Back to Journals » Journal of Asthma and Allergy » Volume 16
Clinical Efficacy among Patients with Chronic Rhinosinusitis with Nasal Polyps and Clinical Features of Obstructive Lung Disease: Post Hoc Analysis of the Phase III SINUS-24 and SINUS-52 Studies
Authors Maspero JF, Bachert C, Martinez FJ ![]() , Hanania NA, Ortiz B, Patel N, Mannent LP, Praestgaard A, Pandit-Abid N, Siddiqui S
, Hanania NA, Ortiz B, Patel N, Mannent LP, Praestgaard A, Pandit-Abid N, Siddiqui S ![]() , Hardin M
, Hardin M
Received 7 January 2022
Accepted for publication 17 May 2022
Published 31 March 2023 Volume 2023:16 Pages 333—342
DOI https://doi.org/10.2147/JAA.S357393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Jorge F Maspero,1 Claus Bachert,2,3 Fernando J Martinez,4 Nicola A Hanania,5 Benjamin Ortiz,6 Naimish Patel,7 Leda P Mannent,8 Amy Praestgaard,7 Nami Pandit-Abid,9 Shahid Siddiqui,6 Megan Hardin7
1Allergy and Respiratory Research Unit, Fundación CIDEA, Buenos Aires, Argentina; 2Upper Airway Research Laboratory, Department of Otorhinolaryngology, Ghent University Hospital, Ghent, Belgium; 3Division of ENT Diseases, CLINTEC, Karolinska Institutet, Stockholm, Sweden; 4Division of Pulmonary and Critical Care, Weill Cornell Medical College, New York, NY, USA; 5Section of Pulmonary and Critical Care Medicine, Baylor College of Medicine, Houston, TX, USA; 6Immunology and Allergy Medical Affairs, Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA; 7Immunology and Inflammation, Sanofi, Cambridge, MA, USA; 8Global Clinical Development, Sanofi, Chilly-Mazarin, France; 9Immunology and Inflammation, Sanofi, Bridgewater, NJ, USA
Correspondence: Jorge F Maspero, Allergy and Respiratory Research Unit, Fundación CIDEA, Paraguay 2035, Buenos Aires, C1121ABE, Argentina, Tel +54 91141837294, Email [email protected]
Purpose: To provide a descriptive summary of clinical efficacy and health-related quality of life (HRQoL) measures in patients with chronic rhinosinusitis with nasal polyps (CRSwNP) and clinical features of obstructive lung disease in the Phase III dupilumab studies SINUS-24 and SINUS-52 (NCT02912468, NCT02898454).
Patients and Methods: Patients met a “broad” definition of having clinical features of obstructive lung disease with any of 3 criteria: (i) pre-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) < 0.70 and smoking history; (ii) patient-reported medical history of chronic obstructive pulmonary disease (COPD); or (iii) asthma with > 10 pack-years’ smoking history. A “narrow” definition including criteria (i) or (ii) was also analyzed. CRSwNP and HRQoL measures were evaluated in all patients and lung function (FEV1; FEV1/FVC ratio) was captured and analyzed only in those patients who had a self-reported history of asthma.
Results: Across both studies, 131 patients met the “broad” definition, of whom 90 also had asthma, and 115 patients met the “narrow” definition, of whom 74 had asthma. CRSwNP outcomes and HRQoL were improved with dupilumab vs placebo in both the broad and narrow subgroups. Among the 90 patients who met the broad definition and had asthma, dupilumab improved pre-bronchodilator FEV1 and FEV1/FVC ratio at Week 16 (least squares mean differences vs placebo: 0.38 L [95% confidence interval: 0.17, 0.59; p = 0.0004] and 4.8% [1.7%, 7.9%; p = 0.0024], respectively) sustained through Week 24. Similar results were seen in the “narrow” subgroup with asthma.
Conclusion: In a population of patients with CRSwNP and clinical features of obstructive lung disease, dupilumab improved CRSwNP and HRQoL outcomes, and, among those with a history of asthma, also improved lung function. These results support further analyses of dupilumab in patients with evidence of type 2 inflammation and obstructive lung disease such as COPD.
Keywords: obstructive lung disease, chronic obstructive pulmonary disease, dupilumab, type 2 inflammation, interleukin-4, interleukin-13
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is an inflammatory disease of the nasal cavity and paranasal sinuses characterized by chronic symptoms such as nasal congestion, rhinorrhea, loss of smell, facial pain and headache, and the presence of nasal polyps (NP) and sinus inflammation.1 Inflammation in CRSwNP is commonly type 2 and involves interleukin (IL)-4 and IL-13, which are key and central drivers of type 2 inflammation in multiple diseases.1–3 Dupilumab is a fully human VelocImmune®-derived monoclonal antibody that binds specifically to IL-4Rα, the shared receptor component for IL-4 and IL-13, thereby inhibiting the proinflammatory actions of these cytokines.4,5 Dupilumab demonstrated an acceptable tolerability profile in Phase 1 studies in healthy volunteers and demonstrated efficacy and acceptable tolerability in Phase 2 and Phase 3 studies in a range of conditions, including asthma, atopic dermatitis, and CRSwNP.6–14 Dupilumab improved lung function and asthma control in adults and adolescents with moderate-to-severe asthma and evidence of type 2 inflammation.11 Dupilumab is approved for selected patients with diseases driven by type 2 inflammation, specifically asthma, CRSwNP, and atopic dermatitis (AD).
In the international, randomized, Phase 3 SINUS-24 (NCT02912468) and SINUS-52 (NCT02898454) studies, dupilumab significantly improved endoscopic, radiologic, clinical, and health-related quality of life (HRQoL) measures vs placebo in adults with severe CRSwNP.13 The broad efficacy demonstrated by dupilumab in these studies suggests that in the populations evaluated, type 2 inflammation and particularly IL-4 and IL-13 are key drivers of CRSwNP. A subset of patients in these studies who had comorbid asthma also demonstrated improvement in CRSwNP efficacy endpoints as well as in lung function as measured by pre-bronchodilator forced expiratory volume in 1 second (FEV1) and FEV1/forced vital capacity (FVC) ratio FEV1/FVC.15
Beyond the broad efficacy observed across multiple type 2 inflammatory diseases, including asthma, CRSwNP, and AD, dupilumab’s efficacy in patients with chronic obstructive pulmonary disease (COPD) and evidence of type 2 inflammation is unknown. To address this question, in this analysis we evaluated a subset of patients in the SINUS studies with severe CRSwNP who also had evidence of obstructive lung disease to assess the potential benefit of dupilumab in COPD. COPD is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases.16 While COPD is a clinical diagnosis that includes integration of subjective measures such as symptoms and risk with objective spirometry with post-bronchodilator FEV1/FVC less than 0.70,16 in research studies, patients with COPD can be identified based on physician diagnosis as well as post-bronchodilator lung function. A subset of patients in the SINUS-24 and SINUS-52 studies had reported either medical history of COPD, or had smoking history and baseline lung function that was suggestive of obstructive lung disease (pre-bronchodilator FEV1/FVC <0.70). While these patients may not necessarily meet a clinical diagnosis of COPD, we postulated that analysis of these patients may nevertheless provide useful insights into the potential impact of dupilumab treatment on patients with persistent airflow obstruction and obstructive lung disease. The aim of this post hoc analysis was to evaluate clinical outcomes and HRQoL in a subset of patients from SINUS-24 and SINUS-52 who had these clinical features of obstructive lung disease, in order to better understand the potential role of targeting type 2 inflammation in patients with COPD.
Materials and Methods
Patients and Study Design
In the SINUS-24 and SINUS-52 studies, eligible patients were ≥18 years of age, had severe CRSwNP, and had either received systemic corticosteroids in the preceding 2 years or had undergone sinonasal surgery. Details of the study designs have been reported previously.13 Briefly, eligible patients had bilateral NP despite intranasal corticosteroids (INCS) treatment, with nasal polyp score (NPS) ≥5 out of 8 (≥2 for each nostril), and ongoing symptoms for at least 8 weeks prior to study entry including nasal congestion and at least one of loss of smell, or anterior or posterior rhinorrhea. Patients with concomitant asthma had to be stable in the 6 weeks prior to study entry using their regular asthma treatment. Patients with FEV1 ≤50% of predicted normal or who had participated in prior dupilumab clinical trials were excluded.
Patients were randomized 1:1 to double-blind treatment with subcutaneous (SC) dupilumab 300 mg or placebo every 2 weeks (q2w) for 24 weeks in SINUS-24, and 1:1:1 to SC dupilumab 300 mg q2w for 52 weeks, SC dupilumab 300 mg q2w for 24 weeks followed by every 4 weeks to 52 weeks, or placebo throughout 52 weeks in SINUS-52.13 Randomization was stratified by the presence of asthma and/or non-steroidal anti-inflammatory drug-exacerbated respiratory disease (NSAID-ERD), prior surgery, and country. All patients received INCS (100 mg of mometasone furoate nasal spray in each nostril twice daily) from 4 weeks prior to randomization to the end of the study. Both studies achieved their primary objective of reduction in the coprimary endpoints of nasal congestion/obstruction score and bilateral NPS at Week 24.
The patient populations evaluated for this post-hoc analysis included patients with features of obstructive lung disease identified using 3 criteria (broad definition): (i) pre-bronchodilator FEV1/FVC <0.70 and smoking history or (ii) patient-reported history of COPD or (iii) asthma and >10 pack-years of smoking history. In addition, a more narrow definition was applied using only criteria (i) and (ii). It should be noted that these are patients with features of COPD, but do not necessarily meet the clinical definition or carry a diagnosis of COPD. A subset of these patients also had a history of asthma, which was identified by self-report. Spirometry was performed at baseline in all patients enrolled in the study, and then during the conduct of the trial only for those with a history of asthma.
Results for placebo and dupilumab 300 mg q2w (the approved dose) from the subgroups of patients with clinical features of obstructive lung disease are presented alongside results in patients with asthma to illustrate the effects of dupilumab on lung function and other outcomes in the wider SINUS-24/52 population. Given the small sample size in the subgroup analyses, data from Week 24 in the SINUS-24 and SINUS-52 studies were pooled to maximize precision, and therefore these subanalyses are limited to the Week 24 timepoint.
Outcome Measures
NPS and the 22-item Sino Nasal Outcome Test (SNOT-22) measure of HRQoL in CRSwNP were assessed at baseline and at 8, 16, and 24 weeks in all patients. University of Pennsylvania Smell Identification Test (UPSIT) was assessed at baseline and at 2, 16, and 24 weeks in all patients. Pre-bronchodilator FEV1 and FEV1/FVC ratio were assessed at baseline in all patients, and at 16 and 24 weeks in patients with a diagnosis of asthma.
Statistical Analyses
Differences in least squares (LS) mean change from baseline between dupilumab and placebo were calculated by fitting an analysis of covariance model with change from baseline at the corresponding visit as the response variable, and the corresponding baseline value, treatment group, asthma/NSAID-ERD status (except for analysis of lung function outcomes), prior surgery history, region (Asia, Latin America, East Europe, or Western countries), and study as covariates. Age, sex, and smoking history were additionally used as covariates in the model for analysis of patients in the narrow subgroup to account for baseline differences. Analysis of change from baseline in FEV1 at Week 24 for patients with asthma was pre-specified. All other analyses described here are post hoc and reported p-values are nominal. Data collected after treatment discontinuation were included. Data after “rescue” with systemic corticosteroids or NP surgery were set to missing and imputed by worst observation carried forward (WOCF); other missing data were imputed by multiple imputation (MI) as described.13 Descriptive statistics include WOCF but not values imputed by MI.
Results
Of 724 patients with severe uncontrolled CRSwNP randomized in the SINUS-24 and SINUS-52 studies, 131 (18%) met the broad definition criteria for features of obstructive lung disease (74 and 57 in the dupilumab 300 mg q2w and placebo groups, respectively) and 115 (16%) met the narrow definition criteria (67 and 48, respectively). A breakdown of the proportion of patients meeting each of the criteria is shown in Table 1 and a flowchart of patient disposition is shown in Supplementary Figure 1. Overall, 105/131 (80%) patients in the broad definition subgroup had baseline pre-bronchodilator FEV1/FVC <0.70 and smoking history, and 18/131 (14%) reported a history of COPD. The corresponding proportions in the narrow definition group were 105/115 (91%) and 18/115 (16%). Demographics and baseline disease characteristics were generally well balanced between the placebo and dupilumab arms in both subgroups, although the placebo patients had numerically greater proportions of women, never smokers, and patients with history of COPD (Tables 1 and 2).
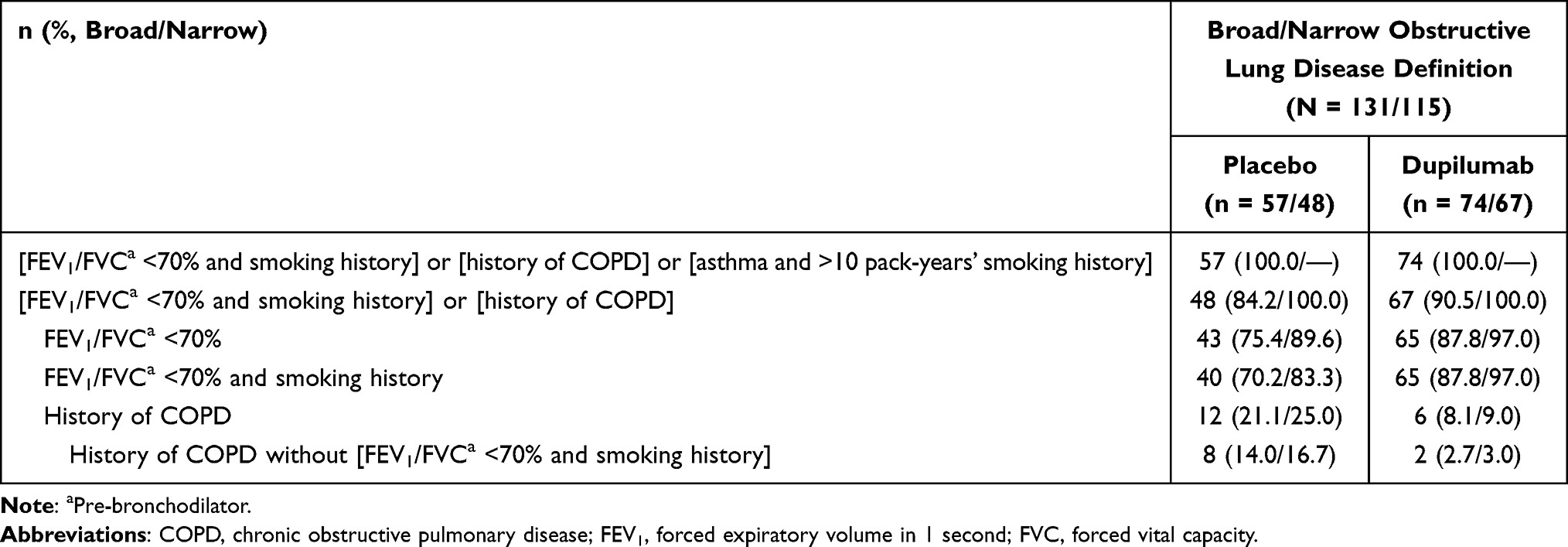 |
Table 1 Breakdown of the Criteria for Clinical Features of Obstructive Lung Disease |
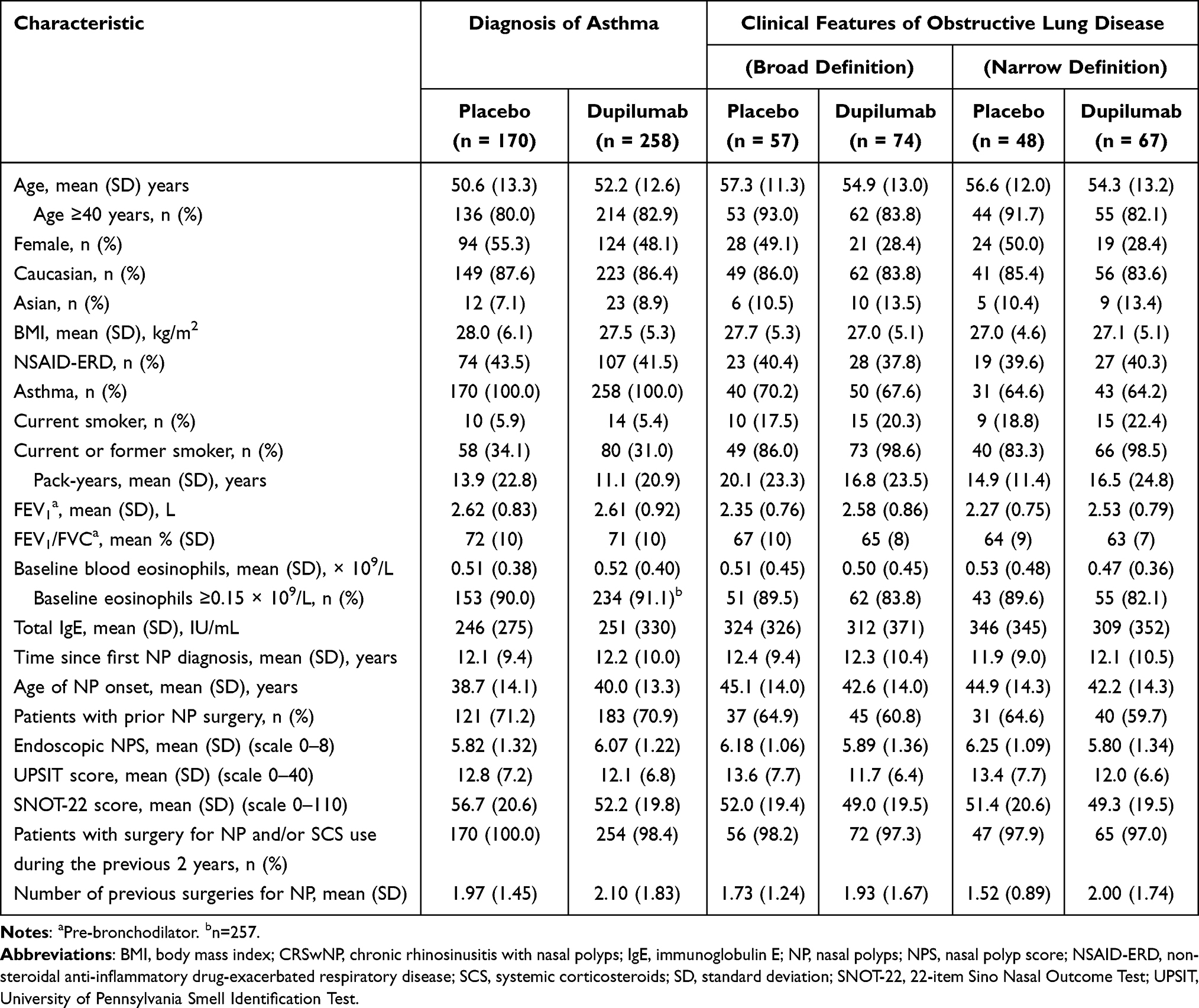 |
Table 2 Demographic and Baseline Characteristics of Subgroups of Patients with CRSwNP from SINUS-24 and SINUS-52 with a Diagnosis of Asthma or with Clinical Features of Obstructive Lung Disease |
Among the patients with features of obstructive lung disease, dupilumab treatment improved measures of CRSwNP disease. In the broad definition subgroup, LS mean (95% confidence interval [CI]) differences for dupilumab vs placebo at Week 24 for NPS were −1.72 (−2.27, −1.16) (Figure 1) and for UPSIT were 9.25 (6.52, 11.99) (Figure 2); both p < 0.0001. Mean SNOT-22 total scores also improved with dupilumab in patients with features of obstructive lung disease: in the broad definition subgroup, at the first assessment (Week 8), the LS mean (95% CI) difference between dupilumab and placebo was −13.14 (−19.77, −6.52), and by Week 24 the difference had increased to −15.45 (−21.88, −9.02); both p < 0.0001 (Figure 3). Similar effects of dupilumab on NPS, UPSIT, and SNOT-22 were seen in the narrow subgroup and in the overall asthma group (Figures 1–3).
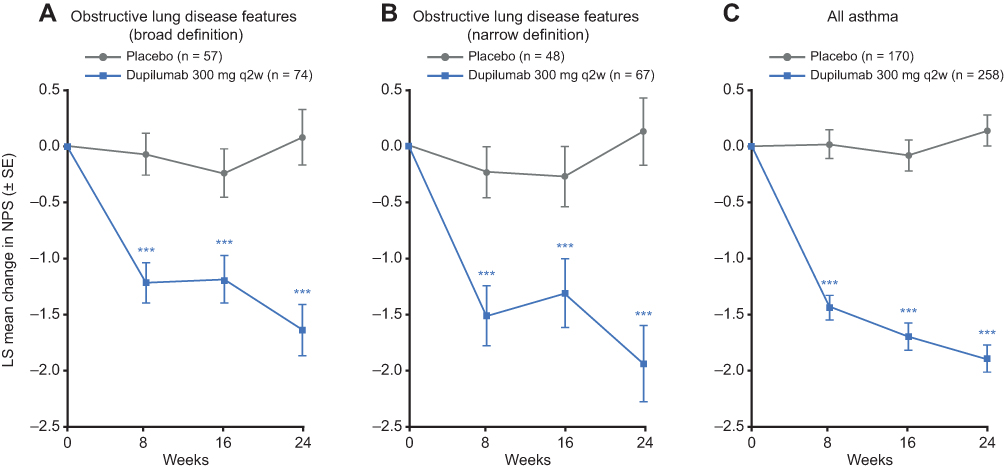 |
Figure 1 Effect of dupilumab on NPS in patients with CRSwNP and clinical features of obstructive lung disease. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; LS, least squares; NPS, nasal polyp score; q2w, every 2 weeks; SE, standard error. Notes: Data are LS mean change (± SE) from baseline in NPS (range 0–8) in patients with CRSwNP and clinical features of obstructive lung disease (broad definition, A; narrow definition, B), or diagnosis of asthma (C). Nominal p vs placebo ***<0.001. |
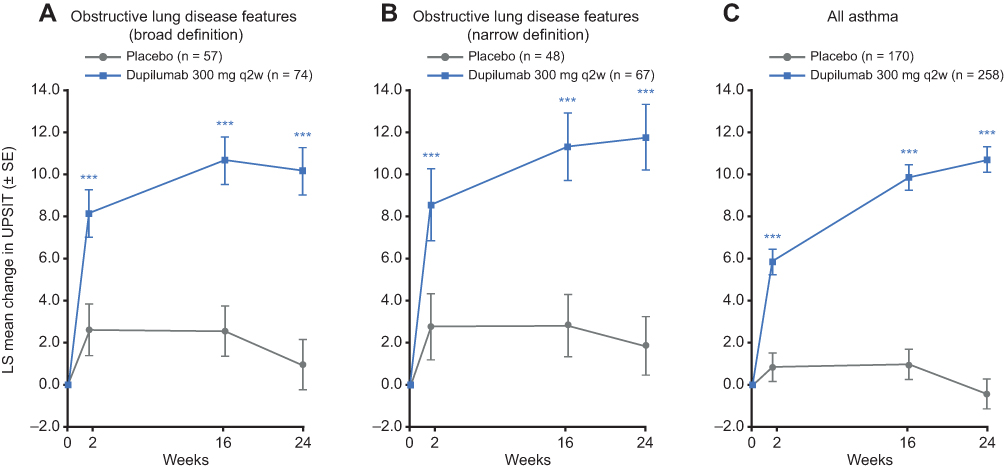 |
Figure 2 Effect of dupilumab on UPSIT score in patients with CRSwNP and clinical features of obstructive lung disease. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; LS, least squares; q2w, every 2 weeks; SE, standard error; UPSIT, University of Pennsylvania Smell Identification Test. Notes: Data are LS mean change (± SE) from baseline in UPSIT (range 0–40) in patients with CRSwNP and clinical features of obstructive lung disease (broad definition, A; narrow definition, B), or diagnosis of asthma (C). Nominal p vs placebo ***<0.001. |
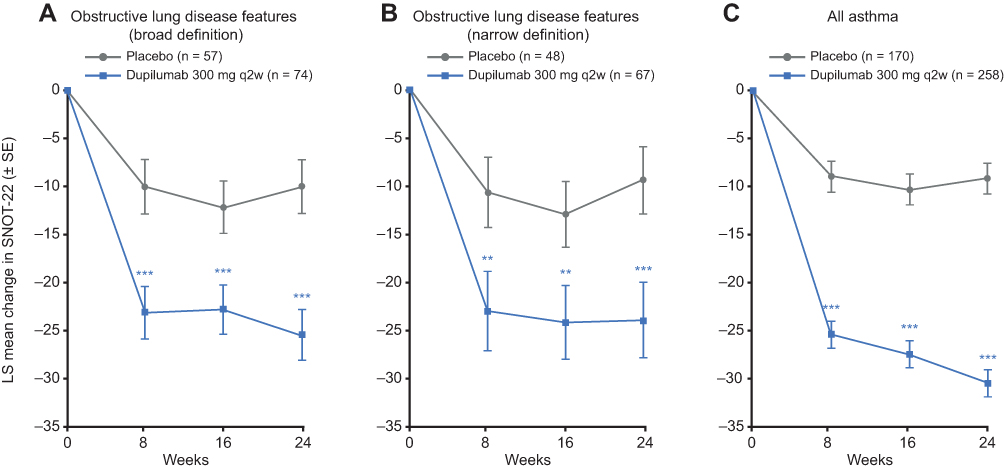 |
Figure 3 Effect of dupilumab on SNOT-22 total score in patients with CRSwNP and clinical features of obstructive lung disease. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; LS, least squares; q2w, every 2 weeks; SE, standard error; SNOT-22, 22-item Sino Nasal Outcome Test. Notes: Data are LS mean change (± SE) from baseline in SNOT-22 (range 0–110) in patients with CRSwNP and clinical features of obstructive lung disease (broad definition, A; narrow definition, B), or diagnosis of asthma (C). Nominal p vs placebo **<0.01, ***<0.001. |
Among the patients with clinical features of obstructive lung disease, 90/131 (69%) in the broad definition group and 74/115 (64%) in the narrow definition group had a diagnosis of asthma and therefore had post-baseline FEV1 assessments at Weeks 16 and 24. In the broad definition subgroup, mean (standard deviation [SD]) baseline pre-bronchodilator FEV1 was 2.45 L (0.76) and 2.43 L (0.92) in the placebo and dupilumab groups, respectively; and FEV1/FVC ratio was 0.68 (0.10) and 0.65 (0.09), respectively (Supplementary Table 1). The corresponding values for the narrow definition subgroup were 2.36 (0.76) and 2.33 (0.79) for FEV1, and 0.64 (0.09) and 0.62 (0.07) for FEV1/FVC ratio. These baseline values were lower (indicating more severe airflow obstruction) than the corresponding values in the overall group with asthma (n = 428) (Supplementary Table 1). In the broad definition subgroup, there was an increase in pre-bronchodilator FEV1 in the dupilumab group compared with placebo at Week 16 (LS mean difference vs placebo: 0.38 L [95% CI: 0.17, 0.59]; p = 0.0004), which was sustained through Week 24 (Figure 4; Supplementary Table 1). Dupilumab treatment also improved FEV1/FVC ratio vs placebo at Week 16 (LS mean difference vs placebo: 0.05 [0.02, 0.08]; p = 0.0024), with improvements sustained through Week 24 (Figure 4; Supplementary Table 1). Similar effects of dupilumab treatment on FEV1 and FEV1/FVC ratio were seen in the narrow definition subgroup (Figure 4; Supplementary Table 1).
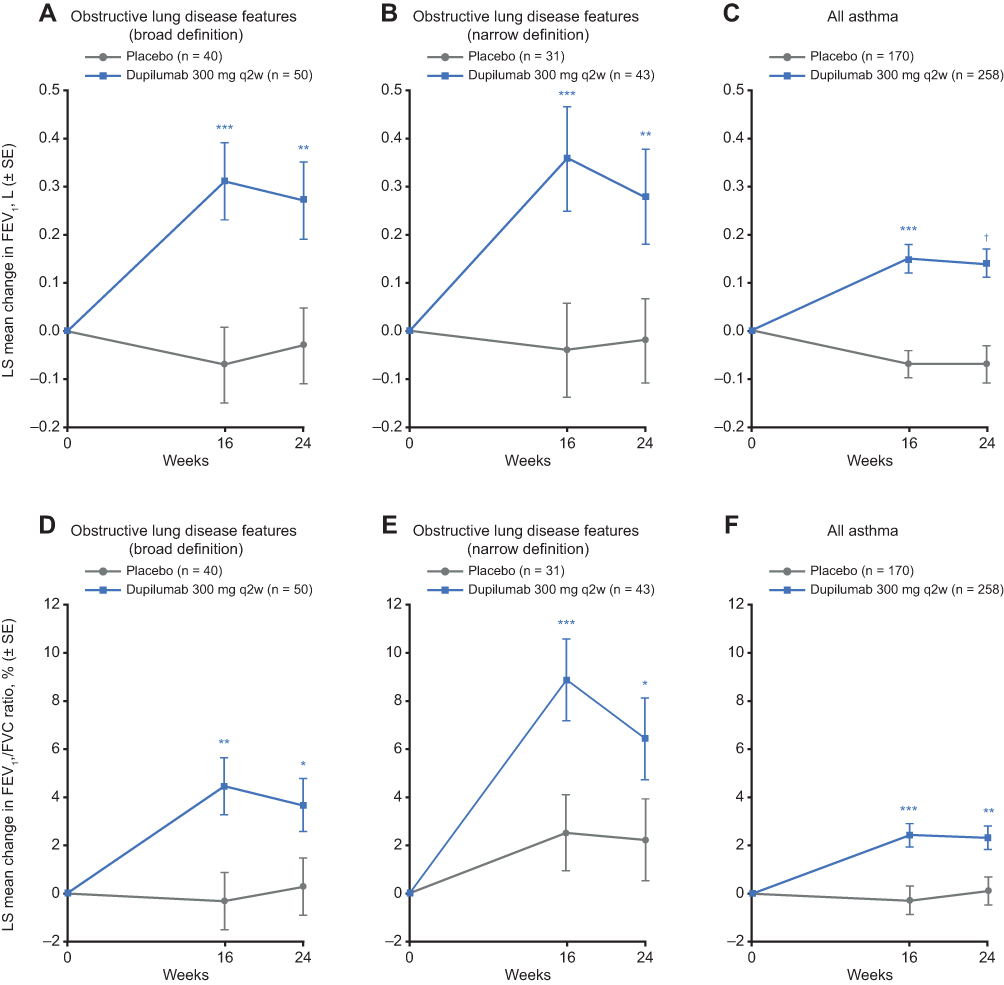 |
Figure 4 Effect of dupilumab on lung function in patients with CRSwNP and clinical features of obstructive lung disease. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; LS, least squares; q2w, every 2 weeks; SE, standard error. Notes: Data are LS mean change (± SE) from baseline in pre-bronchodilator FEV1 (A–C) and pre-bronchodilator FEV1/FVC ratio (D–F) in patients with CRSwNP with diagnosis of asthma and clinical features of obstructive lung disease (broad definition, A and D; narrow definition, B and E), or diagnosis of asthma (C and F). †Pre-specified p vs placebo <0.001. Nominal p vs placebo *<0.05, **<0.01, ***<0.001. |
Discussion
It is common for patients with severe CRSwNP to have coexisting type 2 inflammatory airway disease.17 The term “united airway disease” has been used to describe the manifestation of inflammatory disorder in both the upper and lower airways.18 Treatment for CRSwNP aims to control symptoms, minimize polyp recurrence, and achieve better HRQoL and control of these comorbid conditions. Lung function improvement in patients with CRSwNP and comorbid asthma using dupilumab has been previously shown.13 We assessed the effects of dupilumab in patients with CRSwNP with clinical features of obstructive lung disease because some patients with obstructive lung disease display type 2 inflammatory signatures that are similar to those seen in CRSwNP, asthma, atopic dermatitis, and allergic rhinitis. Lung function was assessed in those patients with CRSwNP and self-reported asthma.
In this analysis, based on pooled data from the randomized Phase III SINUS-24 and SINUS-52 studies, dupilumab treatment was associated with improvements in CRSwNP outcomes in patients with CRSwNP and clinical features of obstructive lung disease, and with improvements in lung function among those patients with CRSwNP, clinical features of obstructive lung disease, and self-reported asthma. Among the patients with features of obstructive lung disease who had a diagnosis of asthma, and therefore had post-baseline spirometry assessments, dupilumab improved lung function outcomes (pre-bronchodilator FEV1 and FEV1/FVC) vs placebo at Week 16, with improvements maintained through Week 24. Similar to the findings in the main SINUS studies, among the patients with features of obstructive lung disease, dupilumab led to improvements in NPS, symptoms, and CRSwNP-related HRQoL. These are hypothesis-generating findings, which support the investigation of dupilumab for efficacy in patients with COPD and evidence of type 2 inflammation.
This post hoc analysis has some limitations. First, the subgroups defined as having clinical features of obstructive lung disease were heterogeneous. This was a post-hoc analysis and we selected a series of criteria to identify a surrogate population to understand the potential response in a population with COPD. This included retrospective identification on the basis of pre-bronchodilator lung function parameters and/or physician diagnosis. The availability of only pre-bronchodilator rather than post-bronchodilator lung function measurements is a major limitation because in many of these patients with pre-existing CRSwNP, smoking history, and abnormal lung function, it may be hard to distinguish late-onset asthma from COPD. The aim was to use this pragmatic subgroup of patients to explore the potential for dupilumab effects in patients with COPD and type 2 inflammation, a group in which there currently are no data on dupilumab clinical efficacy. Therefore, the results of this analysis remain hypothesis-generating. A second limitation was the lack of post-bronchodilator FEV1 data, which were not collected as part of the parent study. Finally, the SINUS studies excluded patients with FEV1 ≤50% of predicted normal, thus excluding patients who may have had more severe lung function impairment. Randomized controlled studies are underway to evaluate the efficacy, safety, and tolerability of dupilumab in patients with moderate-to-severe COPD with type 2 inflammation (NCT03930732, NCT04456673).
Conclusion
While COPD is a clinical diagnosis that is typically identified in clinical trials using physician report as well as post-bronchodilator lung function, these data were unavailable for most patients in the SINUS studies. Consequently, for this post-hoc analysis, an approach was taken to identify patients with features consistent with obstructive lung disease as a surrogate to better understand the potential role for dupilumab in patients with COPD, and results are exploratory and do not necessarily apply to patients with clinically determined COPD. In this subgroup of patients with CRSwNP and clinical features of obstructive lung disease, dupilumab improved CRSwNP, HRQoL outcomes, and, in patients who also had a history of asthma, lung function. This analysis is consistent with the mechanism of dupilumab as a monoclonal antibody that suppresses type 2 inflammation and provides supportive evidence to proceed with efficacy studies in a population with COPD and evidence of type 2 inflammation.
Abbreviations
CI, confidence interval; COPD, chronic obstructive pulmonary disease; CRSwNP, chronic rhinosinusitis with nasal polyps; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; HRQoL, health-related quality of life; IL, interleukin; INCS, intranasal corticosteroids; LS, least squares; NP, nasal polyps; NPS, nasal polyp score; NSAID-ERD, non-steroidal anti-inflammatory drug-exacerbated respiratory disease; q2w, every 2 weeks; SC, subcutaneous; SD, standard deviation; SNOT-22, 22-item Sino Nasal Outcome Test; UPSIT, University of Pennsylvania Smell Identification Test.
Prior Presentation
Some of the data were previously presented at the 2020 American Thoracic Society (ATS) Virtual Symposium (abstract and poster #223).
Data Sharing Statement
Qualified researchers may request access to patient-level data and related study documents including clinical study report, study protocol with any amendments, blank case report form, statistical analysis plan, and dataset specifications. Patient-level data will be anonymized and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi’s data sharing criteria, eligible studies, and process for requesting access can be found at: https://www.vivli.org/
Ethics Approval and Informed Consent
The studies were conducted in accordance with the Declaration of Helsinki and the study protocols were approved by Copernicus Group IRB (Protocol # EFC14146, Tracking # SAN4-16-406; Protocol # EFC14280, Tracking # SAN4-16-417). All patients gave written informed consent.
Acknowledgments
Research sponsored by Sanofi and Regeneron Pharmaceuticals, Inc. ClinicalTrials.gov Identifier: NCT02912468 (SINUS-24) and NCT02898454 (SINUS-52). The authors thank Marcella Ruddy, formerly of Regeneron Pharmaceuticals, Inc., for insight and guidance, Nadia Daizadeh, formerly of Sanofi, for statistical analyses, and Matt Lewis, of Adelphi Communications, for medical writing/editorial assistance funded by Sanofi Genzyme and Regeneron Pharmaceuticals, Inc., in accordance with Good Publication Practice (GPP3).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was sponsored by Sanofi and Regeneron Pharmaceuticals, Inc.
Disclosure
Jorge F. Maspero has been a consultant for AstraZeneca, Sanofi, and Teva; reports speaker fees from Boehringer Ingelheim, GlaxoSmithKline, Menarini, Novartis, and Uriach; and reports research grants from Novartis. Claus Bachert has been an advisory board member for ALK, ASIT Biotech, AstraZeneca, Intrexon Actobiotics, Novartis, Sanofi, and Stallergenes Greer. Fernando J. Martinez has been on steering committees for Afferent/Merck, AstraZeneca, Bayer, Boehringer Ingelheim, Gilead, GlaxoSmithKline, Nitto, Patara/Respivant, Pearl Pharmaceuticals, ProMedior/Roche, ProMetic, Stromedix/Biogen, and Veracyte; has been an advisory board member for AstraZeneca, Bioscale/Proterrix Bio, Boehringer Ingelheim, Chiesi, CSL Behring, Gala, Genentech, GlaxoSmithKline, Novartis, Pearl Pharmaceuticals, Physicians Education Resource, Sunovion, Teva, and Zambon; has been a consultant for Bridge Biotherapeutics, Bristol Myers Squibb, and twoXR; reports continuing medical education presentation support from the Canadian Respiratory Network, Chiesi, CME Outfitters, Dartmouth University, France Foundation, Inova Fairfax, MD Magazine, Methodist Hospital, Miller Communications, National Association for Continuing Education/Haymarket, New York University, PeerView, Prime Education, Rare Diseases Healthcare Communication, Rockpointe, University of Alabama Birmingham, UpToDate, Vindico, WebMD/MedScape, and Zambon; and has been on the data and safety monitoring board for Boehringer Ingelheim and GlaxoSmithKline. Nicola A. Hanania reports research support from AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline; and has been a consultant for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Regeneron Pharmaceuticals, Inc., and Sanofi. Benjamin Ortiz and Shahid Siddiqui are employees of and shareholders in Regeneron Pharmaceuticals, Inc. Naimish Patel, Leda P. Mannent, Amy Praestgaard, Megan Hardin, and Nami Pandit-Abid are employees of and may hold stock and/or stock options in Sanofi. Dr. Benjamin Ortiz is a former employee of Regeneron Pharmaceuticals, Inc. The authors report no other conflicts of interest in this work.
References
1. Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. doi:10.4193/Rhin20.401
2. Gandhi NA, Pirozzi G, Graham NMH. Commonality of the IL-4/IL-13 pathway in atopic diseases. Expert Rev Clin Immunol. 2017;13(5):425–437. doi:10.1080/1744666X.2017.1298443
3. Hulse KE, Stevens WW, Tan BK, Schleimer RP. Pathogenesis of nasal polyposis. Clin Exp Allergy. 2015;45(2):328–346. doi:10.1111/cea.12472
4. Murphy AJ, Macdonald LE, Stevens S, et al. Mice with megabase humanization of their immunoglobulin genes generate antibodies as efficiently as normal mice. Proc Natl Acad Sci USA. 2014;111(14):5153. doi:10.1073/pnas.1324022111
5. Le Floc’h A, Allinne J, Nagashima K, et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy. 2020;75(5):1188–1204. doi:10.1111/all.14151
6. Li Z, Radin A, Li M, et al. Pharmacokinetics, pharmacodynamics, safety, and tolerability of dupilumab in healthy adult subjects. Clin Pharmacol Drug Dev. 2020;9(6):742–755. doi:10.1002/cpdd.798
7. Wenzel S, Castro M, Corren J, et al. Dupilumab efficacy and safety in adults with uncontrolled persistent asthma despite use of medium-to-high-dose inhaled corticosteroids plus a long-acting β2 agonist: a randomised double-blind placebo-controlled pivotal phase 2b dose-ranging trial. Lancet. 2016;388(10039):31–44. doi:10.1016/S0140-6736(16)30307-5
8. Tofte SJ, Papp K, Sadick N, et al. Efficacy and safety of dupilumab for the treatment of moderate-to-severe atopic dermatitis in adults: a pooled analysis of two phase 2 clinical trials. J Am Assoc Nurse Pract. 2018;30(9):529–541. doi:10.1097/JXX.0000000000000088
9. Cork MJ, Thaçi D, Eichenfield LF, et al. Dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: results from a phase IIa open-label trial and subsequent phase III open-label extension. Br J Dermatol. 2020;182(1):85–96. doi:10.1111/bjd.18476
10. Bachert C, Mannent L, Naclerio RM, et al. Effect of subcutaneous dupilumab on nasal polyp burden in patients with chronic sinusitis and nasal polyposis: a randomized clinical trial. JAMA. 2016;315(5):469–479. doi:10.1001/jama.2015.19330
11. Castro M, Corren J, Pavord ID, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. 2018;378(26):2486–2496. doi:10.1056/NEJMoa1804092
12. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375(24):2335–2348. doi:10.1056/NEJMoa1610020
13. Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. 2019;394(10209):1638–1650. doi:10.1016/S0140-6736(19)31881-1
14. Maspero JF, Khan AH, Philpott C, et al. Health-Related Quality of Life Impairment Among Patients With Severe Chronic Rhinosinusitis With Nasal Polyps in the SINUS-24 Trial. J Asthma Allergy. In press.
15. Laidlaw TM, Bachert C, Amin N, et al. Dupilumab improves upper and lower airway disease control in chronic rhinosinusitis with nasal polyps and asthma. Ann Allergy Asthma Immunol. 2021;126(5):584–592.e581. doi:10.1016/j.anai.2021.01.012
16. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 Report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
17. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
18. Giavina-Bianchi P, Aun MV, Takejima P, Kalil J, Agondi RC. United airway disease: current perspectives. J Asthma Allergy. 2016;9:93–100. doi:10.2147/JAA.S81541
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.