Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Clinical Efficacy of Endoscopy-Assisted Anterior Cervical Discectomy and Fusion for Single-Segment Cervical Spondylotic Myelopathy: A Retrospective, Propensity Score-Matched Study
Authors Li T, Ma J, Zhang H, Jiang Q, Ding Y ![]()
Received 17 September 2025
Accepted for publication 10 December 2025
Published 22 December 2025 Volume 2025:21 Pages 1795—1805
DOI https://doi.org/10.2147/TCRM.S568319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Tusheng Li,* Jingbo Ma,* Hanshuo Zhang, Qiang Jiang, Yu Ding
Orthopedics of TCM Senior Department, the Sixth Medical Center of PLA General Hospital, Beijing, People’ s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Ding, Orthopedics of TCM Senior Department, the Sixth Medical Center of PLA General Hospital, Beijing, People’ s Republic of China, Email [email protected]
Purpose: Endoscopy-assisted anterior cervical discectomy and fusion (EA-ACDF), which integrates the advantages of conventional ACDF and spinal endoscopy, is an innovative technique for treating cervical spondylotic myelopathy (CSM). We compared the clinical efficacy of EA-ACDF and ACDF for treating patients with single-segment CSM.
Methods: One-hundred and thirty-six CSM patients were retrospectively included from January 2021 to September 2023, of whom 61 underwent EA-ACDF and 75 underwent ACDF. Propensity score matching (PSM) was conducted to adjust for imbalances in covariates between groups. Then, clinical and imaging outcomes, perioperative data, and complications were compared.
Results: After matching, 108 patients were included and followed for 15– 38 months. Compared to the ACDF group, the EA-ACDF group had less intraoperative bleeding volume, less drainage volume, and shorter postoperative hospital stays (P < 0.05). At 7 days and 3 months after the surgery, the visual analog scale (VAS), Japanese Orthopedic Association score (JOA), and neck disability index (NDI) improved more significantly in the EA-ACDF group (P < 0.05). Regarding imaging, intervertebral height index (IHI), C2-7 cervical lordosis (C2-7 CL), and C2-7 range of motion (C2-7 ROM) exhibited no statistical differences between the two groups (P > 0.05). The complication rates between the EA-ACDF (3.7%) and ACDF (14.8%) groups demonstrated statistical differences (P = 0.046).
Conclusion: Both EA-ACDF and conventional ACDF for single-segment CSM provide satisfactory clinical efficacy. The EA-ACDF procedure provides a clearer surgical field, causes less trauma, allows faster recovery, and has the potential to reduce the risk of complications.
Keywords: cervical spondylotic myelopathy, anterior cervical discectomy and fusion, spinal endoscopy, complications, propensity score matching
Introduction
Cervical spondylotic myelopathy (CSM) has a high prevalence in those older than 55 years of age, leading to spinal cord dysfunction.1,2 Clinically, patients with CSM mainly present with neck-shoulder pain, limb sensory deficits, and motor dysfunction.3,4 Surgery is essential for patients with a clear diagnosis of CSM, which can prevent neurological deterioration. Anterior cervical discectomy and fusion (ACDF) is the standard procedure for treating CSM, due to its advantages in adequate neural decompression and restoration of cervical stability and lordosis.5,6 Nevertheless, the ACDF technique has inherent shortcomings, such as a limited surgical field, difficulties in hemostasis, poor resolution of anatomical structures, and a high risk of decompression of the posterior margin of the vertebral body and spinal cord surface.7,8
With the advances in minimally invasive spine surgery, spinal endoscopic techniques are increasingly applied to cervical ACDF procedures. Due to the presence of clear vision, easy identification of anatomical structures, and more convenient hemostasis, endoscopic surgery can compensate for the inherent limitations of conventional ACDF, making minimally invasive ACDF possible.7,9 Endoscopic-assisted ACDF (EA-ACDF) is a new type of assisted ACDF procedure that fully utilizes the advantages of aqueous and air media with the aim of providing better clinical guidance for the endoscopic treatment of cervical spondylosis. This surgical approach allows for precise decompression under endoscopy, thus avoiding damage to the spinal cord and nerves.9 In 2024, Wu et al7 retrospectively analyzed data from 52 patients with CSM who underwent EA-ACDF or ACDF. They indicated that EA-ACDF could provide better postoperative pain relief and improve the clinical function of the cervical spine. However, the authors did not demonstrate postoperative imaging characteristics and failed to balance confounders in the study design. Currently, there are few clinical studies on the treatment of cervical spondylosis with EA-ACDF, and its feasibility and effectiveness need further exploration. Thus, we compared EA-ACDF with ACDF for treating CSM in terms of clinical function, imaging, and complications. Meanwhile, we applied propensity matching to balance between-group confounding factors and increase the reliability of our findings.
Materials and Methods
Patients’ Data
From January 2021 to September 2023, 136 consecutive eligible patients with CSM at our institution were retrospectively analyzed, of whom 61 underwent EA-ACDF (the EA-ACDF group) and 75 underwent conventional ACDF (the ACDF group). This study was conducted according to the Declaration of Helsinki, with approval obtained from the Ethics Committee of the Sixth Medical Center of PLA General Hospital (HZKY-PJ-2024-18). Patients signed informed consent before surgery.
The inclusion criteria were (1) cervical spinal cord compression with a definitive diagnosis of CSM on imaging; (2) patients with single-segment CSM; (3) ineffective conservative treatment; and (4) suitable for surgery under general anesthesia. The exclusion criteria were (1) presence of cervical spine deformity, infection, or tumor; (2) patients with severe hypertrophy of the ligamentum flavum and severe ossification of the posterior longitudinal ligament (OPLL); (3) developmental cervical stenosis; (4) previous cervical spine surgery; (5) history of mental diseases; (6) incomplete follow-up information.
Considering the nonrandomization of the design and the unbalanced preoperative characteristics, our study implemented a propensity score matching (PSM) to control the influence of confounding factors on the experimental results. Covariates considered to be of practical clinical significance were included, including (1) age, (2) gender, (3) body mass index (BMI), (4) medical history, (5) operative segment, and (6) smoking history.
Surgical Procedure
The same team of surgeons performed all surgeries, following a procedure similar to that described by Wu et al.7 The operation was performed under general anesthesia, and the operative segment was recognized intraoperatively by fluoroscopy. Then, an incision of about 3–4 cm was made in the right anterior neck. Subcutaneous tissues and the platysma muscle were incised sequentially, and blunt and sharp detachments were conducted along the deep layers of the platysma muscle. The deep fascia was incised along the inner edge of the sternocleidomastoid muscle and bluntly separated from the underlying space between the visceral sheath and the vascular sheath to the prevertebral fascia. The prevertebral fascia was cut open to expose the disc. Thereafter, the localization pins were placed in the proximal vertebral body margin. After confirming the responsible segment under fluoroscopy again, the Casper retractor screws were placed in the center of the vertebral body at the upper and lower levels of the responsible segment. Then, the Casper retractors were attached to distract the vertebral body at both ends.
The EA-ACDF Approach
A spinal endoscopic imaging system was attached and the endoscope was inserted. Under aqueous media, the anterior longitudinal ligament and the anterior fibrous ring were incised. Next, the nucleus pulposus was removed using nucleus pulposus forceps, and the cartilaginous endplates were scraped using a small scraper. A power grinder drill and vertebral plate forceps were applied to accurately abrade the osteophyte at the posterior edge of the vertebral body. Then, the fibrous ring and posterior longitudinal ligament were dissected, and the epidural space was explored and decompressed. After confirming the adequate decompression of the dural sac, the proper type of interbody fusion device was placed and fixed with screws. Finally, following sufficient hemostasis, a drain was positioned and the incision was sutured. Figures 1 and 2 depict an endoscopic diagram and a representative case of EA-ACDF, respectively.
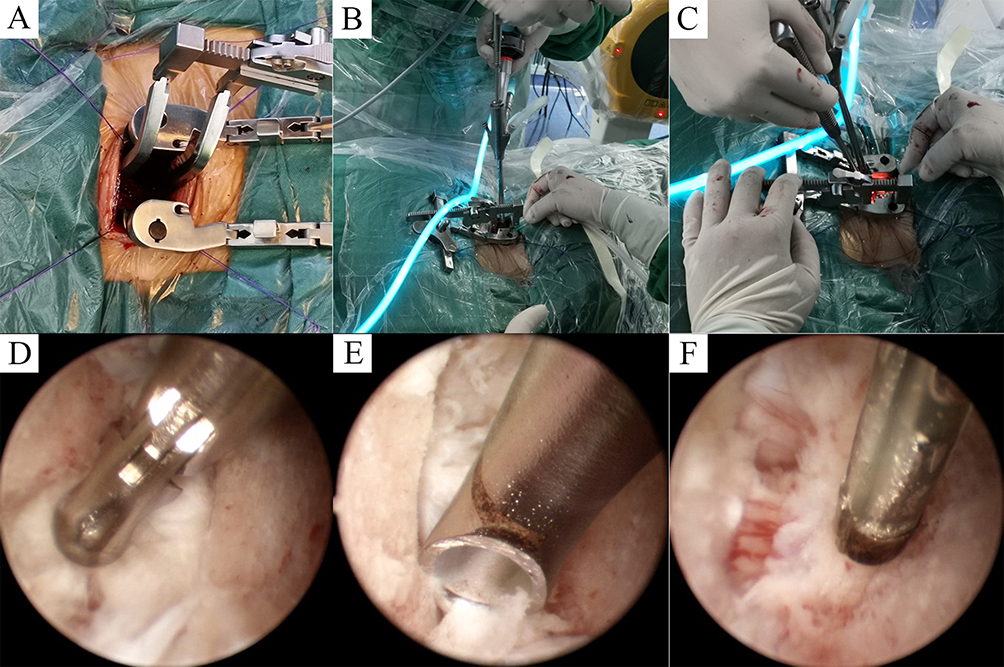 |
Figure 1 Schematic diagram of EA-ACDF technique. (A) Conventional ACDF incision was made; (B and C) Placement of spinal endoscope and then operation; (D) The nucleus pulposus was removed using a nucleus pulposus forceps under endoscopy; (E) A small scraper was used to scraped disc tissue and cartilaginous endplates; (F) Dural sac decompression. |
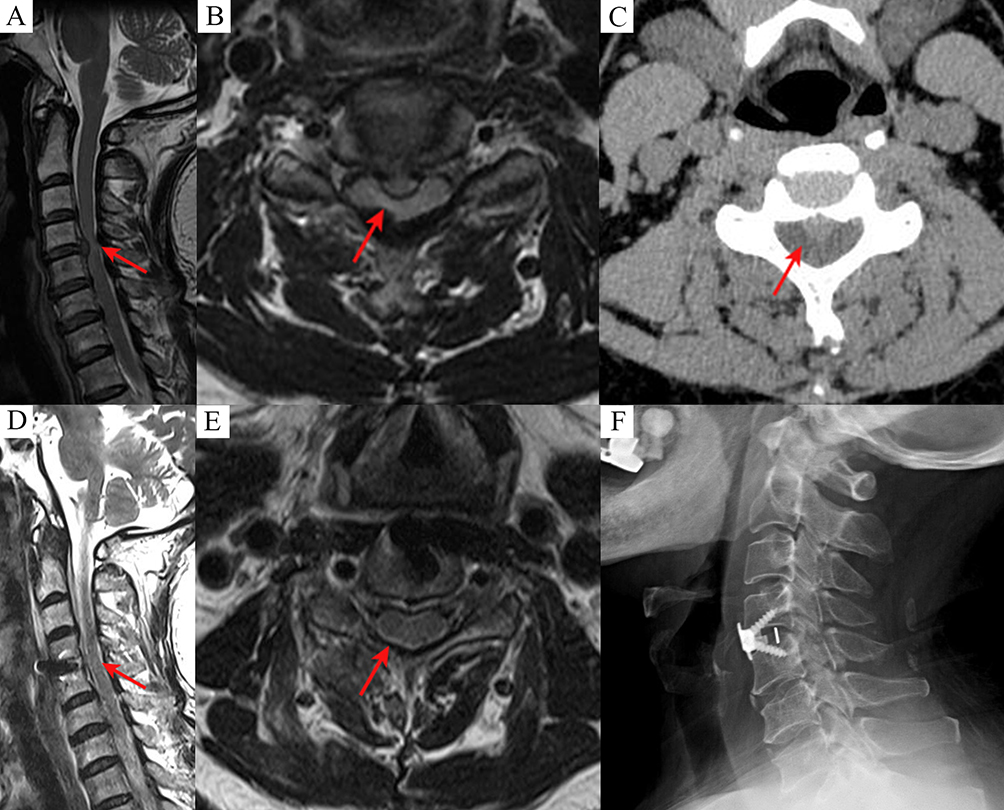 |
Figure 2 Representative case from EA-ACDF. (A–C) Preoperative MRI and CT images indicated C4–5 segment disc herniation compressing the spinal cord (red arrow indicating the herniated disc compressing the spinal cord); (D and E) MRI confirmed the removal of the herniated disc and adequate decompression of the spinal cord (red arrow indicating the herniated disc was removed to decompress the spinal cord); (F) Interbody fusion with internal fixation after surgery. |
The ACDF Approach
The patient was operated on with conventional ACDF without the assistance of spinal endoscopy. Under an air medium, a curette was utilized to scrape the cartilaginous endplates and the remaining nucleus pulposus tissue from the disc. Thereafter, vertebral plate bone forceps were applied to resect the hyperplastic posterior facet joints and the osteophyte of the posterior edge of the vertebral body. After confirming the satisfactory decompression of the dural sac, a proper type of interbody fusion device was placed and secured with screws. Following proper hemostasis, a drain was positioned and the incision was sutured.
Perioperative Data Collection
Perioperative information for all matched CSM patients was compiled, including incision length, operative time, intraoperative blood loss, drainage volume, and postoperative hospital stay. Intraoperative blood loss was estimated based on the amount of change in hematocrit (Hct),10 calculated based on the following formula: intraoperative blood loss (mL) = [(preoperative HCT – HCT on postoperative day 2) / preoperative HCT] × body weight (kg) × 7% × 1000 + intraoperative blood transfusion (mL).
Clinical Assessment
The visual analog score (VAS) was applied to evaluate patients’ neck and/or upper limb pain, whereas the Japanese Orthopaedic Association Score (JOA) and the neck disability index (NDI) were used to determine the status of cervical neurologic function. Questionnaires were evaluated preoperatively, at 7 days, 3 months, 6 months, and 12 months postoperatively, and at the last follow-up.
Imaging Measurement
All patients underwent cervical spine X-ray examinations preoperatively, at 3 months postoperatively, and at the last follow-up. The imaging data included intervertebral height index (IHI), C2-7 cervical lordosis (C2-7 CL) and C2-7 range of motion (C2-7 ROM). The IHI is the height of the responsible intervertebral space normalized against the height of the adjacent vertebrae. Based on a previously reported method,11 the heights of the anterior, middle, and posterior edges were measured separately and averaged. The C2-7 CL was measured using Cobb’s method,12 which refers to the angle between the lower endplate of the C2 and C7. The C2-7 ROM was the relative range of motion between hyperextension and hyperflexion of the cervical C2-7 angle. To minimize measurement error, the imaging data were obtained from two independent evaluators and averaged (Figure 3).
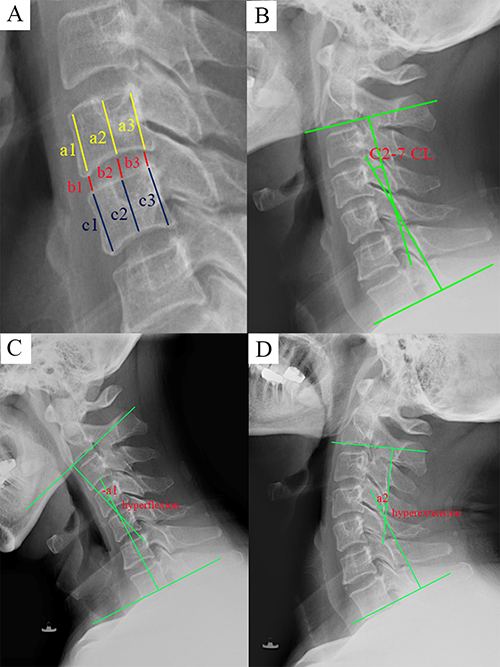 |
Figure 3 An illustration of imaging measurements. (A) The measurement of IHI, IHI = [2(b1+b2+b3)]/[(a1+a2+a3) + (c1+c2+c3)] * 100%; (B) The measurement of C2-7 CL; (C and D)The measurement of C2-7 ROM in hyperflexion and hyperextension; C2-7 ROM = a2 - (-a1). |
Statistical Analysis
Data analysis was conducted using IBM SPSS Statistics 25.0. The normality of continuous variables was assessed using the Kolmogorov–Smirnov test (all group sample sizes > 50), with P ≥ 0.05 indicating a normal distribution. An independent samples t-test was conducted to compare normally distributed continuous data, and exhibited as mean ± standard deviation. Mann–Whitney U-test was applied for non-normally distributed continuous data, and expressed as median (Q1, Q3). Categorical data were analyzed using the chi-square test or Fisher’ s exact test, and presented as frequencies and percentages. Nonparametric tests for related samples and repeated measures analysis of variance were utilized to compare data at different time points within groups. A p-value lower than 0.05 was considered statistically significant.
To reduce selection bias between the two groups, we performed PSM. Propensity scores were estimated using a logistic regression model with group (EA-ACDF vs ACDF) as the dependent variable and age, gender, BMI, medical history, operative segment, and smoking history as independent variables. Patients in the EA-ACDF group were then matched 1:1 to those in the ACDF group on the propensity score using a caliper-based matching algorithm without replacement, with a caliper width of 0.02 on the propensity score scale. Matching was implemented using the PSM procedure in SPSS version 25.0, with randomized case order when drawing matches to minimize order-related bias. Covariate balance before and after PSM was assessed by comparing baseline characteristics between the two groups using appropriate statistical tests (independent samples t-test or Mann–Whitney U-test for continuous variables and chi-square or Fisher’s exact test for categorical variables). A p-value < 0.05 was considered to indicate imbalance, whereas P ≥ 0.05 was regarded as acceptable balance.
Results
Table 1 presents the preoperative general information before matching patients in the two groups, and two unbalanced confounders were identified, including age and smoking history. After matching, 108 patients were included in this study and all confounders exhibited balance (Table 2). The average follow-up length was 24.22 ± 6.30 months (span of 15–38 months) in the EA-ACDF group, compared to 24.06 ± 6.11 months in the ACDF group (span of 15–38 months) (P = 0.889).
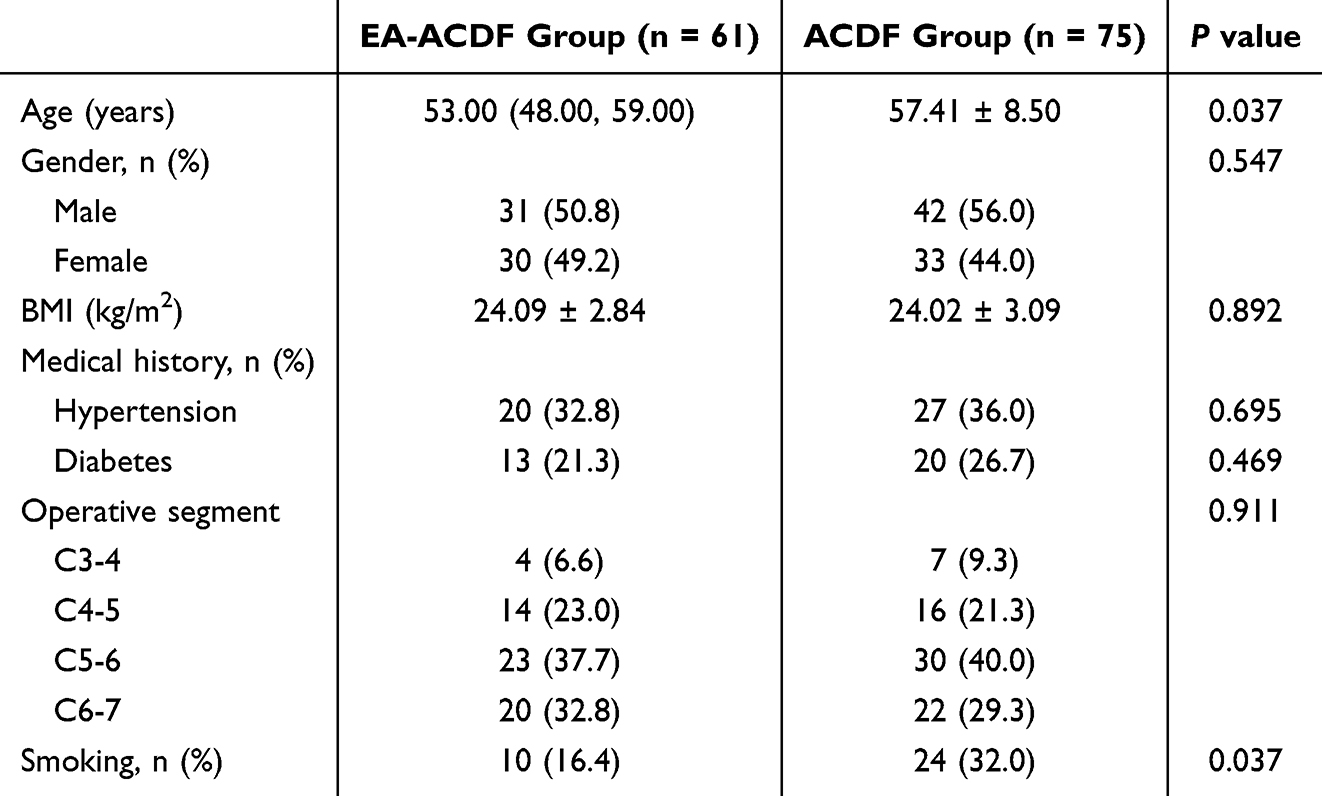 |
Table 1 General Information Before PSM |
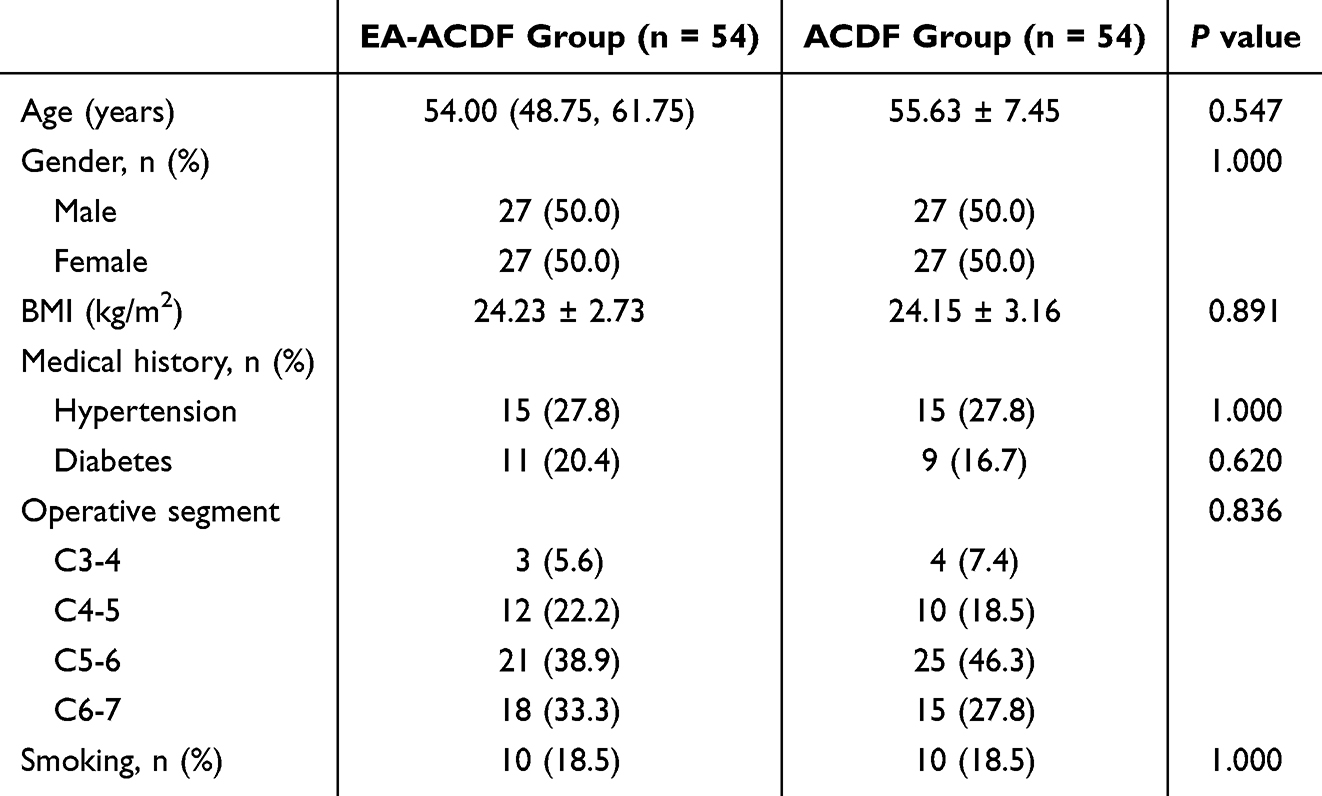 |
Table 2 General Information After PSM |
Perioperative Data
Table 3 summarizes the perioperative data in both groups. Compared with the ACDF group, the EA-ACDF group had a longer operative time (P < 0.05). However, EA-ACDF showed less intraoperative bleeding, less drainage volume, and shorter postoperative hospital stays (P < 0.05), indicating the advantages of less trauma and faster postoperative recovery. The length of incision did not show statistical differences between the two groups (P > 0.05).
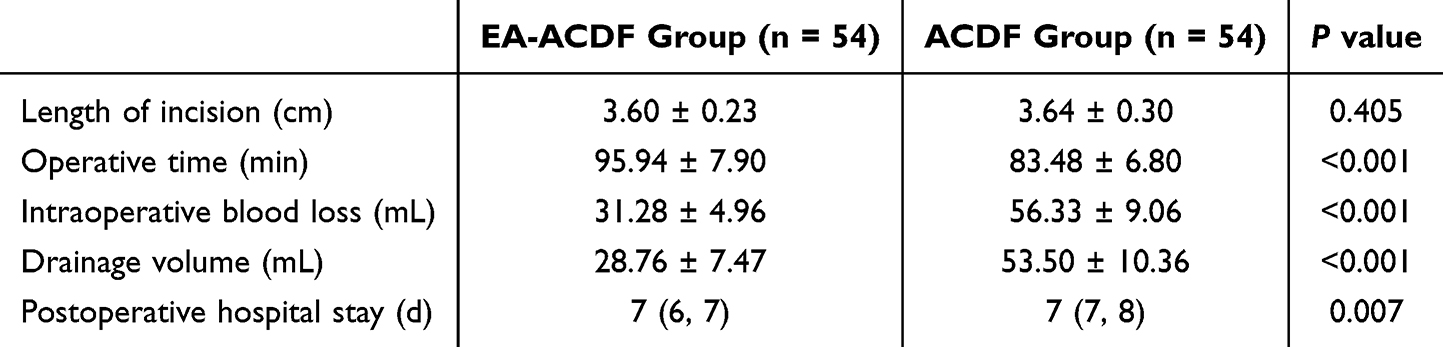 |
Table 3 Perioperative Data of the Two Groups |
Clinical Outcomes
The clinical findings are presented in Table 4. Compared to the preoperative level, postoperative clinical functional scores in both groups exhibited great improvements (P < 0.05), indicating that both surgical procedures were effective in treating CSM. At 7 days and 3 months after surgery, compared to the ACDF group, greater improvements in VAS, JOA, and NDI were found in the EA-ACDF group (P < 0.05), suggesting that EA-ACDF was superior to ACDF in pain relief and neurological recovery after surgery.
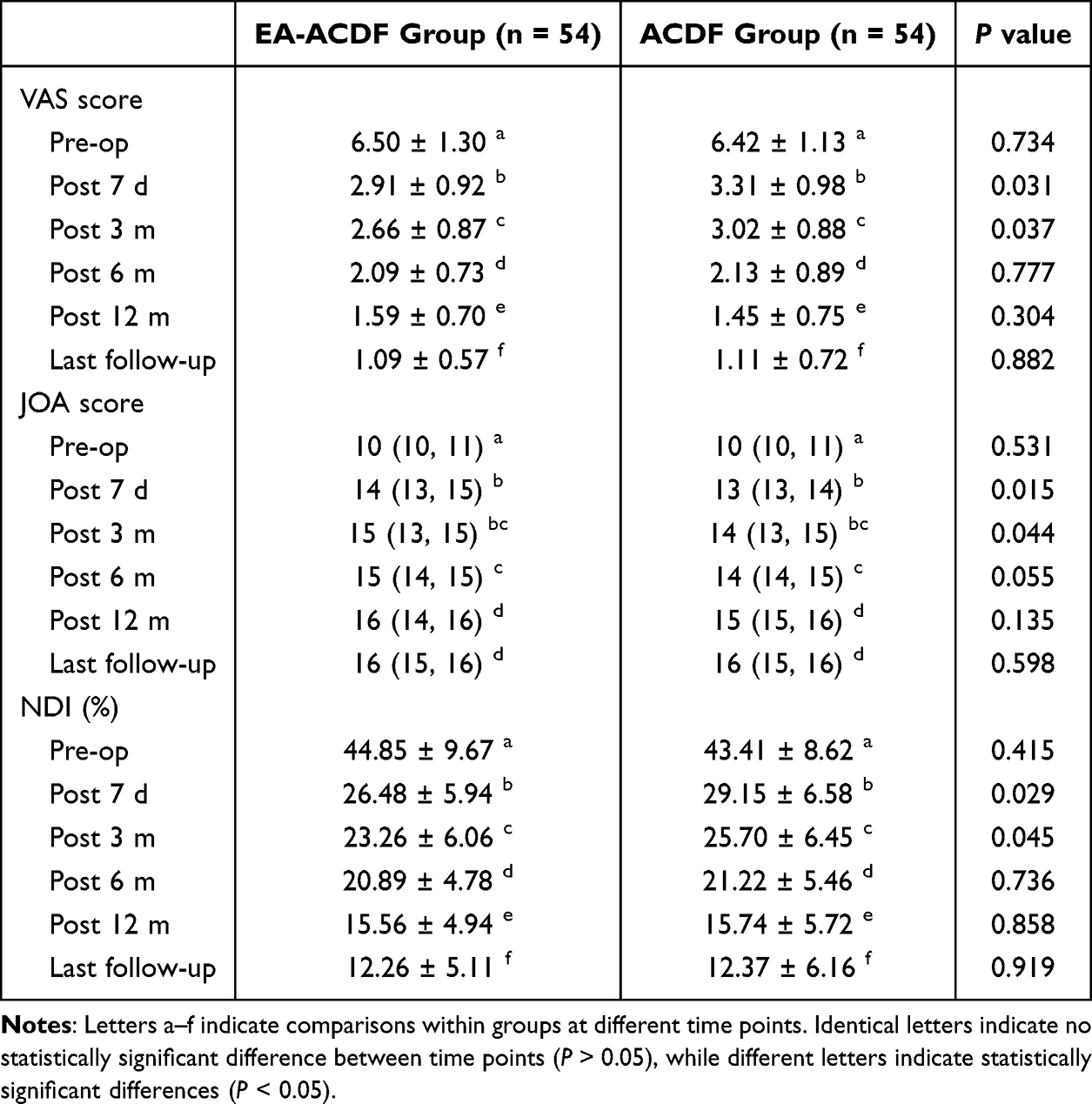 |
Table 4 Clinical Outcomes of the Two Groups |
Imaging Outcomes
Table 5 exhibits the imaging findings of the two groups. The differences in IHI, C2-7 CL and C2-7 ROM between the two groups were not statistically significant (P > 0.05). However, postoperative IHI and C2-7 CL were significantly improved in both groups compared with preoperative values (P < 0.05), indicating that both procedures were effective in restoring and maintaining intervertebral height and cervical curvature.
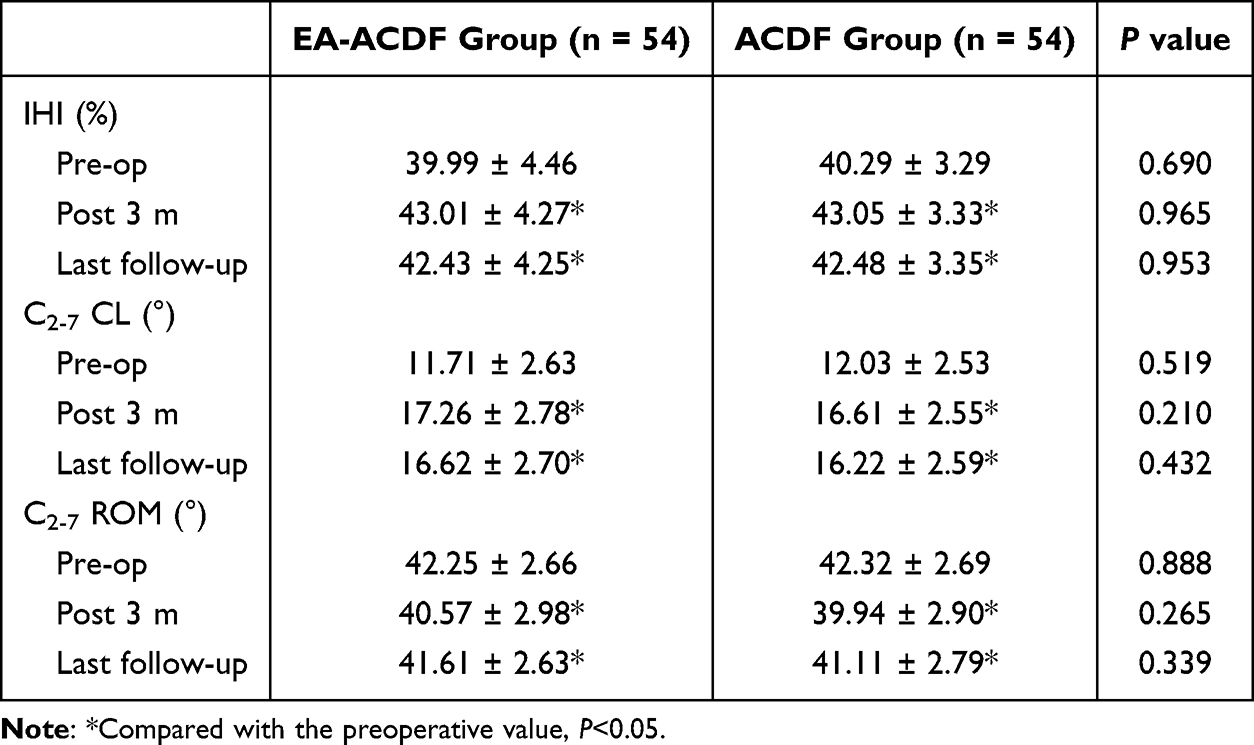 |
Table 5 Imaging Outcomes of the Two Groups |
Complications
The EA-ACDF group included one patient who developed cerebrospinal fluid leakage and one patient who experienced dysphagia (complication rate of 3.7%). In the ACDF group, two cases of cerebrospinal fluid leakage, two cases of neurological dysfunction, two cases of dysphagia, and two cases of hoarseness were seen (complication rate of 14.8%). The complication rates in both groups demonstrated significant differences (P = 0.046) (Table 6). During the follow-up period, neither group of patients experienced serious complications such as adjacent segment disease (ASD) with significant symptoms, fusion failure, implant displacement or fracture.
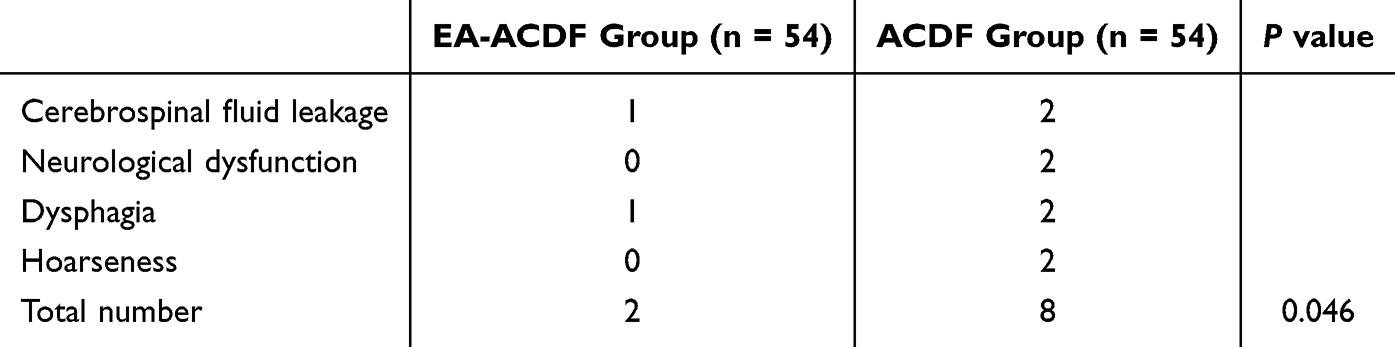 |
Table 6 Complications of the Two Groups |
Discussion
This study aimed to compare the clinical efficacy, imaging outcomes, and complication rates of EA-ACDF versus conventional ACDF in patients with single-segment CSM using a retrospective propensity score–matched design.
CSM is a chronic and progressive cervical degenerative disease whose incidence increases with aging.3,13 In clinical practice, patients with CSM frequently present with the symptoms of neurological dysfunction, mainly due to spinal cord compression and subsequent neurological ischemic changes.4,14 Several factors are involved in the pathogenesis of CSM, including cervical disc herniation, OPLL, hypertrophy of the ligamentum flavum, and osteophyte formation at the posterior margin of the vertebral body.1–3 Surgical intervention is the mainstay of clinical management of CSM, which decompresses the spinal cord and nerve roots, restores cervical stability and curvature, and corrects deformities.15,16
Since the 1960s, ACDF has gradually become the classic procedure for treating cervical degenerative diseases. ACDF has proven to be effective in treating CSM in several studies.17,18 Approaching from the anterior, the ACDF technique can accomplish adequate decompression of the cervical spinal canal without interfering with the dural sac.19 In addition, ACDF is effective in correcting cervical kyphosis and restoring cervical physiological curvature.9,20 Nevertheless, despite the reported strengths of ACDF, many limitations still exist in clinical practice. ACDF is prone to intraoperative and postoperative complications due to limitations, such as a limited surgical field, and difficulty in distinguishing anatomical structures, which seriously affect the clinical outcome of patients.7,8
With the innovation of minimally invasive surgical techniques, microscopy combined with ACDF has been increasingly adopted for treating cervical spondylosis. It enlarges the surgical field of view and provides a clearer vision and more accurate anatomical separation.21,22 However, compared to spinal endoscopy, microscopic techniques have some limitations, such as poor hand-eye coordination, difficulty in maintaining the focus of the surgical field for a long time, aggravation of neck and shoulder strain for the surgeon, and the increased risk of wound infection due to frequent operation of the microscope.9,23,24 In a retrospective study, Higgins et al25 found that the wound infection rate of lumbar decompression surgery with microscope was 4.3%, significantly exceeding the rate observed in the control group. In addition, several studies have shown that spinal endoscopy is an effective alternative to microscopy for the treatment of degenerative disc diseases. Therefore, some scholars attempted to use spinal endoscopy instead of microscopy for ACDF, thereby providing a superior surgical option for the treatment of cervical spondylosis. Recently, Wu et al7 and Tang et al9 reported that spinal endoscopy combined with ACDF for CSM achieved satisfactory clinical outcomes, suggesting the feasibility of this technique. Nevertheless, the authors did not explore the imaging characteristics of different procedures and/or balance confounding factors in the study design, undermining the reliability of their findings. Therefore, this study utilized the PSM method to control for covariates and compare imaging changes, thereby increasing the reliability of our findings.
The EA-ACDF technology integrates the features of conventional ACDF and spinal endoscopy and has new advantages in clinical application. The water medium makes a clearer surgical field of vision, and the application of endoscopic instrumentation allows for more precise decompression of the discs and hyperplastic osteophytes of the posterior edge of the vertebral body, which effectively decreases the risk of spinal cord and nerve root injury. Static water pressure can be maintained under endoscopy, which makes bipolar radiofrequency hemostasis more convenient. Besides, continuous saline irrigation may be able to effectively avoid the risk of postoperative infection at the surgical site.26 Notably, EA-ACDF is designed to maintain a clear surgical field by utilizing water flow rather than increasing water pressure. Switching between air and water media allows for the maintenance of unobstructed water flow and a stable static water pressure, which can effectively prevent complications, such as myeloid hypertension-like syndrome, cervical soft tissue edema, and mediastinal effusion.9
In the present study, all postoperative clinical functional scores of patients greatly improved compared to their preoperative levels. Thus, we believe that both surgical techniques for single-segment CSM can provide satisfactory clinical efficacy. However, the two surgical approaches for CSM still have different characteristics. Compared to conventional ACDF, clinical function scores improved more effectively in the EA-ACDF group at 7 days and 3 months postoperatively, suggesting that EA-ACDF was superior to ACDF in pain relief and neurologic recovery postoperatively, which may be related to the fact that the endoscopic operation of EA-ACDF led to less damage to the spinal cord and nerve roots. Regarding perioperative data, the EA-ACDF group had less intraoperative bleeding volume, less drainage volume, and shorter hospitalization length, suggesting minimal trauma and rapid recovery. In addition, compared to conventional ACDF, EA-ACDF appeared to reduce the incidence of intraoperative and postoperative complications, which may be related to the clear field of view in endoscopic operation and precise decompression. However, the relatively small sample size of this study limits the ability to fully assess the advantage of EA-ACDF in reducing complication rates. Notably, due to the short follow-up period of this study, the exploration of long-term complications is insufficient. For example, long-term complications such as ASD with obvious symptoms, fusion failure, implant displacement or fracture may require reoperation. Therefore, further long-term follow-up studies are needed in the future to comprehensively understand the advantages of EA-ACDF in terms of complications.
In this study, both EA-ACDF and ACDF achieved adequate decompression of the spinal cord in the treatment of CSM. Compared with conventional ACDF, the advantages of EA-ACDF mainly lie in clearer surgical visualization and more precise endoscopic decompression. The indications and contraindications of EA-ACDF are basically the same as those of conventional ACDF. Nevertheless, EA-ACDF as a new technique for treating cervical spondylosis has some limitations. For example, the EA-ACDF technique has a long learning curve, which necessitates extensive experience in open surgery and spinal endoscopic surgery. Furthermore, due to the mutual occlusion of the endoscope and instruments and the small size of the surgical instruments, the efficiency of endoscopic decompression is relatively low, leading to a longer operative time.
EA-ACDF is an effective surgical procedure for the treatment of CSM and deserves further attention. From conventional ACDF to microscope-assisted ACDF or EA-ACDF, the innovation of technology mainly lies in how to make the surgical field clearer, decompression more accurate, and hemostasis simpler, with fewer complications. Therefore, further improvement of optical and endoscopic surgical instruments is necessary to increase decompression efficiency and safety. In addition, in the future, the clinical efficacy of microscope-assisted ACDF should be compared with that of EA-ACDF.
This study had some limitations. Firstly, the features of this study were a retrospective analysis, which made it prone to subjective bias in case selection. Although we applied PSM to control for between-group confounders, bias could not be completely avoided. Furthermore, the sample size was small and all patients were from a single institution. Therefore, prospective, multicenter randomized controlled trials with larger sample sizes and longer follow-up periods are needed to validate our findings and to determine whether the advantages observed in this study can be sustained in the long term. In addition, further research is needed to evaluate the learning curve, cost-effectiveness, and applicability of EA-ACDF in multilevel CSM and other cervical pathologies.
Conclusion
Both EA-ACDF and conventional ACDF for single-segment CSM can provide satisfactory clinical efficacy. The EA-ACDF procedure provides a clearer surgical field, causes less trauma, allows faster recovery, and has the potential to reduce the risk of complications.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethics committee approval by the Committee of the Sixth Medical Center of the PLA General Hospital.
Acknowledgments
The authors acknowledge the Imaging Department and Operation Department of the Sixth Medical Center of PLA General Hospital, for their technical support and expertise in the radiological assessments. Meanwhile, the authors would like to express their gratitude to EditSprings (https://www.editsprings.cn) for the expert linguistic services provided.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is supported by National Natural Science Foundation of China (82274637).
Disclosure
The authors declared no conflicts of interest.
References
1. Xu N, Zhang Y, Zhou G, Zhao Q, Wang S. The value of dynamic MRI in the treatment of cervical spondylotic myelopathy: a protocol for a prospective randomized clinical trial. BMC Musculoskelet Disord. 2020;21(1):83. doi:10.1186/s12891-020-3106-y
2. Davies BM, Mowforth OD, Smith EK, Kotter MR. Degenerative cervical myelopathy. BMJ. 2018;360:k186. doi:10.1136/bmj.k186
3. McCormick JR, Sama AJ, Schiller NC, Butler AJ, Donnally CR. Cervical spondylotic myelopathy: a guide to diagnosis and management. J Am Board Fam Med. 2020;33(2):303–313. doi:10.3122/jabfm.2020.02.190195
4. Ghogawala Z, Terrin N, Dunbar MR, et al. Effect of ventral vs dorsal spinal surgery on patient-reported physical functioning in patients with cervical spondylotic myelopathy: a randomized clinical trial. JAMA. 2021;325(10):942–951. doi:10.1001/jama.2021.1233
5. Lee NJ, Kim JS, Park P, Riew KD. A comparison of various surgical treatments for degenerative cervical myelopathy: a propensity score matched analysis. Global Spine J. 2022;12(6):1109–1118. doi:10.1177/2192568220976092
6. Mesregah MK, Formanek B, Liu JC, Buser Z, Wang JC. Perioperative complications of surgery for degenerative cervical myelopathy: a comparison between 3 procedures. Global Spine J. 2023;13(2):432–442. doi:10.1177/2192568221998306
7. Wu ZP, Wei ZY, Song XL. Comparison of efficacy between endoscope-assisted anterior cervical discectomy and fusion (ACDF) and open ACDF in the treatment of single-segment cervical spondylotic myelopathy. J Orthop Surg Res. 2024;19(1):35. doi:10.1186/s13018-023-04514-w
8. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic anterior decompression versus conventional anterior decompression and fusion in cervical disc herniations. Int Orthop. 2009;33(6):1677–1682. doi:10.1007/s00264-008-0684-y
9. Tang Z, Jian L, Tang Q, et al. The efficacy and safety of mini-open (air/water medium) endoscopy-assisted anterior cervical discectomy and fusion for the treatment of cervical spondylotic myelopathy. Int Orthop. 2024;48(8):2243–2250. doi:10.1007/s00264-024-06212-6
10. Ke C, Tian N, Zhang X, Chen M. Changes in perioperative hemoglobin and hematocrit in patients undergoing total knee arthroplasty: a prospective observational study of optimal timing of measurement. J Int Med Res. 2020;48(11):300060520969303. doi:10.1177/0300060520969303
11. Zhang J, Ruan D, Xuan A, et al. Comparative study of outcomes between allograft intervertebral disc transplantation and anterior cervical discectomy and fusion: a retrospective cohort study at least 5 years of follow-up. Eur Spine J. 2023;32(10):3561–3574. doi:10.1007/s00586-023-07799-x
12. Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ, Holland B. Cobb method or Harrison posterior tangent method: which to choose for lateral cervical radiographic analysis. Spine. 2000;25(16):2072–2078. doi:10.1097/00007632-200008150-00011
13. Bourgonjon B, Duerinck J, Moens M, D’Haens J. Comparison of the effect of anterior and posterior neurosurgical treatment for cervical spondylotic myelopathy: a clinical outcome. Acta Neurol Belg. 2019;119(4):585–593. doi:10.1007/s13760-019-01184-6
14. Abdelmalek G, Uppal H, Coban D, et al. Is cervical disc arthroplasty an effective treatment option for patients with cervical spondylotic myelopathy? A matched cohort analysis compared to anterior cervical discectomy and fusion. Spine J. 2024. doi:10.1016/j.spinee.2024.11.003
15. Quinn JC, Kiely PD, Lebl DR, Hughes AP. Anterior surgical treatment of cervical spondylotic myelopathy: review article. HSS J. 2015;11(1):15–25. doi:10.1007/s11420-014-9408-6
16. Liu K, Shi J, Jia L, Yuan W. Surgical technique: hemilaminectomy and unilateral lateral mass fixation for cervical ossification of the posterior longitudinal ligament. Clin Orthop Relat Res. 2013;471(7):2219–2224. doi:10.1007/s11999-013-2889-7
17. Guo S, Lu S, Kong C, Li X, Liu C. Comparison of clinical outcomes and sagittal alignment after different levels of anterior cervical discectomy and fusion in patients with cervical spondylotic myelopathy: from one-level to three-level. Spine. 2021;46(3):E153–E160. doi:10.1097/BRS.0000000000003746
18. White MD, Farber SH, Pacult MA, et al. Pseudarthrosis after four-level anterior cervical discectomy and fusion without posterior fixation. Neurosurg Focus. 2023;55(3):E4. doi:10.3171/2023.6.FOCUS23303
19. Choi SH, Kang CN. Degenerative cervical myelopathy: pathophysiology and current treatment strategies. Asian Spine J. 2020;14(5):710–720. doi:10.31616/asj.2020.0490
20. Chen SR, LeVasseur CM, Pitcairn S, et al. Surgery-related factors do not affect short-term adjacent segment kinematics after anterior cervical arthrodesis. Spine. 2021;46(23):1630–1636. doi:10.1097/BRS.0000000000004080
21. Cai RZ, Wang YQ, Wang R, Wang CH, Chen CM. Microscope-assisted anterior cervical discectomy and fusion combined with posterior minimally invasive surgery through tubular retractors for multisegmental cervical spondylotic myelopathy: a retrospective study. Medicine. 2017;96(35):e7965. doi:10.1097/MD.0000000000007965
22. Omidi-Kashani F, Ghayem HE, Ghandehari R. Impact of age and duration of symptoms on surgical outcome of single-level microscopic anterior cervical discectomy and fusion in the patients with cervical spondylotic radiculopathy. Neurosci J. 2014;2014:808596. doi:10.1155/2014/808596
23. Siller S, Zoellner C, Fuetsch M, Trabold R, Tonn JC, Zausinger S. A high-definition 3D exoscope as an alternative to the operating microscope in spinal microsurgery. J Neurosurg Spine. 2020;33(5):705–714. doi:10.3171/2020.4.SPINE20374
24. Bible JE, O’Neill KR, Crosby CG, Schoenecker JG, McGirt MJ, Devin CJ. Microscope sterility during spine surgery. Spine. 2012;37(7):623–627. doi:10.1097/BRS.0b013e3182286129
25. Higgins G, Philips J, Iqbal S, Kwong H, Grainger M. Lumbar spine decompressive surgery: should use of the microscope be compulsory? In:
26. Torres KA, Konrade E, White J, et al. Irrigation techniques used in spine surgery for surgical site infection prophylaxis: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2022;23(1):813. doi:10.1186/s12891-022-05763-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of an Enhanced Recovery After Surgery (ERAS) Program in Hip Arthroplasty in a Developing Country: A Propensity Score-Matched Study from Vietnam

Vu PTN, Khanh BHT, Hung HQ, Dao NTN, Sang LN, Chien NV, Bang HT
Journal of Multidisciplinary Healthcare 2025, 18:2731-2747
Published Date: 16 May 2025