Back to Journals » Journal of Asthma and Allergy » Volume 17
Clinical Experience with Berotralstat in Patients with Hereditary Angioedema with Normal C1-Esterase Inhibitor: A Commented Case Series
Authors Kanarek HJ, Mutschelknaus DAS
Received 21 October 2023
Accepted for publication 13 February 2024
Published 23 February 2024 Volume 2024:17 Pages 123—132
DOI https://doi.org/10.2147/JAA.S445893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Henry J Kanarek,* Drew Austin Saville Mutschelknaus*
Kanarek Allergy, Asthma & Immunology, Leawood, KS, USA
*These authors contributed equally to this work
Correspondence: Henry J Kanarek, Tel +1 (913) 451-8555, Fax +1 (913) 327-8553, Email [email protected]
Abstract: Hereditary angioedema (HAE) is a rare genetic disorder characterized by potentially life-threatening episodes of swelling. Most HAE cases are caused by deficient (type I) or dysfunctional (type II) C1-esterase inhibitor (C1-INH) protein. However, some patients present with a subtype of HAE that is associated with normal plasma levels of functional C1-INH protein and complement component 4 (HAE-nC1INH). Treatment of HAE-nC1INH is driven by clinical experience as robust clinical trial data to inform treatment decisions are lacking in this population. This retrospective case series assessed clinical features and treatment outcomes in 15 patients with HAE-nC1INH who initiated long-term prophylaxis with oral berotralstat 150 mg once daily as part of their disease management pathway. Most patients were female (93%), with a median age of 49 years. All patients experienced abdominal swelling attacks. On average, patients tried a mean of 4 different treatments for their HAE, including berotralstat. Although most patients associated prophylactic and on-demand medications that target the bradykinin pathway with improvements in the frequency and/or severity of attacks, treatment outcomes varied considerably between patients, highlighting the importance of a personalized approach to disease management. In this case series, berotralstat was an effective prophylactic treatment option in most patients with HAE-nC1INH. Further studies are required to demonstrate the potential efficacy, safety, and impact on quality of life of currently approved HAE therapies in patients with HAE-nC1INH.
Keywords: hereditary angioedema, normal C1-esterase inhibitor, prophylaxis, berotralstat, lanadelumab, plasma-derived C1-esterase inhibitor, abortive therapy
Introduction
Patients with hereditary angioedema (HAE) experience unpredictable and potentially life-threatening recurrent episodes of swelling that generally affect the extremities, genitals, abdomen, larynx, and face.1–3 Some patients present with a form of HAE with normal C1-inhibitor (HAE-nC1INH), which is associated with normal plasma levels of functional C1-inhibitor (C1-INH) protein and complement component 4 (C4).3 Mutations in genes such as coagulation factor XII (FXII), plasminogen, angiopoietin 1, kininogen 1, heparan sulfate glucosamine 3-O-sulfotransferase-6, and myoferlin have been identified in several patients with HAE-nC1INH. Some of these genes are involved with the production of bradykinin. However, the prevalence and pathophysiology of the disease are less clear than in HAE with low serum level or functional deficiency in C1 inhibitor (HAE-C1INH), and the etiology of the disease remains unknown for many patients.1,4–9 Additionally, HAE-nC1INH is more challenging to definitively diagnose than HAE-C1INH because diagnosis reliant on genetic testing only identifies a small subset of patients with the disease.8,10 Additionally, these genetic tests are not readily available in all clinical practices.1
Overall, the swelling attacks experienced by patients with HAE-nC1INH and patients with HAE-C1INH are similar, but subtle differences exist between them1,7 Patients with HAE-nC1INH typically present with their first symptoms of disease in late adolescence to early adulthood, while the first symptoms of HAE-C1INH typically appear in childhood.1,5,11 Furthermore, patients with symptomatic HAE-nC1INH are predominately female, with exposure to estrogens frequently linked to the onset and exacerbation of swelling attacks.4,5,12–14
Edema of the face, tongue, and oropharynx have been documented more frequently in patients with HAE-nC1INH than in patients with HAE-C1INH.1,6,7,15,16 A review of 57 French patients with confirmed FXII mutations indicated that 74% of patients experienced HAE attacks affecting the ear, nose, and throat, while 80% experienced abdominal attacks13 despite some experts suggesting that patients with HAE-nC1INH typically have fewer abdominal symptoms.1
The occurrence of non-specific presenting symptoms in patients with HAE-nC1INH often results in misdiagnosis, ongoing treatment with inappropriate therapy (ie, antihistamines, corticosteroids, adrenaline) and/or unnecessary procedures (ie, surgical intervention).5,17–19 Furthermore, the absence of robust data from clinical trials evaluating HAE therapies in patients with HAE-nC1INH means that, once diagnosis is suspected, the treatment of this patient population is based on clinical experience in patients with HAE-C1INH. These treatments include a combination of on-demand (ie, injectable ecallantide, injectable icatibant, and infusions of C1-INH concentrate) and prophylactic agents (ie, intravenous or subcutaneous C1-INH concentrate, injectable lanadelumab, and oral berotralstat) that either directly or indirectly target bradykinin metabolism.1,8,14,20–22 In response to these challenges, it is common for physicians of patients with suspected HAE-nC1INH to initiate a trial course of HAE therapies as part of the diagnostic process.23,24 The purpose of this manuscript is to help raise awareness of HAE-nC1INH by exploring the clinical features that trigger a suspected diagnosis, and provide insights into the observed treatment outcomes in a retrospective case series of 15 patients.
Materials and Methods
This report follows CARE reporting guidelines25 and describes a retrospective patient case series using anonymized data. All patients provided written informed consent for their de-identified case information to be retrospectively collected and published.
The medical records of patients from one treatment center in the USA (Kanarek Allergy, Asthma & Immunology) were reviewed to identify patients with HAE-nC1INH who received oral berotralstat 150 mg once daily for long-term prophylaxis as part of their treatment plan. Information was extracted from each patient’s medical record by the author or a designated member of staff at the medical center using a template that included patient age, patient gender, date and description of assessments, areas of the body affected by attacks, details of any major attacks and their outcomes, medical procedures undertaken because of attacks, and details of any treatments given and their associated outcomes.
Given the lack of standardized, validated biochemical diagnostic tests for HAE-nC1INH, physicians often rely on strategies for differential diagnosis. At this practice (Kanarek Allergy, Asthma & Immunology), HAE-nC1INH diagnosis is based on the following clinical criteria: the patient has a history of recurrent angioedema with no signs of concomitant urticaria and no use of medication that is known to cause angioedema, such as angiotensin-converting enzyme inhibitors; laboratory testing indicates that the patient has normal, or close to normal, plasma levels of C4 and C1-INH antigens and normal C1-INH functionality; the patient either has a genetic mutation in one of the genes known to be associated with HAE-nC1INH or has a personal or family history of recurrent angioedema episodes that were non-responsive to high-dose antihistamine therapy for at least 12 weeks. Assessing treatment response to four times daily (QID) antihistamines, multiple courses of steroids, and epinephrine generally takes place over a period of several months. Careful consideration is made to exclude other diagnoses such as chronic spontaneous urticaria (CSU) without wheals. An understanding of attack features like location and duration can help to differentiate CSU from HAE-nC1INH; CSU is less likely to affect the larynx or abdomen and generally attack durations are shorter versus HAE-nC1INH.26 Beyond non-responsiveness to mast-cell targeted therapies (such as omalizumab),1,23–25,27 responsiveness to available HAE abortive medications (ie icatibant or formulations of C1-INH) is a useful and commonly utilized strategy for differential diagnosis.28 Rapid and durable response to HAE medications provides additional evidence for an HAE-nC1INH diagnosis. As noted in a recent survey of physicians who treat HAE, response to HAE-specific medication was used to inform diagnosis by 74% of survey respondents, while only 43% utilized Factor XII genetic testing.28 Patients often have a challenging journey to obtain an accurate diagnosis of HAE-nC1INH and frequently consult several healthcare providers across multiple specialties. As such, some patients in this case series may have trialed and failed high-dose antihistamines or other therapies prior to becoming a patient at Kanarek Allergy, Asthma & Immunology, and such details may not have been included in the chart notes from this practice.
Patient Demographics
A total of 15 patients with HAE-nC1INH treated with oral berotralstat 150 mg once daily for long-term HAE prophylaxis as part of their disease management pathway were included in this case series. All patients indicated they had experienced swelling attacks, with many of them affecting the face, tongue, throat, and/or abdomen prior to starting berotralstat treatment (see Table 1). Only one patient within the group was male, which is consistent with typical preponderance of female patients with HAE-nC1INH. Due to the low likelihood of identifying specific genetic mutations and the availability of other differential diagnostic strategies like response to HAE medications, none of the patients were screened for known mutations associated with the condition.
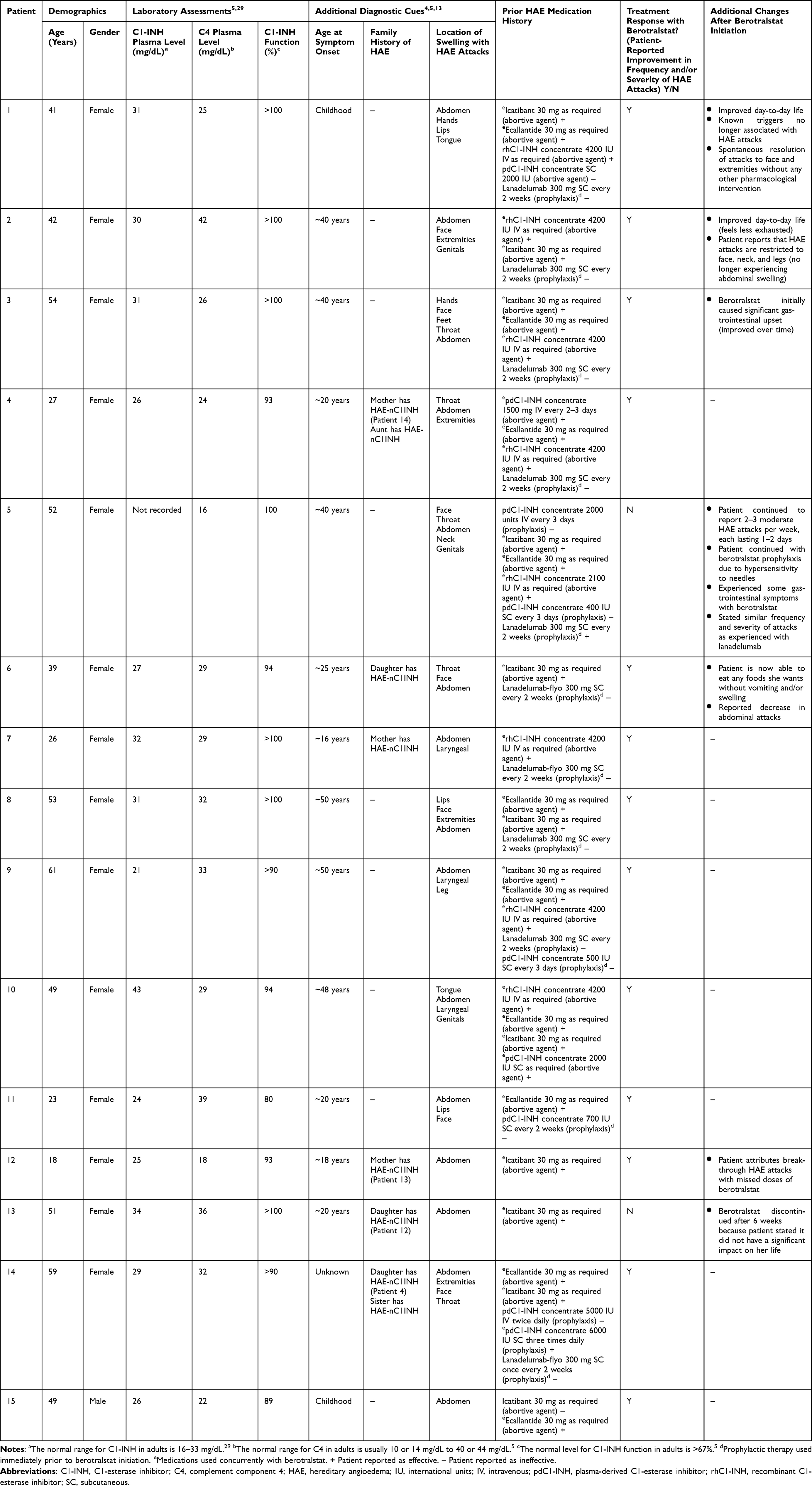 |
Table 1 Patient Demographics with Prior HAE Medication History and Treatment Response with Berotralstat |
Results
HAE-nC1INH Diagnosis
Many patients in this case series noted that they had received prior misdiagnoses, which included menstrual cramps, food allergies, gastrointestinal (GI) disorders (including irritable bowel syndrome), and anaphylaxis. One patient (Patient 2) was also tested for lupus and Lyme disease because of the non-specific presenting symptoms she had experienced before receiving a diagnosis of HAE-nC1INH.
Two patients in the case series indicated they had previously endured medical procedures because of HAE attacks. Patient 5 experienced multiple intubations as a direct consequence of throat swelling, and Patient 6 reported undergoing a hysterectomy and a cholecystectomy as a direct result of abdominal swelling.
The location, severity, and duration of angioedema symptoms were inconsistent with other conditions such as CSU without wheals. Some of the patients in this series experienced severe abdominal swelling that resulted in dehiscence post-Caesarian section or resembled a 4- to 9-month pregnancy which lasted for weeks. With CSU, swelling is less likely to affect the abdomen and, generally, attacks are shorter in duration than with HAE.26
HAE-nC1INH Treatment
In this case series, treatment trialed for the management of HAE-nC1INH varied by patient. Patient-reported treatment outcomes with previous HAE medication have been denoted on Table 1 with a simple legend of + (effective) or – (ineffective). Prophylactic therapies used immediately prior to switching to berotralstat are indicated with footnote “d”, and those agents used concurrently with berotralstat are indicated with footnote “e”. Overall, nine patients in this case series switched directly from lanadelumab to berotralstat prophylaxis, two patients switched from plasma-derived C1-INH (pdC1-INH) concentrate to berotralstat prophylaxis, and four patients initiated berotralstat for prophylaxis after use of abortive therapy only. All patients had access to on-demand abortive therapies while on berotralstat. At the time of manuscript preparation, 13 patients reported that berotralstat improved the frequency and/or severity of their HAE attacks, with several reporting that berotralstat had improved their day-to-day life, reduced or eliminated symptoms of abdominal swelling, and made known triggers less likely to contribute to HAE attacks (see Table 1).
Two of the 15 patients reported that berotralstat did not improve the severity or frequency of HAE attacks. Patient 13 discontinued prophylactic treatment with berotralstat after 6 weeks due to perceived lack of efficacy. Patient 5 continued with berotralstat despite no perceived improvement beyond what she had achieved with lanadelumab as she had become hypersensitive to needles following a dental procedure, rendering her unable to continue with injectable therapies. Berotralstat, an oral medication, provided her with the ability to continue with HAE prophylactic treatment.
GI side effects (described as GI upset) were reported by two patients; both continued treatment with berotralstat as these effects abated over time.
Discussion
Significant unmet needs persist in the diagnosis and treatment of patients with HAE-nC1INH. Here, in this retrospective case series, we explore the clinical features that trigger a suspected diagnosis of HAE-nC1INH and provide insights into the observed treatment.
Although a positive family history of HAE-nC1INH could aid in its diagnosis, it cannot be relied upon as the sole means of identifying patients because HAE-nC1INH appears to have a low penetrance, ultimately leading to some patients having undiagnosed, asymptomatic family members.27 In an Italian study of 32 females with HAE-nC1INH caused by mutations in the coagulation factor XII gene, 44.4% were asymptomatic.14 Accordingly, in our case series, a family history of symptomatic HAE was identified in six patients (Patients 4, 6, 7, 12, 13, and 14. Patients 4 and 14, and Patients 12 and 13 are respective daughter-mother pairs).
While patients with HAE-C1INH usually experience their first symptoms in childhood, patients with HAE-nC1INH often do not present with symptoms until late adolescence or early adulthood.1,5,11,30 In a study of 138 patients with a confirmed diagnosis of HAE-nC1INH, the mean age of symptom onset was 26.8 years, and only 8% of these patients experienced their first swelling attack before the age of 10 years.15,27 Our findings generally support this point, with only 3 of the 15 patients specifically indicating that they may have experienced their first swelling episode during childhood or adolescence. More specifically, Patient 1 reported a severe swelling episode during the fifth grade that affected her feet, and Patient 15 had a history of irritable bowel syndrome with diarrhea and abdominal cramping that occurred throughout childhood. Patient 7 began experiencing swelling episodes in her mid-teens.
Although some experts have suggested that patients with HAE-nC1INH typically have fewer abdominal symptoms than patients with HAE-C1INH,1 case studies indicate that abdominal symptoms may be more common than previously thought.13 Similarly, all 15 patients in this case series reported experiencing at least one attack that affected the abdominal region, suggesting that abdominal pain and/or swelling may be a useful indicator of all forms of HAE. Furthermore, multiple patients in this case series were initially referred from physicians who specialize in GI disorders.
The effects of estrogen on HAE attacks in the HAE-nC1INH population have been well described in the literature.4,5 In our predominantly female case series, 2 of the 14 female patients described HAE attacks that fluctuate according to their menstrual cycle.
The treatment response to HAE therapy is a critical part of the diagnostic process for many patients with suspected HAE-nC1INH.23,24 The number of HAE treatments trialed by patients in our case series ranged from a minimum of two to a maximum of eight. This variability likely reflects the difficulty in achieving a HAE-nC1INH diagnosis, since several therapeutics are often trialed before identifying the correct one for each individual.5,27
To our knowledge, this case series represents one of the first published studies exploring the use of oral berotralstat as a long-term prophylactic treatment option in patients with HAE-nC1INH. Here, most patients indicated that treatment with berotralstat either stabilized their condition or reduced the frequency and/or severity of their HAE attacks. Notably, berotralstat was found to be effective in most patients with HAE-nC1INH who switched from prior prophylaxis with either lanadelumab or pdC1-INH concentrate as well as in patients who used it as their first prophylactic treatment option.
Our findings support those of a case report describing a 60-year-old female with HAE-nC1INH who had a severe needle phobia and benefited from long-term prophylaxis with berotralstat.23 In this case report, berotralstat treatment was initially associated with mild to moderate GI symptoms, including upset stomach and diarrhea, which were self-limiting and managed by ingesting the medication with food.23 In our case series, two patients (Patient 3 and Patient 5) reported that berotralstat treatment was initially associated with some adverse GI symptoms, but the symptoms resolved over time and did not detract from the overall benefits gained from this prophylactic option.
Overall, similar to what was reported in a case series of 23 patients with HAE-nC1INH, our findings indicate that treatment options and disease management strategies recommended for patients with HAE-C1INH may also benefit patients with HAE-nC1INH.5 However, given the heterogeneity in treatment outcomes described in those 23 patients5 and in our case series, it is advisable to adopt a personalized approach to HAE-nC1INH management.
Limitations of our case series include the relatively small sample size, which hampers generalization of the findings to all patients with HAE-nC1INH. Additionally, the retrospective nature of the study means the diagnosis of HAE-nC1INH and the reporting of patient outcomes were not standardized. Patient outcomes were also not quantified in a standardized manner using validated tools such as the angioedema control test (AECT), HAE activity score (HAE-AS), or angioedema quality of life questionnaire (AE-QoL). This made it more difficult to compare the impact of different treatment options on HAE attack frequency and severity.
Conclusions
In summary, the experiences of the patients in our case series indicate that episodes of otherwise unexplained abdominal bloating, pain, and swelling of the hands, extremities, and larynx should raise suspicion of HAE-nC1INH, even if laboratory values rule out a diagnosis of HAE-C1INH. Our findings also support the suggestion that FDA-approved HAE treatments may also benefit patients with suspected or diagnosed HAE-nC1INH and that adoption of a personalized approach to disease management is critical to optimize treatment outcomes. Oral berotralstat 150 mg once daily was an effective prophylactic treatment option in most of the patients in this case series. Further studies in patients with HAE-nC1INH are required to demonstrate the efficacy, safety, and impact on quality of life of HAE therapies, including berotralstat, that may benefit this patient population.
Abbreviations
HAE, hereditary angioedema; C1-INH, C1-esterase inhibitor; C4, complement component 4; CSU, chronic spontaneous urticaria; HAE-C1INH, HAE due to deficiency/defect in C1-INH; HAE-nC1INH, HAE with normal C1-esterase inhibitor and complement component 4; FDA, Food and Drug Administration; pdC1-INH, plasma-derived C1-esterase inhibitor; rhC1-INH, recombinant C1-esterase inhibitor; QID, four times daily.
Data Sharing Statement
The data supporting the conclusions of this manuscript are included within.
Ethics Approval and Informed Consent
This report describes a retrospective patient case series using anonymized data. Patients provided written informed consent for their de-identified case details to be collected, and all data was maintained with confidentiality. IRB review and approval was not sought for this research. This research was exempt from IRB review as it was a retrospective, longitudinal case review and involved an FDA approved medication for standard of care practice and these patients were treated as such.
Consent for Publication
Written informed consent was obtained from the patients for the publication of this case series.
Acknowledgments
The authors would like to thank the patients who contributed to this case series. Medical writing support was provided by Porterhouse Medical Group under the direction of the authors and in line with the GPP 2022 guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Development of this manuscript, writing support, and manuscript submission were funded by BioCryst Pharmaceuticals, Inc. BioCryst did not play a role in the design of the study nor the collection, analysis, and interpretation of data.
Disclosure
HJK is a speaker for AstraZeneca plc, BioCryst Pharmaceuticals, Inc., Pharming Group N.V., and Teva Pharmaceuticals Industries Ltd., and has contracted research with ADMA Biologics, Inc., BioCryst Pharmaceuticals, Inc., BioMarin Pharmaceutical, Inc., Kedrion Biopharma, Inc., Novartis AG, Octapharma AG, Regeneron Pharmaceuticals, Inc., and Takeda Pharmaceutical Company Ltd. DASM has contract research with ADMA Biologics, Inc., BioCryst Pharmaceuticals, Inc., BioMarin Pharmaceutical, Inc., Kedrion Biopharma, Inc., Novartis AG, Octapharma AG, Regeneron Pharmaceuticals, Inc., and Takeda Pharmaceutical Company Ltd. The authors report no other conflicts of interest in this work.
References
1. Busse PJ, Christiansen SC, Riedl MA, et al. US HAEA medical advisory board 2020 guidelines for the management of hereditary angioedema. J Allergy Clin Immunol Pract. 2021;9(1):132–150 e3. doi:10.1016/j.jaip.2020.08.046
2. Caballero T. Treatment of hereditary angioedema. J Investig Allergol Clin Immunol. 2021;31(1):1–16. doi:10.18176/jiaci.0653
3. Longhurst HJ, Bork K. Hereditary angioedema: an update on causes, manifestations and treatment. Br J Hosp Med. 2019;80(7):391–398. doi:10.12968/hmed.2019.80.7.391
4. Bork K, Machnig T, Wulff K, Witzke G, Prusty S, Hardt J. Clinical features of genetically characterized types of hereditary angioedema with normal C1 inhibitor: a systematic review of qualitative evidence. Orphanet J Rare Dis. 2020;15(1):289. doi:10.1186/s13023-020-01570-x
5. Jones DH, Bansal P, Bernstein JA, et al. Clinical profile and treatment outcomes in patients with hereditary angioedema with normal C1 esterase inhibitor. World Allergy Organ J. 2022;15(1):100621. doi:10.1016/j.waojou.2021.100621
6. Riedl MA. Hereditary angioedema with normal C1-INH (HAE type III). J Allergy Clin Immunol Pract. 2013;1(5):427–432. doi:10.1016/j.jaip.2013.06.004
7. Magerl M, Germenis AE, Maas C, Maurer M. Hereditary angioedema with normal C1 inhibitor: update on evaluation and treatment. Immunol Allergy Clin North Am. 2017;37(3):571–584. doi:10.1016/j.iac.2017.04.004
8. Maurer M, Magerl M, Betschel S, et al. The international WAO/EAACI guideline for the management of hereditary angioedema - the 2021 revision and update. Allergy. 2022;77(7):1961–1990. doi:10.1111/all.15214
9. Bork K, Wulff K, Möhl BS, et al. Novel hereditary angioedema linked with a heparan sulfate 3-O-sulfotransferase 6 gene mutation. J Allergy Clin Immunol. 2021;148(4):1041–1048. doi:10.1016/j.jaci.2021.01.011
10. Henao MP, Kraschnewski JL, Kelbel T, Craig TJ. Diagnosis and screening of patients with hereditary angioedema in primary care. Ther Clin Risk Manag. 2016;12:701–711. doi:10.2147/TCRM.S86293
11. Farkas H, Martinez‐Saguer I, Bork K, et al. International consensus on the diagnosis and management of pediatric patients with hereditary angioedema with C1 inhibitor deficiency. Allergy. 2017;72(2):300–313. doi:10.1111/all.13001
12. Bork K, Wulff K, Hardt J, Witzke G, Staubach P. Hereditary angioedema caused by missense mutations in the factor XII gene: clinical features, trigger factors, and therapy. J Allergy Clin Immunol. 2009;124(1):129–134. doi:10.1016/j.jaci.2009.03.038
13. Deroux A, Boccon-Gibod I, Fain O, et al. Hereditary angioedema with normal C1 inhibitor and factor XII mutation: a series of 57 patients from the French National Center of Reference for Angioedema. Clin Exp Immunol. 2016;185(3):332–337. doi:10.1111/cei.12820
14. Bova M, Suffritti C, Bafunno V, et al. Impaired control of the contact system in hereditary angioedema with normal C1‐inhibitor. Allergy. 2020;75(6):1394–1403. doi:10.1111/all.14160
15. Bork K, Gül D, Hardt J, Dewald G. Hereditary angioedema with normal C1 inhibitor: clinical symptoms and course. Am J Med. 2007;120(11):987–992. doi:10.1016/j.amjmed.2007.08.021
16. Bork K. Diagnosis and treatment of hereditary angioedema with normal C1 inhibitor. Allergy Asthma Clin Immunol. 2010;6(1):15. doi:10.1186/1710-1492-6-15
17. Banday AZ, Kaur A, Jindal AK, Rawat A, Singh S. An update on the genetics and pathogenesis of hereditary angioedema. Genes Dis. 2020;7(1):75–83. doi:10.1016/j.gendis.2019.07.002
18. Zanichelli A, Longhurst HJ, Maurer M, et al. Misdiagnosis trends in patients with hereditary angioedema from the real-world clinical setting. Ann Allergy Asthma Immunol. 2016;117(4):394–398. doi:10.1016/j.anai.2016.08.014
19. Lara‐Marquez ML, Christiansen SC, Riedl MA, Herschbach J, Zuraw BL. Threshold‐stimulated kallikrein activity distinguishes bradykinin‐ from histamine‐mediated angioedema. Clin Exp Allergy. 2018;48(11):1429–1438. doi:10.1111/cea.13219
20. Bouillet L, Boccon‐Gibod I, Launay D, et al. Hereditary angioedema with normal C1 inhibitor in a French cohort: clinical characteristics and response to treatment with icatibant. Immun Inflamm Dis. 2017;5(1):29–36. doi:10.1002/iid3.137
21. BioCryst Pharmaceuticals, Inc. ORLADEYO™ (berotralstat) capsules, for oral use – highlights of prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/214094s000lbl.pdf.
22. European Medicines Agency. Summary of opinion (initial authorisation): Orladeyo: berotralstat. Available from: https://www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-orladeyo_en.pdf.
23. Kelbel T. A case of normal C1 esterase inhibitor hereditary angioedema successfully treated with berotralstat. Ann Allergy Asthma Immunol. 2022;128(4):462–463. doi:10.1016/j.anai.2022.01.014
24. Riedl MA, Banerji A, Gower R. Current medical management of hereditary angioedema: follow-up survey of US physicians. Ann Allergy Asthma Immunol. 2021;126(3):264–272. doi:10.1016/j.anai.2020.10.009
25. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D. The CARE Guidelines: consensus-based Clinical Case Reporting Guideline Development. Glob Adv Health Med. 2013;2(5):38–43. doi:10.7453/gahmj.2013.008
26. Maurer M, Magerl M. Differences and similarities in the mechanisms and clinical expression of bradykinin-mediated vs mast cell-mediated angioedema. Clin Rev Allergy Immunol. 2021;61(1):40–49. doi:10.1007/s12016-021-08841-w
27. Zuraw BL, Bork K, Binkley KE, et al. Hereditary angioedema with normal C1 inhibitor function: consensus of an international expert panel. Allergy Asthma Proc. 2012;33(Suppl 1):S145–S156. doi:10.2500/aap.2012.33.3627
28. Riedl MA, Danese M, Danese S, Ulloa J, Maetzel A, Audhya PK. Hereditary angioedema with normal C1 inhibitor: US Survey of Prevalence and Provider Practice Patterns. J Allergy Clin Immunol Pract. 2023;11(8):2450–2456 e6. doi:10.1016/j.jaip.2023.01.023
29. Kerkar P. What is the C1 esterase inhibitor test and why is it ordered? Available from: https://www.epainassist.com/test-and-procedures/what-is-the-c1-esterase-inhibitor-test.
30. Salguero CAS, Chacon AIS. HAE in children- what is the best treatment strategy? Approval of a drug. Int J Aller Medications. 2016;2(1):16. doi:10.23937/2572-3308.1510016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safety Aspects and Rational Use of Lanadelumab Injections in the Treatment of Hereditary Angioedema (HAE): Clinical Insights
Petkova E, Yordanova V, Staevska M, Valerieva A
Drug, Healthcare and Patient Safety 2022, 14:195-210
Published Date: 22 December 2022
A Review of Randomized Controlled Trials of Hereditary Angioedema Long-Term Prophylaxis with C1 Inhibitor Replacement Therapy: Alleviation of Disease Symptoms Is Achievable
Longhurst HJ, Valerieva A
Journal of Asthma and Allergy 2023, 16:269-277
Published Date: 9 March 2023
Prevention of Recurrent Attacks of Hereditary Angioedema (HAE): Berotralstat and Its Oral Bioavailability
Diaz-Menindez M, Morgenstern-Kaplan D, Cuervo-Pardo L, Alvarez-Arango S, Gonzalez-Estrada A
Therapeutics and Clinical Risk Management 2023, 19:313-317
Published Date: 30 March 2023