Back to Journals » Clinical Ophthalmology » Volume 14
Clinical Evaluation of a Novel Preloaded Intraocular Lens Delivery System During Routine Cataract Surgery
Authors Black D, Corbett D ![]() , Roberts TV, Cronin B
, Roberts TV, Cronin B ![]() , Smith PJ, Janakiraman DP, Jackson BE
, Smith PJ, Janakiraman DP, Jackson BE
Received 2 May 2020
Accepted for publication 8 July 2020
Published 12 August 2020 Volume 2020:14 Pages 2291—2300
DOI https://doi.org/10.2147/OPTH.S260925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Daniel Black,1 Dean Corbett,2 Timothy V Roberts,3,4 Brendan Cronin,5 Pamela J Smith,6 D Priya Janakiraman,6 Beth E Jackson6
1Sunshine Eye Clinic, Birtinya, Queensland, Australia; 2Auckland Eye Ltd, Auckland, New Zealand; 3Sydney Medical School, The University of Sydney, Sydney, New South Wales, Australia; 4Vision Eye Institute, Sydney, New South Wales, Australia; 5Queensland Eye Institute, South Brisbane, Queensland, Australia; 6Johnson & Johnson Surgical Vision, Inc., Santa Ana, CA, USA
Correspondence: Daniel Black Tel +61 7 5413-8000
Fax +61 7 5413-8080
Email [email protected]
Purpose: To evaluate the clinical handleability and acceptability of a novel preloaded intraocular lens (IOL) delivery system for implantation of the TECNIS ZCB00 IOL (Johnson & Johnson Surgical Vision, Inc., Santa Ana, CA, USA) during routine small-incision cataract surgery.
Subjects and Methods: In this prospective, open-label, noncomparative, unilateral or bilateral, multicenter study, adult subjects with unilateral or bilateral cataracts scheduled for IOL implantation were enrolled. Surgeons and surgical technicians completed per-eye day-of-surgery and end-of-surgical-day questionnaires. The primary endpoint of the study was the rate of acceptable overall clinical performance of the preloaded IOL delivery system. Other endpoints included additional responses from the questionnaires, preimplantation incision size, and safety.
Results: The study included 91 eyes that underwent cataract surgery and IOL implantation using the preloaded delivery system and were available for the 1-day postoperative visit. Five surgeons and 14 surgical technicians from four investigational sites participated in the study. The rate of acceptable overall clinical performance was 100% (91/91) of eyes, with most responses (78/91; 85.7%) being the highest possible rating of 5 (very satisfied). Favorable responses by most surgeons and surgical technicians regarding additional endpoints further highlighted the handleability and acceptability of the preloaded delivery system. No ocular adverse events or lens findings (ie, no cases of IOL instability, haptic breakage, IOL marking, or crimping) were reported.
Conclusion: The results of this study demonstrated that this preloaded IOL delivery system was safe and effective during routine small-incision cataract surgery.
Trial Registration: German Clinical Trials Register identifier, DRKS00014757.
Keywords: cataract surgery, IOL, preloaded delivery system, clinical handleability
Plain Language Summary
Surgeon and surgical technicians indicate that a new preloaded intraocular lens delivery system is safe and effective in adult subjects during small-incision cataract surgery.
Introduction
Advances in cataract surgery have allowed for intraocular lens (IOL) implantation through small incisions, thus improving postoperative outcomes, such as reduced astigmatism, reduced inflammation, and faster wound healing.1,2 Implantation of foldable IOLs via injection instead of forceps insertion is also thought to lower the risk of early postoperative infection, such as endophthalmitis, by eliminating contact between the IOL and the ocular surface.3,4
Several IOL delivery system options are currently available to surgeons during cataract surgery and generally consist of two broad categories: reusable and disposable. Reusable delivery systems usually comprise handpieces made from noncorrosive metals that can be cleaned and sterilized for reuse and that have a distal receiver for a disposable lens cartridge. The IOL can be housed in a daisy wheel that is manually loaded into the cartridge. However, manual loading of IOLs is associated with several disadvantages, including scratch marks on the optics of the IOL during loading; compression of the IOL during packaging that can result in irregularities on the surface of the optic; stretch marks on the posterior surface of the IOL during injection; surgeon’s error in holding and folding the IOL, leading to reversal of optic; uncontrolled unfolding; and damage resulting from entrapment of the haptic during manual loading into the cartridge or entrapment of the trailing haptic between the plunger and the cartridge.5–8 As a result, preloaded cartridges that can be attached to a reusable handpiece were developed to address these issues, potentially leading to improvements in surgical efficiency and reductions in surgical cost.9 For example, preloaded systems have been previously shown to provide faster, more predictable delivery of the IOL, thus reducing IOL loading errors and the need for additional IOL manipulations.10
Disposable delivery systems are generally single-use, plastic devices comprising a handpiece and a preloaded lens storage system (ie, a cartridge) in one package that can be disposed of after surgery. These disposable systems can provide a convenient, safe, and simple means of delivering a flexible IOL by simplifying and standardizing the preparation of the IOL for implantation. Although disposable preloaded systems have the potential to reduce loading errors that can lead to surgical complications, preloaded delivery systems have been associated with trapped trailing haptics during delivery into the capsular bag,11–14 as well as unfolding of the leading haptic during delivery.15
The UNFOLDER Vitan Handpiece (Model DK7799; Johnson & Johnson Surgical Vision, Inc., Santa Ana, CA, USA) was designed to provide a convenient, safe means of delivering a flexible IOL by simplifying and standardizing the lens preparation for implantation.16 This preloaded IOL delivery system utilizes the same cartridge as the TECNIS iTec Preloaded Delivery system (Johnson & Johnson Surgical Vision, Inc)17 and is similar to that of the UNFOLDER Ultra and Platinum 1 Series inserters, but consists of a reusable twist-style handpiece designed to produce a more controlled, efficient delivery of the preloaded IOL through a 2.2- to 2.4-mm incision.
This study evaluated the clinical handleability and acceptability of a new preloaded IOL delivery system for IOL implantation during routine small-incision cataract surgery.
Materials and Methods
Study Design
This prospective, open-label, noncomparative, unilateral or bilateral, multicenter study was conducted at four study sites with five investigators in New Zealand and Australia (German Clinical Trials Register [DRKS] identifier, DRKS00014757). The study duration was 2 days per eye, including a total of three to five study visits that comprised the following: preoperative examination of both eyes (within 45 days prior to surgery); operative examination for the first eye (0–45 days after preoperative examination; could be conducted on the same day at the investigator’s discretion); 1-day postoperative visit for the first eye; and operative visit and 1-day postoperative visit for the second eye in subjects who met the criteria for bilateral implantation. Ethics committee approval was obtained prior to the start of the trial, and all subjects provided written informed consent prior to their participation. The study was conducted in accordance with the Declaration of Helsinki.
Data on surgeon/surgical technician acceptability and handleability of the preloaded IOL delivery system were obtained through questionnaires completed by surgeons and surgical technicians at the end of each surgical case (ie, the per-eye day-of-surgery questionnaire) and at the end of each surgical day (ie, the end-of-surgical-day questionnaire).
Inclusion and Exclusion Criteria
Subjects were eligible for inclusion in the study if they were aged ≥22 years, had otherwise healthy eyes except for unilateral or bilateral cataracts that were scheduled for IOL implantation, and provided written informed consent.
Key exclusion criteria that applied to each eye included pupil abnormalities (ie, nonreactive, fixed pupils or abnormally shaped pupils) and a history of ocular trauma or ocular surgery that was not resolved/stable.
Descriptions of the Study IOL Delivery System
The study’s preloaded IOL delivery system comprised two major components: a disposable preloaded IOL delivery system and a reusable titanium inserter handpiece (Figure 1). The preloaded IOL delivery system contains the lens module, a preloaded ultraviolet light–absorbing posterior chamber IOL (TECNIS 1-piece monofocal IOL; Model ZCB00; Johnson & Johnson Surgical Vision, Inc.), and a cartridge coated with a hydrophilic coating (Biocoat; Biocoat Incorporated, Horsham, PA, USA) that can be hydrated with either balanced salt solution (BSS) or ophthalmic viscosurgical devices (OVDs) (Figure 1A). The lens module is a polypropylene IOL storage chamber that attaches to the molded cartridge. Delivery of the IOL is aided using haptic shelves (one for the distal haptic and one for the proximal haptic), which ensures that the haptics are completely folded as the IOL approaches the tip of the cartridge for optimal delivery. The modular cartridge of the preloaded IOL delivery system is snapped into the inserter handpiece, which is composed entirely of titanium alloy TI6AL-4V (Figure 1B). Both components are required for folding and inserting the IOL in the capsular bag during small-incision cataract surgery.
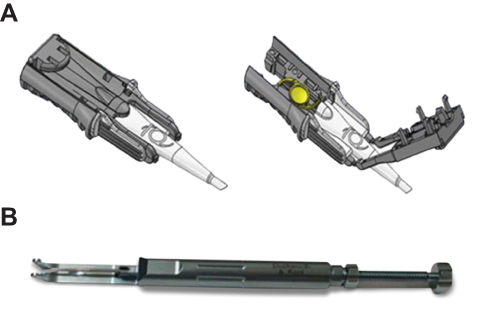 |
Figure 1 The UNFOLDER Vitan Handpiece (Model DK7799). This novel preloaded IOL delivery system consists of a disposable modular cartridge (A) and a reusable titanium handpiece (Model DK7799) (B). |
Surgical Technique
The study lens was prepared for implantation by the surgical technician or surgeon using the following process: hydration of the cartridge with BSS or OVD from the cartridge tip to the hydration port without filling the lens case; removal of the preloaded cartridge from the tray; and preparation of the IOL delivery system by snapping the modular cartridge to the back end of the titanium handpiece, engaging the rod and rotating a half turn. The IOL can be delivered immediately or can remain in the folded position for up to 10 mins; thus, to minimize haptic release time, it is recommended that the IOL is kept in this folded position within the delivery system for 3–10 mins.
Surgeons used their standard, small-incision (2.2–2.4 mm) cataract extraction surgical technique. The incision was either clear corneal, limbal, or scleral tunnel at the discretion of the surgeon. Cataract extraction was undertaken using phacoemulsification or aspiration with or without laser fragmentation. The study IOL was inserted into the capsular bag using the preloaded IOL delivery system, and BSS or an OVD could have been used by surgical technicians to advance the IOL into the folded position. If surgical complications occurred prior to IOL implantation, use of the study IOL delivery system was at the surgeon’s discretion.
Investigators were consistent with their assessment of standard preoperative, intraoperative, and postoperative medication regimens for each eye included in the study. If necessary, ocular serious adverse events (AEs) and/or device-related events were treated with routine ophthalmic medications or medications used to treat the event. All subjects underwent comprehensive preoperative assessment and had a full ophthalmic workup (eg, corrected and uncorrected visual acuity, fundus assessment, intraocular pressure).
Endpoints and Assessments
The primary endpoint of the study was the rate of acceptable overall clinical performance. The success criteria for this endpoint were defined as ≥95% for surgeon per-eye ratings of ≥3 for acceptable overall clinical performance, based on responses to the per-eye day-of-surgery question, “How do you rate the overall performance of the delivery system?” (1 = not satisfied, 3 = moderately satisfied, 5 = very satisfied).
Additional endpoints based on data obtained from the questionnaires completed by surgeons and surgical technicians were also evaluated. Ease-of-use of the preloaded IOL delivery system was assessed by surgeon and surgical technician responses to the following end-of-surgical-day questions: “How do you rate the overall ease-of-use of the insertion system?” (1 = poor/difficult, 5 = excellent/easy; surgeon question) and “Were you able to load the IOL within the 4 steps (hydrate, remove, prepare, and deliver)?” (yes/no; surgical technician question). Reduction of case time was assessed by surgeon responses to the end-of-surgical-day question, “Estimated time-savings per procedure in comparison to non-preloaded, reusable delivery systems”. Time-savings were estimated relative to the non-preloaded, reusable delivery system normally used by each surgeon (reported in minutes and seconds). The rate of removal of potential for loading errors was assessed by surgical technician and surgeon responses to the following end-of-surgical-day questions: “Do you foresee a reduction in loading errors using this delivery system compared to non-preloaded, reusable delivery systems?” (yes/no; surgical technician question) and “How much do you foresee a reduction in loading errors using this preloaded system compared to non-preloaded reusable delivery system?” (1 = not at all, 3 = no change, 5 = significant; surgeon question). Disposition of the IOL and IOL stability was assessed by surgeon and surgical technician responses to the following per-eye day-of-surgery questions: “Was the IOL centered in the capsular bag?” (yes/no; surgeon question) and “Was IOL folded properly prior to insertion (were haptics properly tucked)?” (yes/no; surgical technician question). Ergonomic design for comfort and control of the preloaded IOL delivery system was assessed by surgeon responses to the end-of-surgical-day question, “How do you rate the overall ergonomics (comfort and control ease) of the insertion system?” (1 = poor/difficult, 5 = excellent/easy). Controlled IOL delivery was assessed by surgeon end-of-surgical-day question, “Overall, were the IOL deliveries smooth and controlled?” (yes/no). Minimization of postoperative inflammation and infection was assessed by surgeon responses to the end-of-surgical-day question, “This delivery system will minimize the risk of infection and inflammation compared to non-preloaded, reusable delivery systems” (1 = do not agree, 3 = no difference, 5 = strongly agree).
Incision size was evaluated by reporting the proportion of eyes with preimplantation incision sizes ≤2.2 mm, 2.2 mm to 2.4 mm, and >2.4 mm. A surgical incision gauge was used to measure incision size.
Safety was assessed by reporting the incidence of ocular AEs and lens findings for the operative and 1-day postoperative visits. A slit-lamp examination was performed at the 1-day postoperative visit to identify potential cases of Descemet’s membrane detachment.
Statistical Analysis
Sample size calculation was based on the ability of a two-sided 95% confidence interval to have the precision to within 0.045 of the expected surgeon-acceptance proportion (95% with a score of ≥3 on a scale of 1–5). Based on this assumption, a sample size of 90 procedures was calculated.
The analysis population was based on all eyes implanted with a study IOL and exposed to the study product for questionnaire data rated for each eye and for other clinical data. The analysis group for the results of the questionnaire completed at the end of each surgery day comprised all end-of-surgery day forms for surgeons and surgical technicians.
The operative visit was the key analysis timepoint for the primary endpoint, which was analyzed by calculating the frequency and proportion of eyes with a value of ≥3 for the surgeon rating of the overall performance of the instrument. Analysis timepoints for additional endpoints and safety assessments were the operative and 1-day postoperative visits. Descriptive statistics included the mean and standard deviation (SD) or the frequency and proportion of questionnaire responses.
Results
Disposition and Baseline Characteristics
One-hundred eyes were enrolled in the study, of which 93 eyes underwent surgery and 91 were implanted with a study IOL. For eyes with a study IOL implanted, 78/91 eyes (85.7%) underwent surgery by three surgeons at one of the three Australian study sites (B.C., 27/91 eyes [29.7%]; D.B., 37/91 [40.7%]; T.V.R., 14/91 [15.4%]). The remaining 13/91 eyes (14.3%) underwent surgery by two surgeons at the single New Zealand study site (S.C., 2/91 [2.2%]; D.C., 11/91 [12.1%]). Seven subjects enrolled in the study were screen failures and were not implanted with a lens. In addition, 2/93 eyes were implanted with a nonstudy lens and were therefore excluded from the analysis. The questionnaire rating each eye at the operative visit was completed for all 91 eyes by five surgeons and 14 surgical technicians. There were 45 end-of-surgical-day evaluation forms completed at four investigational sites by five surgeons and 11 surgical technicians. All 91 eyes were available for the 1-day postoperative visit.
Baseline demographics of the study population are summarized in Table 1. Mean (SD) age of the study population was 75.4 (7.4) years, 51.6% were female, and 97.8% were not Hispanic/Latino.
 |
Table 1 Subject Demographics |
Overall Clinical Performance (Primary Endpoint)
For the primary effectiveness endpoint of the rate of acceptable overall clinical performance, 100% (91/91) of the eyes were rated as acceptable by the surgeons in response to the per-eye day-of-surgery question, “How do you rate the overall performance of the delivery system?” (Figure 2). Furthermore, most surgeon responses (78/91; 85.7%) to this question were the highest possible rating of 5 (very satisfied).
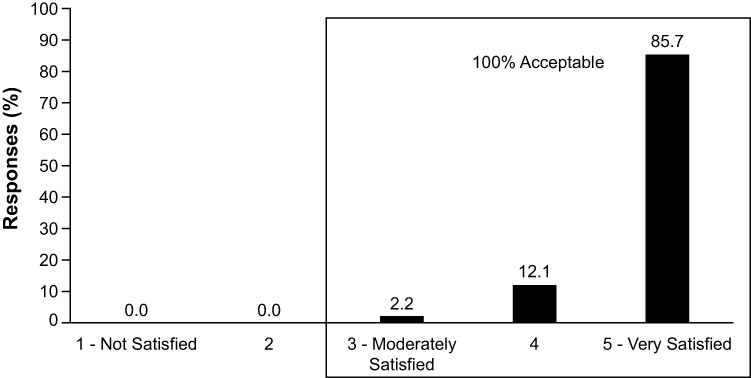 |
Figure 2 Rate of acceptable overall clinical performance (N = 91 eyes). |
Other Endpoints
Ease of Use
Figure 3 presents data based on surgeon end-of-surgical-day forms with responses to the question, “How do you rate the overall ease-of-use of the insertion system?” All responses (45/45; 100% of responses) had an acceptable rating of ≥4, with most responses (38/45; 84.4% of responses) being the highest possible rating of “excellent/easy.”
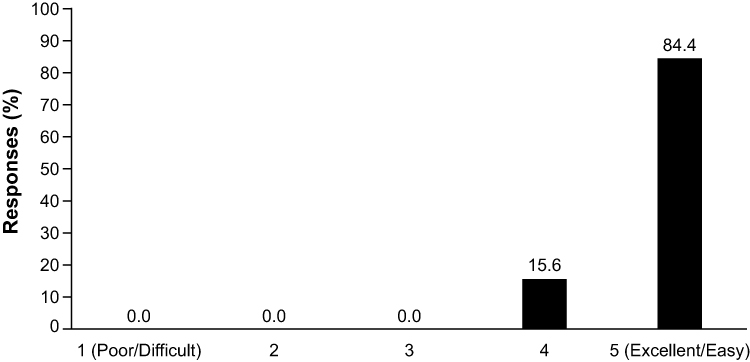 |
Figure 3 Surgeon’s overall ease-of-use evaluation. Based on end-of-surgical-day forms (N = 45 responses) for the question, “How do you rate the overall ease-of-use of the insertion system?” (1 = poor/difficult, 5 = excellent/easy). |
All surgical technicians responded “yes” on the end-of-surgical-day forms for the question, “Were you able to load the IOL within the 4 steps (hydrate, remove, prepare, and deliver)?” (45/45; 100% of responses).
Case Time and Incision Size
Based on all end-of-surgical-day forms, the mean (SD) estimated time-savings per procedure by the surgeon compared with non-preloaded delivery systems were 54.9 s (± 33.5 s). Analysis by study site reported median time-savings ranging from 30 to 90 s at three of the four study sites; one site reported little-to-no time-savings because the IOL was loaded by the surgical technician during the surgical procedure.
Of the 89 eyes with available data, preimplantation incision size ranged from 2.2 to 2.4 mm in most eyes (91.0%); all eyes had a preimplantation size of ≤2.4 mm. After implantation, 28.1% of eyes maintained an incision size of 2.2–2.4 mm, and 71.9% had an incision size of >2.4 mm.
Rate of Removal of Potential for Loading Errors
Based on all end-of-surgical-day forms, responses to the question, “Do you foresee a reduction in loading errors using this delivery system compared to non-preloaded, reusable delivery systems?” reported that most surgical technicians (42/45; 93.3%) anticipated a reduction in loading errors with the preloaded system. In addition, responses to the question based on all end-of-surgical-day forms, “How much do you foresee a reduction in loading errors using this preloaded system compared to non-preloaded reusable delivery system?” indicated that the surgeons foresaw that the delivery system will minimize the potential for loading errors. All responses (45/45; 100%) were rated a 4 or 5, and 57.8% (26/45) of the responses indicated the highest rating: “significant” reduction.
Disposition of the IOL and IOL Stability
Figure 4 presents data based on responses to surgeon and surgical technician questions on the disposition and stability of the study lens for each eye. In response to the question, “Was the IOL centered in the capsular bag?” all surgeons answered “yes” for all eyes (91/91; 100%). Similarly, all surgical technicians answered “yes” for all eyes (91/91; 100%) in response to the question, “Was IOL folded properly prior to insertion?”
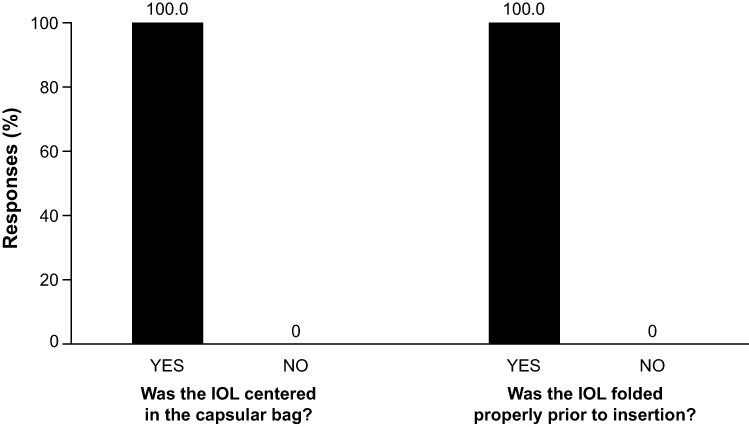 |
Figure 4 Evaluation of disposition of the IOL and IOL stability. Based on responses to the surgeon (N = 91 eyes) per-eye day-of-surgery question, “Was the IOL centered in the capsular bag?” (yes/no) and the surgical technician (N = 91 eyes) per-eye day-of-surgery question, “Was IOL folded properly prior to insertion (were haptics properly tucked)?” (yes/no). |
Ergonomic Design for Comfort and Control
Figure 5 presents data for surgeon ratings from all end-of-surgical-day forms based on responses to the question, “How do you rate the overall ergonomics (comfort and control ease) of the insertion system?” All of the responses (45/45; 100%) were acceptable with a rating of ≥3, and most responses (35/45; 77.8%) were of the highest rating: “excellent/easy.”
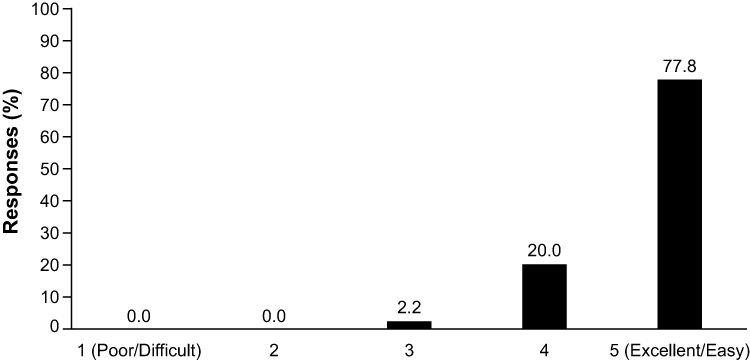 |
Figure 5 Surgeon evaluation of ergonomic design for comfort and control. Based on end-of-surgical-day forms (N = 45 responses) for the question, “How do you rate the overall ergonomics (comfort and control ease) of the insertion system?” (1 = poor/difficult, 5 = excellent/easy). |
Controlled IOL Delivery
Based on all end-of-surgical-day forms for surgeons, all responses (45/45; 100%) to the question “Overall, were the IOL deliveries smooth and controlled?” were affirmative.
Risk of Infection and Inflammation
Based on all end-of-surgical-day forms, responses to the statement, “This delivery system will minimize the risk of infection and inflammation compared to non-preloaded reusable delivery systems” indicated a strong surgeon agreement. All responses (45/45; 100%) were acceptable with a rating of ≥3, and most responses (31/45; 68.9%) were of the highest rating: “strongly agree.”
Safety
No ocular AEs were reported in this study. In addition, no lens findings (ie, no cases of IOL instability, haptic breakage, IOL marking, or crimping) were reported during the study. No cases of Descemet’s membrane detachment were observed at the 1-day postoperative visit.
Discussion
This study demonstrated that this novel preloaded IOL delivery system was safe and effectively delivered the IOL into the capsular bag during cataract surgery. The primary endpoint was met, with 100% of responses indicating that the overall performance of the delivery system was acceptable. In addition, the overall ease-of-use and ergonomic design of the preloaded IOL delivery system were rated as “excellent” by most surgeons, and substantial estimated time-savings per procedure were observed with the preloaded IOL delivery system over other non-preloaded delivery systems. This preloaded IOL delivery system assessed in this study also appeared to be safe, with no serious AEs or lens findings observed during the study.
To our knowledge, this is the first study to provide a comprehensive assessment of surgeon- and surgical technician–rated outcomes on the clinical handleability of an IOL delivery system. In a small, single-center retrospective study, implantation of a hydrophobic acrylic IOL using a preloaded delivery system was rated as “excellent” for ease of insertion and handling during cataract surgery in all 41 (100%) subjects enrolled in the study did not require manipulations of the IOL, and was not associated with AEs during surgery.18 Recently, a single-center clinical study evaluating two preloaded delivery systems demonstrated surgeon- and scrub nurse–rated reductions in preparation time, improvements in operating room workflow, and improvements in handling for both preloaded systems, compared with a manual delivery system.19
In the current study, small preimplantation incision sizes (≤2.4 mm) were observed in all cases. Previous nonclinical and clinical studies evaluating other automated/preloaded IOL delivery systems have also reported similar small incision sizes that ranged from 2.2 to 2.6 mm for most cases.11,18,20-24 The use of smaller incision sizes may be beneficial during IOL implantation as they can promote faster wound healing and reduce the risk of astigmatism, inflammation, and postoperative endophthalmitis.2,25-27
In the current study, surgeons reported an estimated mean time-savings per procedure of approximately 1 min when compared with other non-preloaded delivery systems. Time-and-motion data from a prospective, observational, multicenter study also reported that the TECNIS iTec Preloaded Delivery System significantly reduced total case time, reduced surgeon lens time, reduced surgeon delays, and eliminated lens touches during IOL preparation compared with a manually loaded IOL delivery system.17 In another prospective, observational, multicenter, time-and-motion study, the UltraSert preloaded IOL delivery system was associated with similar lens delivery times relative to a manual IOL delivery system (Monarch) but reductions in total intraoperative surgical case times.28 Therefore, switching from a manual/non-preloaded delivery system to a preloaded IOL delivery system has the potential to improve overall surgery time-savings per surgery day.
Additionally, another prospective observational study comparing the delivery characteristics of preloaded and non-preloaded IOL delivery systems reported that shorter average times for IOL implantation were observed for the preloaded delivery systems, which provided a more predictable delivery and eliminated lens touches.10 Several factors may contribute to the reduced case times observed with preloaded IOL delivery systems, such as screw-speed time and the delivery, unfolding, and stabilization of the folded IOL in the capsular bag. On the other hand, delays may arise as a result of trapped trailing haptics and uncontrolled unfolding of the leading haptic during delivery into the capsular bag. Indeed, cases of trapped trailing haptics (7–19%) and uncontrolled unfolding of the leading haptic (13%) have been reported in currently available preloaded delivery systems.11,12,15 Therefore, the anticipated reductions in case time for the preloaded IOL delivery system in the current study may be explained by a combination of these factors, suggesting that this system provides efficient and controlled delivery of the IOL while maintaining an acceptable enhanced safety profile during cataract surgery.
Potential limitations of note should be taken into consideration when interpreting the findings of this study. The inclusion of 5 surgeons and 14 surgical technicians in the study may have resulted in variable responses to day-of-surgery and end-of-surgical-day questionnaires. Further, the focus of the study was on qualitative, not quantitative, data (ie, time saved), as the key findings from this study were obtained from the surgeon- and surgical technician-rated responses to day-of-surgery and end-of-surgical-day questionnaires. Finally, direct comparison with other IOL delivery systems was not possible given the lack of an active control arm.
Conclusion
In conclusion, the results of this study demonstrate that this novel preloaded IOL delivery system is a safe and effective delivery system for IOL implantation during cataract surgery.
Abbreviations
AE, adverse event; BSS, balanced salt solution; IOL, intraocular lens; OVD, ophthalmic viscosurgical device; SD, standard deviation.
Data Sharing Statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymized data may be granted following review.
Acknowledgments
We wish to thank all patients and investigators who participated in this study. The following investigative sites and surgeons participated in this clinical program: Sunshine Eye Clinic, Birtinya, Queensland, Australia (Daniel Black, MD); Auckland Eye Ltd, Auckland, New Zealand (Stuart Carroll, MD; Dean Corbett, MD); Vision Eye Institute, Sydney, New South Wales, Australia (Timothy V. Roberts, MMed, MD); and Queensland Eye Institute, South Brisbane, Queensland, Australia (Brendan Cronin, MD). Manuscript development and editorial support were provided by ApotheCom (San Francisco, CA, USA) and funded by Johnson & Johnson Surgical Vision, Inc.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
D. Black reports grants from Johnson & Johnson Vision during the conduct of the study, and personal fees from Johnson & Johnson Surgical Vision outside the submitted work. D. Corbett reports personal fees for service outside the submitted work from and acts as a consultant for Johnson & Johnson Surgical Vision, receiving funds for work done including medical consultation and surgery paid at market rates and honoraria and travel expenses commensurate with true costs incurred. T.V. Roberts reports grants from Johnson & Johnson Surgical Vision during the conduct of the study, and speaker fees from Johnson & Johnson Surgical Vision outside the submitted work. B. Cronin received personal fees from Johnson & Johnson Surgical Vision outside the submitted work. P.J. Smith, D.P. Janakiraman, and B.E. Jackson are current employees of Johnson & Johnson Surgical Vision.
References
1. Oshika T, Nagahara K, Yaguchi S, et al. Three year prospective, randomized evaluation of intraocular lens implantation through 3.2 and 5.5 mm incisions. J Cataract Refract Surg. 1998;24(4):509–514. doi:10.1016/S0886-3350(98)80293-9
2. Masket S, Wang L, Belani S. Induced astigmatism with 2.2- and 3.0-mm coaxial phacoemulsification incisions. J Refract Surg. 2009;25(1):21–24. doi:10.3928/1081597X-20090101-04
3. Weston K, Nicholson R, Bunce C, Yang YF. An 8-year retrospective study of cataract surgery and postoperative endophthalmitis: injectable intraocular lenses may reduce the incidence of postoperative endophthalmitis. Br J Ophthalmol. 2015;99(10):1377–1380. doi:10.1136/bjophthalmol-2014-306372
4. Mayer E, Cadman D, Ewings P, et al. A 10 year retrospective survey of cataract surgery and endophthalmitis in a single eye unit: injectable lenses lower the incidence of endophthalmitis. Br J Ophthalmol. 2003;87(7):867–869. doi:10.1136/bjo.87.7.867
5. Nguyen DQ, Saleh TA, Pandey SK, Bates AK. Irregularities on the surface of single-piece AcrySof SA60AT intraocular lenses. J Cataract Refract Surg. 2006;32(3):495–498. doi:10.1016/j.jcrs.2005.12.074
6. Faschinger CW. Surface abnormalities on hydrophilic acrylic intraocular lenses implanted by an injector. J Cataract Refract Surg. 2001;27(6):845–849. doi:10.1016/S0886-3350(00)00804-X
7. Rao SK, Leung AT, Lam DS, Padmanabhan P. In situ tumbling of the AcrySof intraocular lens. J Cataract Refract Surg. 2000;26(2):177–179. doi:10.1016/S0886-3350(99)00347-8
8. Dada T, Muralidhar R. Insertion of the sensar IOL via the Monarch II delivery system. J Cataract Refract Surg. 2005;31(9):1684–1685. doi:10.1016/j.jcrs.2005.09.008
9. Shimizu K, Kobayashi K, Takayama S, Zhaobin G. Preloaded injector for intraocular lens implantation without the use of ophthalmic viscosurgical devices. J Cataract Refract Surg. 2008;34(7):1157–1160. doi:10.1016/j.jcrs.2008.03.034
10. Chung B, Lee H, Choi M, Seo KY, Kim EK, Kim TI. Preloaded and non-preloaded intraocular lens delivery system and characteristics: human and porcine eyes trial. Int J Ophthalmol. 2018;11(1):6–11. doi:10.18240/ijo.2018.01.02
11. Mendicute J, Amzallag T, Wang L, Martinez AA. Comparison of incision size and intraocular lens performance after implantation with three preloaded systems and one manual delivery system. Clin Ophthalmol. 2018;12:1495–1503. doi:10.2147/OPTH.S166776
12. Ong HS, Subash M, Sandhu A, Wilkins MR. Intraocular lens delivery characteristics of the preloaded AcrySof IQ SN60WS/AcrySert injectable lens system. Am J Ophthalmol. 2013;156(1):77–81.e72. doi:10.1016/j.ajo.2013.01.032
13. Rajesh R. Evaluation of semi-preloaded intraocular lens delivery system. ROM J Ophthalmol. 2019;63(1):56–60. doi:10.22336/rjo.2019.9
14. Wang L, Wolfe P, Chernosky A, Paliwal S, Tjia K, Lane S. In vitro delivery performance assessment of a new preloaded intraocular lens delivery system. J Cataract Refract Surg. 2016;42(12):1814–1820. doi:10.1016/j.jcrs.2016.10.014
15. Chaudhary S. Preloaded injectable intraocular lenses: the way forward. Indian J Ophthalmol. 2018;66(3):477. doi:10.4103/ijo.IJO_286_18
16. Johnson & Johnson Vision Inc. TECNIS 1-Piece IOL and SmartLOAD Delivery Technology DFU. Santa Ana, CA: Johnson & Johnson Vision Inc; 2019.
17. Jones JJ, Chu J, Graham J, Zaluski S, Rocha G. The impact of a preloaded intraocular lens delivery system on operating room efficiency in routine cataract surgery. Clin Ophthalmol. 2016;10:1123–1129. doi:10.2147/OPTH.S107726
18. Acar B, Torun IM, Acar S. Evaluation of preloaded IOL delivery system and hydrophobic acrylic intraocular lens in cataract surgery. Open Ophthalmol J. 2018;12:94–103. doi:10.2174/1874364101812010094
19. Borkenstein AF, Borkenstein EM. [Safety first - evaluation of IOL Injector systems]. Klin Monbl Augenheilkd. 2019;236(8):976–982. doi:10.1055/a-0867-9853. German.
20. Haldipurkar SS, Shetty V, Haldipurkar T, et al. Incision size changes after cataract surgery with intraocular lens implantation: comparison of 2 preloaded IOL implantation injectors. J Cataract Refract Surg. 2020;46(2):222–227. doi:10.1097/j.jcrs.0000000000000014
21. Oshika T, Wolfe P. In vitro comparison of delivery performance of 4 preloaded intraocular lens injector systems for corneal and sclerocorneal incisions. J Cataract Refract Surg. 2019;45(6):840–846. doi:10.1016/j.jcrs.2018.10.050
22. Mencucci R, Favuzza E, Salvatici MC, Spadea L, Allen D. Corneal incision architecture after IOL implantation with three different injectors: an environmental scanning electron microscopy study. Int Ophthalmol. 2019;39(2):397–403. doi:10.1007/s10792-018-0825-2
23. Wang L, Wolfe P, Paliwal S, Chernosky A, Kohnen T. Comparative evaluation of corneal incision enlargement after intraocular lens delivery of new preloaded and manual implantation systems. Eur J Ophthalmol. 2019;1120672119882334.
24. Liu J, Wolfe P, Hernandez V, Kohnen T. Comparative assessment of the corneal incision enlargement of four preloaded IOL delivery systems. 2020. J Cataract Refract Surg.
25. Khokhar S, Sharma R, Patil B, Aron N, Gupta S. Comparison of new motorized injector vs manual injector for implantation of foldable intraocular lenses on wound integrity: an ASOCT study. Eye. 2014;28(10):1174–1178. doi:10.1038/eye.2014.162
26. Hayashi K, Yoshida M, Hayashi H. Postoperative corneal shape changes: microincision versus small-incision coaxial cataract surgery. J Cataract Refract Surg. 2009;35(2):233–239. doi:10.1016/j.jcrs.2008.10.031
27. Elkady B, Piñero D, Alió JL. Corneal incision quality: microincision cataract surgery versus microcoaxial phacoemulsification. J Cataract Refract Surg. 2009;35(3):466–474. doi:10.1016/j.jcrs.2008.11.047
28. Goldberg D, Coyle KB, Keith MS, Jones MP, Lane SS, Kim T U.S. multicenter study of time, operational, and economic efficiencies associated with a new preloaded IOL delivery system.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.