneumonia in COPD patients: a population database analysis. Respir Med. 2012;106(8):1124–1133.
4. Fine MJ, Smith MA, Carson CA, et al. Prognosis and outcomes of patients with community-acquired pneumonia: a meta-analysis. JAMA. 1996;275(2):134–141.
5. Restrepo MI, Mortensen EM, Pugh JA, Anzueto A. COPD is associated with increased mortality in patients with community-acquired pneumonia. Eur Respir J. 2006;28(2):346–351.
6. Musher DM, Thorner AR. Community-acquired pneumonia. N Engl J Med. 2014;371(17):1619–1628.
7. Cilli A, Erdem H, Karakurt Z, et al. Community-acquired pneumonia in patients with chronic obstructive pulmonary disease requiring admission to the intensive care unit: risk factors for mortality. J Crit Care. 2013;28(6):975–979.
8. Ko FW, Ip M, Chan PK, Ng SS, Chau S, Hui DS. A one-year prospective study of infectious etiology in patients hospitalized with acute exacerbations of COPD and concomitant pneumonia. Respir Med. 2008;102(8):1109–1116.
9. Pifarre R, Falguera M, Vicente-de-vera C, Nogues A. Characteristics of community-acquired pneumonia in patients with chronic obstructive pulmonary disease. Respir Med. 2007;101(10):2139–2144.
10. Huang WC, Lee CH, Wu MF, et al. Clinical features, bacteriology of endotracheal aspirates and treatment outcomes of patients with chronic obstructive pulmonary disease and community-acquired pneumonia in an intensive care unit in Taiwan with an emphasis on eosinophilia versus non-eosinophilia: a retrospective case–control study. BMJ Open. 2018;8(9):e020341.
11. Eklöf J, Sørensen R, Ingebrigtsen T, et al. Pseudomonas aeruginosa and risk of death and exacerbations in patients with chronic obstructive pulmonary disease: an observational cohort study of 22 053 patients. Clin Microbiol Infect. 2020;26(2):227–234.
12. Chung DR, Song JH, Kim SH, et al. High prevalence of multidrug-resistant nonfermenters in hospital-acquired pneumonia in Asia. Am J Respir Crit Care Med. 2011;184(12):1409–1417. doi:10.1164/rccm.201102-0349OC
13. Huang WC, Wu MF, Huang CC, et al. Dynamics of the lung microbiome in intensive care patients with chronic obstructive pulmonary disease and community-acquired pneumonia. Sci Rep. 2020;10(1):1–10.
14. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017.
15. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44 Suppl 2(Suppl 2):S27–72. doi:10.1086/511159
16. Leung WS, Chu CM, Tsang KY, Lo FH, Lo KF, Ho PL. Fulminant community-acquired Acinetobacter baumannii pneumonia as a distinct clinical syndrome. Chest. 2006;129(1):102–109. doi:10.1378/chest.129.1.102
17. American Thoracic Society. Lung function testing: selection of reference values and interpretative strategies. Am Rev Respir Dis. 1991;144(5):1202–1218. doi:10.1164/ajrccm/144.5.1202.
18. Fine MJ, Hanusa BH, Lave JR, et al. Comparison of a disease-specific and a generic severity of illness measure for patients with community-acquired pneumonia. J Gen Intern Med. 1995;10(7):359–368. doi:10.1007/bf02599830
19. Standards. NCfCL. Performance Standards for Antimicrobial Susceptibility Testing. 12th Informational Supplement. Approved Standard M100-S12. Wayne: National Committee for Clinical Laboratory Standards; 2002.
20. Eller J, Ede A, Schaberg T, Niederman MS, Mauch H, Lode H. Infective exacerbations of chronic bronchitis: relation between bacteriologic etiology and lung function. Chest. 1998;113(6):1542–1548.
21. Miravitlles M, Espinosa C, Fernández-Laso E, Martos JA, Maldonado JA, Gallego M. Relationship between bacterial flora in sputum and functional impairment in patients with acute exacerbations of COPD. Chest. 1999;116(1):40–46.
22. Groenewegen KH, Wouters EF. Bacterial infections in patients requiring admission for an acute exacerbation of COPD; a 1-year prospective study. Respir Med. 2003;97(7):770–777.
23. Garcia-Vidal C, Almagro P, Romaní V, et al. Pseudomonas aeruginosa in patients hospitalised for COPD exacerbation: a prospective study. Eur Respir J. 2009;34(5):1072–1078.
24. Parameswaran GI, Sethi S. Pseudomonas infection in chronic obstructive pulmonary disease. Future Microbiol. 2012;7(10):1129–1132.
25. Gallego M, Pomares X, Espasa M, et al. Pseudomonas aeruginosa isolates in severe chronic obstructive pulmonary disease: characterization and risk factors. BMC Pulm Med. 2014;14(1):1–12.
26. Boixeda R, Almagro P, Díez-Manglano J, et al. Bacterial flora in the sputum and comorbidity in patients with acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:2581.
27. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012.
28. Peng C, Zong Z, Fan H. Acinetobacter baumannii isolates associated with community-acquired pneumonia in West China. Clin Microbiol Infect. 2012;18(12):E491–E493.
29. Wang YC, Lee YT, Yang YS, et al. Risk factors and outcome for colistin-resistant Acinetobacter nosocomialis bacteraemia in patients without previous colistin exposure. Clin Microbiol Infect. 2015;21(8):758–764.
30. Li YJ, Pan CZ, Fang CQ, et al. Pneumonia caused by extensive drug-resistant Acinetobacter baumannii among hospitalized patients: genetic relationships, risk factors and mortality. BMC Infect Dis. 2017;17(1):371. doi:10.1186/s12879-017-2471-0
31. Özgür ES, Horasan ES, Karaca K, Ersöz G, Atış SN, Kaya A. Ventilator-associated pneumonia due to extensive drug-resistant Acinetobacter baumannii: risk factors, clinical features, and outcomes. Am J Infect Control. 2014;42(2):206–208.
32. Restrepo MI, Babu BL, Reyes LF, et al. Burden and risk factors for Pseudomonas aeruginosa community-acquired pneumonia: a multinational point prevalence study of hospitalised patients. Eur Respir J. 2018;52:2.
33. Weiner LM, Webb AK, Limbago B, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. Infect Control Hosp Epidemiol. 2016;37(11):1288–1301.
34. Jernigan JA, Hatfield KM, Wolford H, et al. Multidrug-resistant bacterial infections in U.S. Hospitalized patients, 2012-2017. N Engl J Med. 2020;382(14):1309–1319. doi:10.1056/NEJMoa1914433
35. Chen LK, Kuo SC, Chang KC, et al. Clinical antibiotic-resistant Acinetobacter baumannii strains with higher susceptibility to environmental phages than antibiotic-sensitive strains. Sci Rep. 2017;7(1):6319. doi:10.1038/s41598-017-06688-w
36. Chuang YC, Cheng CY, Sheng WH, et al. Effectiveness of tigecycline-based versus colistin- based therapy for treatment of pneumonia caused by multidrug-resistant Acinetobacter baumannii in a critical setting: a matched cohort analysis. BMC Infect Dis. 2014;14:102. doi:10.1186/1471-2334-14-102
37. Fujitani S, Sun HY, Yu VL, Weingarten JA. Pneumonia due to Pseudomonas aeruginosa: part I: epidemiology, clinical diagnosis, and source. Chest. 2011;139(4):909–919. doi:10.1378/chest.10-0166
38. Eklöf J, Sørensen R, Ingebrigtsen TS, et al. Pseudomonas aeruginosa and risk of death and exacerbations in patients with chronic obstructive pulmonary disease: an observational cohort study of 22 053 patients. Clin Microbiol Infect. 2020;26(2):227–234. doi:10.1016/j.cmi.2019.06.011
39. Tumbarello M, De Pascale G, Trecarichi EM, et al. Clinical outcomes of Pseudomonas aeruginosa pneumonia in intensive care unit patients. Intensive Care Med. 2013;39(4):682–692. doi:10.1007/s00134-013-2828-9
40. Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood Eosinophils and Exacerbations in Chronic Obstructive Pulmonary Disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
41. David B, Bafadhel M, Koenderman L, De Soyza A. Eosinophilic inflammation in COPD: from an inflammatory marker to a treatable trait. Thorax. 2020;76(2):188–195. doi:10.1136/thoraxjnl-2020-215167
42. Wedzicha JA. Eosinophils as Biomarkers of Chronic Obstructive Pulmonary Disease Exacerbation Risk. Maybe Just for Some? Am J Respir Crit Care Med. 2016;193(9):937–938. doi:10.1164/rccm.201601-0015ED
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.